

Abstract
The ability to play a musical instrument represents a unique procedural skill that can be remarkably resilient to disruptions in declarative memory. For example, musicians with severe anterograde amnesia have demonstrated preserved ability to play musical instruments. However, the question of whether amnesic musicians can learn how to play new musical material despite severe memory impairment has not been thoroughly investigated. We capitalized on a rare opportunity to address this question. Patient SZ, an amateur musician (tenor saxophone), has extensive bilateral damage to his medial temporal lobes following herpes simplex encephalitis, resulting in a severe anterograde amnesia. We tested SZ’s capacity to learn new unfamiliar songs by sight-reading following three months of biweekly practices. Performances were recorded and then evaluated by a professional saxophonist. SZ demonstrated significant improvement in his ability to read and play new music, despite his inability to recognize any of the songs at a declarative level. The results suggest that it is possible to learn certain aspects of new music without the assistance of declarative memory.
Introduction
Patients with dense amnesia due to bilateral medial temporal lobe damage (Wilson, Baddeley, & Kapur, 1995; Anderson et al., 2007) or due to dementia of the Alzheimer’s type (Schacter, 1983; Beatty et al., 1988, 1994, 1999; Crystal, Grober & Masur, 1989; Cowles et al., 2003; Fornazzari et al., 2006; for a review see Baird & Samson, 2009) have demonstrated a remarkable ability to continue to perform certain types of activities that they learned prior to brain injury (e.g., driving, playing a musical instrument, and playing golf). The ability to learn and retain new perceptual or motor skills (e.g., rotary pursuit, mirror-tracing, and mirror-reading) and the ability to learn new habits (e.g., probabilistic-learning) are also known to be intact in amnesic patients (e.g., Milner, 1962; Cohen & Squire, 1980; Gabrieli, Corkin, Mickel, & Growdon, 1993; Tranel, Damasio, Damasio, & Brandt, 1994; Hay, Moscovitch & Levine, 2002; Cavaco, Anderson, Allen, Castro-Caldas & Damasio, 2004). Cohen and Squire (1980) found that amnesic patients were able to acquire the mirror reading skill at a normal rate despite poor memory for the words that they had read. This dissociation led these authors to distinguish between declarative forms of memory (dependent on the medial temporal lobe system), and procedural, nondeclarative forms of knowledge which are often spared in amnesic patients. Declarative memory refers to the capacity for conscious recollection about facts and events, whereas nondeclarative memory is expressed through performance rather than recollection (Squire, 2004). Nondeclarative memory includes different forms of learning and memory abilities, including the perceptual and motor skills involved in musical performance. Even though some aspects of the musical performance can be declared, the actual skills are often carried into action without conscious retrieval of information regarding the procedural aspects of music.
Understanding how the brain processes music and how music can help neurological patients heal and overcome adversity is a rapidly growing field of study (Levitin, 2007; Sacks, 2008). A series of case reports have described patients with significant declarative memory impairments who can still play musical instruments somewhat skillfully (Beatty et al., 1988, 1994, 1999; Crystal et al., 1989; Wilson et al., 1995; Beatty, Brumback, & Vonsattel, 1997; Baur, Uttner, Ilmberger, Fesl & Mai, 2000; Cowles et al., 2003; Fornazzari et al., 2006). All of these reports describe instances of amnesic musicians who are able to perform songs that they had learned how to play prior to the onset of their amnesia. Perhaps the most well-known of these cases is Clive Wearing, a renowned musicologist with severe amnesia after sustaining bilateral medial temporal lobe damage due to herpes simplex encephalitis (Wilson et al., 1995). According to the authors, Clive demonstrated an intact ability to “sight-read, obey repeat marks within a short page, and understand the significance of a metronome mark… ornament, play from a figured bass, transpose, and extemporize.” This description of Clive’s musical skills was the first non-neurodegenerative evidence of relatively preserved ability to perform a musical instrument despite severe multi-modal declarative memory impairment. It is currently unknown, however, whether or not Clive is able to learn how to play new songs.
Two early case reports described attempts to teach unfamiliar songs to piano players with dementia of the Alzheimer’s type; one by sight-reading (Beatty et al., 1988) and the other by ear (Beatty et al., 1999). Even though both patients were able to play familiar songs that had been learned premorbidly, their ability to learn a new composition was rather limited. However, the patients’ significant non-amnestic cognitive impairments may have hampered their ability to engage with the training process. Cowles and colleagues (2003) later described the case of a moderately demented patient with probable Alzheimer’s disease who was able to play a new song on the violin and demonstrated some limited capacity to play parts of the song by request (i.e., playing without sheet music) at delays of 0 and 10 minutes. The attempts to cue the patient’s performance by providing the first measures of the new song were found unsuccessful. Fornazzari and colleagues (2006) assessed the ability of a professional pianist with probable Alzheimer’s disease to learn unfamiliar musical pieces and observed “gradual improvements in overall performance and in rhythm, field elements, harmony, melodic accuracy, and sophistication in the accompaniment of the left hand” over a seven day period. However, the authors did not provide any quantification of the improvements. Baur and colleagues (2000) described a herpes simplex encephalitis patient (CH) who learned how to play the accordion, autodidactically, after the onset of her amnesia. Patient CH did not have any premorbid sight-reading training nor did she have any experience of playing a musical instrument. Yet, remarkably, she was able to learn how to play 90 pieces of Austrian and German folk music after listening to the songs on the radio or on tape. Moreover, she was able to play a song when cued with the song title, and she was also able to provide the song title when cued with a recording of the music. This suggests that CH had preserved declarative memory for the music, despite her overall poor performance on a battery of standardized memory tests. Thus, at least some of CH’s intact ability to learn new music could be explained by her reservoir of preserved declarative memory for music. Taken together, the results of the five aforementioned case studies are mixed. Two of the Alzheimer’s patients were unable to learn new music, whereas two other Alzheimer’s patients showed some residual learning. In addition, the findings in encephalitic patient CH are confounded by the patient’s ability to learn new declarative information about music.
