

Abstract
The human lacrimal gland is an essential component of the lacrimal functional unit (LFU). Any perturbation of this unit can lead to the debilitating morbid condition called the dry eye syndrome (DES). The current line of therapy available for dry eye remains supportive and palliative with the patient being dependent on life long and frequent administration of lubricating eye drops. Even advanced therapies like punctual plugs, cyclosporine B administration, and salivary gland auto-transplantation have led to a limited success. Under these scenarios, the option of cell based therapy needs to be explored to provide better and long term relief to these patients. This review gives an overview of the efforts in lacrimal gland regeneration and examines the past and ongoing research in cell based therapies in animals as well as human lacrimal gland cultures. The authors discuss their first of its kind functionally viable human lacrimal gland in vitro culture system from fresh exenteration specimens. A brief overview of research in near future and the potential implications of lacrimal gland regenerative therapies have been discussed.
Keywords: Lacrimal gland, Regeneration, Dry eye, Stem cells
Introduction
The human lacrimal gland is an essential component of the lacrimal functional unit (LFU) which comprises of the lacrimal gland, the ocular surface (cornea, conjunctiva and the meibomian gland) and the associated sensory and motor nerves (Figure 1). The LFU controls the secretion of the major components of the tear film and is overall responsible for maintaining the stability of the tear film, transparency of the cornea and the quality of the image projected onto the retina.1
Figure 1.
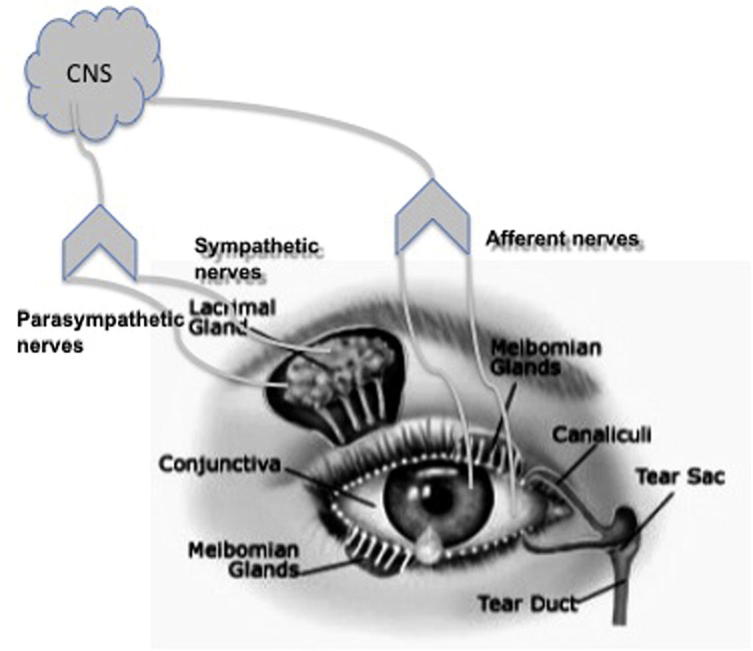
The lacrimal functional unit.
Any perturbation in the stability of the tear film leads to destabilization of the ocular surface which, over a period of time, can lead to the debilitating morbid condition called the dry eye syndrome (DES). The composition of the tear film can be altered due to the dysfunction of either the lacrimal gland or the meibomian glands; however for the purpose of this review we will restrict our discussion to lacrimal gland dysfunction. Lacrimal gland dysfunction and destruction is seen in cases of advancing age, autoimmune disorders, orbital radiotherapy, low androgen pool etc. This lacrimal dysfunction causes hyperosmolarity of tear film resulting in a vicious loop of ocular surface inflammation which is responsible for ocular epithelial damage leading to corneal ulceration and eventual decline in visual acuity.1
The current line of therapy available for dry eye remains supportive and palliative with the patient being dependent on life long, frequent administration of lubricating or hydrating eye drops. Even advanced therapies like punctal plugs, cyclosporine B administration, and salivary gland auto-transplantation have led to a limited success. Under these scenarios, the option of cell based therapy needs to be explored to provide better and long term relief to these patients.
