

Abstract
Objectives
The Web-based integrated public healthcare information system (PHIS) of Korea was planned and developed from 2005 to 2010, and it is being used in 3,501 regional health organizations. This paper introduces and discusses development and performance of the system.
Methods
We reviewed and examined documents about the development process and performance of the newly integrated PHIS. The resources we analyzed the national plan for public healthcare, information strategy for PHIS, usage and performance reports of the system.
Results
The integrated PHIS included 19 functional business areas, 47 detailed health programs, and 48 inter-organizational tasks. The new PHIS improved the efficiency and effectiveness of the business process and inter-organizational business, and enhanced user satisfaction. Economic benefits were obtained from five categories: labor, health education and monitoring, clinical information management, administration and civil service, and system maintenance. The system was certified by a patent from the Korean Intellectual Property Office and accredited as an ISO 9001. It was also reviewed and received preliminary comments about its originality, advancement, and business applicability from the Patent Cooperation Treaty. It has been found to enhance the quality of policy decision-making about regional healthcare at the self-governing local government level.
Conclusions
PHIS, a Web-based integrated system, has contributed to the improvement of regional healthcare services of Korea. However, when it comes to an appropriate evolution, the needs and changing environments of community-level healthcare service and IT infrastructure should be analyzed properly in advance.
Keywords: Public Health Informatics, Systems Integration, Evaluation, District-Level
I. Introduction
We are confronting a new healthcare environment that is rapidly evolving into an aging society. In 2010, the elderly population (over 65 years old) constituted 11.0% of the overall population in South Korea. It is estimated that this percentage will double to 24.3% by 2030 [1]. Moreover, the share of the gross domestic product (GDP) spent on health expenditures has continuously increased in South Korea from 4.5% in 2000 to 7.1% in 2010 [2]. Non-communicable diseases are increasing in relation to extended life expectancy. Moreover, the need for healthcare management is increasing because of the advancement of economic and educational standards [3].
Citizens pursue the maintenance and improvement of their health rather than being in need of illness treatment for survival. This trend is spreading these days as economic standards improve and information flows. Therefore, instead of focusing on the prevention of infectious diseases or getting treatment for diseases, citizens are focusing more on health management, health enhancement, and rehabilitation. With respect to this trend, the public healthcare service should more strongly emphasize the maintenance and enhancement of citizen's health by providing health information and guidance to healthcare utilities. Hence, the national health policy needs to reorganize its system to ensure lifelong health management and the wellness of the population.
Information and communication technologies (ICT) are evolving to create a new information society based on cloud computing, mobile, and smart technologies. These ICT trends will innovate and enable more smart and convenient healthcare services. Therefore, it is thought that ICT evolution will promote the advancement of a healthcare delivery system that will provide easily accessible and intelligent healthcare service throughout people's lives [4].
The Ministry of Health and Welfare (MOHW) of South Korea proactively decided to accept and apply the emerging ICT to the public health information system (PHIS). The information strategy for the PHIS was prepared based on the national master plan of the health and welfare information plan in 1994. The PHIS was revised more than four times between 1995 and 1999, and network-based PHIS for health organization (public health center, public health sub-center, and primary healthcare post) were provided. However, the information strategy for PHIS limited its ability to fulfill the needed contents, innovate business process, and standardize information [5]. There are also other problems of the PHIS, namely, inconvenience, insufficient information management, inaccessibility of medical service information, insufficient information sharing between public health and medical services, low quality of regional statistics on healthcare services, and insufficient application of regional public health policies [5,6].
The roles of PHIS are to generate, analyze, and disseminate data about public health decision-making [7]. MOHW established the information strategy for the PHIS to solve existing problems of the PHIS by adopting newly emerging ICT [6]. The purpose was to innovate a health care information infrastructure that can provide ICT-based services corresponding to the needs of regional healthcare services, such as the enhancement of the health management abilities of regional citizens, reinforcement of integration with external organization and advancement of the nation's health policies, and increase in the business efficiency of public health organizations.
In this paper, we introduce and discuss the developmental process and performance of the new and integrated PHIS of Korea.
II. Case Description
This study reviewed documents about the development process and operation of the PHIS, such as strategic healthcare plans, information strategy, reports and documents on development and operation, and organization.
