

Abstract
Background
Smoking has physical, psychological, and social impacts on women’s health and subsequentlythe community’s health. Therefore, it is important to have an estimation of smoking among Iranian women.Since comprehensive data are not available in this respect, the authors performed a systematic review and metaanalyzedall high-quality studies in this field.
Methods
All available electronic papers were searched by certain keywords and were included in this studyaccording to the inclusion criteria regardless of the publication year. Furthermore, non-electronic resources includingthe final report of research projects, dissertations, unpublished papers (grey literature) and books publishedby the Iranian ministry of health were also evaluated in the study. The materials were assessed for theirquality and meeting the inclusion and exclusion criteria. Considering the high degree of variability in many selectedstudies, we used random effect method for meta-analysis.
Results
The highest and lowest rates of cigarette smoking among women were 10.5% and 0.04%, respectively.The prevalence rates of smoking were different in various subgroups; ranging from 0 to 0.4% in students, 1.1to 3.1% in adults, and 1.4 to 8.7% in all subgroups. According to the meta-analyses performed for the subgroups,the mean age of participants, performing the study in urban or rural areas, and the year of paper publicationwere major sources of heterogeneity.
Conclusion
The studies were highly different with regard to their findings, and it seems that there is an ageand time trend for the findings. Furthermore, the prevalence of smoking was different in various regions of thecountry.
Keywords: Smoking, Cigarette smoking, Prevalence, Meta-analysis, Women
Introduction
Non-infectious diseases comprise 43% of the disease burden around the world; and it is expected that in 2020 the diseases become responsible for 60% of the total disease burden and 73% of all cases of death. Smoking is one of the factors commonly observed in many countries (1). Large epidemiological studies in different countries have shown that smoking is highly correlated with incidence of many non-infectious diseases (2,3). In many countries, smoking is equal to cigarette smoking. Mortality rate of cigarette smokers in all age groups is 2-3 times higher than that in non-smokers. Prevention of non-infectious diseases is based upon identification of primary and major risk factors, and prevention and control of these factors (4,5). Cigarette smoking and alcohol cause cardiovascular disease, myocardial infarction, many serious diseases, as well as many cancers (6).
According to the world health organization (WHO) report, the global prevalence of cigarette smoking is 47% and 12% in men and women, respectively. The rate is 7% for women in the developing countries versus 25% for women in the developed countries (7). Studies in different countries have shown that the rate of smoking is higher in men. However, in most studies a decrease in the gap between the rate of smoking in men and women has been shown (8-10). Therefore, it could be concluded that the prevalence of smoking among women is increasing. The results of a study in the USA demonstrated that the rate of smoking is decreasing among men and increasing among women. The rate of smoking was also higher in girls than boys (11).
In our country, based on the Tehran Lipid and Glucose Study (TLGS), the prevalence of cigarette smoking was 10.6% (22% in men versus 2.1% in women) (12). In the study carried out by Ahmadi et al. in Shiraz, the prevalence rates of smoking among men and women were 26% and 3.6%, respectively (13). The rate of cigarette smoking among women in all the studies carried out in Iran was in the range of 1.3-5.9% (13-16). However, the spectrum of smoking has not been thoroughly investigated in women. In a study carried out in the urban and rural areas of Tehran in 1999 to 2000, the rates of daily smoking in male and female people above 15 were 22.2% and 2.1%, respectively (1). The smoking rates obtained in this study were higher than those reported by the studies performed in the previous years (18,19,21) and lower than those reported in the studies performed later (19,17-22). This may indicate the increasing trend of smoking in the community.
An increasing trend for cigarette smoking among Iranian population has been demonstrated. The results reported by Emami et al. (estimated smoking rate of 12.1% in Tehran) also confirms it (23). According to WHO reports, the rates of smoking and smoking-related diseases are increasing among women, particularly young women; such that the ratio of smoking women has increased 12% all over the world, and frequency of lung cancer in women has exceeded breast cancer in some parts of the world (24).
