

Abstract
Granuloma annulare has been associated with systemic disease including diabetes mellitus. We report a case of a 62-year-old Japanese woman with generalized erythematous granuloma annulare who showed remission after substantial improvement in hyperlipidemia following a strict lipid-lowering diet. The lesion appeared in the lower abdomen one year before current presentation and subsequently spread to other areas of the trunk despite treatment with topical steroid and oral epinastine hydrochloride. Physical examination showed a well-demarcated erythematous plaque measuring 10 cm in diameter with fine scales on the left abdomen, and slightly indurated pinkish plaques of up to 5 cm in diameter on the right side of the abdomen and axillae. Clinical laboratory tests showed mild glucose intolerance (HbA1c 6.2%), mild liver dysfunction (AST: 86 IU/L, ALT: 76 IU/l), slight hypercholesterolemia (total cholesterol: 235 mg/dl), and severe hyperlipidemia (triglyceride: 962 mg/ml). Histopathological examination of the lesions showed homogenization of collagen fibers and granulomatous infiltrates between fibers in the upper and middle dermis. A diagnosis of generalized erythematous granuloma annulare was established based on the clinical and histopathological findings, especially with the distribution on more than one anatomic site. A lipid-lowering diet for three months resulted in major improvement of hyperlipidemia and remission of the skin lesions.
A review of generalized erythematous granuloma annulare in the Japanese literature indicated a well-known association of granuloma annulare with diabetes mellitus, however, the relation with hyperlipidemia was described only recently. This case suggests a possible relationship between granuloma annulare and hyperlipidemia, with possible improvement of granuloma annulare with a lipid-lowering diet.
Keywords: generalized erythematous granuloma annulare, glucose intolerance, hyperlipidemia
Introduction
Granuloma annulare manifests various skin lesions, such as erythematous, plaque, papular, nodular and ulcerative forms, in addition to the typical annular lesion [1]. We report a case of generalized erythematous granuloma annulare with a remission after lipid-lowering diet.
Case presentation
A 62-year-old Japanese woman presented with itchy erythematous skin lesions on the left lower abdomen, the right side of the chest and both axillae. The family history was negative for similar skin lesions. The past history was negative apart from mild liver dysfunction on routine blood tests. The skin lesions were first noticed one year earlier, and subsequently spread to the chest and back in spite of treatment with topical steroid and oral epinastine hydrochloride. Physical examination showed a well-demarcated erythema of approximately 10 cm in diameter with limited fine scales on the left lower abdomen (Figure 1A). Some of the macules on the chest and axillae measured up to 5 cm and were palpable pinkish erythemata surrounded by small red papules at the periphery (Figure 1B, C).
Figure 1.



Clinical photographs. Note the presence of large erythematous plaque measuring 10 × 10 cm in diameter, with limited scaling and well-demarcated border on the left lower abdomen, surrounded by (A) several small erythemata. (B) Erythemata up to 5 cm in diameter were seen on the right abdomen. (C) Erythemata grouped into small red papules were seen in the axillae. [Copyright: ©2014 Watanabe et al.]
Laboratory tests showed HbA1c 6.2% (normal: 4.3–5.8), aspartate aminotransferase (AST) 76 IU/l (normal: 5–40), alanine aminotransferase (ALT) 258 IU/l (normal: 5–35), total cholesterol (T-chol) 235 mg/dl (normal: 110–210), and triglyceride 962 mg/dl (normal: 55–129) (Table 1).
TABLE 1.