We reviewed the functional area of the PHIS as well as the operation and maintenance of the system. The quality and performance of the PHIS were evaluated by survey and performance reports. Measures to evaluate the system were derived from previous research on the evaluation of information systems [8-11]. Lastly, we carried out a cost-benefit analysis of the PHIS.
1. History of PHIS
The MOHW of South Korea started to develop the PHIS based on the national master plan of information for health in 1994. The PHIS was revised more than four times between 1995 and 1999, and it supported the advancement of information processing and workflow in health organizations, such as public health centers, public health sub-centers, and primary healthcare posts.
However, national healthcare information systems were not established effectively or systematically, and the quality of contents and standardization of information were not reasonable either [9]. In particular, various problems regarding the system for public and primary healthcare service at the community level still remain, namely, inconvenience and insufficient information management, inaccessibility of medical service information from the organization, insufficient information sharing between health programs and primary medical services, low quality of statistics on regional healthcare, and insufficient practices of regional health policies [5,6]. The development of newly integrated PHIS, which would contribute to solving the problems of the existing systems, was enabled with the advancement of ICT.
2. Information Strategy for Current PHIS
The information strategy to enhance the PHIS was established in 2005, based on the strategic plan of the national healthcare system and by considering the environmental changes of management and ICT [6]. Directions were established to innovate PHIS as an integrated and advanced system based on recent ICT and to provide reasonable and timely information services to public healthcare services. The expected contributions of the new systems were the enhancement of the health management ability of citizens, reinforcement of integration with external related organizations, the advancement of new national health policies, and improvement regarding the efficiency of public health organizations.
The vision of PHIS, according to the national public healthcare plan, was to provide a high-quality healthcare service that is convenient and efficient to use for citizens anywhere through an electronic health information system. Two goals were defined by which this vision could be accomplished, providing a lifelong health management system for citizens, and strengthening the health industry through ICT.
The PHIS has the following six strategic objectives:
Enhancing consumer-orientation,
Enhancing citizen's health self-management capability,
Providing reasonable health service through ICT,
Active sharing of health information,
Stable ICT infrastructure,
Effective and efficient operation and management of ICT.
The information strategy of the PHIS was established on the basis of strategic plans of the public healthcare delivery system. The vision of the PHIS was defined as the "PHIS based on information technology" to integrate public health organizations and other related organizations, such as health insurance corporations. Specific objectives were set on the basis of policies, group and management, and information technology.
ICT strategies of public healthcare were set into three categories: policy, management, and ICT. Policy-focused strategies are to ensure the safety of healthcare services, improvement in the quality of public healthcare service, improvement of public healthcare services, and provision of basic resources for appropriate public health development. Management-focused strategies are innovation of business process and working practice, efficient information service, ensured security and confidentiality of systems and information, and provision of a collaboration system among institutions. ICT-focused strategies aim at the creation of a stabilized system of combined and linked technologies, analysis of big data and resources, standardized information and technology management and result of an adoption of newly and reliable ICT (Figure 1).
Figure 1.

Information strategy of public healthcare of Korea: vision, goals, objectives and strategies. PHIS: public health information system, ICT: information and communication technology.
3. System Development and Implementation
On the basis of the information strategy, the PHIS was developed progressively from 2006 to 2010. In the first stage, a standardized and Web-based public healthcare information system was built from 2006 to 2007 [12]. Dissemination of the PHIS to public health organizations was done continuously in the second stage [13]. In the third stage, a contingency recovery center was built to provide a foundation based on the operation of the stable information system [14]. In the fourth stage, in December 2011, these measures were expanded and made applicable to all the public health organizations nationwide. Since then, the Korea Health and Welfare Information Service (KHWIS), the agency to manage and support to the PHIS established in January 2010, has implemented the advanced functions of the PHIS, strengthened the information security system, and conducted continuous renewal procedures and maintenance processes (Figure 2).
Figure 2.

Development process of public health information system (PHIS).
4. PHIS: Web-Based Integrated Information Systems for Public Health
The PHIS has been developed as a standardized integrated information system that includes all businesses of public health organizations, such as those of public health centers, public health sub-centers, public health and medical centers, and primary healthcare posts. Moreover, a public health portal has been developed to provide electronic government services to citizens who need information regarding public health services and health management.
