

Abstract
ObjectiveStudies have shown that there is sufficient availability of mammography; however, little is known about geographic variation in capacity. The purpose of this study was to determine the locations and extent of over/undersupply of mammography in 14 southern states from 2002 to 2008.
Data SourcesMammography facility data were collected from the U.S. Food and Drug Administration (FDA). Population estimates, used to estimate the potential demand for mammography, were obtained from GeoLytics Inc.
Study DesignUsing the two-step floating catchment area method, we calculated spatial accessibility at the block group level and categorized the resulting index to represent the extent of under/oversupply relative to the potential demand.
Principal FindingsResults show decreasing availability of mammography over time. The extent of over/undersupply varied significantly across the South. Reductions in capacity occurred primarily in areas with an oversupply of machines, resulting in a 68 percent decrease in the percent of women living in excess capacity areas from 2002 to 2008. The percent of women living in poor capacity areas rose by 10 percent from 2002 to 2008.
ConclusionsOur study found decreasing mammography availability and capacity over time, with substantial variation across states. This information can assist providers and policy makers in their business planning and resource allocation decisions.
Keywords: Health services accessibility, geographic information systems, mammography, health services needs and demands, spatial analysis
The value of mammography is finding breast cancers early when treatment is most effective. Screening recommendations vary widely, with the American Cancer Society recommending annual screening of women aged 40 and older, and the U.S. Preventive Services Task Force recommending biennial screening for only women aged 50–74 years (U.S. Preventive Services Task Force 2009; American Cancer Society 2012). Despite the divergent guidelines, the benefits of mammography are clear—reduced mortality and incidence of late-stage breast cancers, which are more difficult to treat (Norman et al. 2006, 2007; Mandelblatt et al. 2009). The positive results from randomized clinical trials and economic incentives for providers resulted in an explosion of mammography technology in the 1980s. Machines were purchased at an unprecedented rate, such that supply outstripped need by the late 1980s (Brown, Kessler, and Rueter 1990). As Brown, Kessler, and Rueter (1990) show, the costs associated with those unused machines doubled the price of each mammogram performed. Despite evidence of increasing availability of mammography, reports of long wait times and access issues prompted Congress to request an investigation by the Government Accounting Office (GAO; U.S. General Accounting Office 2002). Although the GAO reported adequate capacity nationwide (U.S. General Accounting Office 2002; U.S. Government Accountability Office 2006), they found that over 400 U.S. counties had a net loss of 1 mammography machine from 2001 to 2004, and 25 percent of those counties had a net loss of >25 percent of their mammography machines.
In the last decade, several authors have studied the availability, accessibility, and capacity of mammography in the United States (Marchick and Henson 2005; Wang et al. 2008; Elting et al. 2009; Meersman et al. 2009; Rahman et al. 2009; Elkin et al. 2010; Lian, Struthers, and Schootman 2012; Peipins et al. 2012). Availability is indicative of the spatial distribution of services, while accessibility measures the ease with which people can access those services. Capacity goes a step further, examining both the supply and demand for services. To date, most studies have focused on the relationship between regional variations in mammography accessibility or capacity and breast cancer screening utilization and late-stage diagnosis. In this study, we examined the geographic distribution of mammography facilities and how their placement can create pockets of under/oversupply relative to the underlying population. Using information about the locations of FDA-certified mammography facilities in 14 southern states during the period 2002–2008 and the population distribution of women aged 40+ during the same time interval, we calculated annual, spatial accessibility scores using the two-step floating catchment area (2SFCA) method developed by Luo and Wang (2003). These scores were then categorized into levels of capacity (i.e., no access within 1 hour drive time, inadequate, adequate, or excess) that represent the extent of under/oversupply relative to the demand for services. This information can assist in business growth planning and resource allocation to promote both economic growth and the public’s health. Thus, we present the first longitudinal, multistate assessment of geographic variability in mammography capacity to date.
Methods
Using information about the locations of mammography facilities (supply measured as the number of mammogram machines at each facility) and potential mammography users (demand measured as the number of women aged 40+ in each block group), we performed a series of functions in ArcGIS Version 10.0 (ESRI 2009) to measure the spatial accessibility of mammography facilities to potential users in 14 southern states. To determine whether the capacity of mammography facilities was adequate relative to demand, our measure of spatial accessibility was compared with the threshold needed to achieve the HealthyPeople 2020 objective of 81 percent screening coverage (biennially for all women 40+; U.S. Department of Health and Human Services 2010). To determine whether capacity was excessive, our measure was also compared with a more conservative estimate of 100 percent of women aged 40+ being screened annually, plus an additional 15 percent of all women 40+ going back for a follow-up mammogram.
