

Abstract
Oncology acupuncture has become a new and promising field of research because more and more cancer patients have sought non-pharmacological alternatives for symptom management. While different mechanisms have been proposed to explain its efficacy, including theories of the neural system, endocrine cytokine or immunological regulation, its eventual role has become that of alleviating the side effects induced by chemotherapy or radiotherapy. In this paper, we have reviewed the related articles focusing on acupuncture mechanisms and applications in cancer care to provide a quick sketch of acupuncture in cancer care. A detailed search was performed to identify the randomized controlled trials (RCTs) and systematic reviews on acupuncture in oncology, using PUBMED and Cochrane. The search terms included: Acupuncture, acupressure, and cancer. Additional terms were used to target specific symptoms (i.e., breast cancer, hot flash, xerostomia, nausea, vomiting, cancer pain, insomnia, fatigue). Two authors independently extracted data for analysis and review. Ultimately, 25 articles underwent full-text review. Recent trials made efforts in studying (a) hot flashes in breast cancer, (b) xerostomia induced by radiotherapy in head and neck cancer, (c) nausea and vomiting post-chemotherapy, (d) cancer pain, and (e) fatigue and insomnia in cancer patients. Controversial results for acupuncture application in cancer care appeared in different categories, but a trend emerged that acupuncture can palliate cancer-related symptoms. The research to date certainly offers us a valid complementary therapy in treating cancer-related symptoms. Meanwhile, practical strategies with safe measures for enhancing the efficacy are needed in further interventions, as well as continuing research with a validated methodology.
Keywords: Acupuncture, Cancer, Oncology
INTRODUCTION
With the increasing incidence of cancer and major advances in cancer treatment in recent decades, acupuncture has become a popular complementary treatment in oncology. One European survey highlighted over a third of cancer patients are utilizing complementary therapies for treating their cancer symptoms and/or the side effects of their treatment.[1] Since different cancer patients often share similar symptoms, most complementary therapies are focused on the symptoms rather than the disease itself. Oncology acupuncture is a new field of research. Recent advances from published clinical trials have added evidence to support the use of acupuncture for management of symptoms such as pain, nausea and vomiting, xerostomia, hot flashes, fatigue, anxiety, depression, and insomnia. Acupuncture is based on the meridian theory of Traditional Chinese Medicine and stresses “Qi.” From the viewpoint of western medicine, the mechanism of acupuncture may be explained by neurotransmitter release or modulation of autonomic nervous system (ANS). Recent studies also used sham acupuncture control groups to validate the efficacy of acupuncture.[2] Applying acupuncture in oncology requires constant dialog and communication between qualified practitioners and the oncology team.
Here, we review some review articles and clinical trials including patient-administered acupuncture, electroacupuncture (EA), acupressure, and auricular acupuncture applied in cancer-related symptom treatment. Most studies indicate acupuncture has the potential to act as an adjunctive care in palliating symptoms.[2] This has encouraged deeper investigations and clinical practice to apply this technique in cancer care because of its low side-effect profile and economic cost benefits.
Theory and mechanism
In Traditional Chinese Medicine theory, acupoints are defined as the visceral reaction points on the body surface where the Qi of the viscera and meridians are transfused.
Triggering these acupuncture points promotes the flow of Qi and blood, and regulates visceral function.[3]
In the last half of the 20th century, many studies conducted in animals and humans have demonstrated multiple biological responses related to acupuncture, including (a) neural regulation, (b) endocrine regulation, and (c) immunological regulation.[4]
In neural regulation, some experiments have indicated the relationship between acupuncture and the ANS.[5] According to Traditional Chinese Medicine, “acupuncture is believed to restore the balance of Yin and Yang,” which may correspond to the modern definition that “acupuncture modulates the imbalance between the parasympathetic and sympathetic activity.”[6]
In endocrine regulation, EA evokes serotonin release from the upper brain stem region and hypothalamus and stimulates endogenous opiate release (β-endorphin, enkephalin, endomorphin, and dynorphin) which then alleviates cancer pain.[7] In addition, some neurohormones like γ-aminobutyric acid and glutamate, neuropeptide Y, and brain-derived neurotrophic factors can lead to euphoric sensations and treat the psychological problems of the cancer patients.[8,9]
From the view point of immune modulation, EA may stimulate leukocytes’ (granulocytes and lymphocytes) growth via the hypo-thalamus–pituitary–adrenal axis.[10] Improvements in T-lymphocyte and Natural Killer cell function to promote the recovery of immune function in cancer patients were observed in some studies.[11,12]
METHODS
Our search for articles of acupuncture in the management of each symptom was carried out on 15 September 2012 in the database PUBMED and in the Cochrane Central Register of Controlled Trials. Language restricted to English were applied. Key search terms were: Acupuncture, electroacupuncture, acupressure, and cancer. Additional terms were used to target specific symptoms (i.e., breast cancer, hot flashes, xerostomia, nausea, vomiting, cancer pain, insomnia, fatigue). References of all the included studies were also searched.
