

Abstract
INTRODUCTION
Atypical presentations of appendix have been reported including backache, left lower quadrant pain and groin pain from a strangulated femoral hernia containing the appendix. We report a case presenting an epigastric pain that was diagnosed after computed tomography as a perforated appendicitis on intestinal malrotation.
PRESENTATION OF CASE
A 27-year-old man was admitted with a three-day history of epigastric pain. Physical examination revealed tenderness and defense on palpation of epigastric region. There was a left subcostal incision with the history of diaphragmatic hernia repair when the patient was 3 days old. He had an intestinal malrotation with the cecum fixed at the epigastric region and the inflamed appendix extending beside the left lobe of liver.
DISCUSSION
While appendicitis is the most common abdominal disease requiring surgical intervention seen in the emergency room setting, intestinal malrotation is relatively uncommon. When patients with asymptomatic undiagnosed gastrointestinal malrotation clinically present with abdominal pain, accurate diagnosis and definitive therapy may be delayed, possibly increasing the risk of morbidity and mortality.
CONCLUSION
Atypical presentations of acute appendicitis should be kept in mind in patients with abdominal pain in emergency room especially in patients with previous childhood operation for diaphragmatic hernia.
Keywords: Perforated appendicitis, Unusual presentation, Laparoscopy, Epigastric, Malrotation, Diaphragmatic hernia
1. Introduction
Appendicitis is the most frequent surgical emergency that requires removal of the appendix. Typical symptoms are periumbulical pain radiating to right lower quadrant with peritoneal irritation on abdominal examination, anorexia and fever. Atypical presentations have been reported including backache,1 left lower quadrant pain2 and groin pain from a strangulated femoral hernia containing the appendix.3
We report a case presenting an epigastric pain that was diagnosed after computed tomography (CT) as a perforated appendicitis on intestinal malrotation.
2. Presentation of case
A 27-year-old man was admitted to the Haydarpasa Numune Education and Research Hospital, Emergency Department, Istanbul. He had a three- day history of epigastric pain. The pain was associated with nausea, vomiting, anorexia and high fever.
Physical examination revealed tenderness and defense on palpation of epigastric region. There was a left subcostal incision with the history of diaphragmatic hernia repair when the patient was 3 days old. A laboratory examination revealed an elevated white blood cell (WBC) count at 19,800/μL with 76, 6% neutrophils (absolute neutrophil count: 15,200). Biochemical tests and urinalysis were normal.
Abdominal plain films demonstrated colonic air at epigastric region and left upper quadrant. Intestinal malrotation was not considered in the differential diagnosis at that point. No pneumoperitoneum was evident (Fig. 1). With a wide range of differential diagnosis (acute cholecystitis, perforated ulcer, pancreatitis, etc.), the patient had undergone an abdominal ultrasound that was unable to justify his symptoms. There was only minimal fluid in Morison's pouch. Therefore, he had an abdominal CT scan the next day with IV contrast. He had an intestinal malrotation with the cecum fixed at the epigastric region and the inflamed appendix extending beside the left lobe of liver. Patient had a partial situs viscerus inversus. Liver was located at original place, but stomach, spleen and pancreas were at right side of the abdomen under liver (Fig. 2A and B).
Fig. 1.

Abdominal plain films demonstrated colonic air at epigastric and left upper quadrant.
Fig. 2.
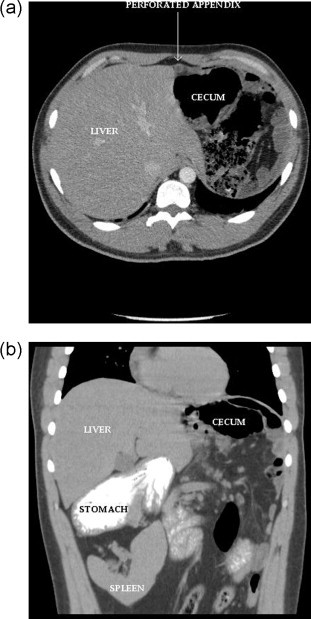
(A) CT shows an intestinal malrotation with the cecum in the epigastric region and the inflamed appendix extending beside the left lobe of liver. (B) The stomach and the spleen were located at the right side of the abdomen.
