

Abstract
AIM: To evaluate the usefulness of contrast-enhanced harmonic endoscopic ultrasound (CH-EUS) in differentiating between pancreatic adenocarcinomas and other pancreatic disease.
METHODS: This retrospective cohort study evaluated 90 patients who were seen between November 2010 and May 2013. All these patients had solid pancreatic masses that had a hypoechoic appearance on EUS. All patients underwent CH-EUS to evaluate this diagnostic method’s usefulness. The mass lesions observed on CH-EUS were classified into three categories based on their echo intensity: hypoenhanced, isoenhanced, and hyperenhanced lesions. We adjusted the sensitivity and the specificity of each category for detecting malignancies. We also estimated the accuracy of CH-EUS by comparing it to a pathological diagnosis.
RESULTS: Of the 90 patients, 62 had a pancreatic adenocarcinoma. Fifty-seven out of 62 pancreatic adenocarcinomas showed a hypoenhanced pattern on CH-EUS. The sensitivity was 92%, the specificity 68% and the accuracy approximately 82%. The area under the curve of the receiver operating characteristic analysis for CH-EUS was 0.799. There is a significant association between the hypoenhanced pattern on CH-EUS and pancreatic duct adenocarcinoma (χ2 = 35.264, P < 0.001). In pathological examinations, the number of specimens for EUS-fine needle aspiration (EUS-FNA) was considered insufficient for diagnosis in three patients, and in two patients, the results were reported to be negative for malignancy. Pancreatic masses in all five patients revealed a hypoenhanced pattern with CH-EUS. Three patients were diagnosed with pancreatic adenocarcinoma based on the pathology results of a biopsy, and the remaining two patients were clinically diagnosed with malignancy.
CONCLUSION: CH-EUS is useful for distinguishing between pancreatic adenocarcinoma and other pancreatic disease. When a pancreatic mass shows a hypoenhanced pattern on CH-EUS but involves either insufficient samples or negative results with EUS-FNA, clinicians might consider performing another pathologic diagnosis on the basis of an EUS-FNA sample or a biopsy.
Keywords: Pancreas neoplasm, Endoscopic ultrasound, SonoVue, Contrast media, Microbubbles
Core tip: This is a retrospective study of 90 patients with a pancreatic hypoechoic masses. We found that contrast-enhanced harmonic endoscopic ultrasound (CH-EUS) can be used for distinguishing between pancreatic adenocarcinoma (n = 62) and other pancreatic disease based on the hypoenhanced pattern on CH-EUS. When considering pancreatic adenocarcinomas as a tumor with a hypoenhanced pattern in CH-EUS and/or showing a positive result in EUS-fine needle aspiration, the sensitivity of detecting pancreatic malignancy increased to 100%.
INTRODUCTION
Endoscopic ultrasonography (EUS) is widely recognized as a diagnostic tool for pancreatic diseases and is superior to other modalities because of its good spatial resolution[1-3]. Tissue sample acquisition through EUS-guided fine-needle aspiration (EUS-FNA) could offer a clearer diagnosis of a pancreatic lesion[4]. However, differentiation between pancreatic tumors and inflammatory tumor-like masses is difficult[5]. Contrast-enhanced harmonic endoscopic ultrasonography (CH-EUS) is a novel technology that reveals not only parenchymal perfusion but also the microvasculature in the pancreas and aids in the differentiation of pancreatic neoplasia from other pancreatic disease[6,7]. Hirroka et al[8] described this new method with a preliminary study in 37 patients with pancreatic disease. This study showed that EUS-enhanced imagery is useful for the diagnosis of pancreatic disease. However, CH-EUS assessments suffered from the limitations caused by blooming artifacts, poor spatial resolution, and low sensitivity to slow flow[5,9]. To overcome these limitations, CH-EUS with a second-generation ultrasound contrast agent was recently developed. The second-generation contrast included a microbubble agent that can achieve good-quality perfusion imaging with harmonic EUS for evaluating the microvasculature of target lesions[10,11]. Therefore, we evaluated the efficacy of CH-EUS with a second-generation ultrasound contrast agent for assessing solid masses in the pancreas. We also estimated the role of CH-EUS as an additional diagnostic method for EUS in pancreatic neoplasia, which is difficult to confirm histologically. Furthermore, we tried to compare the sensitivity and the specificity of CH-EUS and EUS-FNA in the diagnosis of pancreatic neoplasia.