To date, then, available research does not provide a definitive conclusion about whether the ability to learn and play unfamiliar music can be preserved in the context of a severe impairment in declarative memory. Here, we explored the capacity of an amateur musician, who had dense multi-modal anterograde amnesia, to perform and learn a series of new songs after three months of intense practice.
Subject
Patient SZ is a 51-year-old, fully left-handed man (-100 on the modified Geschwind-Oldfield Handedness Questionnaire) with 16 years of education and a bachelor’s degree in engineering. He had a normal developmental history and no neurologic problems until developing herpes simplex encephalitis at age 42. SZ’s MRI scans reveal large bilateral lesions affecting the hippocampus, amygdala, temporal poles, and insular cortices (Figure 1). The damage is more extensive in the left hemisphere, completely destroying the hippocampus, amygdala, temporal pole, adjacent sectors of the anterior temporal lobe, and most of the insular cortex, especially the anterior portion. In addition, the left hemisphere damage extends anteriorly into the basal forebrain and posterior surface of the orbitofrontal cortex. In the right hemisphere, the damage is not as severe and is largely circumscribed to the medial temporal lobe, medial temporal pole, and insular cortex.
Figure 1. MRI scans of patient SZ’s brain.
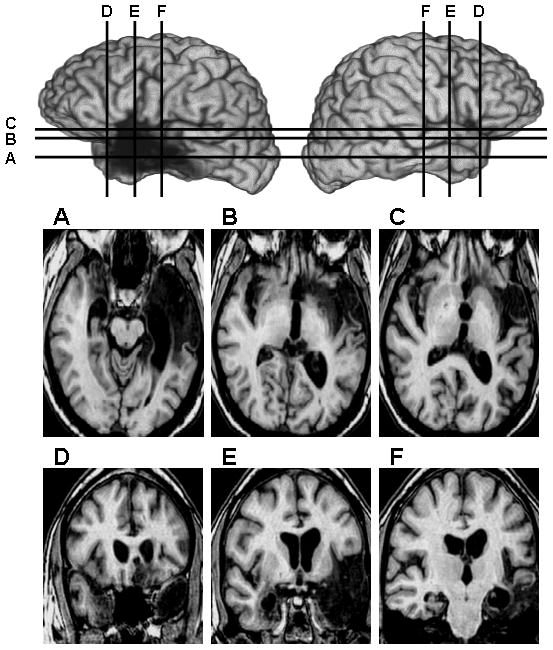
Lateral views of the left hemisphere (left) and right hemisphere (right) are shown in the upper section of the figure, and axial (A–C, middle row) and coronal (D–E, bottom row) slices are shown below. (A) Axial slice depicting bilateral damage to the medial temporal lobe, medial temporal poles, and unilateral damage to a large region of the left temporal lobe. (B & C) Axial slices depicting bilateral damage to the insular cortex and left-sided damage to the basal forebrain and posterior orbitofrontal cortex. (D) Coronal slice depicting bilateral damage to the temporal poles (with only the medial temporal pole affected on the right side), and unilateral damage in the region of the left basal forebrain. (E) Coronal slice depicting bilateral damage to the amygdala and insula, and unilateral damage to a large region of the left temporal lobe. (F) Coronal slice depicting bilateral hippocampal damage and some damage to the left temporal cortices and left posterior insula. All images use radiological convention (i.e., right side of image = left hemisphere and vice versa).