The patient was transferred to the emergency operating room for laparoscopic appendectomy. After scrubbing, we did a vertical incision 5 cm above the umbilicus and insufflation of the abdominal cavity, we explored the abdomen with a 0° optic. We used the supraumbulical optic tractor because we knew that appendix was located in the epigastric region according to CT findings. Another two 5 mm trocars were inserted to the left and the right sides 10 cm above the umbilicus at midclavicular lines. We first noticed the inflamed bowel segment lateral to the left lobe of liver. Appendectomy was performed and the inflamed appendix was extracted in an endobag and was sent to pathology (Figs. 3 and 4). Because of perforated appendix, necrosis and pus at appendectomy site, an intraabdominal drain was placed to prevent abscess formation.
Fig. 3.
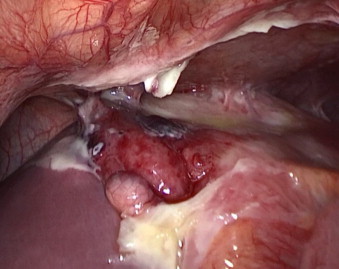
The appearance of the appendix, which was inflamed and perforated.
Fig. 4.
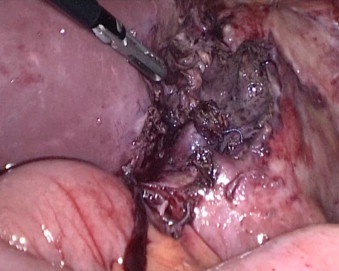
Appendectomy was performed.
The postoperative course was unremarkable and the drain in the epigastric region could be removed on post op day 5. The patient was discharged 6 days later without any complications.
Pathology report mentioned perforated gangrenous appendicitis with an acute periappendicular abscess.
3. Discussion
While appendicitis is the most common abdominal disease requiring surgical intervention seen in the emergency room setting, intestinal malrotation is relatively uncommon.4 Intestinal malrotation represents the errors of rotation of the midgut about the superior mesenteric artery during weeks 5–10 of fetal life and subsequent abnormal fixation to the peritoneal wall. The estimated incidence of intestinal malrotation is 1 in every 500 live births5 based on autopsy series, retrospective reviews,6 and prospective barium enema studies.7 The true incidence of adults with asymptomatic malrotation remains difficult to accurately determine.
The typical history of appendicitis includes pain starting periumbilically before localizing to the right iliac fossa; this is due to the poor localizing property of visceral nerves from the mid-gut, followed by the involvement of somatic nerves (parietal peritoneum) as the inflammation progresses. The pain is usually associated with loss of appetite and fever. Nausea or vomiting may or may not occur.2 However, in our case the pain was located in the epigastric region and no pain was noted in the right abdomen. Although atypical locations are frequently seen,1–3 epigastric localization of acute appendicitis was not reported in the literature.
When patients with asymptomatic undiagnosed gastrointestinal malrotation clinically present with abdominal pain, accurate diagnosis and definitive therapy may be delayed, possibly increasing the risk of morbidity and mortality.4,8
Other cases of appendicitis in adults or adolescents in the context of intestinal malrotation have been described previously,5–7,9–12 frequently with delayed or incorrect initial diagnoses. Several of these prior reports describe the diagnosis of acute appendicitis and gastrointestinal malrotation based on abdominal CT, further immediate dynamic imaging of the intestinal malrotation is often unnecessary, provided the CT is sufficient for surgical planning, as in this case. Furthermore, the sensitivity and specificity of upper gastrointestinal, fluoroscopic barium enema or abdominal ultrasound in adolescent or adult patients for detection of causes of an acute abdomen are limited compared to CT.
In our case, abdominal ultrasonography made the diagnosis of acute appendicitis less likely. However, the persistence of pain and the increasing inflammatory parameters in his blood exams pushed the medical team to further investigate and a CT scan revealed intestinal malrotation with acute appendicitis.
In a study, including 331 cases of intestinal rotation, there were 111 (33, 5%) neonates with malrotation caused by diaphragmatic hernia.13 Our patient had an operation for diaphragmatic hernia when he was 3 days old. Therefore, we should keep in mind the association of diaphragmatic hernia and possibility of intestinal malrotation.