MATERIALS AND METHODS
Patients and equipment
We conducted a retrospective cohort study of 90 patients who presented with pancreatic masses and were seen at our facility from November 2010 to May 2013. These masses were heterogeneous and hypoechoic. Patients underwent CH-EUS to ascertain the character of the mass at the INHA University Hospital. A pathological examination was performed using EUS-FNA samples or on biopsy samples when malignancy was suspected. If the pancreatic mass was suspected to be either a benign or malignant neoplasia but was impossible to get a pathologic diagnosis of due to the location of mass or the inability to obtain specimens with EUS-FNA, the clinical course was tracked until a diagnosis could be confirmed. If a patient could not receive a proper pathologic diagnosis and was not tracked further, then the patient was excluded from this study. We also excluded patients if the mass was clearly revealed as a cystic lesion. Examination of the pancreas by conventional EUS and CH-EUS was performed by one endosonographer, Kim HK, who had conducted more than 8000 EUS procedures. An echoendoscope developed for CH-EUS (GF-UE260-AL5; Olympus Medical systems Co Ltd, Tokyo, Japan) was used. Ultrasound images were analyzed using an ALOKA Prosound Alpha10 processor (ALOKA, Tokyo, Japan). All images were analyzed and reviewed by one endosonographer. The extended pure harmonic detection (E-PHD) mode, which synthesizes receiving frequencies of filtered fundamental and second harmonic components with a transmitting frequency of 8 MHZ, was used for CH-EUS. The ultrasound contrast agent, Sonovue (Bracco international BV, Amsterdam, the Netherlands), was used for CH-EUS. This agent is a second-generation ultrasound contrast agent, consisting of microbubbles of sulfur hexafluoride coated with phospholipids.
Study design
Conventional EUS was performed on all patients. When conventional EUS revealed a mass-like lesion, the imaging mode was changed to the E-PHD mode. After changing to the E-PHD mode, a bolus of 2.4 mL of Sonovue was injected at a speed of 1 mL/s through an 18-gauge cannula placed in the antecubital vein. After infusion, the pancreas was imaged in a real-time fashion for a minimum of 90 s for complete observation of the arterial and venous phases. We observed changes of echo intensity in the mass lesions. If the pancreatic mass was not diagnosed with the first administration of Sonovue, a second dose of 2.4 mL Sonovue was administrated. The mass lesions were classified into three categories based on their echo intensity: hypoenhanced, isoenhanced, and hyperenhanced lesions[12]. This classification was based on the intensity of enhancement relative to the surrounding pancreatic tissue. Hypoenhancement is defined as a lower intensity of enhancement relative to the surrounding pancreatic tissue. Isoenhancement is defined as a similar intensity of enhancement relative to the surrounding pancreatic tissue. Hyperenhancement is defined as a higher intensity of enhancement relative to the surrounding pancreatic tissue (Figure 1). We interpreted the lesion following a modified classification of contrast-enhanced harmonic imaging of the pancreas by transabdominal ultrasound[12-14]. Adenocarcinomas usually have a distinct hypovascular appearance and are usually defined as lesions with hypoenhancement. The sensitivity and specificity of CH-EUS in diagnosing pancreatic adenocarcinoma were assessed. We also estimated the accuracy of CH-EUS in comparison with a pathologic diagnosis. To obtain specimens of the pancreatic mass, EUS-FNA was used initially. If specimen acquisition using EUS failed, pathological diagnoses were determined from a biopsy of a metastatic lesion from tissue such as the liver or the ampulla of Vater (hepatopancreatic ampulla). In one patient, a final diagnosis was made by a pathological examination of the patient’s abdominal effusion. When we did not get a proper specimen to confirm pancreatic disease, we traced the clinical course of patients until we could confirm the diagnosis of the disease.
Figure 1.