In spite of the slight increase in the rate of cigarette smoking among Iranian women, the rate is still much lower than that in men and also in comparison with the rates reported for women in many other countries. Several studies have been performed in this respect and the prevalence rate of smoking among Iranian women was reported in the range of 0.04 to 10.5%. Since the prevalence data is sparse, it seems that carrying out a systematic review and careful analysis of the data could produce valuable information about cigarette smoking among Iranian women.
The aim of this study is to extract maximal available and published data about cigarette smoking among Iranian women in recent years, and to provide a more comprehensive picture of the problem by combining the results obtained in recent years.
Methods
Search strategy: To find the studies related to the prevalence rate of cigarette smoking, Iranian and international electronic sources of Iran-Doc, Iran-Medex, CINAHL, PsycINFO, Embase, Medline, Cochrane Tobacco Addiction Group, SID, EBSCO host, OVID, Science direct, Iranpsych, Pubmed, WHO, BIOMED, Magiran, and Google Scholar were searched for related documents during 1995 to 2011. The search strategy was mainly systematic use of Persian and English keywords with all possible combinations. To improve the search sensitivity, general keywords were used as follows; (woman OR girl) AND (cigarette OR smoking) AND (frequency OR prevalence) AND Iran. The bibliographies of searches were screened to find relevant data. Moreover, in order to access the grey literature, non-electronic resources were searched. The resources includes proceedings of the conferences, dissertations, and the data produced by state and non-state centers and organizations that have research activities in the field of addiction.
Criteria for selection and evaluation of quality of the papers: Firstly, the titles and abstracts of all papers were searched in order to find relevant titles. Then, all papers were searched and relevant papers were reviewed. The aim of the study was to determine the prevalence rate; thus, inclusion criteria were giving an estimation of cigarette smoking among Iranian women, and conduction of the study in Iran. Another inclusion criterion was having acceptable quality with regard to the study population, design, avoiding biases, and the method of dealing with confounding factors. After finding studies with relevant titles, the paper abstracts were evaluated using the STROBE checklist (Strengthening the Reporting of Observational Studies in Epidemiology). The checklist included 22 major items as follows: title and abstract, introduction, methodology and study design, measurement of variables, statistical analysis, aims of the study, results, discussion, and conclusion. Finally, papers that obtained the minimum score of 16 out of 22 were selected for data extraction step of the meta-analysis process and underwent statistical analysis.
In this study, 152 papers were found in the primary search. Then, after reviewing the titles, 120 papers were selected, and after evaluation of the papers for their abstracts, 83 irrelevant papers that did not meet the inclusion criteria were excluded. The remaining 37 studies entered the third step; i.e., qualitative evaluation. The studies with population not representative of the general population, and those having low quality according to the checklist were excluded. Four studies were not included in the analysis owing to wide variations among them and other studies. For example, studies by Amiri et al. in 2003 in Bushehr due to the wide variations equal to 939.75, Ansari et al. in 2006 in Tehran due to insufficient sample size (less than 350 samples), Ismaili Nadimi et al. in 2006 in Rafsanjan due to high variation equal to 886.37, and Divsalar et al. in 2003 in Kerman due to wide variations equal to 546.36 were omitted (25-28). Furthermore, studies that addressed smoking only in men were excluded.
Finally, 12 papers were included in the meta-analysis. However, two papers were not accessible in full text for the authors, and the abstracts were used for analysis. Among the papers selected, three were derived from national projects, and were analyzed separately ( Fig. 1).
Figure 1 .

Flowchart of inclusion of the studies in our systematic review and meta-analysis.
The studies were performed in different regions of Iran and within different groups. They addressed four population subgroups as follows: 1) students in the age range of 11-18, 2) university students at the age of 20 and above, 3) adults in the age range of 20-40, and 4) all individuals of 15-64 years old. Studies that addressed subgroup 3 and the studies on age groups above 35 or with old publication years were analyzed descriptively. Then, a datasheet was prepared to extract the descriptive data, which is enclosed. The datasheet included bibliographic data (place of study, first author’s name, year of study, place of sampling, sample size, prevalence of cigarette smoking in the study, and the mean age range of participants). Moreover, the criteria related to quality of the studies were recorded in the forms.
It should be mentioned that since we did not have access to the details of primary data of each participant, in each study the general data of prevalence of cigarette smoking among women, sample size, place and time of study, and other necessary data were used as aggregated data.