Mammography Facility Data (Supply)
The U.S. Food and Drug Administration (FDA) manages the certification program for all mammography facilities in the United States. Facilities must first apply for accreditation through an FDA-approved accreditation body. Certifying agencies are then responsible for the facility’s annual (i.e., 10–14 months) inspections and all compliance issues, as well as issuing, renewing, revoking, denying, or suspending certificates. More details on the Mammography Quality Standards Act can be found on the FDA’s website (U.S. Food and Drug Administration 2012).
We obtained data from 2002 to 2008 on all FDA-certified mammography facilities in the South (i.e., Texas/TX, Oklahoma/OK, Arkansas/AR, Louisiana/LA, Mississippi/MS, Alabama/AL, Tennessee/TN, Kentucky/KY, Georgia/GA, Florida/FL, South Carolina/SC, North Carolina/NC, Virginia/VA, West Virginia/WV) and its adjacent states through a Freedom of Information Act (U.S. Food and Drug Administration 2012) request in March 2011. Our data file contained facility-specific information such as the address and number of mammography machines on site. Federal facilities, including Veteran’s Administration, military, and Indian Health Service hospitals and clinics, were removed from the file due to their restrictions on eligibility for services. All mammography facilities included in our study were (1) located within the 14 state study region or within a 1 hour drive into a neighboring state and (2) certified all or part of 2002–2008. Mammography facilities were geocoded to their exact address where possible and to the zip code centroid otherwise (more information available in the Appendix).
Population Data (Potential Demand)
Based on the current screening recommendations (U.S. Preventive Services Task Force 2009; American Cancer Society 2012), all women ages 40 and older represent potential mammography users. To examine adequate supply, we defined the potential demand for mammography services as half the number of women aged 40 and older at the block group level in any given year (i.e., assumes biennial screening). For the purpose of this study, we did not set an upper age limit for the population seeking mammography as studies have shown that many women continue to seek mammography well past age 74 (Kagay, Quale, and Smith-Bindman 2006; Tan, Kuo, and Goodwin 2012). To look at oversupply, we chose a more conservative demand population: the number of women aged 40 and up at the block group level in any given year (i.e., assumes annual screening), plus an additional 15 percent that may be called back for second views or diagnostic evaluation (Lewin et al. 2002). Population-weighted (i.e., weighted to the underlying block-level population in 2000) block group centroids signified the locations of potential mammography users. Annual estimates for the population at the block group level were obtained from GeoLytics Inc (2012).
A sensitivity analysis was used to examine the impact of changing the potential demand for services on estimates of mammography capacity. Specifically, we compared estimates across three age groups: (1) women aged 40 and older (baseline scenario); (2) women aged 50 and older; and (3) women aged 50–74 years.
Geographic Analysis
Using ArcGIS Version 10 Network Analyst, we constructed 60-minute catchment areas around each mammography facility using road network data. We then calculated spatial accessibility to mammography facilities using the 2SFCA method (Radke and Mu 2000; Luo and Wang 2003), which provides a supply–demand ratio based on spatially defined assumptions about the interaction between patients and their potential health care providers (i.e., women will choose to visit mammography facilities within 1 hour’s drive from where they live). Step 1 of the 2SFCA is a facility-specific ratio: the number of machines divided by the number of potential users in its catchment area. Step 2 is a user-specific ratio: summing over all the facilities that fall within a preset drive time (in this case, 60 minutes) from the user’s location. The larger the resulting accessibility score, the better the access to mammography services (more details in the Appendix).
Once spatial accessibility was measured, we examined whether the supply was adequate to meet potential demand for services. With 1 mammogram machine being capable of performing 6,000 mammograms per year (3 mammograms/hour, 8 hours/day, 5 days/week for 50 weeks) (8), 1.667 machines per 10,000 women would be needed to screen all women aged 40 and older annually as recommended by the American Cancer Society (1). With a more conservative, biennial screening goal of 81 percent as cited by HealthyPeople 2020 (U.S. Department of Health and Human Services 2010), this would equate to 0.675 machines/10,000 women aged 40+. Our definitions of capacity are further defined in Table 1.