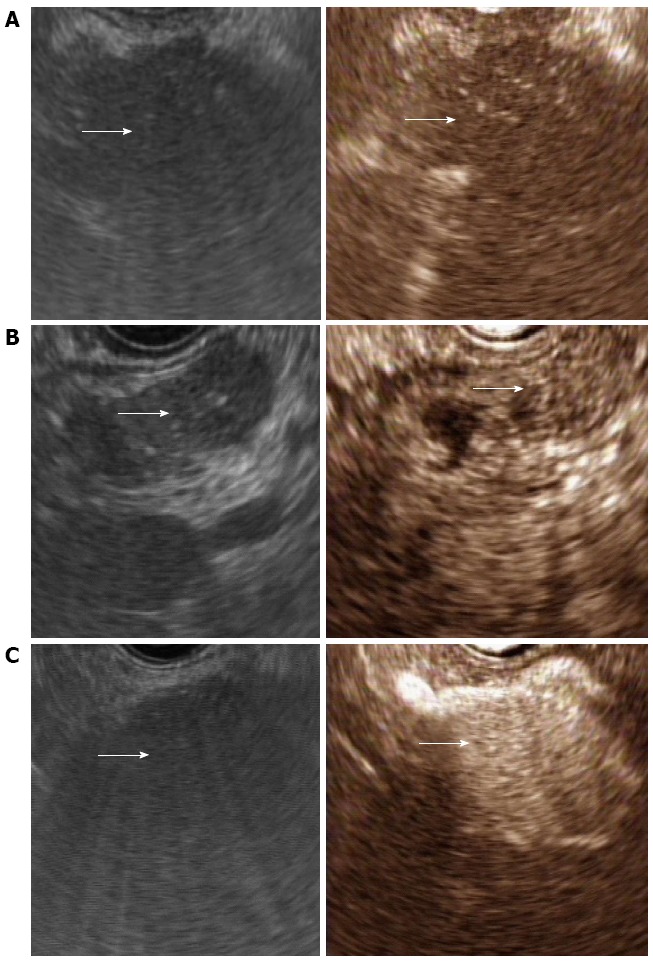
Conventional endoscopic ultrasonography (left) and contrast-enhanced harmonic endoscopic ultrasonography (right). These pictures showed a typical example of a hypoenhancement pattern (A), an isoenhancement pattern (B), and hyperenhancement pattern (C).
Ethics statement
The study protocol and amendments were approved by the Institutional Review Boards at our hospital (IUH-IRB 13-100).
Statistical analysis
All statistical analyses were performed using a statistical software package (SPSS 11.5 for Windows, SPSS, Inc, Chicago, IL, United States). Cross-tabular analyses were performed, accompanied by the chi-square test. Receiver operating characteristic analysis was performed to estimate the diagnostic accuracy of CH-EUS in pancreatic adenocarcinoma. The area under the curve (AUC) was calculated and the 95% confidence intervals (95%CI) were determined.
RESULTS
The sampling frame included 112 patients, and 22 patients who did not have a histological diagnosis were excluded. Sixteen of the 22 patients were lost to follow-ups. The remaining six patients had pancreatic masses accompanied with neoplasia originating at other sites, making it difficult to assess whether the pancreatic mass was metastatic or of pancreatic origin. This left 90 patients with a pancreatic mass who were enrolled. The median age of the study subjects was 63.5 years (range, 19-86 years) and the male:female ratio was about 2:1 (62:28 cases). The final diagnoses based on histological findings with EUS-FNA or surgical resection were pancreatic adenocarcinoma (n = 62), pancreatitis (n = 19), neuroendocrine tumor (n = 3), solid pseudopapillary tumor (n = 1), anaplastic carcinoma (n = 1), diffuse large B cell lymphoma (n = 1), and Castleman’s disease (n = 1). The clinically diagnosed malignancies applied to two cases in which EUS-FNA results were unsatisfactory or where insufficient specimens were obtained. Clinically diagnosed malignancy was defined as the pancreatic mass showing suspected malignancy in EUS on the basis of the echogenicity and morphology, or increasing tumor size during the tracking period. Positron emission tomography-computed tomography was performed in these patients and all pancreatic masses yielded positive results using this technique. These patients did not survive longer than 6 months after finding the pancreatic masses.
Of the 62 pancreatic ductal adenocarcinomas, 57 had a hypoenhanced pattern in CH-EUS. Two cases had isoenhanced patterns, and three cases had hyperenhanced patterns. Hypoenhanced patterns in CH-EUS had a high sensitivity (91.93%) for detecting pancreatic adenocarcinomas. The positive predictive value was 86.36%, the negative predictive value 79.16%, the specificity 67.85%, and the accuracy 84.45%. The AUC for pancreatic adenocarcinoma detected by hypoenhanced patterns on CH-EUS was 0.799. There is a significant association between hypoenhanced patterns on CH-EUS and pancreatic duct adenocarcinomas (χ2 = 35.264, P < 0.001). In contrast, pancreatitis comprised a large proportion of hyperenhanced pancreatic masses in CH-EUS (8/16). Two neuroendocrine tumors and three pancreatic adenocarcinomas were found to have a hyperenhanced pattern (Table 1). Five of the patients with pancreatic neoplasia could not be diagnosed with pancreatic neoplasia by EUS-FNA. Diagnoses could not be made in three of the patients due to insufficient samples. Two patients showed negative results in EUS-FNA. Three patients were diagnosed with a pancreatic adenocarcinoma by surgical resection. Two patients were diagnosed with pancreatic malignancy after a clinical follow-up. Interestingly, all of them had a hypoenhanced pattern on CH-EUS. Fifty-eight out of 90 patients underwent EUS-FNA. The sensitivity of the EUS-FNA in these 58 patients was 90.19% and the specificity 100%. When we assumed that pancreatic adenocarcinomas were the tumors with hypoenhanced patterns on CH-EUS and/or a positive result with EUS-FNA, the sensitivity with which pancreatic adenocarcinomas was diagnosed was 100% and the specificity 85.71% (Figure 2).