Selection criteria
We included only the recent reviews and randomized controlled trials (RCTs) investigating acupuncture applied in cancer-related symptoms within the past 8 years.
Data collection and analysis
Two independent reviewers screened the abstracts and titles of all the articles for eligibility. When the reviewers felt that the abstract or title was potentially useful, full copies of the article were retrieved and considered for eligibility by all reviewers.
When discrepancies occurred between reviewers, the reasons were identified and a final decision was made based on the agreement of all reviewers. In the end, 25 articles, including RCTs and systemic reviews, were retrieved for the final analysis [Figure 1]. And the major conclusions of included RCTs and systemic reviews in acupuncture applied in cancer-related symptoms would be summarized in Table 1. The common acupoints applied in oncology-related problem would be list in Table 2.
Figure 1.
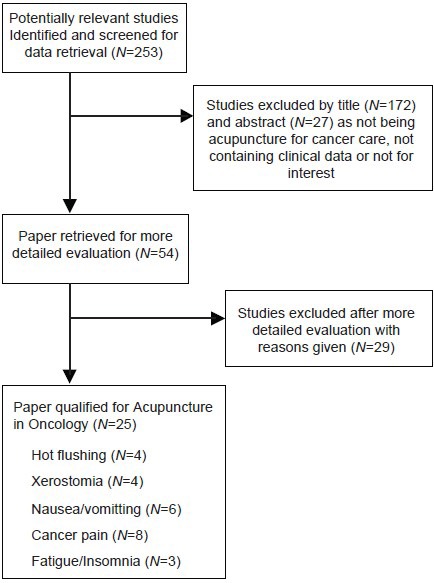
Reviewing process flowchart
Table 1.
Recent RCT and systemic reviews in acupuncture applied in cancer-related symptoms
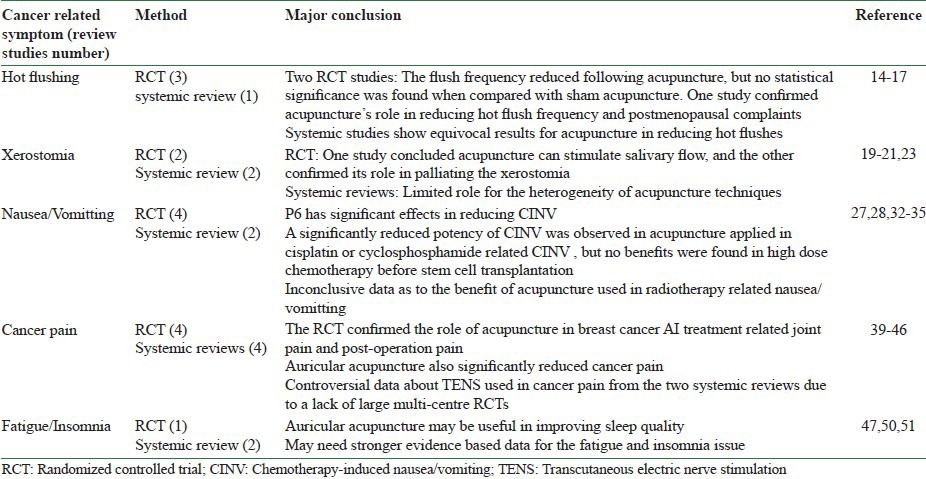
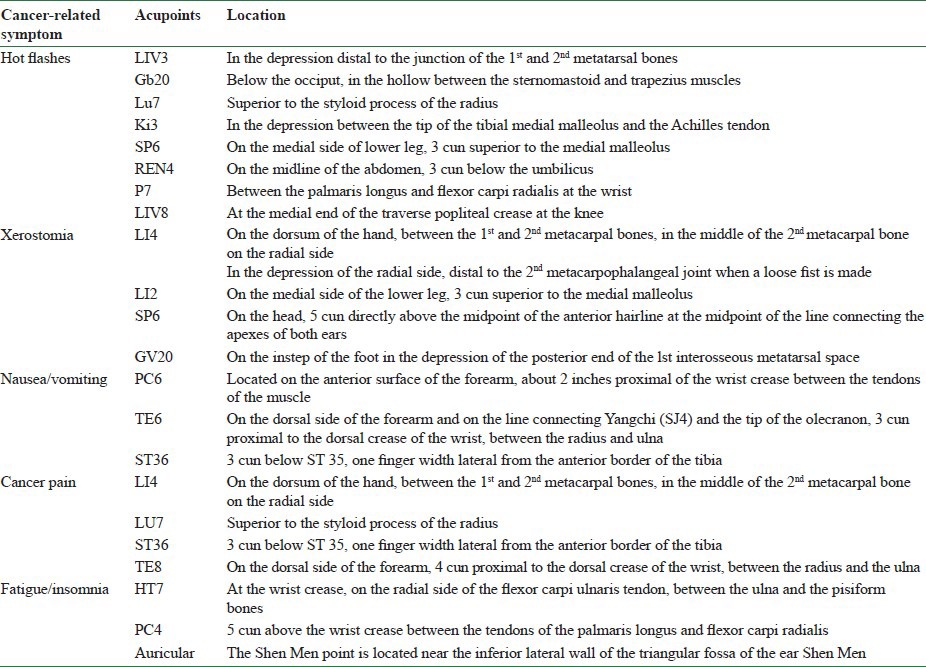
Table 2.