Data extraction: In this step, a form with eight sections was designed. Then, basic data required for the study was collected. The required information included the bibliographic data (subject, title, journal’s name, and author) and methodological data (methodology and study design), as well as the information on the prevalence of cigarette smoking among women, general characteristics of the samples, methods of data evaluation, groups or target groups, and quantitative data of the samples such as mean age of smokers, amount of smoking, and elimination of confounding variables.
Heterogeneity of definitions makes comparison of the results difficult. Therefore, to avoid it, we adopted the definitions provided by the WHO. Considering the WHO definition, cigarette smokers were selected with regard to the history of the number of cigarettes smoked during a day as follows:
Active smoker: an individual who smokes more than seven cigarettes per week (at least one cigarette per day)
Heavy smoker: an individual who smokes more than 20 cigarettes per day (29-31).
Statistical analysis: In this step, the prevalence rate of women’s cigarette smoking in all related descriptive studies were collected. Then, variances of each study were determined using the binomial distribution formula. Using heterogeneity test (Cochrane Q test), statistically significant difference among findings of the studies were determined, and then random effect model was used in the estimation. The point estimation and 95% confidence interval (95% CI) were calculated by describing the findings in the forest plot. All statistical analyses were performed using STATA, version 10.
Results
By evaluating the quality of full text of 12 relevant papers, 33173 women were eligible to be included in the study. The details of the data used in the meta-analysis are depicted in Table 1. The lowest prevalence of cigarette smoking among Iranian women (0.04%) was reported by Kelishadi et al. in Isfahan, 2003. They evaluated the prevalence of smoking among students in the age range of 11-18 in urban and rural areas with a large samples size. These factors could explain the low prevalence rate. The highest prevalence rate of smoking among Iranian women (10.5%) was reported by Amiri et al. in Bushehr, 2003. The prevalence rate was significantly higher than those reported in other Iranian studies. This can be explained by performing the study on the urban population, and in the age range of 25-64, among whom 68% were above 35.
Table 1. Characteristics of studies that met the inclusion criteria for meta-analysis of smoking prevalence among women.
|
Place of study (source) |
Sub groups | Age | Prevalence (%) |
Sample size |
Place of sampling |
Time of Publication |
Time of study |
| Bandar-abbas | All of age groups | 15< | 0.9 | 1810 | Urban | 2007 | 2007 |
| Semnan | All of age groups | 30-70 | 0.5 | 2104 | Both | 2005 | 2005 |
| Tehran | All of age groups | 15< | 2.1 | 11801 | Urban | 2001 | 1998-2001 |
| 17 regions of Tehran | All of age groups | 25-64 | 4.2 | 1573 | Urban | 2003 | 2002-3 |
| All of province | All of age groups | 15-69 | 9.7 | 26618 | Both | 1990 | 1990 |
| All of province | All of age groups | 15-64 | 4.2 | 84706 | Both | 2005 | 2005 |
| All of province | All of age groups | 15-64 | 1.4 | 5281 | Both | 2007 | 2007 |
| Isfahan | Students | 11-18 | 0.04 | 1950 | Both | 2004 | 2003 |
| Zahedan | Students | 14-17 | 0.4 | 475 | Urban | 2003 | 2003 |
| Kerman | Students | 11-18 | 0.4 | 860 | Urban | 2002 | 2002 |
| Orumie | adult | 20-44 | 3.6 | 3000 | Urban | 2004 | 2004 |
| Gonabad | adult | 20-40 | 1.7 | 356 | Urban | 2004 | 2004 |
Study on the subgroup of students: The overall prevalence in three eligible studies was 0.19% (95% CI= 0- 0.4). However, the findings were found to be significantly incongruent (I2= 0.54) (Table 2). Results of meta-analysis for this subgroup showed the lowest prevalence rate in this subgroup, which is explained by the low mean age of the students (Fig.2).
Table 2. Comparative results in evaluated subgroups with regard to smoking prevalence among women.
| Subgroup | Prevalence rate | P | 95% CI | incongruity | I2 |
| Students | 0.19% | 0.00-1 | 0-0.47 | 4.3 | 0.54 |
| Adults | 2.12% | 0.00-1 | 1.1-3.1 | 140.1 | 0.96 |
| National studies | 5.098% | 0.00-1 | 1.4-8.7 | 1229.4 | 0.99 |
Fig. 2.