Table 1.
The vascular patterns of each pancreatic disease in contrast-enhanced harmonic endoscopic ultrasonography
| Total | Adenocarcinoma | Neuroendocrine tumor | Clinically diagnosed malignancy | Pancreatitis | Others | |
| Hypoenhancement | 66 | 57 | 1 | 2 | 6 | 0 |
| Isoenhancement | 8 | 2 | 0 | 0 | 5 | 1 |
| Hyperenhancement | 16 | 3 | 2 | 0 | 8 | 3 |
| Total | 62 | 3 | 2 | 19 | 4 |
Figure 2.
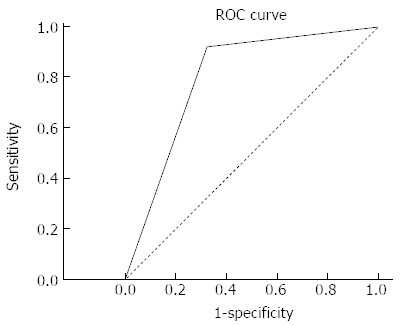
Receiver operating characteristic curve. Hypoenhancement pattern, determined by contrast-enhanced harmonic endoscopic ultrasonography, was calculated to diagnose pancreatic adenocarcinoma with the area under the receiver operating characteristic (ROC) curve of 0.799.
DISCUSSION
Pancreatic adenocarcinomas comprise over 90% of pancreatic tumors[15]. Pancreatic adenocarcinomas appear as heterogeneous hypoechoic masses with irregular margins on EUS[16]. The sensitivity of detecting pancreatic adenocarcinomas is 89%-100% in conventional EUS[17]. However, distinguishing pancreatic adenocarcinoma and benign disease such as a focal pancreatitis only on the basis of these EUS findings is difficult because both have similar morphology and echogenicity. In this situation, CH-EUS is useful to characterize pancreatic masses. When microbubbles in contrast agents are hit by an ultrasonic wave, the vibration creates a back-scattered acoustic shadow. The shadow is reproduced as an opacification. Vascular structures are highlighted as hyperechoic[4]. Thus, CH-EUS is able to evaluate the microvasculature of target lesions and parenchymal perfusion and can distinguish pancreatic neoplasia from benign pancreatic diseases[4,18]. According to Napoleon et al[19], CH-EUS can diagnose pancreatic adenocarcinoma with a high sensitivity (88%). Kitano et al[12] reported a similar result recently. They studied 277 patients with pancreatic solid lesions detected by conventional EUS who underwent CH-EUS for evaluation of the vascularity. CH-EUS depicted hypoenhancement of the masses diagnosed as pancreatic carcinomas with a sensitivity of 95.1% and specificity of 89.0%. Moreover, the microbubbles, which consists of gases other than air, in second-generation ultrasound contrast agents can be oscillated or broken by lower acoustic power[20-22]. Because of this, microvessels and parenchymal perfusion can be visualized to a greater extent than that achieved with CH-EUS using first-generation contrast agents, which have microbubbles of air[14,23,24]. According to a recent study, the sensitivity and specificity of CH-EUS with second-generation contrast agents in detection of pancreatic adenocarcinoma were 94% and 89%, respectively[20]. In the present study, when the pancreatic adenocarcinoma appeared as a mass with hypoenhancement on CH-EUS, the sensitivity was 91.93%, positive predictive value was 86.36%, negative predictive value 79.16%, specificity 67.85%, and accuracy 84.45%. Furthermore, there is a significant association between the hypo-enhancement pattern and pancreatic adenocarcinoma. Generally, pancreatic adenocarcinoma is regarded as a pancreatic mass showing a hypoenhancement pattern in CH-EUS. The reason why pancreatic cancer shows a hypoenhancement pattern on CH-EUS is that pancreatic cancer has a hypovascular structure and the mean vascular density of pancreatic adenocarcinoma is low and often inferior to that of the normal pancreatic parenchyma[25]. In addition, on pathological examination, the adenocarcinoma is characterized by the presence of marked desmoplasia, which justifies its hard consistency[26]. Because of these characteristics, the margins and size of the lesion are distinguished well with the surrounding enhanced normal pancreatic tissue[27]. In addition, microbubbles adopted in second-generation contrast agents do not leak out from blood vessels and the pancreatic adenocarcinoma is increasingly demarcated as a hypoenhanced lesion. Fusaroli et al[28] also reported that the hypoenhanced pancreatic mass is very sensitive and accurate for the prediction of adenocarcinoma (96% and 82%, respectively). This result was supported by our results. Therefore, we recommend that CH-EUS be performed upon pancreatic masses when it is difficult to distinguish pancreatic adenocarcinoma from other pancreatic diseases. It would be a helpful tool for diagnosis of pancreatic adenocarcinoma.