Common acupoints applied in cancer care
ACUPUNCTURE APPLIED IN ONCOLOGY-RELATED PROBLEM
Hot flashes
Hot flashes are a common complaint in nearly 70% of breast cancer patients.[13] They may be related to abrupt menopause or anti-estrogen therapy (tamoxifen or aromatase inhibitors). Acupuncture (a complementary modality) plays some role in reducing the hot flashes in breast cancer patients on treatment with accompanying side effects. Two recent RCT studies showed acupuncture may decrease the frequency of hot flashes, but not to a statistically significant level when compared with sham acupuncture.[14,15] Another RCT enrolled breast cancer patients who had all taken tamoxifen for more than 3 months, and compared the Kupperman index and frequency of hot flashes between the patients who received true acupuncture (TA) and those who received sham acupuncture (SA). A significant benefit was found in this study.[16] A systemic review indicated evidence from sham-controlled RCTs for the limited effects of acupuncture in treating hot flashes in breast cancer patients, and more pharmacologic agents, including megestrol acetate, clonidine, and selective serotonin reuptake inhibitors (SSRI), need to be tested.[16,17] Although the mechanism is uncertain, it is hypothesized that neurotransmitters are involved in thermoregulation.[18]
Xerostomia
Radiation-induced xerostomia is a common symptom in patients with head and neck cancer (HNC) because radiotherapy fields frequently encompass the major salivary glands. Once the accumulated dose exceeds 26 Gy, the radiation damage to salivary gland tissue is difficult to reverse. The dry mouth sensation definitely influences a patient's quality of life (QoL). Thus, some conventional modalities that have been applied include (a) salivary replacement treatment, (b) mechanical and pharmacological stimulants, (c) cholinergic muscarinic agonist (pilocarpine), and (d) improved radiation dosimetry. In recent years, “acupuncture” has received much more attention stemming from a hypothesis that acupuncture may stimulate salivary flow accompanied by corresponding central nervous system (CNS) functional magnetic resonance imaging (fMRI) changes in radiation-induced xerostomia.[19] Some systemic reviews have given evidence indicating that acupuncture's benefit in irradiation-induced xerostomia is limited and further high-quality RCTs are still needed.[20,21] A recent non-RCT study showed preventive acupuncture led to significantly improved salivary flow rates and decreased xerostomia-related symptoms,[22] and another RCT by David reported significant reduction in pain, dysfunction, and xerostomia with good tolerance.[23] The possible mechanism for palliating xerostomia using acupuncture may be related to the neuropeptides modulating the salivary secretion in a complex process orchestrated by both the sensory and the autonomic nervous systems.[24]
Nausea/vomiting
Both ASCO (American Society of Clinical Oncology) and NCCN (National Comprehensive Cancer Network) state the 5-hydroxytryptamine (5HT3) antagonists and neurokinin 1 (NK1)-receptor antagonist can reduce chemotherapy-induced nausea/vomiting (CINV). However, there are still many patients who cannot tolerate these symptoms because they deeply impair the patients’ QoL and delay the chemotherapy course.[25] Application of acupuncture in cancer-related nausea/vomiting has been studied since 1990s.[26] In 1998, the National Institutes of Health Consensus Statement on Acupuncture noted that promising results have emerged showing the efficacy of acupuncture in adult postoperative and chemotherapy-induced nausea and vomiting. A review article indicated the benefits of EA in chemotherapy-induced acute vomiting, but studies combining EA with state-of-the-art antiemetics and in patients with refractory symptoms are needed to determine the clinical relevance.[27] The most popular acupoints applied in this problem are P6 and S36, both of which belong to the Chinese stomach meridian.[28] Improving vagal modulation and HRV (Heart rate variability) change were observed to be related to reducing post-chemotherapy nausea/vomiting.[29] Several acupuncture studies have applied different chemotherapy regimes such as cisplatin or cyclophosphamide. They revealed that acupuncture combined with antiemetics can effectively decrease the incidence and degree of cisplatin- and cyclophosphamide-induced delayed nausea and vomiting and that the effect of acupuncture is better than that of sham acupuncture.[30,31] Two multicenter longitudinal RCTs have also shown significant benefits of acupuncture in alleviating the severity of both acute and delayed vomiting.[32,33]