Details of the PHIS are given below. The public health portal was intended to provide guidance about public health affairs and public health businesses, health information, and reservations for public health organizations to regional citizens who utilize the public health agency. Further, it had the goal of providing one-stop civil services through websites regarding services such as the issue of proof documents or viewing of the medical history of registered people. The public healthcare information system for public health administration and businesses was developed after redesigning of business processes and tasks.
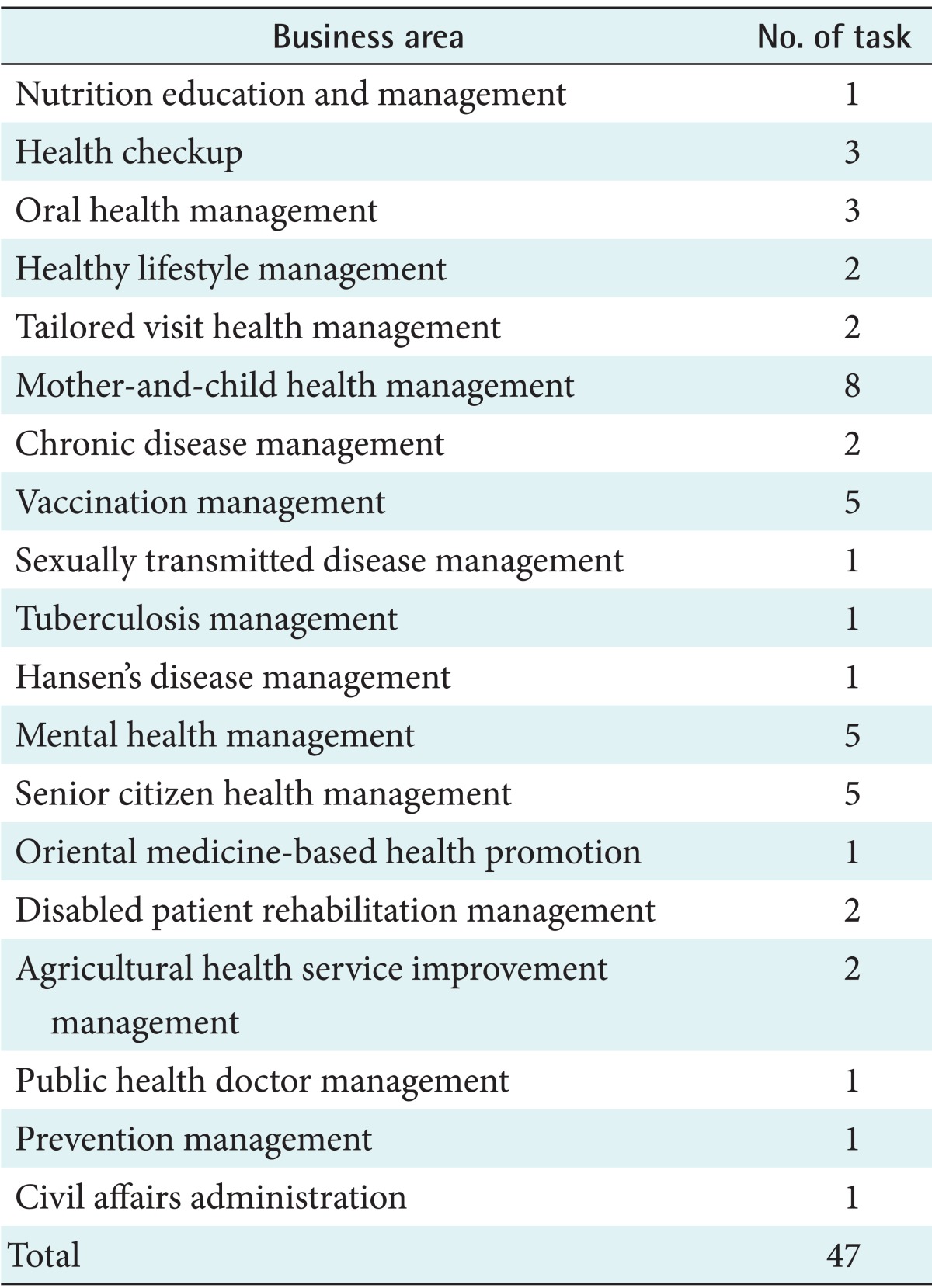
By the end of 2011, 47 tasks out of 19 public health businesses were implemented through the PHIS. As a result, seamless exchanges of data and integration were accomplished for tasks (public health businesses, administration tasks, and medical care services) that were conducted within public health organizations (Table 1).