Histology, anatomy and physiology
The lacrimal gland is a tubulo-acinar exocrine gland that consists of secretory columnar epithelium arranged in a lobular pattern. These secretory acinar cells empty their secretions into ducts that anastomose into larger excretory ducts which drain onto the ocular surface. Both the acinar and the ductal cells have numerous vesicles in their apical portion while the base is associated with a basement matrix. Enveloping the secretory acinar cells are myoepithelial cells that contract and squeeze them enabling the draining of the secretory components into the ducts. Between the lacrimal lobes are fibroblasts, which produce the collagen and matrix of interstitial spaces, and mast cells, which secrete histamine and heparin. In addition to this basic tissue architecture, the lacrimal gland is highly inundated with trafficking B and T lymphocytes as well as plasma cells.2
The lacrimal gland has both the sympathetic as well as parasympathetic innervation.3 These nerves have a large number of cholinergic fibers and fewer adrenergic fibers. The parasympathetic postganglionic neural cell bodies are found in the pterygopalatine (sphenopalatine) ganglion as well as the ciliary ganglion. Sympathetic fibers arise in the superior cervical ganglion. There is also some sensory innervation of the gland from the trigeminal ganglia.4
The lacrimal gland secretes a number of proteins like lysozyme, lactoferrin, lipocalin, and scIgA.5 The secretion of these proteins is regulated by the nerves and their associated neurotransmitters or neuropeptides.2 The important receptors present on the lacrimal gland are acetylcholine receptors like muscarinic M3, vasoactive intestinal peptide types I and II and norepinephrine receptors like alpha 1 and beta.6 Other receptors present are for interacting with neuropeptide Y, adrenocorticotrophic hormone (ACTH) and alpha- melanocyte stimulating hormone (MSH). Since the epithelial cells of the gland are extensively coupled by junctional complexes, secondary messengers like inositol triphosphate can easily diffuse between cells and activate the unstimulated cells too.2
The dry eye syndrome
The International Dry Eye Workshop, 20071 defined dry eye as:
“Dry eye is a multifactorial disease of the tears and ocular surface that results in symptoms of discomfort, visual disturbances and tears film instability with potential damage to the ocular surface. It is accompanied by increased osmolarity of tear film and inflammation of the ocular surface.”
Dry eye is associated with a high incidence of ocular morbidity. The current prevalence of dry eye in the world is estimated at around 11% to 22%.7 In the Indian context, these numbers are estimated to be around 18.4–20%.8, 9 These epidemiological numbers are a good indicator of the need for research on dry eye syndrome.
The etiology of DES involves a vicious loop of tear hyperosmolarity, tear film instability and ocular surface inflammation.10 In addition to this, there is also loss of anti-inflammatory environment within the gland which may happen in cases of low androgen pool. Severe dry eye is also seen in patients of Sjogren’s syndrome in which auto-antigens are expressed at the surface of the epithelial cells. These cause homing and retention of tissue specific CD4 and CD8 cells, leading to immune-mediated destruction of the acinar and ductal components.
Orbital radiation therapy, which is a commonly used modality in the treatment of oculo-adenexal disorders including malignant tumors, has also been implicated in the development of DES in patients. Despite a rapid evolution in the field of radiotherapy over the past years, a significant number of patients are still seen with acute and chronic ophthalmic complications including severe dry eye.11, 12 Preliminary data from our institute indicate that chronic dry eye develops in over 49% of the patients who undergo external beam radiation therapy for ocular malignancies (unpublished data).
Contact lens wear is yet another condition that may lead to the development of severe dry eye in long-term users. Reduced corneal sensitivity and tear film hyperosmolarity are the probable underlying mechanisms.1
The current treatment modalities available for DES are lubricating agents like hydroxymethyl cellulose, solutions containing bicarbonates and potassium, hyposmotic artificial tears and artificial serum. In cases of severe dry eye, therapies such as anti-inflammatory medications (cyclosporin A, corticosteroids), pharmacological tear stimulants like diquafosol, rebamipide, ecabet sodium, pilocarpine etc. have also been used. In certain severe cases, surgical interventions like punctal occlusion and salivary gland auto-transplantation are done to slow down the progress of the condition and minimize detrimental sequale.13
On recommendation of the committee on the therapy and management of dry eye, the treatment or management protocol for this condition is now shifting toward employing strategies that would increase the natural production of tears, maintain ocular surface integrity and reduce or eliminate the levels of existing inflammation.13 With these objectives in mind various therapeutic avenues are being explored with the inclusion of cell therapy for restoring the function of the damaged lacrimal gland.