Although the sensitivity of EUS for pancreatic adenocarcinoma detection is very high, the diagnostic specificity is only 53%[29]. EUS-FNA is useful to overcome this specificity. The sensitivity of EUS-FNA for solid pancreatic masses reaches 95% with a specificity of 100%[30]. However, despite these advantages, negative EUS-FNA findings sometimes do not help determine whether a pancreatic mass requires surgery or follow-up, because of the possibility of false-negative findings.
In the course of Kitano’s study[12], there were five cases with false-negative EUS-FNA findings, but all these cases showed hypoenhancement patterns in CH-EUS. Likewise, five pancreatic malignancies in our study were not diagnosed as pathological malignancy with EUS-FNA. Interestingly, all those pancreatic masses showed hypoenhancement patterns using CH-EUS. All these masses were finally diagnosed as malignant through pathology results following surgical resection or clinical follow-up. When considering pancreatic adenocarcinomas as a tumor with a hypoenhancement pattern using CH-EUS and/or a positive result in EUS-FNA, the sensitivity of detecting pancreatic malignancy is increased to 100%.
Therefore, if CH-EUS reveals a hypoenhancement pattern in a pancreatic mass that showed negative or inconclusive results in EUS-FNA diagnostics, we recommend performing a pathological diagnosis again using EUS-FNA. If a second pathological diagnosis is impossible, we recommend observation of the clinical course to avoid missing a malignancy.
There were three cases of neuroendocrine tumors in our study. Two out of the three neuroendocrine tumors had hyperenhancement patterns, and the third had an isoenhancement pattern. Our result supported the finding that neuroendocrine tumors are hypervascular lesions using CH-EUS techniques with a sensitivity of 79%[12]. We surmise that the reason for isoenhancement patterns in neuroendocrine tumors is that the size of the tumor was too large (3.9 cm × 3.5 cm) to be accompanied by necrosis. Therefore, vascular structure was not visible on CH-EUS, and the mass was misinterpreted as an isoenhancement pattern. However, neuroendocrine tumors were too few to analyze in this study. Further studies with more patients are therefore required to investigate the characteristic features of neuroendocrine tumors using CH-EUS, and to estimate the diagnostic abilities of CH-EUS.
Our study has a few limitations. As our study is a retrospective single center study, selection bias is a possible problem. Secondly, the number of enrolled patients was too small to form a definite conclusion. Although our results were similar to those of other recent studies, and our study showed the possibilities of the use of CH-EUS for differential diagnoses in pancreatic disease, a large prospective study is required to reach a definite conclusion. Thirdly, our entire study was performed and reviewed by a single endoscopist. As a result, interpretation errors might be present in our study. In our study, the sensitivity and specificity of CH-EUS for detecting pancreatic adenocarcinoma were lower than those of the other studies[13,19,31]. We believe that these results are related to interpretation errors.
In conclusion, CH-EUS is a useful tool for the detection of pancreatic adenocarcinoma and differentiation between pancreatic malignancies and other pancreatic benign diseases. However, due to its low specificity, CH-EUS cannot be an alternative tool of EUS-FNA, which is used in the definitive diagnosis of pancreatic cancer. We recommend that a pathological diagnosis be performed on the lesion to reveal the hypoenhancement pattern in CH-EUS to avoid missing a malignancy.
COMMENTS
Background
One of the most important and challenging tasks of pancreatic endoscopic ultrasound is differentiation between pancreatic tumors and inflammatory tumor-like masses. Contrast-enhanced harmonic endoscopic ultrasonography (CH-EUS) is reported to improve diagnosis of pancreatic cancers. Nevertheless, CH-EUS suffers from limitations such as blooming artifacts, poor spatial resolution, and low sensitivity to slow flow. To overcome these, CH-EUS with a second-generation ultrasound contrast agent was recently developed.