However, there have still been negative results of acupuncture on CINV. A randomized controlled single-blind trial that focused on high-dose chemotherapy and autologous peripheral blood stem cell transplantation showed no benefit from acupuncture.[34]
Therefore, the effect in radiotherapy-induced nausea/vomiting is not conclusive, as there are both positive and negative results.[35,36]
Cancer pain
Cancer pain is a refractory symptom in oncology. The World Health Organization suggested managing pain should begin with the use of time-honored opioids, but it also recommends the use of adjuvant therapies such as acupuncture and other complementary and alternative modalities early in the management process.[37] The main mechanism of the analgesic effect of acupuncture may be related to its effect in decreased substance P and upregulating plasma β-endorphin levels.[38] Since there are various manual approaches to acupuncture, there is no definite conclusion as to its effectiveness. A systemic review of RCTs evaluating any type of invasive acupuncture for cancer pain indicated insufficient evidence to judge whether acupuncture is effective, due to methodological limitations, small sample sizes, poor reporting, and inadequate analysis.[39] Meanwhile, a meta-analysis showed Transcutaneous Electric Nerve Stimulation (TENS) may have a role in pain management, but there was insufficient available evidence to determine its effectiveness in treating cancer-related pain.[40,41] However, closer inspection shows positive results, for example, a randomized controlled blind study with 90 patients found auricular acupuncture may significantly reduce pain intensity from cancer patients who are in pain, despite stable analgesic treatment.[42] Providing massage and acupuncture in addition to usual care also resulted in decreased pain among postoperative cancer patients, when compared with usual care alone.[43] Similar significant benefits were also observed in RCTs comparing true body and auricular acupuncture with the sham group, concluding acupuncture can relieve Aromatase inhibitors induced arthralgia and joint stiffness.[44,45] This is because cancer pain may arise not only from cancer itself, but also from cytokine or other related treatments. More focused and rigorous, methodological quality studies are necessary to assess the clinical efficacy of acupuncture for cancer pain.[46]
Fatigue/insomnia
Cancer-related fatigue is a multidimensional phenomenon that is self-perceived, and includes physical, emotional, cognitive, and behavioral components. It is usually accompanied by symptoms such as depression and insomnia. As part of complementary therapy, acupuncture has been studied in this field for several decades. A methodologically feasible RCT compared acupuncture, acupressure, and sham acupressure in post-chemotherapy fatigue patients and found positive results in enhancing patients’ general fatigue (P < 0.001), physical fatigue (P = 0.016), activity (P = 0.004), and motivation (P = 0.024).[47] A single-arm, phase II pilot study showed clinically meaningful results in improving post-chemotherapy fatigue with acupuncture.[48] On the other hand, insomnia may lead to fatigue and depression, which are also commonly observed in cancer patients. A recent RCT evaluated 80 patients and revealed acupuncture can effectively reduce malignant-related depression and improve the sleep quality of cancer patients.[49] A meta-analysis also indicated auricular acupuncture may improve sleep quality better than medications such as diazepam.[50] However, studies focused on cancer-related fatigue and insomnia are difficult to clearly understand because many confounding factors need to be considered. A Cochrane systematic review of acupuncture for insomnia concluded, “The current evidence is not sufficiently extensive or rigorous enough to support the use of any form of acupuncture for treating insomnia.”[51] The data so far show acupuncture causes sedative and hypnotic effects in cancer patients when used for treating nervousness and insomnia. Further methodologically strong, randomized controlled studies with a large sample size are needed to assess the usefulness of acupuncture for cancer-related fatigue and insomnia.