On the neuropsychological evaluation (Tranel, 2009), SZ revealed a profound anterograde amnesia (Table 1). He was unable to recall or recognize any declarative information, verbal or visual, even after repeated presentations. Despite his severe declarative memory impairment, SZ has shown relatively preserved premorbid driving abilities (participant #2 in Anderson et al., 2007) and has demonstrated normal ability to acquire and retain a series of new perceptual-motor skills (subject #2 in Cavaco et al., 2004), suggesting intact procedural memory. Likewise, he also demonstrated intact performances on measures of working memory. His overall general intellectual functioning falls in the low average range, somewhat below expectations given his educational background. Some of his IQ scores were artificially reduced by his inability to remember the task instructions and his slowed processing speed. However, when examining specific measures that are known to be good indicators of premorbid intellectual functioning (e.g., reading ability, vocabulary, similarities, and matrix reasoning) his scores are in the average to above average range, well within normal expectations. His block design score and arithmetic achievement score are below expectations given his engineering background, a finding which might be partially related to the time constraint imposed by both tests that negatively affected his performance due to his slowed processing speed and poor memory for the task instructions. SZ’s basic language functioning, including naming and comprehension, is preserved (likely due to his left-handedness) despite extensive damage to critical language areas in the left hemisphere. His speech is fluent, well-articulated, and nonparaphasic, with normal rate, volume, and prosody. He does have a tendency to perseverate during conversations, often times repeating the same phrases multiple times. Additionally, he performed poorly on a test of verbal associative fluency. His basic visuospatial, visuoperceptual, and visuoconstructional abilities are mostly intact, although, once again, his slowed processing speed and tendency to forget task instructions at times adversely affected his test performance. He reported no signs of any depression or anxiety. He displayed a normal range of affect, including laughter and irritability. His anger is usually triggered by situations where he feels his independence is being hindered or his intelligence is being questioned. SZ displays a profound lack of awareness for his memory impairment (i.e., anosognosia), and will typically deny having any problems, or even weaknesses, in the domain of memory.
Table 1.
Neuropsychological evaluation
| Cognitive Areas | Neuropsychological Measures | Score | z-score | ||
|---|---|---|---|---|---|
| Intellect/Academic Achievement | Wechsler Adult Intelligence Scale-III * | Verbal IQ | 95 | −0.33 | |
| Performance IQ | 78 | −1.47 | |||
| Full Scale IQ | 87 | −0.87 | |||
| Digit Span | 9 | −0.33 | |||
| Max forward = 6; Max backward = 4 | |||||
| Vocabulary | 11 | 0.33 | |||
| Similarities | 11 | 0.33 | |||
| Block Design | 7 | −1.00 | |||
| Matrix Reasoning | 12 | 0.67 | |||
| Wide Range Achievement Test-III * | Reading | 109 | 0.60 | ||
| Spelling | 105 | 0.33 | |||
| Arithmetic | 93 | −0.47 | |||
|
| |||||
| Language | Boston Naming Test ** | 52 | −0.80 | ||
| Token Test ** | 44 | 1.00 | |||
|
| |||||
| Visuospatial perception | Judgment of Line Orientation ** | 28 | 1.33 | ||
| Benton Facial Recognition Test ** | 47 | 0.50 | |||
|
| |||||
| Learning and Memory | Wechsler Memory Scale-III * | Auditory Immediate Index | 65 | −2.33 | x |
| Visual Immediate Index | 53 | −3.13 | x | ||
| Immediate Memory Index | 51 | −3.27 | x | ||
| Auditory Delayed Index | 46 | −3.60 | x | ||
| Visual Delayed Index | 50 | −3.33 | x | ||
| Auditory Delayed Recognition Index | 55 | −3.00 | x | ||
| General Memory Index | 45 | −3.67 | x | ||
| Working Memory Index | 91 | −0.60 | |||
| Logical Memory Test ** | Immediate recall | 10 | −2.67 | x | |
| Delayed recall | 0 | −3.00 | x | ||
| Recognition | 11 | −5.10 | x | ||
| Auditory Verbal Learning Test ** | Trial 1 | 1 | −4.01 | x | |
| Trial 2 | 3 | −2.74 | x | ||
| Trial 3 | 5 | −2.18 | x | ||
| Trial 4 | 7 | −2.02 | x | ||
| Trial 5 | 5 | −3.74 | x | ||
| 30′ delayed recall | 0 | −3.24 | x | ||
| 30′ delayed recognition | 14 hits | −0.40 | |||
| 14 false positives | −13.88 | x | |||
| Benton Visual Retention Test (Form C) ** | Correct | 4 | −2.45 | x | |
| Errors | 12 | −3.06 | x | ||
| Complex Figure Test ** | 30′ delayed recall | 0 | −3.46 | x | |
| Warrington Recognition Memory Test ** | Words | 23 | −2.67 | x | |
| Faces | 30 | −2.33 | x | ||
|
| |||||
| Executive Functions | Trail Making Test (time in seconds) ** | A | 55 | −2.00 | x |
| B | 147 | −2.00 | x | ||
| Controlled Oral Word Association Test ** | 17 | −2.22 | x | ||
|
| |||||
| Visuomotor Abilities | Complex Figure Test ** | Copy | 32 | 0.44 | |
| Grooved Pegboard Test (time in seconds) ** | Dominant Hand (Left) | 78 | −1.05 | ||
| Nondominant Hand (Right) | 92 | −1.67 | |||
|
| |||||
| Emotional Functioning | Beck Depression Inventory ** | 0 | minimal symptomatology | ||
| Beck Anxiety Inventory ** | 2 | minimal symptomatology | |||
Scores are presented in standard/scaled scores (*) or as raw scores (**). The WAIS-III subtest scores are age-corrected scaled scores. The z-scores were calculated with reference to demographically matched normative samples (Tranel, 2009). Results that are below expectations or that are defective in comparison to demographically matched normative samples are marked with an X (i.e., scores greater than 2 standard deviations from the normative mean).
