

Abstract
Objectives
The aims of this study were to develop a smartphone application to encourage breast self-examination (BSE), and to evaluate the effects of this application in terms of modifying BSE behavior.
Methods
A smartphone application, based on the Android OS, was developed with functions including a BSE date alarm, a reminder to encourage mother and daughter to practice BSE together, record keeping, and educational content with video clips. Females aged 19 and over were enrolled to evaluate the effectiveness of the application. Two series of questionnaires were carried out (before and after use of the application) by e-mail, telephone, and face-to-face interviews between July and September 2012.
Results
Forty-five subjects were enrolled in the study (age 29.5-5.9 years). Of the participants, only 28 (62.2%) had ever practiced BSE and only one of these (2.2%) was carried out at the appropriate time, based on the results of the baseline survey. After using the application, the number of participants practicing BSE increased from 28 to 32 (62.2% to 71.1%, p = 0.503). In subgroup analysis (age < 30 years), the number of participants using BSE increased from 8 to 18 (36.4% to 81.8%, p = 0.002), and the number of those using it at the appropriate time rose from 1 to 15 (2.2% to 33.3%, p < 0.001).
Conclusions
The use of the developed smartphone application increased BSE in females younger than 30 years. To confirm the long-term benefits of the mobile application, additional studies must be carried out.
Keywords: Breast Cancer, Breast Self-Examination, Cellular Phone
I. Introduction
Breast cancer is one of the most common cancers in females worldwide, and is the leading cause of cancer-related deaths among females in developing countries [1]. In Korea, breast cancer is the second most common cancer in females [2]. In 2008, the incidence of breast cancer was 18.7 per 100,000 people, and it has since increased at an average rate of 6.6% per year [2]. Breast cancer is prevalent in females aged 15-34 in Korea, and as such, those affected are on average 10-15 years younger than in the United States [3-5].
Breast cancer has a relatively good prognosis, with an overall 5-year survival rate of 89.5%, and 98.2% in patients with stage 0. However, the 5-year overall survival rate of females with stage IV cancer is only 30.5% [6], highlighting the importance of detecting and treating breast cancer at an early stage. Females who practice breast self-examination (BSE) are usually diagnosed at an earlier stage than those who do not [7]. Mammograms and BSE are the most widely used screening methods for the early detection of breast cancer. In Korea, the National Cancer Center recommends monthly BSE for females older than 30 years and a mammogram every 2 years for females over 40 years of age [8].
In the Korean National Cancer Screening Survey of 1,255 females conducted in 2007, 88.0% were aware of BSE. However, the percentage of females performing regular or irregular BSE was very low (13.2% and 16.1%, respectively) [9], which is lower than in other Asian countries [10-12]. Appropriate interventions are therefore needed to encourage BSE. There have been previous attempts to achieve this, such as oral contraceptive packaging in the United States, and a short message service (SMS) in India, which have been used to encourage BSE, and both trials demonstrated positive results [13,14].
In recent years, the use of smartphones has been increasing rapidly. For example, in Korea, smartphone use accounted for 47.7% of the total mobile phone usage in 2012 [15], and the average time spent on a smartphone by users was 2.4 hours per day [15]. Due to the widespread use of smartphones, many mobile health applications for the management of chronic diseases, such as hypertension and diabetes, have been developed. As a result, more than 40,000 mobile health applications are now available on multiple platforms, and several studies of these have been conducted [16-19]. However, most of these mobile phone studies have focused on the management of chronic disease, for example, to help with weight loss or lifestyle changes [20,21].
Although the early detection of breast cancer is critical, no studies have attempted to facilitate BSE using a smartphone application. The aims of this study were therefore to develop a smartphone application promoting BSE, and to evaluate its effectiveness.
II. Methods
1. Mobile Application Development
The first step in this study was to develop a prototype mobile application. Based on analysis of the market share of mobile phone operating systems (OS) in Korea, Android OS is the market leader, and so an Android-based smartphone application was developed. The application had a reminder function for the optimal day for BSE, which was calculated based on the menstrual cycle. After the initial development, feedback was received from the patients enrolled in the study. Based on this feedback, a second application was developed, introducing educational video clips demonstrating how to accurately carry out BSE. A multi-disciplinary panel of experts, composed of a medical informatics professor, a radiation oncologist, a breast cancer surgeon, and nurses, reviewed this second application, and their comments and feedback were used to complete the final application (Figure 1).