Side effects and complication management
The safety issues concerning oncology acupuncture practice have become imperative, since cancer patients usually have a more complicated medical status and are at higher risk of developing adverse reactions from acupuncture. Patients with coagulation dysfunction or severe thrombocytopenia with a bleeding tendency should be paid special attention. In patients with a cardiac pacemaker or intracardiac defibrillator, EA should be avoided. Direct insertion of needle into a tumor nodule or ulcerated wound, as well as lymphedematous limbs should be avoided. Sterile needles are obligatory. Severe adverse effects of acupuncture are rare and easily handled, such as a small hemorrhage, fainting, or syncope, bruising, dizziness, needle breakage, pneumothorax, or nerve damage. A multicentric survey from Germany observed that if it is used according to the established safety rules and carefully at appropriate anatomic regions, it is a safe treatment method.[52]
Based on our experience, patients with sepsis or those in shock are unsuitable for acupuncture. Other conditions caused due to treatment, such as cancer-related neutropenia [absolute neutrophil count (ANC) <500/μl] or thrombocytopenia (platelet < 20,000/μl), as well as immune-compromised condition or major co-morbidities should always be kept in mind. Before the first visit, approval and communication should be obtained from the patients and the primary oncologist.
THE PERSPECTIVE ROLE OF ACUPUNCTURE IN ONCOLOGY
The increase in the overall survival of cancer patients is attributed to the rapid progress of cancer treatment modalities. More and more attention has been focused on complementary and alternative medicine. Acupuncture is a well-established technique in this field. Many studies showed benefits of the technique to multiple cancer-related symptoms, as discussed above. Note, however, that the study design with respect to the study population, sample size, methodological quality, mode of TENS, treatment duration, method of administration, and outcome measures used was not uniform and some equivocal conclusions were reached. Based on the holistic cancer care viewpoint and current RCT data, the clinical application and study of acupuncture in oncology should be simultaneously evaluated. To be more persuasive, standardized clinical protocols, and the types and points of acupuncture for each symptom should be elucidated and investigated further. As encouraging evidence continues to emerge, acupuncture could play a more prominent role in integrative cancer care.
ACKNOWLEDGMENTS
The authors would like to thank the team members of the National Yang-Ming University, School of Medicine, Institute of Traditional Medicine for their participation.
REFERENCES
- 1.Molassiotis A, Fernadez-Ortega P, Pud D, Ozden G, Scott JA, Panteli V, et al. Use of complementary and alternative medicine in cancer patients: A European survey. Ann Oncol. 2005;16:655–63. doi: 10.1093/annonc/mdi110. [DOI] [PubMed] [Google Scholar]
- 2.Sagar SM. Acupuncture as an evidence-based option for symptom control in cancer patients. Curr Treat Options Oncol. 2008;9:117–26. doi: 10.1007/s11864-008-0063-3. [DOI] [PubMed] [Google Scholar]
- 3.Rong P, Zhu B, Li Y, Gao X, Ben H, Li Y, et al. Mechanism of acupuncture regulating visceral sensation and mobility. Front Med. 2011;5:151–6. doi: 10.1007/s11684-011-0129-7. [DOI] [PubMed] [Google Scholar]
- 4.Moritaka K, Zeredo JL, Kimoto M, Nasution FH, Hirano T, Toda K. Response properties of nucleus reticularis lateralis neurons after electroacupuncture stimulation in rats. Am J Chin Med. 2010;38:869–80. doi: 10.1142/S0192415X10008317. [DOI] [PubMed] [Google Scholar]
- 5.Carpenter RJ, Dillard J, Zion AS, Gates GJ, Bartels MN, Downey JA, et al. The acute effects of acupuncture upon autonomic balance in healthy subjects. Am J Chin Med. 2010;38:839–47. doi: 10.1142/S0192415X10008287. [DOI] [PubMed] [Google Scholar]