Lacrimal gland regeneration
Currently available data on the etiopathogenesis and treatment of dry eye are still insufficient to explain how alteration in tear film composition can cause such a vicious cycle of tear film instability and chronic ocular inflammation. Even though a lot of research is being directed toward profiling the proteins, lipids and other constituents of human tear yet there is a glaring lack of comparative data between normal individuals and dry eye patients.
Animal lacrimal gland in vitro cultures
An important area of investigation in this field is to find a common link between tear film osmolarity, tear film break up response and the resultant inflammatory stress. In order to facilitate these studies, not just in vivo models but also in vitro models are being developed that would greatly assist the investigation into the secretory repertoire of lacrimal gland epithelia, regulation of secretion and etiopathogenesis of lacrimal gland involvement in disorders like Sjogren’s syndrome.
Past two decades have seen evolution in the procedure for in vitro culturing of lacrimal gland acinar cells. Oliver et al.14 published one of the first reports on in vitro culture of rat lacrimal gland acinar cells wherein they described a method for culturing a dividing population of morphologically differentiated rat lacrimal acinar cells on a three-dimensional, reconstituted basement membrane gel. The cultured acinar cells proliferated on the basement matrix and showed the presence of cytoplasmic secretory granules.14 However, their culture system could only maintain the epithelial cells for 6–7 days after which fibroblast overgrowth was observed. Successful in vitro culture of lacrimal acinar cells was first achieved and published by Meneray and Rismondo in two separate reports in 1994.15, 16 Reports from Hann et al.17 and numerous subsequent authors have emphasized the importance of media formulation, supplement profile and extracellular matrix composition for optimal growth and functionality of lacrimal acinar cells.
A major problem faced by all these investigators was that the lacrimal acinar cells could not be induced to proliferate significantly in vitro until Schonthal et al.18 in 2000 improvised on the media composition by the use of epidermal growth factor (EGF), dihydrotestosterone (DHT), Matrigel™ and HepatoStim™ culture medium.18 A number of recent publications also report the use of polyethersulfone dead-end tube19, denuded amniotic membrane20 as scaffolds and rotary cell culture system21 for successful in vitro culture of rat or rabbit lacrimal glands. The effect of androgens and androgen analogs on in vitro culture of lacrimal acinar cells has helped elucidate the control that the androgens exert on the synthesis and secretion of secretory component17, 22, 23, 24 as well as other biochemical parameters related to the lacrimal secretion including the basal tear flow rate.25
The culture systems developed for the lacrimal acinar cells have also been optimized to assess the functionality of these cells. The currently employed conditions for the in vitro culture of these secretory cells support the in vivo mimicry of their secretion pattern as elucidated by the detection of scIgA, lactoferrin, lysozyme, lacritin and a number of other tear proteins in the culture supernatant.
You et al.26 showed that post injection of interleukin into the mouse lacrimal gland which destroys areas in the gland, stem-like cells migrate toward the site of injury and heal the wound. These cells could also be harvested and grown under in vitro conditions. However, the authors report minimum in vitro growth from uninjured gland. In contrast, the recent study by Shatos et al.27 on rat lacrimal gland and our own experience with human lacrimal gland tissue28 showed that stem-like cells are present in the native, uninjured gland too which can be maintained under appropriate in vitro conditions.
Human lacrimal gland in vitro cultures – our experience
In-vitro work on human lacrimal gland cultures is scarce, possibly due to the difficulty in obtaining human tissue for research. To the best of our knowledge and literature search, there is just one report published by Yoshino et al.29 in 2000, which dealt with establishing human lacrimal cultures from cadaveric tissue. However, the study was a limited report which only partially explored the secretory potential of the cells and the various sub-populations present.
Our group has been working with human lacrimal gland cultures since 2008 and we were the first to report the establishment of functionally viable human lacrimal gland in vitro cultures from fresh exenteration specimens.28 Our results show successful establishment of human lacrimal gland cultures on three matrices: Matrigel™, collagen-1 and denuded human amniotic membrane. We have extensively characterized our culture system using markers for epithelial, myoepithelial and mesenchymal origin by immunohistochemistry/immunocytochemistry and flow cytometry. Our established cultures show the capacity to synthesize and secrete quantifiable levels of major tear proteins like scIgA, lactoferrin and lysozyme into the culture supernatant. We have successfully shown that these lacrimal epithelial cultures can be maintained in vitro, with intact secretory function, for a minimum period of 21 days. In addition, we also reported that by day 16–18, these in vitro cultures show the appearance of ‘spherules’ and structures that look like ductal connections between them (Figure 2). We believe that this indicates their potential for in vitro gland formation.