Research frontiers
The microbubbles in the second-generation ultrasound contrast agent have a distinctive structure in comparison with those in first-generation agents. The microbubbles consist of gases other than air. Because of this, the microbubble can be oscillated or broken by lower acoustic power, allowing microvessels and parenchymal perfusion to be visualized to a greater extent than that achieved in CH-EUS with first-generation agents.
Innovations and breakthroughs
In the current study, CH-EUS was a very effective diagnostic tool for detection of pancreatic adenocarcinoma with the 92% sensitivity, 68% specificity, and 82% accuracy. This result is very similar with the results of previous reports. However, our result has a unique significance: it indicates the role of CH-EUS as an additional diagnostic tool for pancreatic adenocarcinoma. Five patients with suspected pancreatic cancer revealed hypoenhancement patterns in CH-EUS, but their diagnosis failed in the pathologic examination results of EUS-fine needle aspiration (EUS-FNA). As a result, three patients were diagnosed with pancreatic adenocarcinoma after surgical resection, and the remaining two patients were clinically diagnosed with malignancy.
Applications
This study suggested that CH-EUS is useful for distinction between pancreatic adenocarcinoma and other pancreatic disease and if the pancreatic mass reveals a hypoenhancement pattern in CH-EUS with negative results or insufficient samples in EUS-FNA, clinicians might consider performing a pathologic diagnosis again with EUS-FNA or surgical resection.
Terminology
Clinically diagnosed malignancy was defined if the pancreatic mass showed suspected malignancy in EUS on the basis of the echogenicity and morphology, or an increasing tumor size during the tracking period. Positron emission tomography-computed tomography was performed and all pancreatic masses in these patients yielded positive results in this examination. These patients did not survive longer than 6 mo after identification of the pancreatic masses.
Peer review
This is a good retrospective study in which the authors analyzed the efficacy of CH-EUS in diagnosis of pancreatic cancer. The result shows CH-EUS has the ability to distinguish pancreatic cancer from other pancreatic benign lesions and suggests that the presence of lesions showing a hypoenhancement pattern in CH-EUS may indicate pancreatic cancer.
Footnotes
Supported by An Inha University Research Grant
P- Reviewers: Ahmed F, Razek AAKA, Seicean A S- Editor: Gou SX L- Editor: A E- Editor: Liu XM
References
- 1.Rösch T, Lorenz R, Braig C, Feuerbach S, Siewert JR, Schusdziarra V, Classen M. Endoscopic ultrasound in pancreatic tumor diagnosis. Gastrointest Endosc. 1991;37:347–352. doi: 10.1016/s0016-5107(91)70729-3. [DOI] [PubMed] [Google Scholar]
- 2.Gress FG, Hawes RH, Savides TJ, Ikenberry SO, Cummings O, Kopecky K, Sherman S, Wiersema M, Lehman GA. Role of EUS in the preoperative staging of pancreatic cancer: a large single-center experience. Gastrointest Endosc. 1999;50:786–791. doi: 10.1016/s0016-5107(99)70159-8. [DOI] [PubMed] [Google Scholar]
- 3.Ngamruengphong S, Li F, Zhou Y, Chak A, Cooper GS, Das A. EUS and survival in patients with pancreatic cancer: a population-based study. Gastrointest Endosc. 2010;72:78–83, 83.e1-2. doi: 10.1016/j.gie.2010.01.072. [DOI] [PubMed] [Google Scholar]
- 4.Kongkam P, Ang TL, Vu CK, Dy FT, Yasuda K, Rerknimitr R, Varadarajulu S, Dhir V, Chong VH, Zhen DJ, et al. Current status on the diagnosis and evaluation of pancreatic tumor in Asia with particular emphasis on the role of endoscopic ultrasound. J Gastroenterol Hepatol. 2013;28:924–930. doi: 10.1111/jgh.12198. [DOI] [PubMed] [Google Scholar]