Figure 1.

Mobile application development. The application was developed in three stages, based on feedback from the public and an expert panel. The experts comprised a medical informatics professor, a radiation oncologist, a breast cancer surgeon, and nurses.
The developed Android OS-compatible application had several functions to facilitate BSE, including a "reminder" of the optimal day to perform it, motivational tools including the participant's mother, record keeping, and educational contents supported by the National Cancer Information Center (Figure 2). The purpose of the "reminder" function is to calculate the most effective day to carry out BSE. While setting up the application, users are prompted to input details of their menstrual cycle. If the menstrual cycle is regular, the last day of the last menstruation period and the menstrual cycle are entered using the touch screen. The optimal day for BSE (7 days after the onset of menses) is then calculated and stored in the smartphone (Figure 3). If subjects have irregular menstrual cycles or are undergoing the menopause, they can specify their own optimal BSE day each month. Once the recommended day for BSE has been entered into the application, a series of reminders is triggered on the optimal day, as well as 1 day before and 1 day after (Figure 4).
Figure 2.

Overview of smart application. (A) A "reminder" of the optimal day to perform breast self-examination (BSE), (B) record keeping, (C) BSE video clip, and (D) breast cancer prevention information.
Figure 3.
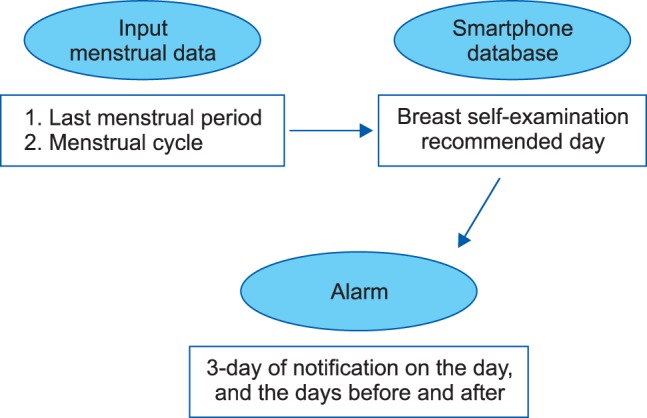
Breast self-examination (BSE) reminders. The recommended day for BSE was generated using data about the last menstrual period and menstrual cycle and was stored in the smartphone. When the recommended day approached, a series of three reminders was triggered.
Figure 4.

Breast self-examination (BSE) reminder procedure. (A) Input user menstrual cycle, (B) calculate recommended day for BSE, and (C) alarm when the recommended day approaches.
An additional function is to encourage the user to involve her mother so that they can perform BSE together. When the application reminds the user of her recommended BSE day, the "mother motivation function" allows the user to call her mother using a notification function. If the user touches the notification bar, the application moves to the telephone call menu. Through use of this feature, a middle-aged mother who is in the menopause is encouraged to do BSE with her daughter (Figure 5A). This feature is linked to the record-keeping function, where a user can register her BSE performance status. A participant can also choose to update whether her mother performed BSE after the mother motivational notification. All information pertaining to BSE is then stored in the smartphone, and the user can confirm when she has practiced BSE, and whether she did so with her mother (Figure 5B).
Figure 5.

The 'mother motivation function'. (A) An alert saying "call mother" is generated. If the user clicks on the alarm notification bar, the application asks her to call her mother. (B) An option for the user to state that she is "with mom" is then generated, and the application records whether breast self-examination was performed with her mother.
Additionally, the application contains educational tools, since previous studies have demonstrated that educational content increases both knowledge of breast cancer and the practice of BSE [3]. The application therefore contained video clips outlining how to perform BSE, as well as information on breast cancer, such as breast cancer risk factors, prevention methods, and high-risk groups.
2. Inclusion Criteria
The study protocol was approved by the Institutional Review Board of the Ajou University Hospital in 2012. Participants were recruited via an advertisement to Ajou University students, associated workers, and local residents. Inclusion criteria required participants to own a smartphone, be aged 19 years and over, and have no history of breast cancer. The study was performed between July and September 2012.
3. Evaluation of the Effectiveness of the Application
The required sample size (n = 47) was calculated based on a statistical significance level of 0.05 using McNemar test, and the BSE practice rate in Korea (30%) [9], and worldwide (70%), according to previous studies [13,14].