Table 1.
Tasks of each business area of public health information system
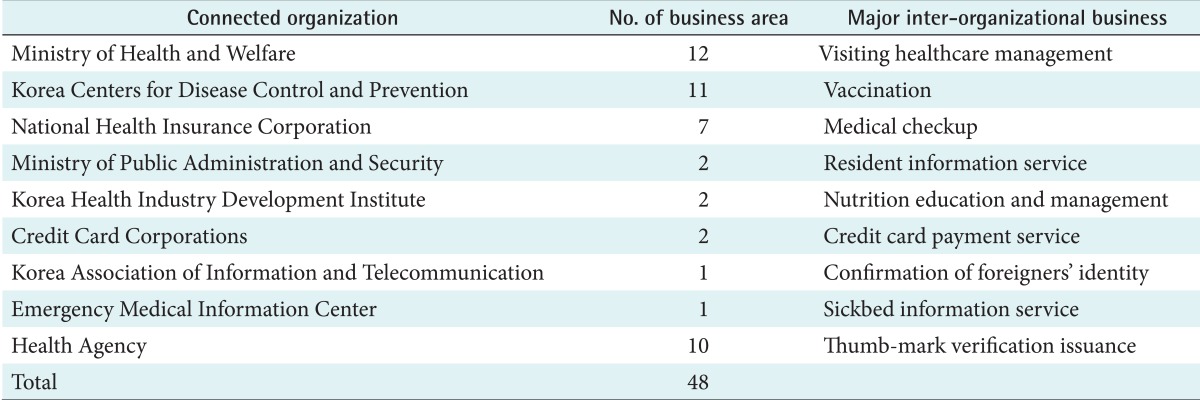
In addition, it enabled efficient cooperation on 48 interorganizational tasks by 9 related organizations: the Korean Centers for Disease Control and Prevention, National Health Insurance Corporation, Health Insurance Review & Assessment Service, Korean National Tuberculosis Association, Ministry of Public Administration and Security, National Cancer Center, Korea Health Industry Development Institute, Emergency Medical Information Center, and Korea Association of Information and Telecommunication [9] (Table 2).
Table 2.
Number of inter-organizational business area of public health information system
Standardized Electronic Medical Records (EMRs) have been applied in information systems for medical care and support for treatment. EMRs have been adopted by and managed in the public health organizations where health or medical care services are provided. Medical records and clinical testing results can be sent to other public healthcare organization if patients consent. This can guarantee the continuity of public health or medical treatment services and reduce overlapping inspections or checkups. Standardized EMRs also create databases extracted from raw data regarding health administration, health businesses, and healthcare services stored in the PHIS, which are essential to the program evaluation and policy making. Selected database resources are required in business evaluation and policy making through raw data that were collected through task performance, such as health administration, health businesses, and healthcare services stored in the PHIS. User-oriented analytical tools, installed within the system, enable the timely and reasonable analysis and mining of information. For example, multi-dimensional analysis can provide suitable information for lifelong health management to individuals.
A disaster recovery system was added during the second stage of system development, and it ensured the continuity of the system. The system would be activated in case of an unexpected emergency situation in the system, such as temporary system error, calamity, or natural disaster [14] (Figure 3).
Figure 3.

Conceptual configuration of public health information system (PHIS). KCDC: Korea Centers for Disease Control and Prevention, NCC: National Cancer Center, NHIC: National Health Insurance Corporation, HIRA: Health Insurance Review & Assessment Service, KNTA: Korean National Tuberculosis Association, MOPAS: Ministry of Public Administration and Security, CRM: customer relationship management, KMS: knowledge management system, PACS: picture archiving and communications system, DW: data warehouse, EMR: Electronic Medical Record.