Table 1.
Definitions of Mammography Capacity
| Variable | Definition | Assumptions |
|---|---|---|
| No access within 1 hour | No mammography machines within a 1 hour drive from population-weighted block group centroid | N/A |
| Inadequate capacity | ≤0.674 machines/10,000 women | Biennial screening of 81% of women aged 40+ |
| Poor capacity | No access within 1 hour or inadequate capacity | Same as above |
| Adequate capacity | >0.674 machines/10,000 women | Same as above |
| Excess capacity | ≥1.917 machines/10,000 women | Annual screening of 100% of women aged 40+, plus 15% recalled for further evaluation |
Results
Mammography Availability and Capacity in the South over Time
The total number of FDA-certified mammography facilities/mammography machines in the South and its bordering states that fell within one or more block group catchment areas in the South generally decreased over time, from 3,342 facilities and 5,137 machines in 2002 to 3,283 facilities and 4,707 machines in 2008 (see Figure 1). Most of the decrease was between the years 2006 and 2008, and in areas with excess capacity. The loss of 430 mammography machines (5,137 in 2002 to 4,707 machines in 2008), coupled with an increase in the population of women aged 40+ in block groups with access to one or more facilities (11 percent increase from 2002 to 2008), shifted 70 percent of block groups with excess capacity in 2002 to adequate capacity in 2008. In contrast, only 10 percent of block groups with poor capacity in 2002 were able to attain adequate capacity by 2008 and only 8 percent of block groups with no access within 1 hour had any improvement in capacity over time. In fact, only 1 of the 38 block groups with no access within 1 hour in 2002 was able to attain adequate capacity by 2008.
Figure 1.
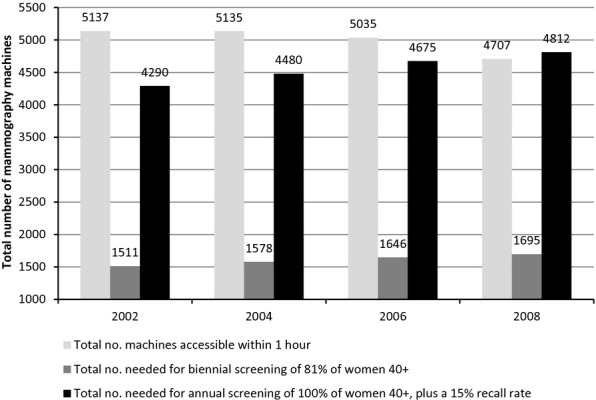
Extent of Oversupply of Mammography Machines in the South over Time, 2002–2008
Extent of Oversupply of Mammography Machines in the South over Time
Translated in another way, we determined whether the aggregate supply of mammography machines is capable of meeting the potential demand for services in the study region (see Figure 1). In 2002, there were 3.4 times more mammography machines available than would be needed to screen 81 percent of women aged 40+ biennially (5,137 : 1,511 machines) and about 20 percent more than would be needed to screen 100 percent of women 40+ annually, plus an estimated 15 percent needing second views/diagnostic services (5,137 : 4,290 machines). However, the oversupply of mammography machines declined over time. By 2008, there were 2.8 times more mammography machines available than would be needed to screen 81 percent of women 40+ biennially (4,707 : 1,695 machines), and about 100 less than what would be needed to screen 115 percent annually (4,707 : 4,812 machines).
Geographic Variation in Mammography Capacity
The geographic distribution of mammography capacity at the block group level is highlighted in Figure 2. In the entire 14-state study region, the proportion of women aged 40 and older living in areas with poor mammography capacity rose by 10 percent, from 1.17 percent (n = 260,947) in 2002 to 1.29 percent (n = 323,895) in 2008 (see Table 2). From 2002 to 2008, the percent of women aged 40+ living in poor capacity areas rose in most states, except for North Carolina, Tennessee, Virginia, and West Virginia. Oklahoma and Mississippi showed the largest increases in poor capacity (+0.91 percent and +0.89 percent, respectively), and Virginia showed the most improvement (−0.47 percent). In absolute terms, Texas contributed the most women to the total number of women living in poor capacity areas in the South (44 percent in 2008).
Figure 2.