Musical experience
SZ received musical training on his saxophone between the ages of 12 and 18. In high school, SZ played in a jazz band that at one time competed at the national level and won the second place prize. After graduating from high school, he stopped playing the saxophone and did not resume playing until three years after his brain injury (i.e., over 27 years later). Both of SZ’s parents stated that they were impressed with how seamlessly he was able to play the saxophone again after such a long hiatus. For the past six years, SZ has been playing in an amateur orchestra. The conductor considers him an average saxophonist, rating him a 5 on a 10 point scale when compared to the other members of the orchestra (all of whom are healthy and without any notable memory problems or brain damage). According to the conductor, SZ is a good sight-reader and his main difficulties are maintaining a consistent tempo and staying in time with the band. The conductor stated that while most members of the orchestra tend to fall behind when playing, SZ tends to play too fast. Additionally, SZ will often skip repeat signs while reading sheet music. Consequently, no one has ever observed SZ enter into a never-ending loop, where he would continuously repeat a section of a song, forgetting each time that he had already repeated that same section. In order to reduce his rapid playing tempo and make sure he properly follows repeat signs, SZ’s mother accompanies him to all practices and concerts, and helps him follow along on the sheet music. An interesting feature of SZ’s personality and playing style is that he will only play music on his saxophone when provided with sheet music. He claims that he is unable to “play by ear” and consistently refuses any request to improvise a song or complete a song when cued or primed with the beginning notes. The one exception to this rule is his warm-up song, “Windy”, which he knows by heart and will routinely and spontaneously play without any sheet music. Of note, this song was written in 1967 by The Associations, over three decades before the onset of his brain injury.
In terms of music preferences, SZ stated that he likes “all styles” of music and has no particular preference. He often says, “music is the universal language… for children of all ages.” Interestingly, since his brain injury, music has become part of his identity. When asked about his dream job, he replied that he would like to be “a professional musician.” Moreover, he has stated that “music is empowering” and brings him immense joy in life. Both of his parents agree with this sentiment and have observed that music has a calming effect on SZ’s mood and has helped reduce occurrences of agitation and irritability.
Several anecdotes vividly illustrate the severity of SZ’s memory impairment while playing music. One example occurred at the end of a concert that SZ and his orchestra performed in front of an audience of approximately 500 people. A few minutes after the show was over, the audience congregated in the concert hall’s main entrance, waiting for the musicians to join them for a post-concert celebratory reception. One of the study’s co-investigators (J.S.F) approached SZ and inquired about when the concert would start. SZ, completely unaware that he and his orchestra had just finished performing a nearly 2-hour long concert, replied, “I think we’ll probably start here in a few minutes.” In a previous unpublished experiment, SZ was asked to play the song, “You Raise Me Up” (as performed by Josh Groban) eight consecutive times in a 22-minute period, taking a 30–60 second break in between each rendition. At the beginning and end of each of the 8 trials, SZ was asked whether he recognized the song and whether he had played the song before. In all cases, he denied having seen or played the song before. His amnesia was so dense that he would forget having played the song within a mere 30 seconds of completion. Of note, the song “You Raise Me Up” was written after the onset of his amnesia. This particular version was contained on one page of sheet music and could be played in approximately two minutes. Thus, even with a massive amount of exposure over a short period of time, SZ was unable to remember the music.
Procedures
Informed written consent was obtained from SZ and his family prior to participating in the study. The University of Iowa Institutional Review Board approved all study procedures. The conductor of SZ’s orchestra provided us with the sheet music (11 songs in total) that the orchestra would be learning once they returned from a holiday period. These 11 songs comprised our target condition. Based on his parents report, SZ had never seen nor played any of the target songs at anytime in his life. We also included sheet music for 5 control songs, all of which were only played during the testing sessions (i.e., he never practiced or played these songs in-between testing sessions). Blinded to the stimulus condition, the expert rater (author H.v.T.) classified the songs from 1 to 10, according to its level of difficulty for an amateur musician (Table 2).
Table 2.