Two series of surveys were conducted by e-mail, telephone, and face-to-face interviews, before and after the study period. Before use of the application, the age, marital status, level of education, family history of cancer, perception of BSE, and frequency of BSE use were determined (Appendix A). After the initial survey, participants were introduced to our mobile application and asked to download and use it. The developed application could be downloaded through the Google Play application store. A second survey about BSE status was performed two months later with patients who had downloaded and used the application (Appendix B).
4. Data Analysis
The characteristics of the subjects and their major variables were analyzed in terms of both percentage and frequency. BSE practice before and after use of the mobile application was then calculated using McNemar test. For analysis, two-tailed tests were used, and p < 0.05 was considered to indicate statistical significance. The collected data were analyzed using the MedCalc statistical software package (MedCalc, Mariakerke, Belgium; http://www.medcalc.be/).
III. Results
Fifty-nine subjects were initially enrolled in the study; however, 14 participants were eliminated from the analysis since they either failed to complete a questionnaire, could not be contacted, or did not reinstall the application after changing smartphones and upgrading the operating system. Overall, data from 45 participants were analyzed.
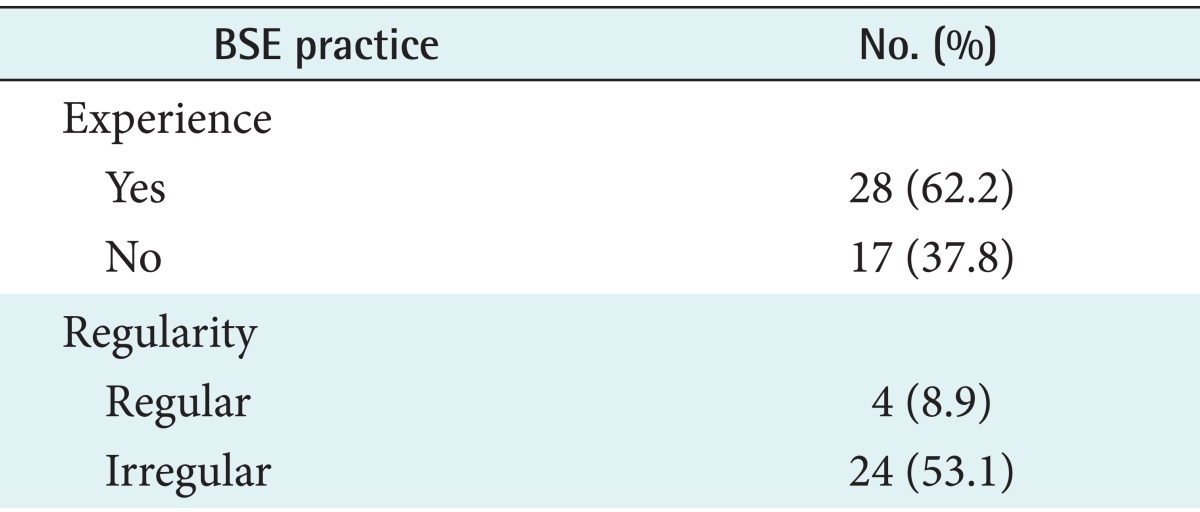
The baseline survey revealed that the average age of participants was 29.5 ± 5.9 years and that 60% (n = 27) of subjects were unmarried. Sixty-eight percent of participants were employed, while most (88.9%) had graduated from college or university. The prevalence of a family history of breast cancer was 4% (Table 1). Of the 45 enrolled subjects, 28 (62%) had previously performed BSE. Before using the application, only four subjects (8.9%) practiced BSE regularly, and only one participant (2.2%) knew the optimal time to perform BSE (Table 2).
Table 1.