5. Operation and Maintenance Organization of PHIS
Public healthcare organizations, located in rural or urban counties, were set as targets for implementation of the PHIS. There are 16 hospital-like public health and medical centers, and 238 public health centers that are responsible for public healthcare services to citizens at the county level. To make primary healthcare service more accessible, there are 1,346 public health sub-centers in townships and 1,901 primary healthcare posts in underserved villages [15].
KHWIS, as the professional IT management of the PHIS, manages the big data and system of the PHIS. The organization manages and analyzes healthcare data accumulated in the integrated PHIS of those health and medical organizations. It also operates and supports the right usage of the system in professional ways.
A call center within KHWIS is responsible for user support and maintenance of the PHIS. To collect users' requests and establish a supportive system, a call center (165 counsel agents) has been in operation since 2008, and inquiries and comments about the PHIS are processed through personal visits as well as telephone and online counseling. Moreover, the updated user manual of the PHIS is distributed annually to support and enhance usability.
We evaluated user satisfaction and the quality of service of the call center in December 2010. A 5-point Likert scale was used to evaluate the operation of the PHIS call center. The average satisfaction level with counseling agents' kindness was 4.14. The correct guidance of counseling agents was 4.15. Moreover, overall satisfaction with the call center was 3.99, and satisfaction with connectivity was 3.64 [9] (Table 3).
Table 3.
Service quality of call center for public health information system

Values are presented as number (%).
6. Usage and Quality of PHIS
According to the surveys conducted in December 2012, all of the 3,501 public health organizations adopted and implemented the PHIS: 238 public health centers, 16 public health medical centers, 1,346 public health sub-centers, and 1,901 primary healthcare posts. The number of business representatives using the PHIS in 2011 was 29,201, and the total number of accesses to the system was 46,620,671 cases (an average of 154,886 cases per day). EMR of the PHIS, including dental and herbal treatment services, increased from 377,381 cases in 2008 to 1,410,179 cases in 2012 (Figure 4).
Figure 4.
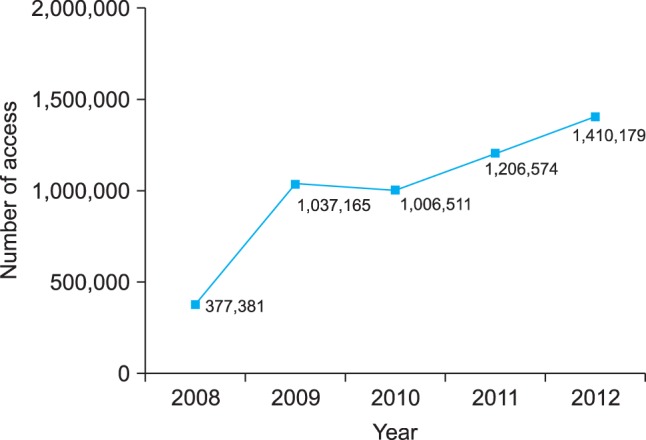
Usage trends of Electronic Medical Records of public health information system (2008-2012).