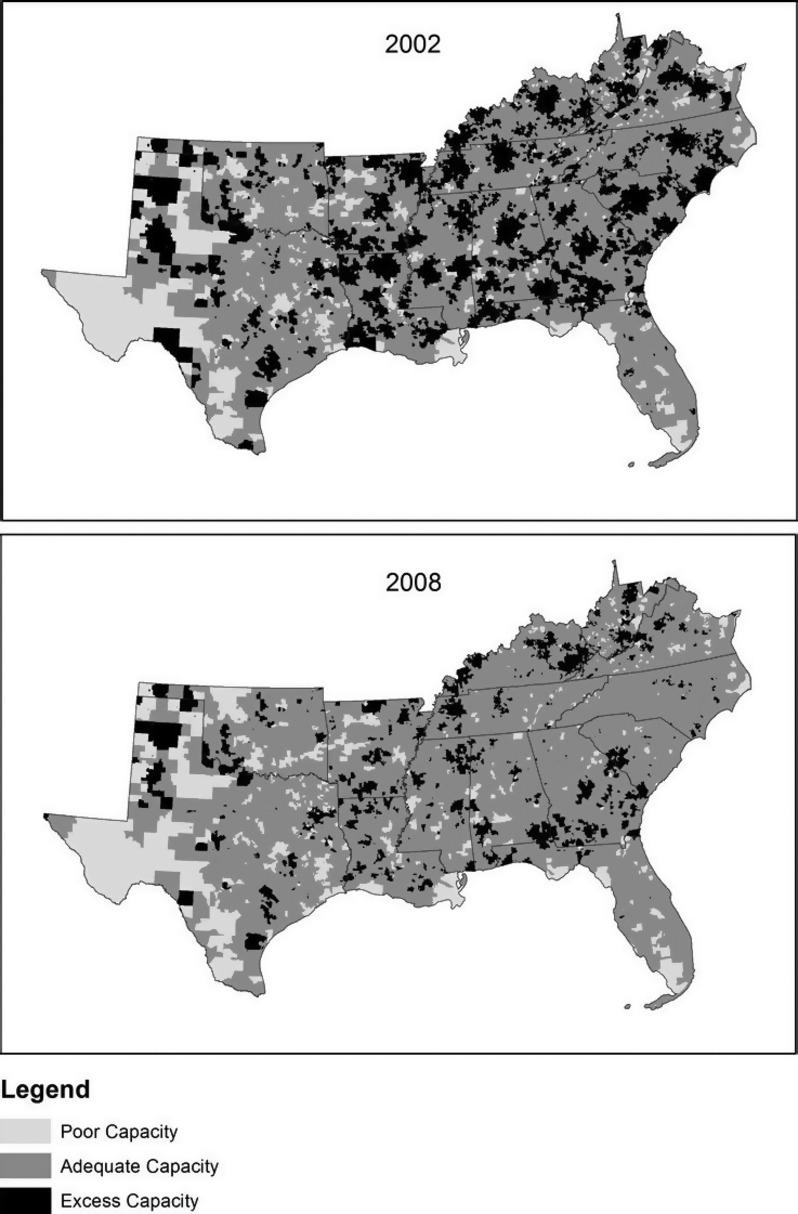
Regional Variation in Mammography Capacity in the South, 2002 and 2008
Table 2.
Proportion of Women Aged 40+ Who Live in Areas with Poor or Excess Mammography Capacity by State and Year, 2002–2008
| 2002 | 2004 | 2006 | 2008 | |||||
|---|---|---|---|---|---|---|---|---|
| Poor | Excess | Poor | Excess | Poor | Excess | Poor | Excess | |
| N (% Pop) | N (% Pop) | N (% Pop) | N (% Pop) | N (% Pop) | N (% Pop) | N (% Pop) | N (% Pop) | |
| 14 states | 260,947 (1.17) | 7,493,756 (33.49) | 267,116 (1.14) | 6,139,331 (26.27) | 279,637 (1.15) | 4,605,372 (18.89) | 323,895 (1.29) | 2,411,942 (9.61) |
| AL | 12,584 (1.16) | 550,414 (50.78) | 10,179 (0.92) | 380,108 (34.22) | 12,455 (1.09) | 208,097 (18.23) | 14,637 (1.26) | 138,856 (11.97) |
| AR | 11,162 (1.72) | 362,280 (56.60) | 8,019 (1.20) | 410,192 (61.52) | 10,517 (1.53) | 291,698 (42.47) | 15,358 (2.19) | 178,779 (25.54) |
| FL | 28,848 (0.66) | 440,604 (10.09) | 30,727 (0.67) | 216,160 (4.70) | 34,381 (0.71) | 82,179 (1.70) | 34,110 (0.69) | 75,475 (1.53) |
| GA | 3,237 (0.18) | 940,282 (51.09) | 4,615 (0.24) | 669,354 (34.14) | 5,216 (0.25) | 429,914 (20.55) | 5,714 (0.26) | 244,347 (11.06) |
| KY | 2,497 (0.26) | 421,240 (43.33) | 3,134 (0.31) | 468,314 (46.79) | 3,558 (0.34) | 460,564 (44.55) | 4,688 (0.44) | 292,408 (27.57) |
| LA | 8,927 (0.88) | 661,894 (65.22) | 9,990 (0.97) | 654,031 (63.21) | 12,443 (1.23) | 501,326 (49.70) | 10,962 (1.08) | 169,056 (16.62) |
| MS | 6,048 (0.93) | 314,741 (48.26) | 6,803 (1.01) | 293,570 (43.78) | 7,631 (1.12) | 196,475 (28.73) | 12,610 (1.82) | 107,733 (15.55) |
| NC | 5,952 (0.31) | 678,467 (34.79) | 6,327 (0.31) | 596,887 (29.18) | 6,636 (0.31) | 462,026 (21.49) | 5,492 (0.24) | 107,982 (4.81) |
| OK | 18,721 (2.29) | 178,322 (21.80) | 19,886 (2.38) | 113,817 (13.64) | 17,979 (2.11) | 105,795 (12.43) | 27,461 (3.20) | 39,637 (4.62) |
| SC | 608 (0.06) | 541,397 (55.36) | 707 (0.07) | 385,796 (37.71) | 1,888 (0.18) | 274,013 (25.60) | 4,394 (0.40) | 71,591 (6.46) |
| TN | 8,978 (0.65) | 632,861 (45.53) | 7,702 (0.53) | 635,317 (44.10) | 8,300 (0.55) | 487,401 (32.45) | 9,720 (0.63) | 243,713 (15.71) |
| TX | 113,610 (2.53) | 929,598 (20.72) | 118,234 (2.50) | 806,143 (17.05) | 118,453 (2.37) | 654,781 (13.12) | 144,114 (2.80) | 443,182 (8.62) |