Play list and assessment results comparing change from Time 1 to Time 2
| Play List
|
Assessment Results
|
|||||||
|---|---|---|---|---|---|---|---|---|
| Condition | Order | Song Title | Difficulty Level | Intonation | Sound Quality | Rhythmic Awareness | Notes Awareness | Sight-reading Accuracy |
| Target Songs | ||||||||
| 2 | Sleigh Ride | 5 | = | + | + | + | + | |
| 3 | Jesus, Jesus Rest Your Head | 4 | − | − | − | = | = | |
| 4 | First Suite in Eb for Military Band (part I. Chaconne) | 6 | − | − | = | + | = | |
| 7 | If Thou Be Near | 6 | − | − | − | = | = | |
| 8 | Brighton Beach | 5 | − | − | + | + | + | |
| 9 | Mountain Greenery | 5 | − | − | − | = | = | |
| 10 | Joshua | 7 | + | + | + | + | + | |
| 11 | The Belle of Chicago | 5 | = | − | + | + | = | |
| 12 | Old Scottish Melody | 6 | = | − | = | = | + | |
| 13 | Second American Folk Rhapsody | 5 | = | = | + | + | + | |
| 14 | Elsa’s Procession To The Cathedral | 5 | = | + | + | + | + | |
| Control Songs | ||||||||
| 1 | Memory | 4 | − | − | = | + | − | |
| 5 | First Suite in Eb for Military Band (part II. Intermezzo) | 3 | − | − | − | + | + | |
| 6 | First Suite in Eb for Military Band (part III. March) | 7 | − | − | = | + | + | |
| 15 | Them Basses | 4.5 | + | + | + | + | = | |
| 16 | Take the Coltrane | 6 | = | − | = | − | − | |
Assessment results (−) Time 2 < Time 1; (+) Time 2 > Time 1; (=) Time 2 = Time 1.
SZ’s musical performances were recorded during two separate testing sessions (time 1 and time 2) separated by 100 days. Time 1 occurred one week before the orchestra started rehearsing. Time 2 occurred after three months of continuous rehearsals during which the orchestra met twice a week for at least one hour per rehearsal. In total, SZ practiced the target songs for at least 30 hours between time 1 and time 2. During each testing session, SZ performed 16 different songs in a room by himself (i.e., without the orchestra). All songs were played by sight-reading using sheet music. The songs were presented in the same order each time (see Table 2). At the beginning of each song, the examiner presented SZ with the sheet music and asked him whether he recognized the name of the song and whether he remembered having played the song before. SZ then proceeded to play the song using a tenor saxophone (key of Bb). All performances were recorded using a digital audio recorder.
Each song was judged by a professional saxophonist (author H.v.T.; http://www.saxunlimited.com) who was blinded to both the song order (i.e., before versus after three months of practice) and type of song (i.e., target versus control song). SZ’s performances at time 1 and time 2 were rated on five different measures (intonation, sound quality, rhythmic awareness, notes awareness, and overall sight-reading accuracy). All ratings were provided on a 10-point scale with 0 being extremely poor performance and 10 being an adequate performance for an amateur musician. Intonation corresponds to the pitch accuracy between played intervals (with A=440Hz as reference). Sound quality depends on the flow of air and the pressure on the mouthpiece. Rhythmic awareness refers to the correct identification of the notated rhythm and the immediate correction when the duration of sound does not correspond to what is expected. Notes awareness refers to the correct identification of the written notes and the immediate correction when the sound does not correspond to what is expected based on the sheet music. The overall sight-reading accuracy refers to compliance with the sheet music instructions regarding: notes, rhythm, and tempo (e.g., Adagio-slow, Allegro-fast, Presto-very fast), dynamics (e.g., PP-very soft, FF-very loud, crescendo-get gradually louder, decrescendo-get gradually softer), and repeat signs.
Results
Declarative memory
SZ did not recognize any of the target or control songs at time 1 or time 2. In all cases, he completely denied having any memory or recognition for the song. The one exception was target song #7, “If Thou Be Near” by Bach. In both testing sessions, he recognized the name Bach on the sheet music and claimed that he “thinks” he has played the song before. As previously stated, both of his parents claim that he never played any of the target songs prior to Time 1. Therefore, we believe that his claim for recognizing this particular song is purely due to his recognition of the composer.
Musical performance
The Mann-Whitney U test was used to compare the performance on the target songs and the control songs at time 1 (i.e., before he had any practice playing the target songs). No significant differences (p>0.05) were found on any of the five measures (Figure 2). Additionally, there were no significant differences (Mann-Whitney U=27; p=0.954) on the level of difficulty between the target (median=4; mean rank=8.5) and the control (median=4.5; mean rank=8.6) songs (Table 2).
Figure 2. SZ’s performance on the Target and Control songs at Time 1 and Time 2.

The results are presented as median scores. The error bars represent the range between minimum and maximum scores. Time 1 corresponds to dark grey bars and Time 2 to the light grey bars. No significant differences were found between target and control songs at Time 1 on any of the measures. SZ’s performance improved significantly on the target songs from Time 1 to Time 2, as measured by Notes Awareness and Overall Sight-Reading Accuracy indices. His performance on the control songs did not change significantly from Time 1 to Time 2.
SZ demonstrated improvement from Time 1 to Time 2 on notes awareness (for 7/11 target songs) and overall sight-reading accuracy (for 6/11 target songs), and neither of these measures showed any decline over time for any of the target songs (see Table 2 for a song by song breakdown). Positive changes over time were also found on intonation (1/11), sound quality (3/11), and rhythmic awareness (6/11). For the control songs, positive changes over time were found on notes awareness (for 4/5 control songs), overall sight reading accuracy (2/5), intonation (1/5), sound quality (1/5), and rhythmic awareness (1/5).