General demographic characteristics of the participants (n = 45)
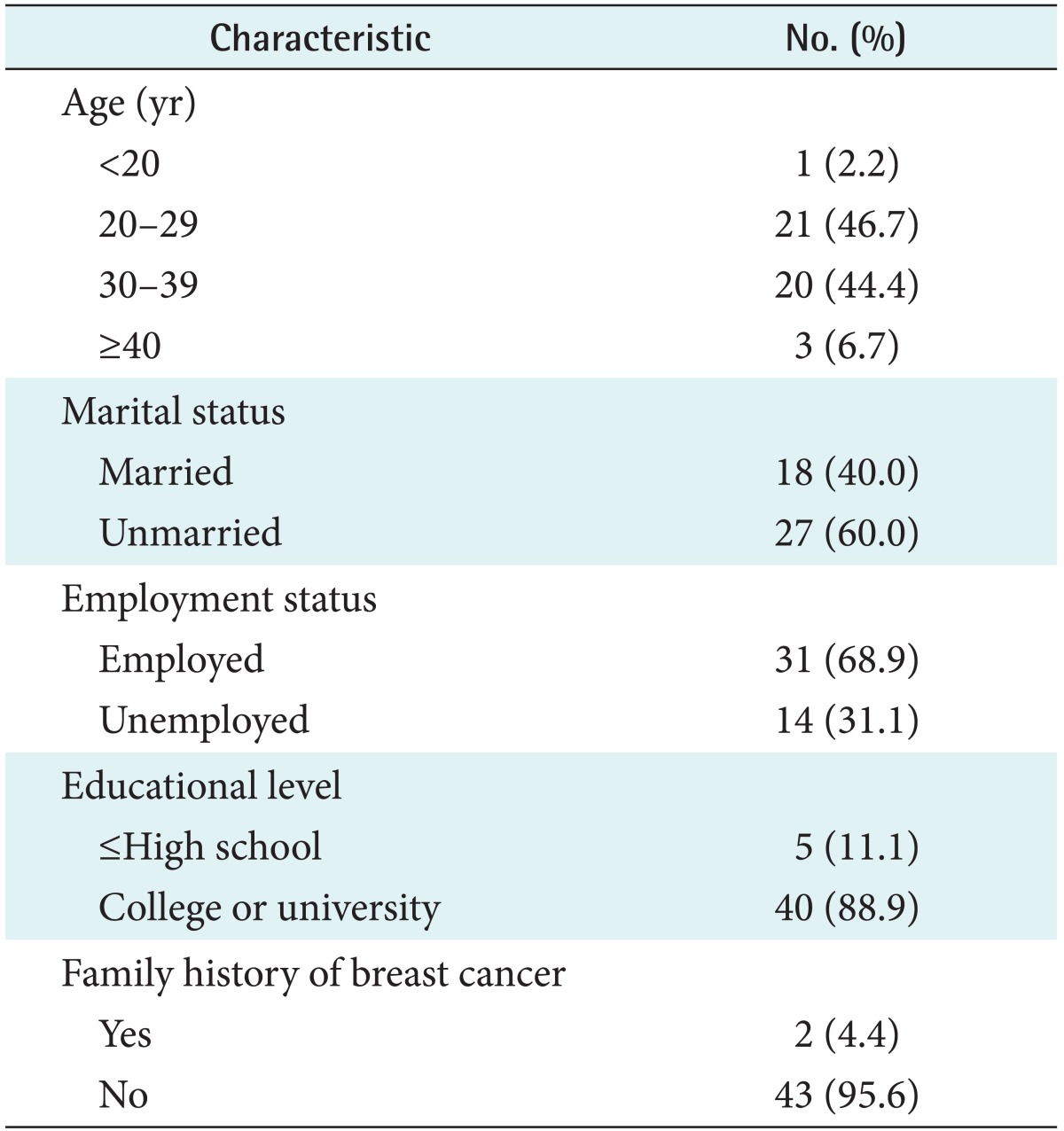
Table 2.
Baseline breast self-examination (BSE) practice before use of the mobile application (n = 45)
aSeven days after the start of menstruation.
Differences in the practice of BSE before and after use of the smartphone application were assessed. The number of subjects performing BSE increased from 28 to 32 (62.2% to 71.1%), although the difference was not statistically significant (p = 0.503). Subgroup analysis was then carried out based on the age, marital status, profession, and level of education of the participants. In the subgroup of users under 30 years of age, the rate of BSE practice increased from 36.4% to 81.8% after using the application (p = 0.002). In contrast, the rate of BSE practice in subjects over 30 years of age decreased from 87% to 60.9%. Other factors, such as marital status, profession, and education level, did not appear to influence BSE practice. We developed a function to induce BSE at the optimal time (7 days after menstruation onset). Overall, the practice of BSE at the optimal time increased from 2.2% to 33.3% (p < 0.001) (Table 3). The developed application has a function to encourage BSE through the daughter's stimulation. Actually, six participants (13.3%) performed BSE with their mothers using the "mother motivation function". The purposes of BSE are to detect the presence of an abnormal mass that requires additional evaluation and to motivate patients to go to the hospital. After practicing BSE using the smartphone application, four subjects (8.9%) detected an abnormal mass, which led to a hospital visit.