| VA | 29,263 (1.72) | 624,227 (36.72) | 30,134 (1.69) | 321,678 (18.07) | 29,680 (1.59) | 296,958 (15.95) | 24,059 (1.25) | 142,538 (7.39) |
| WV | 10,512 (2.23) | 211,429 (44.74) | 10,659 (2.24) | 187,964 (39.44) | 10,500 (2.18) | 154,145 (31.97) | 10,576 (2.19) | 156,645 (32.47) |
A sensitivity analysis used to examine the impact of changing the potential demand for services (i.e., number of women included in the denominator) revealed the most extensive changes in areas defined as having excess mammography capacity (see Table 3). In the entire study region, excess capacity increased substantially as the potential demand for services narrowed by age restrictions, despite overall declines from 2002 to 2008. Although poor capacity increased 10 percent from 2002 to 2008 in the population of women aged 40+, the number of women living in poor capacity block groups increased about 5 percent in women aged 50+ and decreased about 7 percent in women aged 50–74 years. State-specific estimates are available by request.
Table 3.
Sensitivity Analysis of Mammography Capacity across Different Age Groups, 2002 and 2008
| 2002 | 2008 | ||||
|---|---|---|---|---|---|
| Age Group | Poor N (% Pop) | Excess N (% Pop) | Poor N (% Pop) | Excess N (% Pop) | |
| 14 states | 40+ | 260,947 (1.17) | 7,493,756 (33.49) | 323,895 (1.29) | 2,411,942 (9.61) |
| 50+ | 122,035 (0.81) | 11,691,776 (77.88) | 147,850 (0.85) | 10,482,529 (60.25) | |
| 50–74 | 81,771 (0.71) | 10,251,194 (89.50) | 88,339 (0.66) | 11,009,551 (82.00) | |
Discussion
Our study found a substantial amount of variation in mammography capacity in the southern United States. Many rural areas of the South had less than adequate capacity to fill the demand for mammography services, whereas many large cities had more than enough capacity. Generally, the amount of supply relative to demand improved over time, with fewer areas having an overabundance of supply (68 percent reduction in the proportion of women living in excess capacity areas over time). However, the proportion of women aged 40+ living in areas with poor capacity grew by 10 percent. Hence, although there was less oversupply of mammography machines over time, the maldistribution of resources was not remedied. Large, contiguous geographic areas remained without adequate access to mammography throughout the study period.