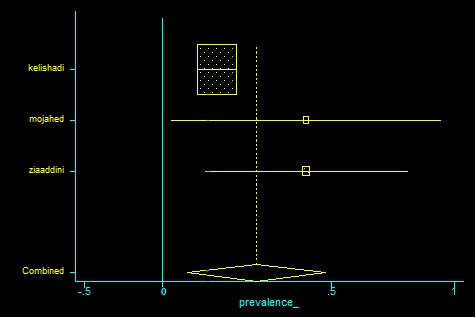
Comparative results in evaluated subgroups with regard to smoking prevalence among students.
Study on the subgroup of adults: The overall prevalence rate for six eligible studies was 2.12% (95% CI= 1.1-3.1). Nevertheless, the studies were found to be significantly incongruent with regard to their findings (I2= 0.96) (Table 2).
In these studies, the wide and sometimes different age range of participants and accumulation of the data obtained from urban and rural areas led to incongruity. Therefore, meta-analysis results for this subgroup were separately interpreted ( Fig. 3).
Fig. 3.
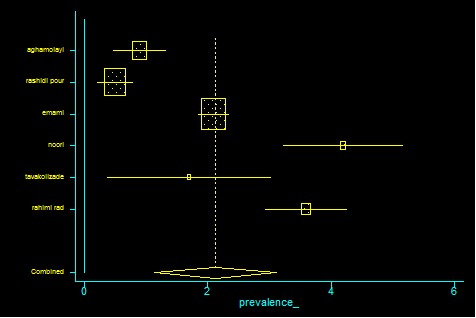
Comparative results in evaluated subgroups with regard to smoking prevalence among adults.
Results of meta-analysis in national studies: The overall prevalence rate for three eligible studies was 5.098% (95% CI= 1.4-8.7). Nevertheless, it was found that the studies were significantly incongruent in their results (I2= 0.96). ( Table 2) Publication years and accumulation of the data from urban and rural areas around the country were major sources of incongruity, and thus the results of meta-analysis for these studies were evaluated separately (Fig. 4).
Fig. 4.
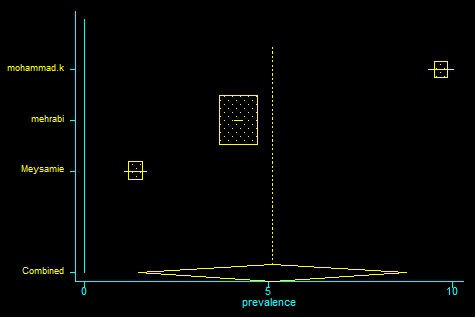
Comparative results in evaluated subgroups with regard to smoking prevalence among national studies.
Discussion
In this study, it was attempted to achieve an estimation of the overall prevalence of cigarette smoking among Iranian women by evaluating the findings reported in other studies. Results of the current study demonstrated that in the three subgroups evaluated, smoking rate among Iranian women is estimated within the range of 0.19-5.09%. There is a significant incongruity among the studies with regard to their findings. Using meta-analysis of the subgroups, major sources of incongruity in the studies were determined as the mean age, living in urban or rural areas, and publication year of the papers.
The overall prevalence rates of cigarette smoking among Iranian women in different regions of the country were 0.19, 2.12, and 5.09% for students, adults, and national surveys in all provinces of the country, respectively. The rates are comparable with the WHO estimation of 4.3% in 2005 (32). The rates reported in various studies were different owing to the difference in the study area extent, place of sampling, and the sample size. Major factors influencing the difference in the prevalence rates reported were the mean age, living in urban or rural areas, and the year of carrying out the study and publishing the papers.
In the current study, comparing the overall prevalence of cigarette smoking among Iranian women in urban and rural areas was not possible owing to the small number of studies meeting the analysis criteria.
In the study, the highest quality paper was the one written by Meysami et al. in 2007 titled as the smoking pattern among Iranian adult population. They reported the smoking rate among Iranian women as 1.4% (33). In their study, adults age groups in urban and rural areas and characteristics of the population under study were clearly defined.