Table 3.
Comparison of breast self-examination (BSE) at baseline and after 2 months of using the application (n = 45)
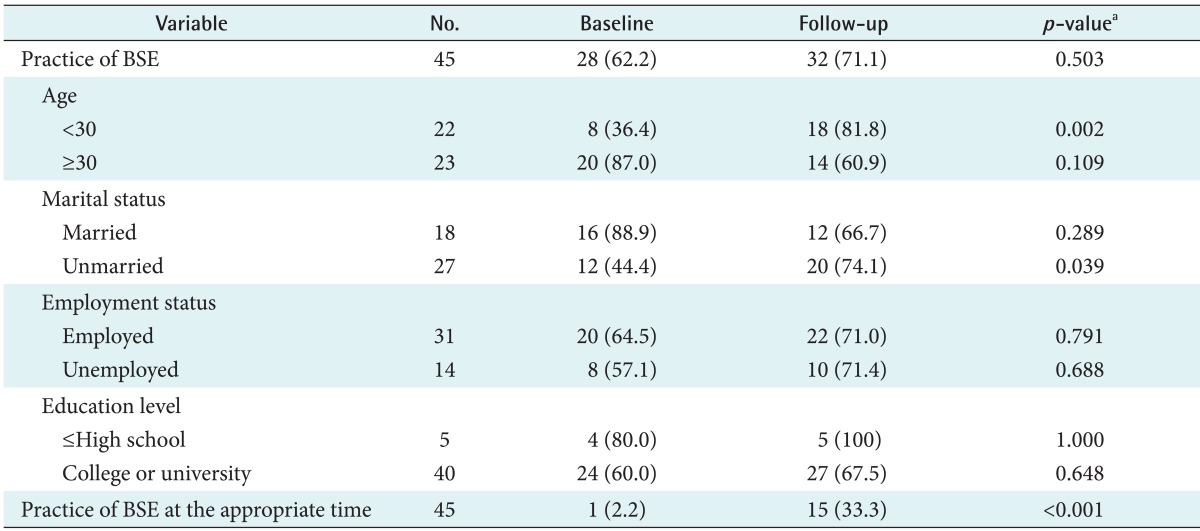
Values are presented as number (%).
aMcNemar test.
IV. Discussion
The results demonstrated that the use of the proposed smartphone application could increase BSE practice. In the baseline survey, most subjects were aware of BSE (86.7%); however, the number of participants who had ever practiced BSE was moderate (62.2%), and few of those (9%) performed BSE regularly. Interestingly, the rate of regular BSE is significantly lower than has been observed in other Asian countries, which ranges from 67.0% to 84.4% [10,11,22]. After using our mobile application, the overall BSE practice rate increased from 62.2% to 71.1%, and the practice of BSE at the appropriate time significantly increased from 2.2% to 33.3%.
There have been several previous attempts to encourage BSE. In the United States, BSE prompts on oral contraceptive packaging were encouraged, and after 3 months of intervention, the rate of appropriately timed BSE increased from 24.5% to 68.1% [13]. Although the application resulted in increased BSE, it required the cooperation of pharmaceutical companies, which cannot easily be controlled. In India, a study using a SMS was performed in 2008, leading to an increase in the practice of BSE from 40.0% to 72.6% after six months [14].
Unlike previous studies, we used a smartphone application to improve BSE practice because this approach has several advantages. Today, people spend significant amounts of time using smartphones throughout the day, and mobile applications can be freely downloaded from the Google Play store. Due to their availability, accessibility, and low cost, smartphone applications are likely to be increasingly used for the improvement of health and disease screening. In addition, smartphones can provide multimedia content, including images, text, and video clips, all of which can help users to improve their health.
The overall frequency of BSE did not increase significantly after smartphone application use. However, subgroup analysis showed that the effectiveness of this technology varies by age group. The practice of BSE increased significantly, but only in females less than 30 years of age. This may be due to differences in smartphone usage since younger people tend to be more accustomed to using applications, such as social networks and mobile messaging services, compared with older participants [15]. It is possible that alternative, less complicated, technological approaches (such as SMS or e-mail alerts) may be more effective in older females. In previous studies about smoking cessation, SMS as a health behavior intervention was used, and the smoking quit rate was significantly increased (Table 3) [21].