- 6.Takahashi T. Mechanism of acupuncture on neuromodulation in the gut: A review. Neuromodulation. 2011;14:8–12. doi: 10.1111/j.1525-1403.2010.00295.x. [DOI] [PubMed] [Google Scholar]
- 7.Lin JG, Chen WL. Acupuncture analgesia: A review of its mechanisms of actions. Am J Chin Med. 2008;36:635–45. doi: 10.1142/S0192415X08006107. [DOI] [PubMed] [Google Scholar]
- 8.Yu LL, Liu RP, Gao XY, Liu K, Li L, Ben H, et al. Development of studies on neurochemical mechanism of acupuncture underlying improvement of depression. Zhen Ci Yan Jiu. 2011;36:383–7. [PubMed] [Google Scholar]
- 9.Wang XJ, Wang LL. A mechanism of endogenous opioid peptides for rapid onset of acupuncture effect in treatment of depression. Zhong Xi Yi Jie He Xue Bao. 2010;8:1014–7. doi: 10.3736/jcim20101102. [DOI] [PubMed] [Google Scholar]
- 10.Mori H, Nishijo K, Kawamura H, Abo T. Unique immunomodulation by electro-acupuncture in humans possibly via stimulation of the autonomic nervous system. Neurosci Lett. 2002;320:21–4. doi: 10.1016/s0304-3940(02)00012-5. [DOI] [PubMed] [Google Scholar]
- 11.Zhang SY, Du YQ. Effects of warming needle moxibustion on improvement of gastrointestinal and immune function in patients with postoperation of colorectal cancer. Zhongguo Zhen Jiu. 2011;31:513–7. [PubMed] [Google Scholar]
- 12.Kim SK, Bae H. Acupuncture and immune modulation. Auton Neurosci. 2010;157:38–41. doi: 10.1016/j.autneu.2010.03.010. [DOI] [PubMed] [Google Scholar]
- 13.Carpenter JS, Andrykowski MA, Cordova M, Cunningham L, Studts J, McGrath P, et al. Hot flashes in postmenopausal women treated for breast carcinoma: Prevalence, severity, correlates, management, and relation to quality of life. Cancer. 1998;82:1682–91. [PubMed] [Google Scholar]
- 14.Kim DI, Jeong JC, Kim KH, Rho JJ, Choi MS, Yoon SH, et al. Acupuncture for hot flushes in perimenopausal and postmenopausal women: A randomised, sham-controlled trial. Acupunct Med. 2011;29:249–56. doi: 10.1136/aim.2011.004085. [DOI] [PubMed] [Google Scholar]
- 15.Deng G, Vickers A, Yeung S, D’Andrea GM, Xiao H, Heerdt AS, et al. Randomized, controlled trial of acupuncture for the treatment of hot flashes in breast cancer patients. J Clin Oncol. 2007;25:5584–90. doi: 10.1200/JCO.2007.12.0774. [DOI] [PubMed] [Google Scholar]
- 16.Hervik J, Mjaland O. Acupuncture for the treatment of hot flashes in breast cancer patients, a randomized, controlled trial. Breast Cancer Res Treat. 2009;116:311–6. doi: 10.1007/s10549-008-0210-3. [DOI] [PubMed] [Google Scholar]
- 17.Lee MS, Kim KH, Choi SM, Ernst E. Acupuncture for treating hot flashes in breast cancer patients: A systematic review. Breast Cancer Res Treat. 2009;115:497–503. doi: 10.1007/s10549-008-0230-z. [DOI] [PubMed] [Google Scholar]
- 18.Borud EK, Alraek T, White A, Fonnebo V, Grimsgaard S. The effect of TCM acupuncture on hot flushes among menopausal women (ACUFLASH) study: A study protocol of an ongoing multi-centre randomised controlled clinical trial. BMC Complement Altern Med. 2007;7:6. doi: 10.1186/1472-6882-7-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Deng G, Hou BL, Holodny AI, Cassileth BR. Functional magnetic resonance imaging (fMRI) changes and saliva production associated with acupuncture at LI-2 acupuncture point: A randomized controlled study. BMC Complement Altern Med. 2008;8:37. doi: 10.1186/1472-6882-8-37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.O’Sullivan EM, Higginson IJ. Clinical effectiveness and safety of acupuncture in the treatment of irradiation-induced xerostomia in patients with head and neck cancer: A systematic review. Acupunct Med. 2010;28:191–9. doi: 10.1136/aim.2010.002733. [DOI] [PubMed] [Google Scholar]
- 21.Jedel E. Acupuncture in xerostomia: A systematic review. J Oral Rehabil. 2005;32:392–6. doi: 10.1111/j.1365-2842.2005.01445.x. [DOI] [PubMed] [Google Scholar]
- 22.Braga FP, Lemos CA, Junior, Alves FA, Migliari DA. Acupuncture for the prevention of radiation-induced xerostomia in patients with head and neck cancer. Braz Oral Res. 2011;25:180–5. doi: 10.1590/s1806-83242011000200014. [DOI] [PubMed] [Google Scholar]