The Wilcoxon test for paired samples was applied to compare the expert’s scoring of each song at time 1 and time 2. According to the professional musician’s evaluation, after three months of intense exposure to the music during biweekly orchestra practices, patient SZ demonstrated significant improvement on the performance of the target songs, as measured by notes awareness (median=7 at Time 1 and median=9 at Time 2; mean of the negative ranks=0; mean of the positive ranks=4; Z=−2.414, p=0.016, r=−0.51) and overall sight-reading accuracy (median=7 at Time 1 and median=8 at Time 2; mean of the negative ranks=0; mean of the positive ranks=3.5; Z=−2.214, p=0.027, r=−0.47;) (Figure 2 and Table 2). No significant improvements were found on the other measures (i.e., intonation, sound quality, and rhythm awareness).
The comparisons between time 1 and time 2 for the control songs did not reveal any significant changes. For three indices (intonation, sound quality, rhythmic awareness), his performance on the control songs was numerically lower at Time 2; this never occurred on the target songs. The Mann-Whitney U test was used to compare the level of difficulty of the songs that showed improvement versus those that did not. No significant difference (p>0.05) was found.
Discussion
Patient SZ showed significant improvement when learning a series of new unfamiliar songs over a three-month period of intensive training despite his complete inability to consciously remember having played any of the music. The learning was confined to measures tapping into perceptual-motor aspects of saxophone playing, including notes awareness and sight-reading accuracy. In essence, he demonstrated content specific sight-reading improvements such that his ability to read musical notations on sheet music and translate these notations into movements became more accurate for the practiced songs.
Different brain regions have been shown to play a role in the perceptual-motor aspects of music. For example, playing a musical instrument by sight-reading has been found to activate the superior parietal cortex, bilaterally, both in professional musicians (Sergent, Zuck, Terriah & MacDonald, 1992) and in musically-naive individuals after training (Stewart et al., 2003). The basal ganglia and the cerebellum have been found to be engaged in the performance of a memorized musical composition by blindfolded pianists (Parsons, Sergent, Hodges, & Fox, 2005). Human lesion studies have also implicated these brain regions in the acquisition of new perceptual and motor skills (e.g., Laforce & Doyon, 2001; Cavaco et al., 2011). High-resolution MRI images clearly indicate that the superior parietal cortex, the basal ganglia, and the cerebellum are not damaged in SZ, and thus, may be contributing to his improved musical performance on perceptual-motor aspects of learning.
While SZ demonstrated significant learning on perceptual-motor aspects of music, the effect was modest in size. The professional musician that scored his performance speculated that most of his students would have shown a much greater improvement (compared to SZ) if they had repeatedly practiced the material over a three month time period. However, the present study was not designed to ascertain whether the magnitude of SZ’s learning was within or below the “normal” range. The normality of learning, vis-à-vis whether a patient with severe anterograde amnesia is capable of learning to perform new music at a normal rate, is a completely separate issue from whether any new musical learning can take place in such a patient. The absence of a healthy “control” group narrows the scope of the discussion, but does not compromise the main finding — the contrast between SZ’s learning to play new music, and his inability to remember the music at a declarative level is clear and robust.
The assessment of SZ’s learning may have been altered due to the testing environment, which differed substantially from his practice environment with his orchestra. Since on both testing sessions SZ played the saxophone by himself, it is unclear whether his performance would be enhanced when playing with the full orchestra. Notably, the training of the target songs was accomplished in the context of orchestra practice. During this training, SZ received extra visual and auditory cues from the conductor, his mother, and the other musicians in the orchestra. These immediate external references may have facilitated better pitch correction and rhythmic awareness, and this is certainly something that can be tested in a future study. Non-declarative knowledge has been suggested to be essentially inflexible and non-relational, and the expression of this type of memory is potentiated when the conditions at the assessment mirror the original learning conditions (Cohen, Poldrack & Eichenbaum, 1997). Additionally, SZ’s training process did not avoid the occurrence of errors. Error elimination is known to be particularly problematic in amnesic patients (Baddeley & Wilson, 1994). In the absence of declarative (explicit) recollection of prior training experiences, an amnesic patient tends to make the same errors over and over. It is reasonable to speculate that a longer training period, individually tailored and based on an errorless approach, would have produced better learning results in SZ.
The piecemeal improvement in SZ’s musical memory is likely to reflect the complexity of cognitive processes necessary to learn a new musical piece. The acquisition, integration, and retrieval of both declarative and non-declarative knowledge are all part of the musical learning process. Healthy musicians benefit from the conscious recollection of prior exposure to a particular song. With repeated exposure, a normal musician tends not to read all the written information on a piece of sheet music, but rather, develops a “feel” for the song’s progression and over time develops a “muscle memory” for the song itself. This combination of declarative and procedural learning may contribute to more efficient eye-hand spans (i.e., the separation between eye position and hand position when sight-reading music; Furneaux & Land, 1999), and subsequently to better and smoother performances.