However, this study has novel approaches to induce BSE and prevent breast cancer. First, we adopted the optimal timing of intervention based on user's menstrual cycle data. Because breast tissue softens and an abnormal mass can be more easily distinguished from normal breast tissue 7 days after the onset of menses, this user-tailored method could improve the effectiveness of BSE. Actually, during the study, we used repeated reminders to notify users of their optimal BSE date, which significantly increased the proportion of females carrying out BSE at the appropriate time from 2.2% to 33.3% (p < 0.001). However, this is still lower than the results of a previous study carried out in the United States [13]. This suggests that a multimodality method that is more sophisticated than simple notifications may be required to further increase the frequency of BSE. There have been previous attempts to modify health-related behavior using smartphone technology. For example, with human immunodeficiency virus-infected patients, collaborative methods to improve drug adherence, including videos about the effects of the drugs and personalized feedback from the physician, increased the overall adherence to the medication regimen [23]. In a study on weight loss, a sociable robot-based application interacted with the user, and was successful in modifying behavior and achieving weight loss [24]. Our study could therefore be further improved by including additionally mixed interventions, such as physicians' feedback.
Second, we used the social support of family to induce BSE. The prevalence of breast cancer is high in females aged 50-60 years [25]. However, many females in this age group do not know how to accurately perform BSE and live apart from their children. Also, the smartphone penetration rate for older people is increasing. The use of smartphones has sharply increased from 4.6% (2011) to 46.8% (2012) for those in their fifties, and from 9.5% (2011) to 35.9% (2012) for those in their sixties [26]. Therefore, we included a function encouraging participants and their mothers to practice BSE together. Although the application reminded users to call their mothers at the appropriate time so they could practice BSE together, only 6 of the 45 participants (13.3%) actually did BSE with their mothers during the study period. However, we believe that using daughters' recommendation to motivate their mothers could be an effective method to promote BSE in menopausal females. Social support could be an effective intervention in mobile health.
Third, we focused on the possibility of a mobile screening test for breast cancer. Mammography is a screening method for breast cancer in Korea, but dense breast tissue, which could decrease the accuracy of mammogram results is common in Korean women. Therefore, the use of ultrasonography for the detection of breast cancer is used to compensate for the lower accuracy of mammography. Because ultrasonography is not covered by the national health insurance, an additional charge is incurred. On the contrary, BSE improves the accuracy of mammography in breast cancer screening without the burden of increased expenses [27]. During daily practice, a palpable mass is the most common sign used by physicians to identify potential breast tumors. Participants could learn and apply BSE through the smartphone application containing a video clip. Four of the participants (8.9%) found an abnormal mass after BSE, and went to the hospital to have the mass assessed. This suggests that use of the smartphone application could facilitate the early detection of an abnormal breast mass, and potentially cancer.
It must, however, be noted that our study had several limitations. Most of our participants (88.9%) were highly educated and had graduated from university. This is significant, as the practice of BSE is significantly correlated with education [12,28]. Additional studies including participants with a wider range of education levels should therefore be performed. Another limitation was the short study period (2 months) since BSE should be performed regularly over a long period. However, to evaluate the long-term effects of the smartphone application, a central server capable of data collection and analysis may be required. To determine the long-term effect, the researchers need financial support to build a real-time data collection system and legal support regarding privacy to accumulate smartphone user's data. Also, it is necessary to reduce loss to follow-up. Unlike other interventions, the smartphone application could be removed by a user unintentionally through OS upgrade or a change of smartphone. Therefore, regular feedback is required to confirm use of the application.
In conclusion, our findings demonstrate the potential benefit of using a smartphone application to enhancing BSE practice using reminders, a "mother motivation" function, record keeping, and educational content. These results may facilitate the development of more sophisticated mobile screening methods for breast cancer.
Acknowledgments
This work was supported by the National Research Foundation of Korea grant funded by the Korea government (No. 2010-0028631 to R. W. Park). The study was also supported by grants of the Korea Health Technology R&D Project of the Ministry of Health and Welfare, Korea (A112022 to R. W. Park).