- 23.Pfister DG, Cassileth BR, Deng GE, Yeung KS, Lee JS, Garrity D, et al. Acupuncture for pain and dysfunction after neck dissection: Results of a randomized controlled trial. J Clin Oncol. 2010;28:2565–70. doi: 10.1200/JCO.2009.26.9860. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Dawidson I, Angmar-Mansson B, Blom M, Theodorsson E, Lundeberg T. The influence of sensory stimulation (acupuncture) on the release of neuropeptides in the saliva of healthy subjects. Life Sci. 1998;63:659–74. doi: 10.1016/s0024-3205(98)00317-8. [DOI] [PubMed] [Google Scholar]
- 25.Osoba D, Zee B, Warr D, Latreille J, Kaizer L, Pater J. Effect of postchemotherapy nausea and vomiting on health-related quality of life. The Quality of Life and Symptom Control Committees of the National Cancer Institute of Canada Clinical Trials Group. Support Care Cancer. 1997;5:307–13. doi: 10.1007/s005200050078. [DOI] [PubMed] [Google Scholar]
- 26.Dundee JW, Ghaly RG, Bill KM, Chestnutt WN, Fitzpatrick KT, Lynas AG. Effect of stimulation of the P6 antiemetic point on postoperative nausea and vomiting. Br J Anaesth. 1989;63:612–8. doi: 10.1093/bja/63.5.612. [DOI] [PubMed] [Google Scholar]
- 27.Ezzo JM, Richardson MA, Vickers A, Allen C, Dibble SL, Issell BF, et al. Acupuncture-point stimulation for chemotherapy-induced nausea or vomiting. Cochrane Database Syst Rev. 2006;2 doi: 10.1002/14651858.CD002285.pub2. CD002285. [DOI] [PubMed] [Google Scholar]
- 28.Ezzo J, Streitberger K, Schneider A. Cochrane systematic reviews examine P6 acupuncture-point stimulation for nausea and vomiting. J Altern Complement Med. 2006;12:489–95. doi: 10.1089/acm.2006.12.489. [DOI] [PubMed] [Google Scholar]
- 29.Streitberger K, Ezzo J, Schneider A. Acupuncture for nausea and vomiting: An update of clinical and experimental studies. Auton Neurosci. 2006;129:107–17. doi: 10.1016/j.autneu.2006.07.015. [DOI] [PubMed] [Google Scholar]
- 30.Lao L, Zhang G, Wong RH, Carter AK, Wynn RL, Berman BM. The effect of electroacupuncture as an adjunct on cyclophosphamide-induced emesis in ferrets. Pharmacol Biochem Behav. 2003;74:691–9. doi: 10.1016/s0091-3057(02)01069-9. [DOI] [PubMed] [Google Scholar]
- 31.Sima L, Wang X. Therapeutic effect of acupuncture on cisplatin-induced nausea and vomiting. Zhongguo Zhen Jiu. 2009;29:3–6. [PubMed] [Google Scholar]
- 32.Dibble SL, Luce J, Cooper BA, Israel J, Cohen M, Nussey B, et al. Acupressure for chemotherapy-induced nausea and vomiting: A randomized clinical trial. Oncol Nurs Forum. 2007;34:813–20. doi: 10.1188/07.ONF.xxx-xxx. [DOI] [PubMed] [Google Scholar]
- 33.Molassiotis A, Helin AM, Dabbour R, Hummerston S. The effects of P6 acupressure in the prophylaxis of chemotherapy-related nausea and vomiting in breast cancer patients. Complement Ther Med. 2007;15:3–12. doi: 10.1016/j.ctim.2006.07.005. [DOI] [PubMed] [Google Scholar]
- 34.Streitberger K, Friedrich-Rust M, Bardenheuer H, Unnebrink K, Windeler J, Goldschmidt H, et al. Effect of acupuncture compared with placebo-acupuncture at P6 as additional antiemetic prophylaxis in high-dose chemotherapy and autologous peripheral blood stem cell transplantation: A randomized controlled single-blind trial. Clin Cancer Res. 2003;9:2538–44. [PubMed] [Google Scholar]
- 35.Enblom A, Johnsson A, Hammar M, Onelov E, Steineck G, Borjeson S. Acupuncture compared with placebo acupuncture in radiotherapy-induced nausea: A randomized controlled study. Ann Oncol. 2012;23:1353–61. doi: 10.1093/annonc/mdr402. [DOI] [PubMed] [Google Scholar]
- 36.Enblom A, Lekander M, Hammar M, Johnsson A, Onelöv E, Ingvar M, et al. Getting the grip on nonspecific treatment effects: Emesis in patients randomized to acupuncture or sham compared to patients receiving standard care. PLoS One. 2011;6:e14766. doi: 10.1371/journal.pone.0014766. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Running A, Seright T. Integrative Oncology: Managing cancer pain with complementary and alternative therapies. Curr Pain Headache Rep May. 2012;16:325–31. doi: 10.1007/s11916-012-0275-x. [DOI] [PubMed] [Google Scholar]