SZ did not show significant improvement on some of the indices, namely sound quality, intonation, and rhythmic awareness. The sound quality of a musician is a relatively stable non-declarative skill, i.e., it is less dependent on content specific training than all the other measures and significant changes are more likely to require extensive training. Intonation and rhythmic awareness are partially related to a musician’s ability to convey the emotional undertone or “prosody” of the song’s melody in such a manner that the timing and inflection of each note seamlessly merges with the subsequent note, creating a coherent musical piece that conveys a distinct “feeling.” When SZ’s music recordings were played to professional and amateur musicians, those listeners commented that the sound was somewhat “robotic” or “machine-like” in nature. SZ’s basic perception of music and his processing of emotions in musical stimuli were not explored. Likewise, we did not specifically measure whether SZ’s saxophone playing is generally “flat” with regard to emotion for all music that he plays. However, there are indications that he is able to convey at least some emotion while playing the saxophone. During his warm-up song, “Windy,” the sound was much more vibrant and filled with emotion. Likewise, during testing, all measures were above the floor (see Figure 2) suggesting that at least some aspects of emotion were present when he played the saxophone. Future studies examining the learning of new musical material in amnesic patients could consider using experimental designs with similar assessment and training conditions, multiple expert raters, and the inclusion of foil excerpts for the raters (i.e., clips played by different musicians interspersed with those played by the patient).
In summary, the ability to play a musical instrument represents a unique procedural skill that appears to be resilient to disruption of declarative memory. Previous studies have not answered definitively the question of whether amnesic musicians are capable of learning new music. The present study capitalized on a rare opportunity to address this issue by exploring the capacity to learn new songs in an amateur musician with severe non-progressive anterograde memory impairment. The patient’s performance, before and after three months of prolonged exposure and practice, highlighted the distinction between some preserved capacity to acquire non-declarative memories for new musical material and the complete inability to learn any declarative information about the songs. The magnitude of this new learning was relatively modest and appeared to be confined to the perceptual-motor aspects of playing new music.
Acknowledgments
We are greatly indebted to SZ and his family for their unwavering support and continued commitment to brain research. We also would like to thank SZ’s caregivers and his orchestra for allowing us to observe. Nicolau Pinto Coelho, Mikiko Kanemitsu, Gilberto Bernardes, and Fernando Ramos provided important musical expertise, Kenneth Manzel contributed with the neuropsychological evaluation, and Steven W. Anderson provided invaluable comments on earlier versions of this manuscript. This research was supported by NIH P50 NS19632 and the Kiwanis Foundation.
References
- Anderson SW, Rizzo M, Skaar N, Stierman L, Cavaco S, Dawson J, et al. Amnesia and driving. Journal of Clinical and Experimental Neuropsychology. 2007;29:1–12. doi: 10.1080/13803390590954182. [DOI] [PubMed] [Google Scholar]
- Baddeley A, Wilson BA. When implicit learning fails: amnesia and the problem of error elimination. Neuropsychologia. 1994;32:53–68. doi: 10.1016/0028-3932(94)90068-x. [DOI] [PubMed] [Google Scholar]
- Baird A, Samson S. Memory for music in Alzheimer’s disease: Unforgettable? Neuropsychological Review. 2009;19:85–101. doi: 10.1007/s11065-009-9085-2. [DOI] [PubMed] [Google Scholar]
- Baur B, Uttner I, Ilmberger J, Fesl G, Mai N. Music memory provides access to verbal knowledge in a patient with global amnesia. Neurocase. 2000;6:415–421. [Google Scholar]
- Beatty WW, Brumback RA, Vonsattel JP. Autopsy-proven Alzheimer disease in a patient with dementia who retained musical skill in life. Archives of Neurology. 1997;54:1448. doi: 10.1001/archneur.1997.00550240008002. [DOI] [PubMed] [Google Scholar]
- Beatty WW, Zavadil KD, Bailly RC, Rixen GJ, Zavadil LE, Farnham N, et al. Preserved musical skill in a severely demented patient. International Journal of Clinical Neuropsychology. 1988;10:158–64. [Google Scholar]
- Beatty WW, Winn P, Adams RL, Allen EW, Wilson DA, Prince JR, et al. Preserved cognitive skills in dementia of the Alzheimer type. Archives of Neurology. 1994;51:1040–6. doi: 10.1001/archneur.1994.00540220088018. [DOI] [PubMed] [Google Scholar]
- Beatty WW, Rogers CL, Rogers RL, English S, Testa JA, Orbelo DM, et al. Piano playing in Alzheimer’s disease: Longitudinal study of a single case. Neurocase. 1999;5:459–69. [Google Scholar]