Figure 2.

Human lacrimal gland in vitro cultures: phase contrast microscope images.
Toward the long-term goal of cell therapy in chronic dry eye condition, we have also looked for the presence of stem-like cells in the native human lacrimal gland as well as in the established cultures. From the criteria available, we have used ABCG2, CD117 positivity and ALDH levels, clone formation ability, quiescence and label retaining properties to indicate the presence of stem-like cells.
Using flow cytometry and immunochemistry we have shown preliminary evidence indicating the presence of stem-like cells (ABCG2 positive, ALDH high) in the native human lacrimal gland as well as in our in vitro cultures. In the native gland around 3.1 ± 0.61% of the cells showed ABCG2 positivity and around 3.8 ± 1.26% showed high levels of ALDH (Figure 3). In the in vitro cultures, the number of cells that showed ABCG2 positivity by day 14 is 0.3 ± 0.15%, which decreased slightly to 0.2 ± 0.13% by day 21. Similar is the case with ALDH. CD117, which is a stem cell marker in exocrine glands, also showed positivity: at time = 0 about 6.7 ± 2.0% of the cells were CD117 positive. This number reduced to 0.2 ± 0.05 by day 14 and 0.2 ± 0.05 by day 21 in vitro (Figure 4)
Figure 3.

FACS analysis of fresh human lacrimal gland cells.
Figure 4.

FACS analysis of cultured human lacrimal gland cells.
In order to enrich the number of stem cells in vitro we have also cultured these cells as free floating ‘lacrispheres’ which are very similar to salispheres and prostaspheres. These spheres show a fourfold increase in CD117 positive cells (0.8%), increased clone forming ability and higher percentage of label retaining cells than the adherent cultures (unpublished data).
We believe that these lacrispheres are very similar in their phenotype as well as cellular architecture to salispheres. Since the latter is being used as a potential cell therapy for restoring function in animal model of xerostomia,30 we believe similar results could be expected from lacrispheres too.
Conclusion
Even though we have come a long way in managing the chronic dry eye patients and improving their quality of life, yet there are a number of aspects that still need to be looked at and addressed. One of the principle areas that need focused attention is to understand the mechanisms behind the development and progression of this condition and to develop biomarker(s) for this condition. A large, well-defined, staged and age-matched study would probably be required for this.
A lot of fundamental science we know of dry eye today has been by correlating animal data with human scenario. In order to lend credibility to the accrued knowledge, it is essential that a comparative study be made between human and mouse or rabbit tears and ocular surface protein–lipid profiles. This would enable us to identify the common components and pathways involved in various forms of this disorder and would also give important clues about the treatment of this condition.
The last couple of years have seen an increase in the knowledge about the presence of stem-like cells in the lacrimal gland of mice,26 rat27 and humans.28 These studies indicate the inherent potential of the gland to heal itself following an insult. In contrast, the recent study by Shatos et al.27 on rat lacrimal gland and our own experience with human lacrimal gland showed that stem-like cells are present in the native, uninjured gland too which can be maintained under appropriate in vitro conditions.
Another important area that needs to be explored carefully is the potential to use cell therapy in chronic cases of dry eye. Cell therapy is being used successfully to treat a similar condition called xerostomia involving the salivary gland under preclinical settings.30 Even though there is not enough work that has been done toward cell therapy in dry eye, yet its similarity with salivary gland leads us to believe that a similar therapeutic approach may prove beneficial to the chronic patients of dry eye too (Figure 5).
Figure 5.

Potential cell therapy for aqueous deficient dry eye.
The presence of stem cells in the lacrimal gland is an important finding that leads us to believe that these cells can be recruited to salvage the damaged gland. However, before we take a leap of faith, the viability, homing and functionality of these cells need to be established by more extensive in vitro studies and independent animal experimentation. Subsequent use of cell based therapies to rescue and regenerate diseased lacrimal gland in humans is a promising prospect.