- 38.Lee HJ, Lee JH, Lee EO, Lee HJ, Kim KH, Lee KS, et al. Substance P and beta endorphin mediate electroacupuncture induced analgesic activity in mouse cancer pain model. Acupunct Electrother Res. 2009;34:27–40. doi: 10.3727/036012909803861095. [DOI] [PubMed] [Google Scholar]
- 39.Paley CA, Johnson MI, Tashani OA, Bagnall AM. Acupuncture for cancer pain in adults. Cochrane Database Syst Rev. 2011;1 doi: 10.1002/14651858.CD007753.pub2. CD007753. [DOI] [PubMed] [Google Scholar]
- 40.Robb K, Oxberry SG, Bennett MI, Johnson MI, Simpson KH, Searle RD. A cochrane systematic review of transcutaneous electrical nerve stimulation for cancer pain. J Pain Symptom Manage. 2009;37:746–53. doi: 10.1016/j.jpainsymman.2008.03.022. [DOI] [PubMed] [Google Scholar]
- 41.Hurlow A, Bennett MI, Robb KA, Johnson MI, Simpson KH, Oxberry SG. Transcutaneous electric nerve stimulation (TENS) for cancer pain in adults. Cochrane Database Syst Rev. 2012;3 doi: 10.1002/14651858.CD006276.pub3. CD006276. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Alimi D, Rubino C, Pichard-Leandri E, Fermand-Brule S, Dubreuil-Lemaire ML, Hill C. Analgesic effect of auricular acupuncture for cancer pain: A randomized, blinded, controlled trial. J Clin Oncol. 2003;21:4120–6. doi: 10.1200/JCO.2003.09.011. [DOI] [PubMed] [Google Scholar]
- 43.Mehling WE, Jacobs B, Acree M, Wilson L, Bostrom A, West J, et al. Symptom management with massage and acupuncture in postoperative cancer patients: A randomized controlled trial. J Pain Symptom Manage. 2007;33:258–66. doi: 10.1016/j.jpainsymman.2006.09.016. [DOI] [PubMed] [Google Scholar]
- 44.Crew KD, Capodice JL, Greenlee H, Brafman L, Fuentes D, Awad D, et al. Randomized, blinded, sham-controlled trial of acupuncture for the management of aromatase inhibitor-associated joint symptoms in women with early-stage breast cancer. J Clin Oncol. 2010;28:1154–60. doi: 10.1200/JCO.2009.23.4708. [DOI] [PubMed] [Google Scholar]
- 45.Crew KD, Capodice JL, Greenlee H, Apollo A, Jacobson JS, Raptis G, et al. Pilot study of acupuncture for the treatment of joint symptoms related to adjuvant aromatase inhibitor therapy in postmenopausal breast cancer patients. J Cancer Surviv. 2007;1:283–91. doi: 10.1007/s11764-007-0034-x. [DOI] [PubMed] [Google Scholar]
- 46.Choi TY, Lee MS, Kim TH, Zaslawski C, Ernst E. Acupuncture for the treatment of cancer pain: A systematic review of randomised clinical trials. Support Care Cancer. 2012;20:1147–58. doi: 10.1007/s00520-012-1432-9. [DOI] [PubMed] [Google Scholar]
- 47.Molassiotis A, Sylt P, Diggins H. The management of cancer-related fatigue after chemotherapy with acupuncture and acupressure: A randomised controlled trial. Complement Ther Med. 2007;15:228–37. doi: 10.1016/j.ctim.2006.09.009. [DOI] [PubMed] [Google Scholar]
- 48.Vickers AJ, Straus DJ, Fearon B, Cassileth BR. Acupuncture for postchemotherapy fatigue: A phase II study. J Clin Oncol. 2004;22:1731–5. doi: 10.1200/JCO.2004.04.102. [DOI] [PubMed] [Google Scholar]
- 49.Feng Y, Wang XY, Li SD, Zhang Y, Wang HM, Li M, et al. Clinical research of acupuncture on malignant tumor patients for improving depression and sleep quality. J Tradit Chin Med. 2011;31:199–202. doi: 10.1016/s0254-6272(11)60042-3. [DOI] [PubMed] [Google Scholar]
- 50.Chen HY, Shi Y, Ng CS, Chan SM, Yung KK, Zhang QL. Auricular acupuncture treatment for insomnia: A systematic review. J Altern Complement Med. 2007;13:669–76. doi: 10.1089/acm.2006.6400. [DOI] [PubMed] [Google Scholar]
- 51.Cheuk DK, Yeung WF, Chung KF, Wong V. Acupuncture for insomnia. Cochrane Database Syst Rev. 2007;3 doi: 10.1002/14651858.CD005472.pub2. CD005472. [DOI] [PubMed] [Google Scholar]
- 52.Ernst G, Strzyz H, Hagmeister H. Incidence of adverse effects during acupuncture therapy-a multicentre survey. Complement Ther Med. 2003;11:93–7. doi: 10.1016/s0965-2299(03)00004-9. [DOI] [PubMed] [Google Scholar]