Differences in mammography capacity (or density of facilities) have been shown to influence mammography screening utilization and/or breast cancer stage at diagnosis in several recent studies (Marchick and Henson 2005; Wang et al. 2008; Elting et al. 2009; Meersman et al. 2009; Rahman et al. 2009; Elkin et al. 2010). These studies found that living in an area with poor mammography capacity decreased the likelihood of receiving a timely mammogram and/or increased the likelihood of a late-stage diagnosis. Similarly, Marchick and Henson (2005) found that living in an area with greater mammography capacity increased the likelihood of women with breast cancer being diagnosed at an earlier stage (i.e., in situ). Some have even suggested that excess capacity may create unnecessary demand for services (i.e., screening at greater than recommended intervals) and ultimately, more false-positive tests leading to invasive breast biopsies (Mushlin 1990). Although the focus of our study was providing an accurate measure of mammography capacity that better classifies areas of over/undersupply, it is noteworthy that mammography capacity has been tied to patient-level outcomes and thus has the potential to improve population health outcomes when intervened upon.
In this study, we improved upon previous studies of mammography capacity by accounting for the geographic locations and magnitude of supply and demand points, rather than aggregating data over administrative boundaries (e.g., presence/absence of mammography facilities in a particular county). We also provided a comprehensive picture of how capacity changed over space and time. Despite these strengths, we note some limitations. Although informed by the literature and standard screening guidelines, the choice of the demand population and catchment area size is likely to impact one’s estimates. Researchers are currently grappling with these issues (Luo and Qi 2009; McGrail and Humphreys 2009; Luo and Whippo 2012) and measurement changes have been made over the years (e.g., E2SFCA, V2SFCA, McGrail Access Index); however, these studies have tended to focus on gradients of spatial accessibility, rather than predefined thresholds of capacity needed to serve large populations. In addition, none of these studies have conducted their analysis across multiple states. By showing the sensitivity of our estimates across different age groups, we have shown the importance of considering varying definitions of demand in one’s analysis. Additional work is needed to develop and disseminate programs/tools that address the catchment area size problem, particularly across multiple states that have disparate actual and perceived travel burdens.
Findings from this multistate, longitudinal assessment of mammography capacity lay the groundwork for a variety of future studies and interventions to increase capacity in the South. We have measured geographic patterns of mammography capacity that can assist policy makers, particularly at state and local levels, in (1) attracting for-profit mammography facilities to areas with poor capacity with monetary/tax incentives; (2) developing outreach programs using mobile mammography units to increase access to mammography; and (3) making informed, resource allocation decisions with public health funds and grants. Further research investigations can help accomplish these goals. Specifically, it is important to replicate these methods on a national basis to determine capacity across the United States, examine how different catchment area sizes might affect the results, and explore the optimal locations for additional fixed and/or mobile machines to increase capacity using suitability analysis and location–allocation techniques. There is also an opportunity for policy makers at the federal level to integrate a similar measurement approach into their current determination of Health Professional Shortage Areas, Medically Underserved Areas/Populations, and Primary Care Shortage Areas, which currently do not make use of time or distance parameters.
The rise of mammography in the United States in the 1980s was well documented by Brown, Kessler, and Rueter (1990). In this study, we noted a downward trend in the availability of mammography over time, suggesting that the market could not sustain the rate of growth seen in the 1980s. Although the balance of supply and demand improved during the study period, we found that places with poor capacity largely remained unchanged over time. In fact, the number of women living in areas with poor capacity increased by 10 percent. Initiatives aimed at identifying and implementing cost-effective strategies to improve access to mammography in these areas are sorely needed.
Acknowledgments
Joint Acknowledgment/Disclosure Statement: Dr. Jan Eberth was the recipient of a cancer prevention fellowship supported by the National Cancer Institute (R25T CA57730, Shine Chang, Ph.D., Principal Investigator) and the National Institutes of Health (MD Anderson Cancer Center Support Grant CA016672) during the course of the study. Dr. Elting was supported by “Disparities in Mammography Screening in the Rural South” DISP 070743503 from Susan G. Komen for the Cure and “CERCIT: Comparative Effectiveness Research on Cancer in Texas” RP101207 Cancer Prevention and Research Institute of Texas. The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the National Cancer Institute or the National Institutes of Health. The funding sources played no role in any aspect of this study, including no role in data collection, analysis, or interpretation; writing of the manuscript; or the decision to submit it for publication.