The highest rate was reported in a study performed in Bushehr on people above 25 in the capital city of the province, while the lowest rate was reported in a study on male and female students in the age range of 11 to 18, living in rural areas of Isfahan. Regarding the people’s culture in rural areas and the negative attitude toward smoking by girls and women in these areas, it was shown that the rate was lower in the studies that were performed on rural population or rural and urban population collectively (17).
According to the WHO report in 2008, the rate of cigarette smoking among Iranian women was higher than that among Iraqis (1.6%), women in the UAE (1.2%), less than that in Turkey (14.8%), and almost similar to the rates in other Persian Gulf countries (32).
In another study conducted by the WHO on the Iranian population, a decrease in the smoking rate was reported from 1991 (3.4%) to 2000 (1.5%) (34). Also, the studies have shown that the rate of smoking among Iranian women is much less than all other European countries except Azerbaijan (0.4%) (35).
However, since in the Iranian culture there is a negative attitude toward smoking by women and in all the studies included in the study, the surveys were performed by asking the people about smoking, there is a possibility for under-report. For instance, Sarafzadegan et al reported a statistically significant difference between the rates of self-report and chemical indices of smoking in women (1.3% versus 6.7%) (15).
The increasing rate of smoking among young women in the developing countries is a major concern for the WHO in public health and prevention of the diseases. Improved health condition and consequently increasing proportion of the elderly population in the developing countries leads to an increase in the rate of non-infectious diseases in these countries. Therefore, it is necessary for these countries to adopt appropriate measures to reduce risk factors of these diseases. Smoking is a confirmed risk factor in this respect. Moreover, women comprise a target and susceptible group in health systems and maintaining their health is of great importance. Cigarette smoking by women is not only a major health problem in Iran and the eastern Mediterranean countries, but also all over the world. According to the WHO report in 2005, the number of smoking women has increased by 60% in the past 20 years. Results of global surveys on smoking status among adolescents have shown that the rate of smoking is increasing in girls of 13 to 15 worldwide. However, in the current study, the rate of smoking among female students was lower (33).
One of the limitations of the current study was that most relevant studies were performed on a certain population subgroup such as students, university students, adolescents, the young, specific age groups, or different parts of the country. Several studies in the country have addressed the rate of smoking among boys and men. There was only one study on smoking rate among women. In general, few studies with acceptable sample size and study design were available on different age groups of the Iranian women population.
The definition of being a smoker and inclusion criteria were different for various studies. This makes comparison of different studies difficult. It is suggested that a uniform framework for the study design, methodology, and definition of the variables be adopted for similar studies.
Carrying out studies only on the smoking rate among women is not sufficient, and studies on all age groups and also certain groups of women should be performed. However, similar to original studies, these meta-analyses are prone to inevitable limitations, biases, and errors. To achieve a more accurate picture with higher reliability, it is suggested to perform studies with similar and standard methodology at the national level in this respect.
Conclusion
Results of this systematic review indicate that prevalence of smoking among Iranian women is less than the rates reported by the WHO. Moreover, the rate of smoking among Iranian women is significantly less than the rates reported for the EMRO region (Eastern Mediterranean Regional Office) and reports of the WHO. Prevalence rate of smoking in our country has not probably changed in comparison with previous decades (32).
Owing to the large number of studies with different methodologies and results, and evaluation of the current status, it is difficult to predict the future status of smoking among women. However, it seems that prevalence of cigarette smoking among women above 25 and adults is higher than the rates in other age groups. Considering the high proportion of young population, an increase in the rate of smoking among Iranian women is predictable.
References
- 1. A National Profile of Noncommunicable Disease Risk Factors in the I.R. of IRAN, Ministry of Health and Medical Education Center for Disease Control 2005.