Results of laboratory tests before and after lipid-lowering diet.
| Initial visit |
At the end of lipid-lowering diet for
|
||
|---|---|---|---|
| 1 month | 3 months | ||
| aspartate aminotransferase (IU/l) | 86 | 33 | 33 |
| alanine aminotransferase (IU/l) | 76 | 26 | 29 |
| γ-glutamyl transpeptidase (IU/l) | 267 | 252 | 243 |
| Total cholesterol (mg/dl) | 235 | 281 | 294 |
| Triglyceride (mg/dl) | 962 | 331 | 366 |
| HbA1C | 6.2% | 5.8% | 5.8% |
Histopathological examination of biopsy material obtained from the left and right abdomen and stained with hematoxylin and eosin (H&E) showed similar changes, including homogenized but poorly stained collagen fibers and granulomatous infiltration of histiocytes, lymphocytes and giant cells between the fibers in the upper and middle dermis. Histiocytes were also scattered among the collagen fibers (Figure 2A). Elastica-van-Gieson staining showed diminished fractured elastic fibers, but no phagocytosis of giant cells. Alcian-blue staining confirmed the presence of mucin deposition between collage fibers (Figure 2B). Immunostaining for CD68 demonstrated many histiocytes and Langhans giant cells (Figure 2C). A diagnosis of a generalized erythematous papular type of granuloma annulare was established based on the clinical and histopathological findings together with the distribution pattern of the lesion (on more than one anatomic site).
Figure 2.
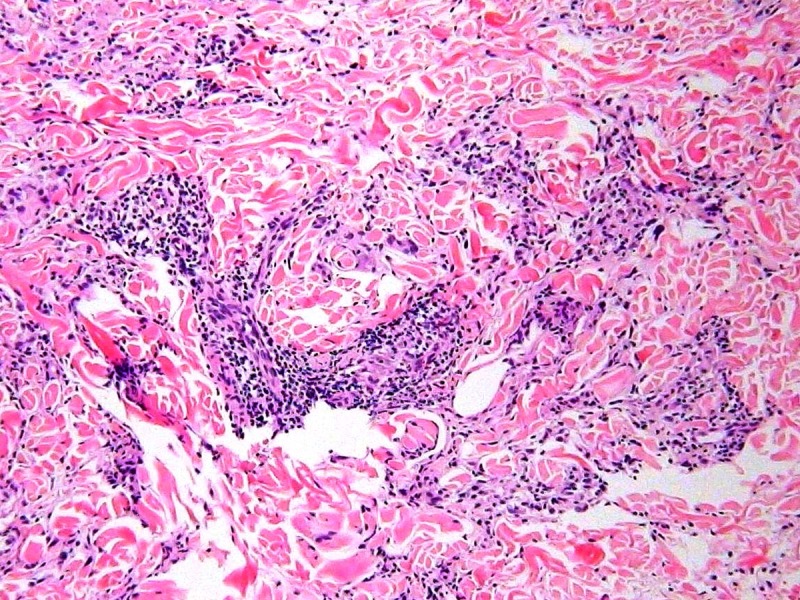
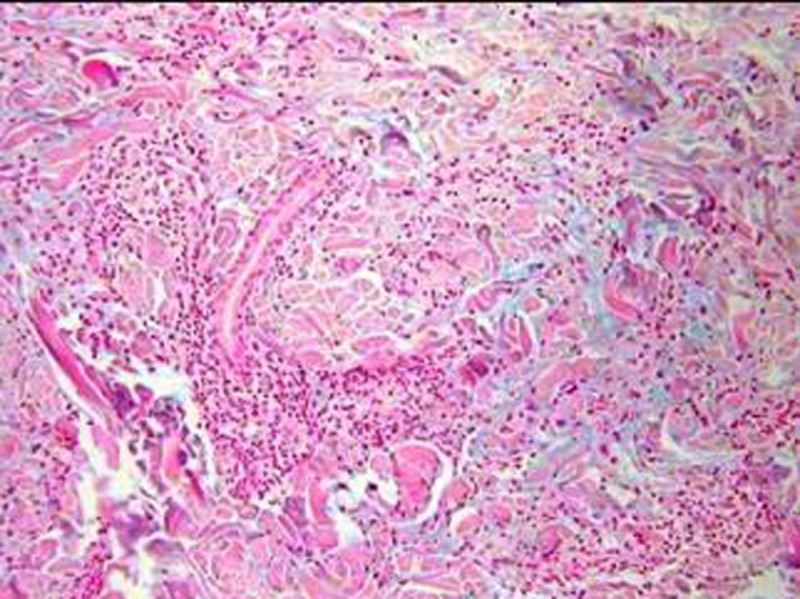
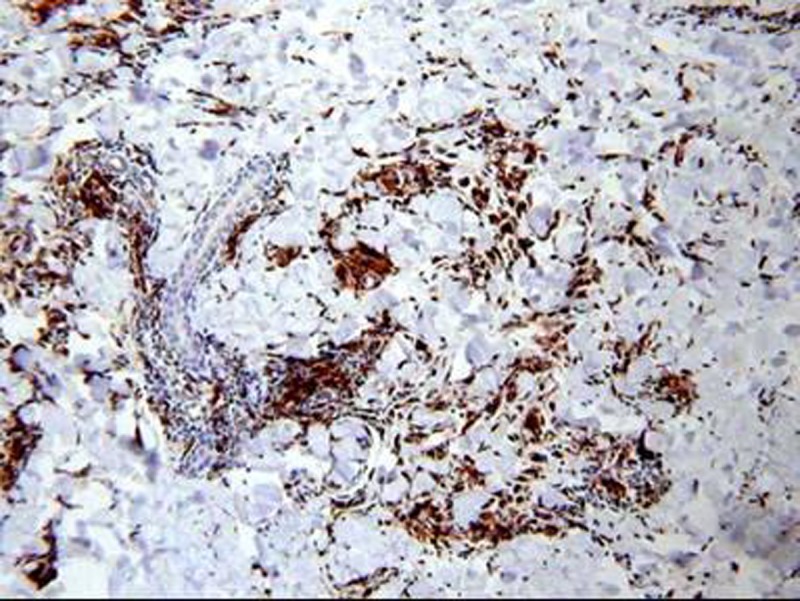
Histopathological findings. (A) A high power view of hematoxylineosin stained biopsy section showing infiltrates forming a granuloma composed mainly of histiocytes and giant cells intermingled with lymphocytes. (B) Alcian-blue staining confirmed mucin deposition between collagen fibers. (C) Immunostaining for CD68 demonstrated many histiocytes and giant cells. [Copyright: ©2014 Watanabe et al.]