- 5.Xu C, Li Z, Wallace M. Contrast-enhanced harmonic endoscopic ultrasonography in pancreatic diseases. Diagn Ther Endosc. 2012;2012:786239. doi: 10.1155/2012/786239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Reddy NK, Ioncică AM, Săftoiu A, Vilmann P, Bhutani MS. Contrast-enhanced endoscopic ultrasonography. World J Gastroenterol. 2011;17:42–48. doi: 10.3748/wjg.v17.i1.42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Hocke M, Ignee A, Dietrich CF. Contrast-enhanced endoscopic ultrasound in the diagnosis of autoimmune pancreatitis. Endoscopy. 2011;43:163–165. doi: 10.1055/s-0030-1256022. [DOI] [PubMed] [Google Scholar]
- 8.Hirooka Y, Goto H, Ito A, Hayakawa S, Watanabe Y, Ishiguro Y, Kojima S, Hayakawa T, Naitoh Y. Contrast-enhanced endoscopic ultrasonography in pancreatic diseases: a preliminary study. Am J Gastroenterol. 1998;93:632–635. doi: 10.1111/j.1572-0241.1998.179_b.x. [DOI] [PubMed] [Google Scholar]
- 9.Hocke M, Dietrich CF. Vascularisation pattern of chronic pancreatitis compared with pancreatic carcinoma: results from contrast-enhanced endoscopic ultrasound. Int J Inflam. 2012;2012:420787. doi: 10.1155/2012/420787. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Romagnuolo J, Hoffman B, Vela S, Hawes R, Vignesh S. Accuracy of contrast-enhanced harmonic EUS with a second-generation perflutren lipid microsphere contrast agent (with video) Gastrointest Endosc. 2011;73:52–63. doi: 10.1016/j.gie.2010.09.014. [DOI] [PubMed] [Google Scholar]
- 11.Kannengiesser K, Mahlke R, Petersen F, Peters A, Ross M, Kucharzik T, Maaser C. Contrast-enhanced harmonic endoscopic ultrasound is able to discriminate benign submucosal lesions from gastrointestinal stromal tumors. Scand J Gastroenterol. 2012;47:1515–1520. doi: 10.3109/00365521.2012.729082. [DOI] [PubMed] [Google Scholar]
- 12.Kitano M, Kudo M, Yamao K, Takagi T, Sakamoto H, Komaki T, Kamata K, Imai H, Chiba Y, Okada M, et al. Characterization of small solid tumors in the pancreas: the value of contrast-enhanced harmonic endoscopic ultrasonography. Am J Gastroenterol. 2012;107:303–310. doi: 10.1038/ajg.2011.354. [DOI] [PubMed] [Google Scholar]
- 13.Kitano M, Kudo M, Maekawa K, Suetomi Y, Sakamoto H, Fukuta N, Nakaoka R, Kawasaki T. Dynamic imaging of pancreatic diseases by contrast enhanced coded phase inversion harmonic ultrasonography. Gut. 2004;53:854–859. doi: 10.1136/gut.2003.029934. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Săftoiu A, Dietrich CF, Vilmann P. Contrast-enhanced harmonic endoscopic ultrasound. Endoscopy. 2012;44:612–617. doi: 10.1055/s-0032-1308909. [DOI] [PubMed] [Google Scholar]
- 15.Klöppel G, Maillet B. Histological typing of pancreatic and periampullary carcinoma. Eur J Surg Oncol. 1991;17:139–152. [PubMed] [Google Scholar]
- 16.Lee SH, Ozden N, Pawa R, Hwangbo Y, Pleskow DK, Chuttani R, Sawhney MS. Periductal hypoechoic sign: an endosonographic finding associated with pancreatic malignancy. Gastrointest Endosc. 2010;71:249–255. doi: 10.1016/j.gie.2009.08.023. [DOI] [PubMed] [Google Scholar]
- 17.DeWitt J, Devereaux B, Chriswell M, McGreevy K, Howard T, Imperiale TF, Ciaccia D, Lane KA, Maglinte D, Kopecky K, et al. Comparison of endoscopic ultrasonography and multidetector computed tomography for detecting and staging pancreatic cancer. Ann Intern Med. 2004;141:753–763. doi: 10.7326/0003-4819-141-10-200411160-00006. [DOI] [PubMed] [Google Scholar]