Appendix A
Questionnaire for demographic characteristics of the participants and their breast self-examination status before using the application (translated to English from original Korean version)

Appendix B
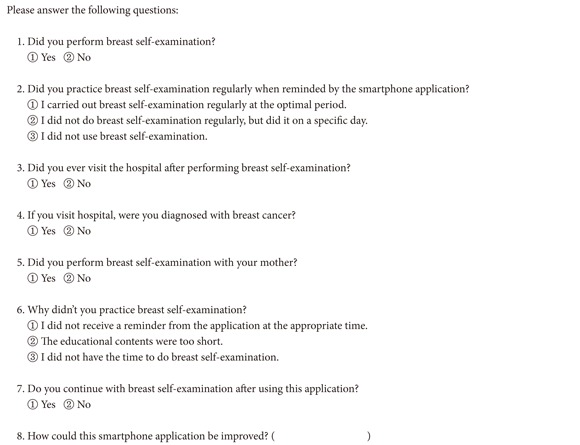
Questionnaire on breast self-examination after using the application (translated to English from original Korean version)
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61(2):69–90. doi: 10.3322/caac.20107. [DOI] [PubMed] [Google Scholar]
- 2.Jung KW, Park S, Kong HJ, Won YJ, Lee JY, Seo HG, et al. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2009. Cancer Res Treat. 2012;44(1):11–24. doi: 10.4143/crt.2012.44.1.11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Shin KR, Park HJ, Kim M. Practice of breast self-examination and knowledge of breast cancer among female university students in Korea. Nurs Health Sci. 2012;14(3):292–297. doi: 10.1111/j.1442-2018.2012.00696.x. [DOI] [PubMed] [Google Scholar]
- 4.Leong SP, Shen ZZ, Liu TJ, Agarwal G, Tajima T, Paik NS, et al. Is breast cancer the same disease in Asian and Western countries? World J Surg. 2010;34(10):2308–2324. doi: 10.1007/s00268-010-0683-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Son BH, Ahn SH, Lee MH, Park SK, Kim SW Korean Breast Cancer Society. Hereditary breast cancer in Korea: a review of the literature. J Breast Cancer. 2008;11(1):1–9. [Google Scholar]
- 6.Korea Breast Cancer Society. Breast cancer facts & figures [Internet] Seoul, Korea: Breast Cancer Society; c2008. [cited at 2008 Oct 1]. Available from: http://www.kbcs.or.kr/journal/file/2006_2008_Breast_Cancer_Facts_and_Figures_updated.pdf. [Google Scholar]
- 7.Koibuchi Y, Iino Y, Takei H, Maemura M, Horiguchi J, Yokoe T, et al. The effect of mass screening by physical examination combined with regular breast self-examination on clinical stage and course of Japanese women with breast cancer. Oncol Rep. 1998;5(1):151–155. doi: 10.3892/or.5.1.151. [DOI] [PubMed] [Google Scholar]
- 8.Oh DK, Shim JI, Han M, Kim Y, Lee HY, Jun JK, et al. Breast cancer screening in Korean women: report of the national cancer screening program in 2008. J Breast Cancer. 2010;13(3):299–304. [Google Scholar]
- 9.Yoo BN, Choi KS, Jung KW, Jun JK. Awareness and practice of breast self-examination among Korean women: results from a nationwide survey. Asian Pac J Cancer Prev. 2012;13(1):123–125. doi: 10.7314/apjcp.2012.13.1.123. [DOI] [PubMed] [Google Scholar]
- 10.Loh SY, Chew SL. Awareness and practice of breast self-examination among Malaysian women with breast cancer. Asian Pac J Cancer Prev. 2011;12(1):199–202. [PubMed] [Google Scholar]
- 11.Rosmawati NH. Knowledge, attitudes and practice of breast self-examination among women in a suburban area in Terengganu, Malaysia. Asian Pac J Cancer Prev. 2010;11(6):1503–1508. [PubMed] [Google Scholar]
- 12.Yavari P, Pourhoseingholi MA. Socioeconomic factors association with knowledge and practice of breast self-examination among Iranian women. Asian Pac J Cancer Prev. 2007;8(4):618–622. [PubMed] [Google Scholar]
- 13.Ferris DG, Golden NH, Petry LJ, Litaker MS, Nackenson M, Woodward LD. Effectiveness of breast self-examination prompts on oral contraceptive packaging. J Fam Pract. 1996;42(1):43–48. [PubMed] [Google Scholar]
- 14.Khokhar A. Short text messages (SMS) as a reminder system for making working women from Delhi Breast Aware. Asian Pac J Cancer Prev. 2009;10(2):319–322. [PubMed] [Google Scholar]
- 15.Korea Internet and Security Agency. Survey on the wireless Internet usage [Internet] Seoul, Korea: Korea Internet and Security Agency; c2012. [cited at 2012 Feb 28]. Available from: http://isis.kisa.or.kr/board/index.jsp?pageId=040000&bbsId=7&itemId=795&pageIndex=1. [Google Scholar]