Disclosures
None.
Disclaimers
None.
Supporting Information
Additional Supporting Information may be found in the online version of this article:
Author Matrix.
Mammography Facilities.
References
- American Cancer Society. 2012. Breast Cancer Early Detection: American Cancer Society Recommendations for Early Breast Cancer Detection in Women without Breast Symptoms” [accessed on August 22, 2012]. Available at http://www.cancer.org/Cancer/BreastCancer/MoreInformation/BreastCancerEarlyDetection/breast-cancer-early-detection-acs-recs.
- Brown ML, Kessler LG, Rueter FG. Is the Supply of Mammography Machines Outstripping Need and Demand? An Economic Analysis. Annals of Internal Medicine. 1990;113(7):547–52. doi: 10.7326/0003-4819-113-7-547. [DOI] [PubMed] [Google Scholar]
- Elkin EB, Ishill NM, Snow JG, Panageas KS, Bach PB, Liberman L, Wang F, Schrag D. Geographic Access and the Use of Screening Mammography. Medical Care. 2010;48(4):349–56. doi: 10.1097/MLR.0b013e3181ca3ecb. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elting LS, Cooksley CD, Bekele BN, Giordano SH, Shih YCT, Lovell KK, Avritscher EBC, Theriault R. Mammography Capacity: Impact on Screening Rates and Breast Cancer Stage at Diagnosis. American Journal of Preventive Medicine. 2009;37(2):102–8. doi: 10.1016/j.amepre.2009.03.017. [DOI] [PubMed] [Google Scholar]
- ESRI. ArcGIS Version 10.0 [Software] Redlands, CA: ESRI; 2009. [Google Scholar]
- GeoLytics Inc. Annual Estimates Premium 2001–2008. East Brunswick, NJ: GeoLytics Inc; 2012. [Google Scholar]
- Kagay CR, Quale C, Smith-Bindman R. Screening Mammography in the American Elderly. American Journal of Preventive Medicine. 2006;31(2):142–9. doi: 10.1016/j.amepre.2006.03.029. [DOI] [PubMed] [Google Scholar]
- Lewin JM, D’Orsi CJ, Hendrick RE, Moss LJ, Isaacs PK, Karellas A, Cutter GR. Clinical Comparison of Full-Field Digital Mammography and Screen-Film Mammography for Detection of Breast Cancer. American Journal of Roentgenology. 2002;179(3):671–7. doi: 10.2214/ajr.179.3.1790671. [DOI] [PubMed] [Google Scholar]
- Lian M, Struthers J, Schootman M. Comparing GIS-Based Measures in Access to Mammography and Their Validity in Predicting Neighborhood Risk of Late-Stage Breast Cancer. PLoS ONE. 2012;7(8):e43000. doi: 10.1371/journal.pone.0043000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luo W, Qi Y. An Enhanced Two-Step Floating Catchment Area (E2SFCA) Method for Measuring Spatial Accessibility to Primary Care Physicians. Health and Place. 2009;15(4):1100–7. doi: 10.1016/j.healthplace.2009.06.002. [DOI] [PubMed] [Google Scholar]
- Luo W, Wang F. Measures of Spatial Accessibility to Healthcare in a GIS Environment: Synthesis and a Case Study in Chicago Region. Environment and Planning B: Planning and Design. 2003;30(6):865–84. doi: 10.1068/b29120. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luo W, Whippo T. Variable Catchment Sizes for the Two-Step Floating Catchment Area (2SFCA) Method. Health and Place. 2012;18(4):789–95. doi: 10.1016/j.healthplace.2012.04.002. [DOI] [PubMed] [Google Scholar]
- Mandelblatt JS, Cronin KA, Bailey S, Berry DA, Draisma HJ, de Koning G, Hui H, Lee SJ, Munsell M, Plevritis SK, Ravdin P, Schechter CB, Sigal B, Stoto MA, Stout NK, Venier NT, van Ravesteyn J, Zelen M, Feuer EJ. Effects of Mammography Screening under Different Screening Schedules: Model Estimates of Potential Benefits and Harms. Annals of Internal Medicine. 2009;151(10):738–47. doi: 10.1059/0003-4819-151-10-200911170-00010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marchick J, Henson DE. Correlations between Access to Mammography and Breast Cancer Stage at Diagnosis. Cancer. 2005;103:1571–80. doi: 10.1002/cncr.20915. [DOI] [PubMed] [Google Scholar]