- 2.Hughes K, Choo M, Kuperan P, Ong CN, Aw TC. Cardiovascular risk factors in relation to cigarette smoking: a population-based survey among Asians in Singapore. Atherosclerosis. 1998;137:253–58. doi: 10.1016/s0021-9150(97)00268-2. [DOI] [PubMed] [Google Scholar]
- 3.Immaura H, Tanaka A, Hirae C, Futagami T, Yushimura Y, Uchida K, Kobata D. Relationship of cigarette smoking to blood pressure & serum lipid & lipoprotein in men. Clin Exp Pharmacol Physiol. 1996;23:397–402. doi: 10.1111/j.1440-1681.1996.tb02748.x. [DOI] [PubMed] [Google Scholar]
- 4. The WHO stepwise approach (Surveillance of risk factors for noncommunicable diseases); World Health Organization; Geneva 2001.
- 5. STEPS Instrument for NCD Risk Factors (Core and Expanded Version 1.4); World Health Organization; Geneva 2003.
- 6.Haenle MM, Brockmann OS, Kron M, Bertling U, Mason AR, Steinbach G. et al. Overweight, physical activity, tobacco and alcohol consumption in a cross-sectional random sample of German adults. BMC Public Health. 2006;6:233. doi: 10.1186/1471-2458-6-233. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. World Health Organization information [homepage on the Internet]. Smoking and woman [updated August, 1997];176 Fact. Available from:http://whqlibdoc.who.int/fact_sheet/1997/FS_176_eng.pdf
- 8.Johnson CA, Palmer HP, Chou CP, Pang Z, Zhou D, Dong L. et al. Tobacco use among youth and adults in Mainland China: The China Seven Cities Study. Public Health. 2006;120:1156–69. doi: 10.1016/j.puhe.2006.07.023. [DOI] [PubMed] [Google Scholar]
- 9. Nobile CGA, Trani F, Di Sandro M, Angelillo IF (2006). Cigarette smoking and alcohol behavior among adolescents in Italy. Public Health, 120: 942-45. [DOI] [PubMed]
- 10.Musaigera AO, Abdulraoof N. Social factors associated with smoking among men in the United Arab Emirates. Public Health. 2004;118:450–52. doi: 10.1016/j.puhe.2003.08.003. [DOI] [PubMed] [Google Scholar]
- 11.Benowitz NL, Hatsukami D. Gender differences in the pharmacology of nicotine addiction. Addiction biology. 1998;3(4):389–404. doi: 10.1080/13556219871930. [DOI] [PubMed] [Google Scholar]
- 12.Azizi F, Rahmani M, Emami H, Mirmiran P, Hajipour R, Madjid M. et al. Cardiovascular risk factors in an Iranian urban population: Tehran lipid and glucose study (phase 1) Soz Praventivmed. 2002;47(6):408–426. doi: 10.1007/s000380200008. [DOI] [PubMed] [Google Scholar]
- 13.Ahmadi J, Khalili H, Jooybar R, Namazi N, Mohammadagaei P. Prevalence of cigarette smoking in Iran. Psychol Rep. 2001;89:339–341. doi: 10.2466/pr0.2001.89.2.339. [DOI] [PubMed] [Google Scholar]
- 14.Mehrabi S, Delavari A, Moradi Gh, Esmailnasab N, Pooladi A, Alikhani S, Alaeddini F. Smoking among 15 to 64 Year-Old Iranian People in 2005. Iranian Journal of Epidemiology. 2007;3:1–9. [Google Scholar]
- 15.Saraf-Zadegan N, Boshtam M, Shahrokhi S, Naderi GA, Asgary S, Shahparian M, Tafazoli F. Tobacco use among Iranian men, women and adolescents. Eur J Public Health. 2004;14:76–78. doi: 10.1093/eurpub/14.1.76. [DOI] [PubMed] [Google Scholar]
- 16.Ahmadi J, Khalili H, Jooybar R, Namazi N, Aghaei PM. Cigarette smoking among Iranian medical students, resident physicians and attending physicians. Eur J Med Res. 2001;6:406–408. [PubMed] [Google Scholar]
- 17.Kelishadi R, Ardalan G, Gheiratmand R, Majdzadeh R, Delavari A, Heshmat R. et al. Smoking behavior and its influencing factors in a national – representative sample of Iranian adolescents: Caspian study. Prev Med. 2006;42(6):423–6. doi: 10.1016/j.ypmed.2006.03.001. [DOI] [PubMed] [Google Scholar]