- Cavaco S, Anderson SW, Allen JS, Castro-Caldas A, Damasio H. The scope of preserved procedural memory in amnesia. Brain. 2004;127:1853–1867. doi: 10.1093/brain/awh208. [DOI] [PubMed] [Google Scholar]
- Cavaco S, Anderson SW, Correia M, Magalhães M, Pereira C, Tuna A, et al. Task-specific contribution of the human striatum to perceptual-motor skill learning. Journal of Clinical and Experimental Neuropsychology. 2011;33:51–62. doi: 10.1080/13803395.2010.493144. [DOI] [PubMed] [Google Scholar]
- Cohen NJ, Squire LR. Preserved learning and retention of pattern analyzing skill in amnesia: dissociation of knowing how and knowing that. Science. 1980;210:207–209. doi: 10.1126/science.7414331. [DOI] [PubMed] [Google Scholar]
- Cohen NJ, Poldrack RA, Eichenbaum H. Memory for items and memory for relations in the procedural/declarative memory framework. Memory. 1997;5:131–178. doi: 10.1080/741941149. [DOI] [PubMed] [Google Scholar]
- Cowles A, Beatty WW, Nixon SJ, Lutz LJ, Paulk J, Paulk K, et al. Musical Skill in Dementia: A Violinist Presumed to Have Alzheimer’s Disease Learns to Play a New Song. Neurocase. 2003;9:493–503. doi: 10.1076/neur.9.6.493.29378. [DOI] [PubMed] [Google Scholar]
- Crystal H, Grober E, Masur D. Preservation of musical memory in Alzheimer’s disease. Journal of Neurology, Neurosurgery, and Psychiatry. 1989;52:1415–1416. doi: 10.1136/jnnp.52.12.1415. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fornazzari L, Castle T, Nadkarni S, Ambrose M, Miranda D, Apanasiewicz, et al. Preservation of episodic musical memory in a pianist with Alzheimer disease. Neurology. 2006;66:610–611. doi: 10.1212/01.WNL.0000198242.13411.FB. [DOI] [PubMed] [Google Scholar]
- Furneaux S, Land MF. The effects of skill on the eye-hand span during musical sight-reading. Proceedings of the Royal Society of London Series B. 1999;266:2435–2440. doi: 10.1098/rspb.1999.0943. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gabrieli JDE, Corkin S, Mickel SF, Growdon JH. Intact acquisition and long-term retention of mirror-tracing skill in Alzheimer’s disease and in global amnesia. Behavioral Neuroscience. 1993;107:899–910. doi: 10.1037//0735-7044.107.6.899. [DOI] [PubMed] [Google Scholar]
- Hay JF, Moscovitch M, Levine B. Dissociating habit and recollection: evidence from Parkinson’s disease, amnesia and focal lesion patients. Neuropsychologia. 2002;40:1324–1334. doi: 10.1016/s0028-3932(01)00214-7. [DOI] [PubMed] [Google Scholar]
- Laforce R, Doyon J. Distinct contribution of the striatum and cerebellum to motor learning. Brain & Cognition. 2001;45:189–211. doi: 10.1006/brcg.2000.1237. [DOI] [PubMed] [Google Scholar]
- Levitin DJ. This is your brain on music. New York: Plume; 2007. [Google Scholar]
- Milner B. Colloques Internationaux du Centre National de la Recherche Scientifique. Physiologie de L’Hippocampe, colloques internationaux. 107. Paris: Centre National de la Recherche Scientifique; 1962. Les troubles de la mémoire accompagnant des lésions hippocampiques bilatérales; pp. 257–272. [Google Scholar]
- Parsons LM, Sergent J, Hodges DA, Fox PT. The brain basis of piano performance. Neuropsychologia. 2005;43:199–215. doi: 10.1016/j.neuropsychologia.2004.11.007. [DOI] [PubMed] [Google Scholar]
- Sacks O. Musicophilia: Tales of music and the brain. New York: Random House; 2008. [Google Scholar]
- Schacter DL. Amnesia observed: remembering and forgetting in a natural environment. Journal of Abnormal Psychology. 1983;92:236–242. doi: 10.1037//0021-843x.92.2.236. [DOI] [PubMed] [Google Scholar]
- Sergent J, Zuck E, Terriah S, MacDonald B. Distributed neural network underlying musical sight-reading and keyboard performance. Science. 1992;257:106–109. doi: 10.1126/science.1621084. [DOI] [PubMed] [Google Scholar]
- Squire LR. Memory systems of the brain: a brief and current perspective. Neurobiology of Learning and Memory. 2004;82:171–177. doi: 10.1016/j.nlm.2004.06.005. [DOI] [PubMed] [Google Scholar]
- Stewart L, Henson R, Kampe K, Walsh V, Turner R, Frith U. Brain changes after learning to read and play music. Neuroimage. 2003;20:71–83. doi: 10.1016/s1053-8119(03)00248-9. [DOI] [PubMed] [Google Scholar]
- Tranel D. The Iowa-Benton school of neuropsychological assessment. In: Grant I, Adams KM, editors. Neuropsychological assessment of neuropsychiatric disorders. 3. New York: Oxford University Press; 2009. pp. 66–83. [Google Scholar]
- Tranel D, Damasio AR, Damasio H, Brandt JP. Sensorimotor skill learning in amnesia: Additional evidence for the neural basis of nondeclarative memory. Learning and Memory. 1994;1:165–179. [PubMed] [Google Scholar]
- Wilson BA, Baddeley AD, Kapur N. Dense amnesia in a professional musician following herpes simplex virus encephalitis. Journal of Clinical and Experimental Neuropsychology. 1995;17:668–81. doi: 10.1080/01688639508405157. [DOI] [PubMed] [Google Scholar]