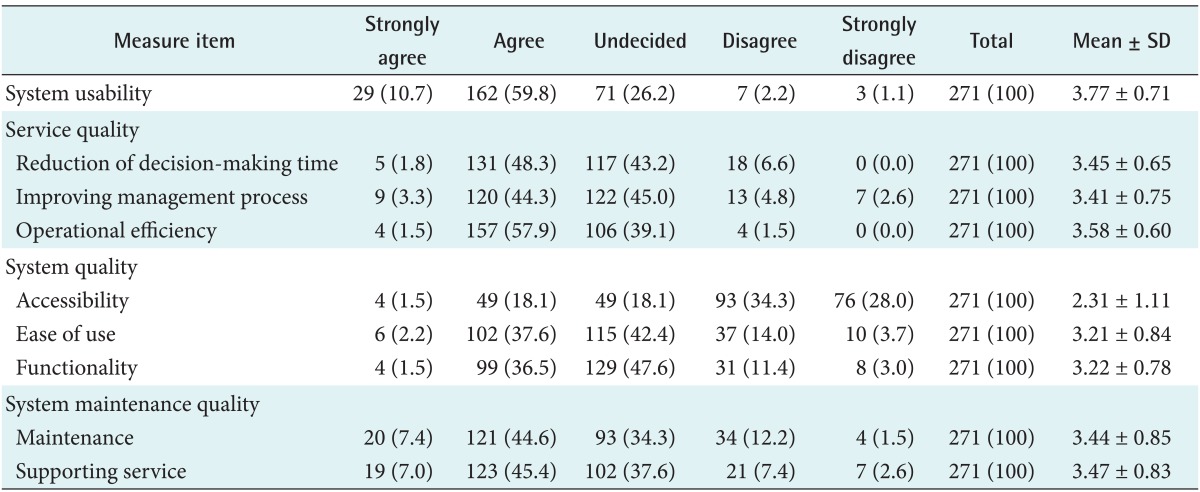
A survey was carried out to evaluate the quality of the PHIS in 2010, and data was collected from 271 users [16]. The survey collected data regarding four quality factors of information systems by a 5-point Likert scale: usefulness, system quality, service quality, and maintenance quality [8-11]. Regarding the usability of the PHIS, there were more responses expressing satisfaction (70.0%) than dissatisfaction (3.3%).
The service quality of the PHIS was evaluated in terms of three factors: time reduction of decision-making, improvement of business process, and operation efficiency. All factors revealed more positive responses than negative responses. In terms of time reduction of decision-making, 50.1% of respondents gave positive responses, but 6.6% responded negatively. As for improvement of business process, 47.6% gave positive responses, but 7.4% responded negatively. Operation efficiency also was evaluated positively, 59.4% gave positive answers, but only 1.5% responded negatively.
The system quality of the PHIS was evaluated in terms of three factors: accessibility, ease of use, and functionality. For system accessibility, 62.3% gave negative responses and 19.6% answered positively. However, ease of use and functionality of the system were evaluated more positively than accessibility. Ease of use and functionality obtained 39.8% and 38.0% of positive responses, and 17.7% and 14.4% negative responses, respectively.
The quality of system management was measured in terms of the technical maintenance and user support of the system. It was also evaluated positively. Regarding the technical maintenance of the system, 52.0% gave positive responses, and 13.7% responded negatively. For user support, 52.4% gave positive responses and 10.0% responded negatively (Table 4).
Table 4.
User evaluation of quality of public health information system
The intellectual and business quality of the PHIS was demonstrated by certification. The PHIS was certified by a patent from the Korean Intellectual Property Office, and accredited as ISO 9001 in 2011. It also received preliminary review comments about its originality, advancement, and business applicability from the Patent Cooperation Treaty in 2012.
7. Cost-Benefit Analysis
We analyzed the cost-benefit of the PHIS by using costs and measurable benefits from 2006 to 2012. The cost-benefit ratio was 2.34. The economic benefits of the PHIS were US$109,216, and the total costs were US$46,766. The amounts of money were measured by nominal value.
Economic benefits were obtained from five categories: labor, health education and monitoring, clinical information management, administration and civil service, and maintenance [17,18]. Costs included purchasing expenses of hardware and software as well as expenses of system development and maintenance (Table 5).
Table 5.
Estimated cost and benefits of public health information system (2006-2012)
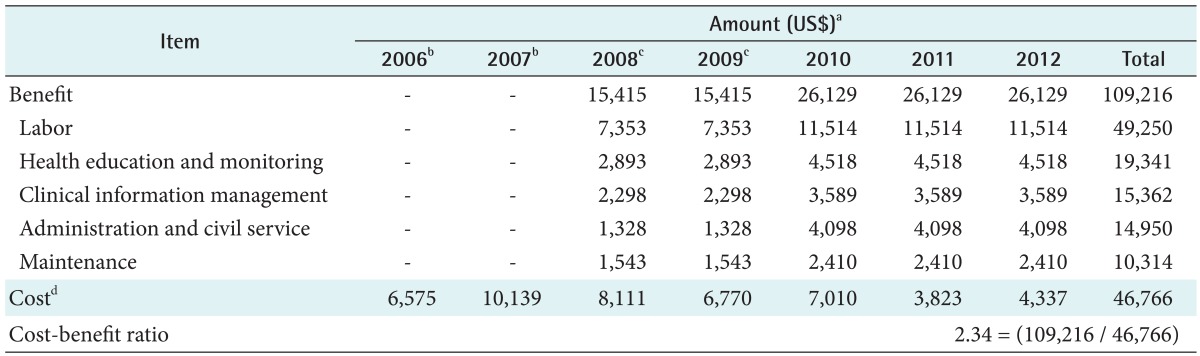
Values are presented as number (%).