4. Conclusion
Atypical presentations of acute appendicitis should be kept in mind in patients with abdominal pain in emergency room especially in patients with previous childhood operation for diaphragmatic hernia. CT scan is superior to ultrasonography in the diagnosis of atypical localization of the appendix.
Conflict of interest
The authors declare that there is no conflict of interest.
Funding
None.
Ethical approval
Patient signed consent to publish the case report.
Authors’ contribution
Odabasi M and Arslan C performed endoscopic and surgical procedures; Yildiz MK, Eris C, Gunay E, Muftuoglu T, Ozkan E, Aktekin A and Abuoglu H contributed to writing the article and reviewing the literature in a comprehensive literature search; Odabasi M designed and prepared the manuscript.
Footnotes
This is an open-access article distributed under the terms of the Creative Commons Attribution-NonCommercial-No Derivative Works License, which permits non-commercial use, distribution, and reproduction in any medium, provided the original author and source are credited.
References
- 1.Stevenson W.O. A case of appendicitis with most unusual symptoms. Canadian Medical Association Journal. 1938;39:263–264. [PMC free article] [PubMed] [Google Scholar]
- 2.Talanow R. An unusual manifestation of acute appendicitis with left flank pain. Radiology Case. 2008;2:8–11. doi: 10.3941/jrcr.v2i1.27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Nguyen E., Komenaka I. Strangulated femoral hernia containing a perforated appendix. Canadian Journal of Surgery. 2004;47:68–69. [PMC free article] [PubMed] [Google Scholar]
- 4.Welte F.J., Grosso M. Left-sided appendicitis in patient with congenital gastrointestinal malrotation: a case report. Journal of Medical Case Reports. 2007;1:92. doi: 10.1186/1752-1947-1-92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Keith J.C.T.J., Buday S.J., Price P.D., Smear J. Asymptomatic midgut rotational anomalies in adults: 2. Case reports and review of the literature. Contemporary Surgery. 2003;59:322–325. [Google Scholar]
- 6.Malek M.M., Burd R.S. Surgical treatment of malrotation after infancy: a population-based study. Journal of Pediatric Surgery. 2005;40:285–289. doi: 10.1016/j.jpedsurg.2004.09.028. [DOI] [PubMed] [Google Scholar]
- 7.Kantor J.L. Anomalies of the colon. Radiology. 1934;23:651–662. [Google Scholar]
- 8.Au A.C.Y., Syed A., Bradpiece H.A. A rare case of intestinal malrotation presenting as appendicitis in late adulthood. Journal of Strength and Conditioning Research. 2010;8:3. doi: 10.1093/jscr/2010.8.3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Hollander S.C., Springer S.A. The diagnosis of acute left-sided appendicitis with computed tomography. Pediatric Radiology. 2003;33:70–71. doi: 10.1007/s00247-002-0829-x. [DOI] [PubMed] [Google Scholar]
- 10.Lin C.J., Tiu C.M., Chou Y.H., Chen J.D., Liang W.Y., Chang C.Y. CT presentation of ruptured appendicitis in an adult with incomplete intestinal malrotation. Emergency Radiology. 2004;10:210–212. doi: 10.1007/s10140-003-0316-1. [DOI] [PubMed] [Google Scholar]
- 11.Hou S.K., Chern C.H., How C.K., Kao W.F., Chen J.D., Wang L.M. Diagnosis of appendicitis with left lower quadrant pain. Journal of the Chinese Medical Association. 2005;68:599–603. doi: 10.1016/S1726-4901(09)70101-7. [DOI] [PubMed] [Google Scholar]
- 12.Pinto A., Di Raimondo D., Tuttolomondo A., Fernandez P., Caronia A., Lagalla R. An atypical clinical presentation of acute appendicitis in a young man with midgut malrotation. Radiography. 2007;13:164–168. [Google Scholar]
- 13.Rescorla F.J., Shedd F.J., Grosfeld J.L., Vane D.W., West K.W. Anomalies of intestinal rotation in childhood: analysis of 447 cases. Surgery. 1990;108:710–715. discussion 715–6. [PubMed] [Google Scholar]