Funding agencies
IAEA, DBT, HERF, C-Tracer, Sudhakar and Sreekanth Ravi Brothers.
Financial disclosure
None.
Method of literature search
A search of Pubmed database (1979-till date) was conducted. Medline and Ophthalmic literature databases were also searched. The following key words were used: Lacrimal gland/lacrimal in vitro studies/dry eye syndrome. Additional sources include review of publications cited in other articles. Google search was also used to find publication that may be missed in the above databases.
Conflict of interest
The authors declared that there is no conflict of interest.
Footnotes
Peer review under responsibility of Saudi Ophthalmological Society, King Saud University.

References
- 1.The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye Workshop (2007). The ocular surface 2007;5:75–92. [DOI] [PubMed]
- 2.Walcott B. The lacrimal gland and its veil of tears. News Physiol Sci. 1998;13:97–103. doi: 10.1152/physiologyonline.1998.13.2.97. [DOI] [PubMed] [Google Scholar]
- 3.Matsumoto Y., Tanabe T., Ueda S. Immunohistochemical and enzymehistochemical studies of peptidergic, aminergic and cholinergic innervation of the lacrimal gland of the monkey (Macaca fuscata) J Auton Nerv Syst. 1992;37:207–214. doi: 10.1016/0165-1838(92)90042-f. [DOI] [PubMed] [Google Scholar]
- 4.Van der Werf F., Baljet B., Prins M. Innervation of the lacrimal gland in the cynomolgous monkey: a retrograde tracing study. J Anat. 1996;188:591–601. [PMC free article] [PubMed] [Google Scholar]
- 5.Tiffany J.M. The normal tear film. Dev Ophthalmol. 2008;41:1–20. doi: 10.1159/000131066. [DOI] [PubMed] [Google Scholar]
- 6.Mauduit P., Jammes H., Rossignol B. M3 muscarinic acetylcholine receptor coupling to PLC in rat exorbital lacrimal acinar cells. Am J Physiol. 1993;264:1550–1560. doi: 10.1152/ajpcell.1993.264.6.C1550. [DOI] [PubMed] [Google Scholar]
- 7.Abelson M.B., Ousler G.W., Maffei C. Dry eye in 2008. Curr Opin Ophthalmol. 2009;20:282–286. doi: 10.1097/ICU.0b013e32832b7578. [DOI] [PubMed] [Google Scholar]
- 8.Gupta N., Prasad I., Himashree G. Prevalence of dry eye at high altitude: a case controlled comparative study. High Alt Med Biol. 2008;9:327–334. doi: 10.1089/ham.2007.1055. [DOI] [PubMed] [Google Scholar]
- 9.Sahai A., Malik P. Dry eye: prevalence and attributable risk factors in a hospital-based population. Indian J Ophthalmol. 2005;53:87–91. doi: 10.4103/0301-4738.16170. [DOI] [PubMed] [Google Scholar]
- 10.Gilbard J.P., Rossi S.R., Heyda K.G. Ophthalmic solutions, the ocular surface, and a unique therapeutic artificial tear formulation. Am J Ophthalmol. 1989;107:348–355. doi: 10.1016/0002-9394(89)90657-0. [DOI] [PubMed] [Google Scholar]
- 11.Alberti W. Acute and late side effects of radiotherapy for ocular disease: an overview. Front Radiat Ther Oncol. 1997;30:281–286. doi: 10.1159/000425714. [DOI] [PubMed] [Google Scholar]
- 12.Durkin S.R., Roos D., Higgs B. Ophthalmic and adnexal complications of radiotherapy. Acta Ophthalmol Scand. 2007;85:240–250. doi: 10.1111/j.1600-0420.2006.00822.x. [DOI] [PubMed] [Google Scholar]
- 13.Management and therapy of dry eye disease: report of the Management and Therapy Subcommittee of the International Dry Eye Workshop (2007). The ocular surface 2007;5:163–178. [DOI] [PubMed]
- 14.Oliver C., Waters J.F., Tolbert C.L. Growth of exocrine acinar cells on a reconstituted basement membrane gel. In Vitro Cell Dev Biol. 1987;23:465–473. doi: 10.1007/BF02628416. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Meneray M.A., Fields T.Y., Bromberg B.B. Morphology and physiologic responsiveness of cultured rabbit lacrimal acini. Invest Ophthalmol Vis Sci. 1994;35:4144–4158. [PubMed] [Google Scholar]