aApplied to the currency exchange rates: 1 US$ = 1,050 KRW. bThere were no benefits in the period of system development from 2006 to 2007. cBenefits of 2008 and 2009 are acquired from 162 health institutions. dCost in each year includes purchasing expenses of hardware and software, expenses of system development and maintenance.
III. Discussion
South Korea's public health organizations provide public health services and primary medical services in addition to implementing public health programs to citizens in urban and rural districts. Public health organizations are particularly responsible for the underserved or low-income populations as well as in other countries. To put an emphasis on service itself and supply more qualified service, the use of ICT-based information systems was deemed a proper strategic method.
The MOHW of South Korea had gradually introduced the ICT-based PHIS since the late 1980s. However, there have been many limitations in introducing the system, namely, integration between tasks or organizations, production of information in terms of businesses and services, and user-centered service support [5]. With the increasing popularity of the Internet and advancement of ICT technology, a new ICT environment has been actively established.
To solve problems related to the previous information system, strategic plans were made in 2005 to establish a national healthcare information system, and healthcare information standardization at the national level was also started from that time. The development of the PHIS in South Korea was completed in 2007. The newly developed Web-based and integrated PHIS was disseminated to those public health organizations successfully until 2012.
Users' positive evaluation of PHIS has been demonstrated in terms of service quality (time reduction of decision-making, improving business process, and operational efficiency), system quality (ease of use and functionality), and system maintenance quality (technical maintenance and supporting service for usage). However, dissatisfaction with system accessibility was found. Problems with system accessibility may occur because of ICT networks or the environment of health organizations in rural or remote sites.
The implications of the integrated PHIS may be summarized as follows. First, from the perspective of the national outcome, service accessibility and convenience have been improved by enabling information sharing among public health organizations and healthcare-related organizations. As public health organizations can share medical records in the Web environment upon the consent of patients, the number of overlapping inspections and the waiting time has been decreased. The risk of medical malpractice or overtreatment of patients with chronic diseases has also been decreased through the exchange of medical care information. By enabling the issuance of medical reports through the e-government, the burden of patients visiting public health organizations has been eliminated. Moreover, the public health portal has increased the self-care and health literacy of patients or citizens.
Secondly, the new PHIS has enhanced the work efficiency and effectiveness of public health organizations. Office automation has been enabled through electronic medical care information, and management costs for medical records have been reduced. Real-time checking of information related to the safety and redundancy of prescribed drugs is provided by the drug utilization review system, which prevents inappropriate use of drugs. Further, through the exchange of electronic administrative information with external organizations, tasks, such as overlapping data input or confirmation of documents, have been eliminated or altered so that they can be carried out more effectively.
Furthermore, by automatically producing and reporting public documents in the PHIS, task productivity has increased. For instance, the number of manual task has decreased, and the public services have improved. Moreover, since the general improvement of the information system following the changes in the environment and functions of public healthcare has been made possible, overlapping system development has been prevented, and the burden of management and operation have been reduced.
Thirdly, from the public healthcare policy perspective, the establishment and scientific monitoring and evaluation of healthcare policy have increased. Information on the policies of the PHIS has been sufficiently provided and used in the establishment and evaluation of district healthcare policy. In addition, the time required for the formulation and evaluation of business plans has been reduced. Information on various diseases has been reported electronically, and a group within the national disease response system that can promptly take actions has been formed by the development of the distribution system. It was found that the new PHIS reduced the decision-making time and the number of overlapping tasks as compared to the previous information system.
Lastly, from the perspective of technological applications, intellectual property rights (patent) have been secured from the Korea Intellectual Property Office, and ISO 9001 verification has been received from the International Organization for Standardization. These signify objectivity with respect to the quality of the information system as well as operations management. Moreover, a leading IT technological foundation in the field of public healthcare information services has been built in an international environment.