- 18.Krishna SG, Lee JH. Endosonography in solid and cystic pancreatic tumors. J Interv Gastroenterol. 2011;1:193–201. doi: 10.4161/jig.1.4.19971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Napoleon B, Alvarez-Sanchez MV, Gincoul R, Pujol B, Lefort C, Lepilliez V, Labadie M, Souquet JC, Queneau PE, Scoazec JY, et al. Contrast-enhanced harmonic endoscopic ultrasound in solid lesions of the pancreas: results of a pilot study. Endoscopy. 2010;42:564–570. doi: 10.1055/s-0030-1255537. [DOI] [PubMed] [Google Scholar]
- 20.Kitano M, Sakamoto H, Kudo M. Contrast-enhanced endoscopic ultrasound. Dig Endosc. 2013:Epub ahead of print. doi: 10.1111/den.12179. [DOI] [PubMed] [Google Scholar]
- 21.Lee TY, Cheon YK, Shim CS. Clinical role of contrast-enhanced harmonic endoscopic ultrasound in differentiating solid lesions of the pancreas: a single-center experience in Korea. Gut Liver. 2013;7:599–604. doi: 10.5009/gnl.2013.7.5.599. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Matsumoto K, Kato H, Tomoda T, Sakakihara I, Noma Y, Yamamoto N, Sonoyama T, Tsutsumi K, Sadamori H, Okada H, et al. [Two cases of lymphoepithelial cyst of the pancreas confirmed by contrast-enhanced endoscopic ultrasound] Nihon Shokakibyo Gakkai Zasshi. 2013;110:1823–1830. [PubMed] [Google Scholar]
- 23.Gheonea DI, Streba CT, Ciurea T, Săftoiu A. Quantitative low mechanical index contrast-enhanced endoscopic ultrasound for the differential diagnosis of chronic pseudotumoral pancreatitis and pancreatic cancer. BMC Gastroenterol. 2013;13:2. doi: 10.1186/1471-230X-13-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hocke M, Dietrich CF. [Contrast-enhanced endoscopic ultrasound in the diagnosis of pancreatic diseases] Dtsch Med Wochenschr. 2013;138:732–734. doi: 10.1055/s-0032-1332963. [DOI] [PubMed] [Google Scholar]
- 25.Matsubara H, Itoh A, Kawashima H, Kasugai T, Ohno E, Ishikawa T, Itoh Y, Nakamura Y, Hiramatsu T, Nakamura M, et al. Dynamic quantitative evaluation of contrast-enhanced endoscopic ultrasonography in the diagnosis of pancreatic diseases. Pancreas. 2011;40:1073–1079. doi: 10.1097/MPA.0b013e31821f57b7. [DOI] [PubMed] [Google Scholar]
- 26.Kitano M, Sakamoto H, Matsui U, Ito Y, Maekawa K, von Schrenck T, Kudo M. A novel perfusion imaging technique of the pancreas: contrast-enhanced harmonic EUS (with video) Gastrointest Endosc. 2008;67:141–150. doi: 10.1016/j.gie.2007.07.045. [DOI] [PubMed] [Google Scholar]
- 27.D'Onofrio M, Zamboni G, Faccioli N, Capelli P, Pozzi Mucelli R. Ultrasonography of the pancreas. 4. Contrast-enhanced imaging. Abdom Imaging. 2007;32:171–181. doi: 10.1007/s00261-006-9010-6. [DOI] [PubMed] [Google Scholar]
- 28.Fusaroli P, Spada A, Mancino MG, Caletti G. Contrast harmonic echo-endoscopic ultrasound improves accuracy in diagnosis of solid pancreatic masses. Clin Gastroenterol Hepatol. 2010;8:629–634.e1-2. doi: 10.1016/j.cgh.2010.04.012. [DOI] [PubMed] [Google Scholar]
- 29.Brand B, Pfaff T, Binmoeller KF, Sriram PV, Fritscher-Ravens A, Knöfel WT, Jäckle S, Soehendra N. Endoscopic ultrasound for differential diagnosis of focal pancreatic lesions, confirmed by surgery. Scand J Gastroenterol. 2000;35:1221–1228. doi: 10.1080/003655200750056736. [DOI] [PubMed] [Google Scholar]
- 30.Eloubeidi MA, Jhala D, Chhieng DC, Chen VK, Eltoum I, Vickers S, Mel Wilcox C, Jhala N. Yield of endoscopic ultrasound-guided fine-needle aspiration biopsy in patients with suspected pancreatic carcinoma. Cancer. 2003;99:285–292. doi: 10.1002/cncr.11643. [DOI] [PubMed] [Google Scholar]
- 31.Ogura T, Masuda D, Kurisu Y, Ohama H, Imoto A, Takii M, Takeuchi T, Inoue T, Tokioka S, Umegaki E, et al. Splenic artery aneurysm masquerading as a pancreatic tumor--diagnosis by contrast-enhanced endoscopic ultrasound. Endoscopy. 2012;44 Suppl 2 UCTN:E428–E429. doi: 10.1055/s-0032-1325861. [DOI] [PubMed] [Google Scholar]