- 18.Kelishadi R, Hashemipoor M, Sarrafzadegan N, Sadri GhH, Bashardoost N, Alikhasi H. et al. Effects of some environmental factors on smoking and the consequences of smoking on major cardiovascular disease (CVD) risk factors in adolescent: Isfahan healthy heart program-heart health promotion from childhood. Journal of medical faculty Guilan university of medical sciences. 2004;50(13):75–62. [Google Scholar]
- 19.Majdzadeh SR, Zamani GH, Kazemi SH. Qualitative survey on the factors affecting tendency to Hookan in Hormozgan province and appropriate campaign methods against it. Hakim research journal. 2002;3(5):183–7. [Google Scholar]
- 20.Mojahed A, Bakhshani NM. Prevalence of smoking and drug abuse in students of Zahedan high schools Tabib-e-Shargh. Journal of Zahedan university of medical sciences and health services. 2004;1(16):59–65. [Google Scholar]
- 21.Ziaadini H, Zarezadeh A, Heshmati F. The prevalence rate of substance abuse and addiction and some relevant factors among junior and senior high school students in Kerman city (2000-2001) Journal of Kerman university of medical sciences. 2006;13(2):84–94. [Google Scholar]
- 22.Ziaadini H, Ziaadini MR. The prevalence of tobacco use and dependency and its relation to some demographic factors in people aged 12 and over in rural sample. Journal of fundamentals of mental health. 2006;8:17–22. [Google Scholar]
- 23.Emami H, Habibian S, Salehi P, Azizi F. Pattern and smoking habit in an urban area in Tehran, Tehran Glucose and Lipid Study, 2001. Pejouhesh. 2003;27(1):47–52. [Google Scholar]
- 24. Tobacco Control in developing countries WHO, World bank, the economics advisory service, oxford university press 2000; :361-362.
- 25.Amiri Amiri, M M, Emami SR, Nabipoor I, Nosrati A, Iranpoor D, Soltanian A. et al. cardiovascular risk factor in bushehr monica project of WHO. Iranian Sout Medical Journal. 2004;6(2):151–161. [Google Scholar]
- 26.Ansari R, Mokhtari MR, Khosravi A. Prevalence and cause of smoking in the medicine students. . Koomesh . 2007;9(1):21–26. [Google Scholar]
- 27.Esmaieli Nadimi A, Ahmadi J. Cigarette smoking among urban population of Rafsanjan . Hormozgan Uni Med J. 2004;7(4):173–177. [Google Scholar]
- 28.Divsalar K, nakhaei N, amini MR. The relationship between religious activities and cigarette smoking in one of the university students in Kerman, . Journal of Teb va Tazkie. 2007;16(3-4):63–69. [Google Scholar]
- 29. World Health Organization: Process for a Global Strategy on Diet Physical Activity and Health Geneva: World Health organization; 2003.
- 30.Smith CS, Greenland P, Grundy MS. Prevention Conference V: Beyond Secondary Prevention: Identifying the High-Risk Patient for Primary Prevention: Executive Summary. Circulation. 2000;101:111–16. doi: 10.1161/01.cir.101.1.111. [DOI] [PubMed] [Google Scholar]
- 31. The World Health Report 1999. Combating the Tobacco Epidemic. World health organization. Geneva, World Health Organization, 1999.
- 32. World Health Organization. Report on the Global Tobacco Epidemic 2008. The MPOWER package. Geneva, World Health Organization, 2008.
- 33.Meysamie A, Ghaletaki R, Haghazali M, Asgari F, Rashidi A, Khalilzadeh O, Esteghamati A, Abbasi M. Pattern of tobacco use among the Iranian adult population. Tob Control. 2010;19:125–128. doi: 10.1136/tc.2009.030759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Mohammad K, Noorbala AA, Majdzadeh SR, Karimloo M. Trend of smoking prevalence in Iran from 1991 to 1999 based on two national health survey. Hakim Res. 2000;3(4):290–297. [Google Scholar]
- 35. World Health Organization [homepage on the Internet]. The European tobacco control report, 2007. Geneva: WHO, Regional Office for Europe, [updated 2007; cited 2007 Dec]. Available from: http://www.euro.who.int/document/e89842.