- 16.Rismondo V., Gierow J.P., Lambert R.W. Rabbit lacrimal acinar cells in primary culture: morphology and acute responses to cholinergic stimulation. Invest Ophthalmol Vis Sci. 1994;35:1176–1183. [PubMed] [Google Scholar]
- 17.Hann L.E., Kelleher R.S., Sullivan D.A. Influence of culture conditions on the androgen control of secretory component production by acinar cells from the rat lacrimal gland. Invest ophthalmol Vis Sci. 1991;32:2610–2621. [PubMed] [Google Scholar]
- 18.Schonthal A.H., Warren D.W., Stevenson D. Proliferation of lacrimal gland acinar cells in primary culture. Stimulation by extracellular matrix, EGF, and DHT. Exp Eye Res. 2000;2000(70):639–649. doi: 10.1006/exer.2000.0824. [DOI] [PubMed] [Google Scholar]
- 19.Long L., Liu Z., Wang T. Polyethersulfone dead-end tube as a scaffold for artificial lacrimal glands in vitro. J Biomed Mater Res B Appl Biomater. 2006;78:409–416. doi: 10.1002/jbm.b.30502. [DOI] [PubMed] [Google Scholar]
- 20.Schrader S., Wedel T., Kremling C. Amniotic membrane as a carrier for lacrimal gland acinar cells. Graefes Arch Clin Exp Ophthalmol. 2007;245:1699–1704. doi: 10.1007/s00417-007-0612-7. [DOI] [PubMed] [Google Scholar]
- 21.Schrader S., Kremling C., Klinger M. Cultivation of lacrimal gland acinar cells in a microgravity environment. Br J Ophthalmol. 2009;93:1121–1125. doi: 10.1136/bjo.2008.137927. [DOI] [PubMed] [Google Scholar]
- 22.Kelleher R.S., Hann L.E., Edwards J.A. Endocrine, neural, and immune control of secretory component output by lacrimal gland acinar cells. J Immunol. 1991;146:3405–3412. [PubMed] [Google Scholar]
- 23.Sullivan D.A., Bloch K.J., Allansmith M.R. Hormonal influence on the secretory immune system of the eye: androgen control of secretory component production by the rat exorbital gland. Immunology. 1984;52:239–246. [PMC free article] [PubMed] [Google Scholar]
- 24.Sullivan D.A., Kelleher R.S., Vaerman J.P. Androgen regulation of secretory component synthesis by lacrimal gland acinar cells in vitro. J Immunol. 1990;145:4238–4244. [PubMed] [Google Scholar]
- 25.Azzarolo A.M., Mircheff A.K., Kaswan R.L. Androgen support of lacrimal gland function. Endocrine. 1997;6:39–45. doi: 10.1007/BF02738800. [DOI] [PubMed] [Google Scholar]
- 26.You S., Kublin C.L., Avidan O. Isolation and propagation of mesenchymal stem cells from the lacrimal gland. Invest Ophthalmol Vis Sci. 2011;52:2087–2094. doi: 10.1167/iovs.10-5686. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Shatos M.A., Haugaard-Kedstrom L., Hodges R.R. Isolation and characterization of progenitor cells in uninjured, adult rat lacrimal gland. Invest Ophthalmol Vis Sci. 2012;53:2749–2759. doi: 10.1167/iovs.11-9025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tiwari S., Ali M.J., Balla M.M. Establishing human lacrimal gland cultures with secretory function. PloS one. 2012;7:e29458. doi: 10.1371/journal.pone.0029458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Yoshino K. Establishment of a human lacrimal gland epithelial culture system with in vivo mimicry and its substrate modulation. Cornea. 2000;19:S26–S36. doi: 10.1097/00003226-200005001-00007. [DOI] [PubMed] [Google Scholar]
- 30.Lombaert I.M., Brunsting J.F., Wierenga P.K. Rescue of salivary gland function after stem cell transplantation in irradiated glands. PloS One. 2008;3:e2063. doi: 10.1371/journal.pone.0002063. [DOI] [PMC free article] [PubMed] [Google Scholar]