Treatment with topical diflorasone diacetate ointment was started. Consultation with the Department of Internal Medicine regarding glucose intolerance, liver dysfunction and hyperlipidemia was followed by a lipid-lowering diet for a period of three months. Strict adherence to the latter resulted in marked improvement of hyperlipidemia. One month later, the skin lesions showed clear remission, together with improvement in laboratory data (Table 1).
Discussion
Granuloma annulare often shows generalized distribution of the skin manifestations that cover more than one anatomic site [2]. The generalized form of granuloma annulare also tends to exhibit various types of skin lesions [3]. The present case demonstrated generalized skin lesions of erythematous type together with papular type. The frequency of the erythematous type is reported to be approximately 16%, and 14 Japanese cases, including the present case, have been reported since 1966 [4–15]. The age distribution of the reported Japanese cases ranged from 50 to 70, with no gender difference, with a distribution mainly on the extremities (Table 2).
TABLE 2.
Summary of Japanese cases with generalized erythematous granuloma annulare reported in the literature between 1966 and 2013.
| Age | 49 – 92 (median 59.5) |
| Gender | males 6, females 8 |
| Location | trunk 7, arms 12, legs 11 |
| Complications | diabetes mellitus 6, rheumatoid arthritis, 1, malignancy 1 |
| Treatments | topical steroid 9, none 1 |
| Prognosis | remission 5, partial remission 3, stable 3 |
The association of granuloma annulare with diabetes mellitus is well documented, together with other less frequent complications of autoimmune disorders and internal malignancy [14]. The association of granuloma annulare with dyslipidemia was recently reported [16]. In the study by Wu et al, dyslipidemia was more common in generalized than localized/disseminated disease, and the annular lesion morphology was associated with hypercholesterolemia. Our review of the Japanese literature on generalized erythematous granuloma annulare showed that 6 out of 14 had glucose intolerance, 1 had rheumatoid arthritis, and 1 had internal malignancy.