- 16.Chomutare T, Fernandez-Luque L, Arsand E, Hartvigsen G. Features of mobile diabetes applications: review of the literature and analysis of current applications compared against evidence-based guidelines. J Med Internet Res. 2011;13(3):e65. doi: 10.2196/jmir.1874. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Holtz B, Lauckner C. Diabetes management via mobile phones: a systematic review. Telemed J E Health. 2012;18(3):175–184. doi: 10.1089/tmj.2011.0119. [DOI] [PubMed] [Google Scholar]
- 18.Lim S, Kang SM, Shin H, Lee HJ, Yoon JW, Yu SH, et al. Improved glycemic control without hypoglycemia in elderly diabetic patients using the ubiquitous healthcare service, a new medical information system. Diabetes Care. 2011;34(2):308–313. doi: 10.2337/dc10-1447. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Liang X, Wang Q, Yang X, Cao J, Chen J, Mo X, et al. Effect of mobile phone intervention for diabetes on glycaemic control: a meta-analysis. Diabet Med. 2011;28(4):455–463. doi: 10.1111/j.1464-5491.2010.03180.x. [DOI] [PubMed] [Google Scholar]
- 20.Song TM, Ryu S, Lee SH. u-Health service for managing chronic disease: a case study on managing metabolic syndrome in a health center in South Korea. Healthc Inform Res. 2011;17(4):260–266. doi: 10.4258/hir.2011.17.4.260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Free C, Knight R, Robertson S, Whittaker R, Edwards P, Zhou W, et al. Smoking cessation support delivered via mobile phone text messaging (txt2stop): a single-blind, randomised trial. Lancet. 2011;378(9785):49–55. doi: 10.1016/S0140-6736(11)60701-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Sreedharan J, Muttappallymyalil J, Venkatramana M, Thomas M. Breast self-examination: knowledge and practice among nurses in United Arab Emirates. Asian Pac J Cancer Prev. 2010;11(3):651–654. [PubMed] [Google Scholar]
- 23.Moore JO, Hardy H, Skolnik PR, Moss FH. A collaborative awareness system for chronic disease medication adherence applied to HIV infection. Conf Proc IEEE Eng Med Biol Soc. 2011;2011:1523–1527. doi: 10.1109/IEMBS.2011.6090367. [DOI] [PubMed] [Google Scholar]
- 24.Kidd CD, Breazeal C. Robots at home: understanding long-term human-robot interaction; Proceedings of the IEEE/RSJ International Conference on Intelligent Robots and Systems; 2008 Sep 22-26; Nice, France. pp. 3230–3235. [Google Scholar]
- 25.Héry C, Ferlay J, Boniol M, Autier P. Changes in breast cancer incidence and mortality in middle-aged and elderly women in 28 countries with Caucasian majority populations. Ann Oncol. 2008;19(5):1009–1018. doi: 10.1093/annonc/mdm593. [DOI] [PubMed] [Google Scholar]
- 26.Korea Information Society Development Institute. Smart device usage and lifestyle of retirement age [Internet] Gwacheon, Korea: Korea Information Society Development Institute; c2013. [cited 2013 Mar 25]. Available from: http://www.kisdi.re.kr/kisdi/fp/kr/publication/selectResearch.do?cmd=fpSelectResearch&sMenuType=2&controlNoSer=43&controlNo=13124&langdiv=1. [Google Scholar]
- 27.Knutson D, Steiner E. Screening for breast cancer: current recommendations and future directions. Am Fam Physician. 2007;75(11):1660–1666. [PubMed] [Google Scholar]
- 28.Haji-Mahmoodi M, Montazeri A, Jarvandi S, Ebrahimi M, Haghighat S, Harirchi I. Breast self-examination: knowledge, attitudes, and practices among female health care workers in Tehran, Iran. Breast J. 2002;8(4):222–225. doi: 10.1046/j.1524-4741.2002.08406.x. [DOI] [PubMed] [Google Scholar]