- McGrail MR, Humphreys JS. Measuring Spatial Accessibility to Primary Care in Rural Areas: Improving the Effectiveness of the Two-Step Floating Catchment Area Method. Applied Geography. 2009;29(4):533–41. [Google Scholar]
- Meersman SC, Breen N, Pickle LW, Meissner HI, Simon P. Access to Mammography Screening in a Large Urban Population: A Multi-Level Analysis. Cancer Causes and Control. 2009;20(8):1469–82. doi: 10.1007/s10552-009-9373-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mushlin AI. Oversupply of Screening Mammography Units: Why Should Internists Care? Annals of Internal Medicine. 1990;113(7):489–90. doi: 10.7326/0003-4819-113-7-489. [DOI] [PubMed] [Google Scholar]
- Norman S, Localio A, Zhou L, Weber A, Coates R, Malone K, Bernstein L, Marchbanks P, Liff J, Lee N, Nadel M. Benefit of Screening Mammography in Reducing the Rate of Late-Stage Breast Cancer Diagnoses (United States) Cancer Causes and Control. 2006;17(7):921–9. doi: 10.1007/s10552-006-0029-3. [DOI] [PubMed] [Google Scholar]
- Norman S, Russell Localio A, Weber A, Coates R, Zhou L, Bernstein L, Malone K, Marchbanks P, Weiss L, Lee N, Nadel M. Protection of Mammography Screening against Death from Breast Cancer in Women Aged 40–64 Years. Cancer Causes and Control. 2007;18(9):909–18. doi: 10.1007/s10552-007-9006-8. [DOI] [PubMed] [Google Scholar]
- Peipins LA, Miller J, Richards TB, Bobo JK, Liu T, White MC, Joseph D, Tangka F, Ekwueme DU. Characteristics of US Counties with No Mammography Capacity. Journal of Community Health. 2012;37(6):1239–48. doi: 10.1007/s10900-012-9562-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Radke J, Mu L. Spatial Decompositions, Modeling and Mapping Service Regions to Predict Access to Social Programs. Geographic Information Sciences. 2000;6(2):105–12. [Google Scholar]
- Rahman S, Price JH, Dignan M, Lindquist PS, Jordan TR. Access to Mammography Facilities and Detection of Breast Cancer by Screening Mammography: A GIS Approach. International Journal of Cancer Prevention. 2009;2(6):403–13. [PMC free article] [PubMed] [Google Scholar]
- Tan A, Kuo Y-F, Goodwin JS. Integrating Age and Comorbidity to Assess Screening Mammography Utilization. American Journal of Preventive Medicine. 2012;42(3):229–34. doi: 10.1016/j.amepre.2011.11.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services. 2010. Healthy People 2020: Topics and Objectives – Cancer” [accessed on January 18, 2013]. Available at http://www.healthypeople.gov/2020/topicsobjectives2020/overview.aspx?topicid=5. [DOI] [PubMed]
- U.S. Food and Drug Administration. 2012. Radiation-Emitting Products: Mammography Quality Standards Act and Program” [accessed on September 12, 2012]. Available at http://www.fda.gov/radiation-emittingproducts/mammographyqualitystandardsactandprogram/default.htm.
- U.S. General Accounting Office. 2002. Mammography: Capacity Generally Exists to Deliver Services” [accessed on January 18, 2013]. Available at http://www.gao.gov/new.items/d02532.pdf.
- U.S. Government Accountability Office. 2006. Mammography: Current Nationwide Capacity is Adequate, but Access Problems May Exist in Certain Locations” [accessed on January 18, 2013]. Available at http://www.gao.gov/assets/260/250848.pdf.
- U.S. Preventive Services Task Force. 2009. Screening for Breast Cancer” [accessed on August 22, 2012]. Available at http://www.uspreventiveservicestaskforce.org/uspstf/uspsbrca.htm.
- Wang F, McLafferty S, Escamilla V, Luo L. Late-Stage Breast Cancer Diagnosis and Health Care Access in Illinois. Professional Geographer. 2008;60(1):54–69. doi: 10.1080/00330120701724087. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Author Matrix.
Mammography Facilities.