The distinct features of the present case were the following: 1) the skin lesions were mainly noted on the trunk, 2) high serum triglyceride level (962 mg/dl), 3) mild glucose intolerance, and 4) liver dysfunction. In this regard, there has been little information in the literature on hyperlipidemia in erythematous granuloma annulare. Moreover, granuloma annulare often spontaneously resolves after a biopsy especially in the erythematous type [15]. The clinical improvement noted in the present case could have been triggered by the biopsy, topical application of the steroid ointment and/or beneficial changes in both glucose intolerance and hyperlipidemia following lipid-lowering diet. However, one cannot dismiss the possible involvement of hyperlipidemia in the activity of granuloma annulare. Therefore, the presented case suggests the possible relationship between granuloma annulare and hyperlipidemia, with possible improvement of granuloma annulare by lipid-lowering diet.
With the increased concern on adult lifestyle-related diseases in recent years, physicians need to pay attention to granuloma annulare and dermatologists should be aware of the relation between granuloma annulare and various internal diseases. We should also be aware of generalized lesions, which can be easily overlooked as non-specific skin lesions, and conduct skin biopsy to establish a definitive diagnosis.
This case was presented at the 74th Tokyo Division Meeting of the Japanese Dermatological Association.
Footnotes
Funding: None.
Competing interests: The authors have no conflicts of interest to disclose.
References
- 1.Katsuoka K, et al. Granuloma annulare in a patient with diabetes mellitus. [Article in Japanese] Hifubyo Shinryo. 1989;11:35. [Google Scholar]
- 2.Izumi H, et al. Two cases of non-annular type generalized granuloma annulare. [Article in Japanese] Rinsho Hifuka. 1996;9:719–21. [Google Scholar]
- 3.Dicken CH, Carrington SG, Winkelmann RK. Generalized granuloma annulare. Arch Dermatol. 1969;99(5):556–63. [PubMed] [Google Scholar]
- 4.Nagai R, et al. Granuloma annulare. [Article in Japanese] Hifu Rinsho. 1966;8:544. [Google Scholar]
- 5.Miyake K, et al. A case of generalized granuloma annulare. [Article in Japanese] Rinsho Hifuka. 1969;23:911. [Google Scholar]
- 6.Sato Y, et al. Generalized granuloma annulare. [Article in Japanese] Rinsho Hifuka. 1970;24:353. [Google Scholar]
- 7.Maumi F. Atypical granuloma annulare. [Article in Japanese] Rinsho Hifuka. 1969;23:1019. [Google Scholar]
- 8.Shimada Y. Four cases of granuloma annulare. [Article in Japanese] Rinsho Hifuka. 1974;28:685. [Google Scholar]
- 9.Ogino A, Tamaki E. Atypical granuloma annulare. Transition from erythema to multiple type. Dermatologica. 1978;156(2):97. [PubMed] [Google Scholar]
- 10.Araki T, et al. Generalized granuloma annulare with atypical clinical features. [Article in Japanese] Hifu Rinsho. 1981;23:1789. [Google Scholar]
- 11.Okusa Y, et al. Erythematous granuloma annulare. [Article in Japanese] Hifu Rinsho. 1986;28:359. [Google Scholar]
- 12.Tsutsui K, et al. A case of atypical granuloma annulare. [Article in Japanese] Hifu Rinsho. 1989;31:855. [Google Scholar]
- 13.Ebihara T, et al. A case of erythematous granuloma annulare. [Article in Japanese] Jpn J Dermatol. 1991;101:900. [Google Scholar]
- 14.Nakama T, et al. A case of generalized form of atypical granuloma annulare. [Article in Japanese] Rinsho Hifuka. 1998;52:337. [Google Scholar]
- 15.Konohana I, et al. A case of erythematosus granuloma annulare. [Article in Japanese] Rinsho Hifuka. 1993;47:479. [Google Scholar]
- 16.Wu W, Robinson-Bostom L, Kokkotou E, Jung HY, Kroumpouzos G. Dyslipidemia in granuloma annulare: a case-control study. Arch Dermatol. 2012;148(1):1131–6. doi: 10.1001/archdermatol.2012.1381. [DOI] [PubMed] [Google Scholar]