However, additional improvement of the PHIS should be done for the desired and convenient services, such as telemedicine services for medically vulnerable populations living in rural or isolated regions, information exchange with private clinics or hospitals, and mobile healthcare services.
This study was limited in terms of the analysis and sources used, such as literature, documents and secondary data about development and users' evaluation of the PHIS of South Korea. Thus, it may be insufficient to fully evaluate the quality and performance of the PHIS. As the PHIS is being implemented and reinforced, and it is vital to the management on public health systems and quality enhancement of healthcare services, additional studies on improving the quality and the performance of the PHIS should be conducted.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Statistics Korea. Population Projections by Province: 2010-2040. Daejeon, Korea: Statistics Korea; 2012. [Google Scholar]
- 2.Organisation for Economic Co-operation and Development. OECD health data 2012: how does Korea compare [Internet] Paris, France: OECD; 2012. [cited at 2012 Nov 20]. Available from: http://www.oecd.org/korea/BriefingNoteKOREA2012inKorean.pdf. [Google Scholar]
- 3.National Health Insurance Corporation. 2011 major statistics about health insurance. Seoul, Korea: National Health Insurance Corporation; 2012. [Google Scholar]
- 4.Kim JW. Alternatives to adopt smart public healthcare service. IT Policy Res. 2011;7:1–29. [Google Scholar]
- 5.Ryu SW, Chang YS, Lee SY, Rhee HS, Yoon KI, Lee WJ, et al. Improving strategy of regional healthcare information system in Korea. Seoul, Korea: Korea Institute for Health and Social Affairs; 2006. [Google Scholar]
- 6.Ministry of Health and Welfare. Information strategy planning for public health. Seoul, Korea: Ministry of Health and Welfare; 2005. [Google Scholar]
- 7.AbouZahr C, Boerma T. Health information systems: the foundations of public health. Bull World Health Organ. 2005;83(8):578–583. [PMC free article] [PubMed] [Google Scholar]
- 8.Ministry of Health and Welfare. 2006 report on information of public health. Seoul, Korea: Ministry of Health and Welfare; 2006. [Google Scholar]
- 9.Ministry of Health and Welfare. 2007 report on information of public health. Seoul, Korea: Ministry of Health and Welfare; 2007. [Google Scholar]
- 10.Ministry of Health and Welfare. 2008 report on information of public health. Seoul, Korea: Ministry of Health and Welfare; 2008. [Google Scholar]
- 11.DeLone WH, McLean ER. The DeLone and McLean model of information systems success: a ten-year update. J of Manag Inf Syst. 2003;19(4):9–30. [Google Scholar]
- 12.Maenpaa T, Suominen T, Asikainen P, Maass M, Rostila I. The outcomes of regional healthcare information systems in health care: a review of the research literature. Int J Med Inform. 2009;78(11):757–771. doi: 10.1016/j.ijmedinf.2009.07.001. [DOI] [PubMed] [Google Scholar]
- 13.Korea Health and Welfare Information Service. Statistics on healthcare information service. Seoul, Korea: Korea Health and Welfare Information Service; 2012. [Google Scholar]
- 14.Park JH, Kim GM. A survey research on status of healthcare informatization. Seoul, Korea: Korea Health Promotion Foundation; 2010. [Google Scholar]
- 15.Ko IS, Chang H. Development of extended technology acceptance model on the intention of using PHR. J Korean Soc Health Inf Health Stat. 2013;38(1):26–38. [Google Scholar]
- 16.Choi W, Rho MJ, Park J, Kim KJ, Kwon YD, Choi IY. Information system success model for customer relationship management system in health promotion centers. Healthc Inform Res. 2013;19(2):110–120. doi: 10.4258/hir.2013.19.2.110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Korea Health and Welfare Information Service. Report on SR status of 2012. Seoul, Korea: Korea Health and Welfare Information Service; 2012. [Google Scholar]
- 18.Ministry of Health and Welfare. 2012 national information plan for implementation. Seoul, Korea: Ministry of Health and Welfare; 2012. [Google Scholar]