

Abstract
A 68-year-old man with a previous right total hip arthroplasty presented with acute pain in the right hip, and no associated trauma was reported. The previous hybrid arthroplasty consisted of a ceramic femoral head articulating on an ultra-high-molecular-weight polyethylene liner. The unusual diagnosis of fractured ceramic femoral head was made and an urgent revision arthroplasty was performed to remove the ceramic bearing as well as all implants that may have come into contact with the ceramic. This case report highlights the material properties of ceramics in total hip arthroplasties as well as the importance of regular follow-up in these patients.
Background
John Charnley is regarded as the father of modern arthroplasty as he developed the ‘low-friction’ arthroplasty.1 By decreasing the friction between the bearing surfaces in the prosthesis, the longevity of the implant could be improved as the wear rate would decrease. Ceramic bearings have demonstrated the lowest wear rates of any bearing combination.2 The properties of ceramics that lead to low wear rates are improved lubrication due to the hydrophilic nature of ceramics as well as a greater hardness as compared with metal improving manufacturing to decrease surface roughness.3
The biomechanical properties of ceramics mean that although its wear characteristics are good, it remains a brittle material undergoing no plastic deformation before fracturing. This complication typically results when a hard-on-hard (ceramic-on-metal and ceramic-on-ceramic) bearing surface combination is used. When a ceramic femoral head is combined with a relatively soft material such as ultra-high-molecular-weight polyethylene (UHMWPE), fracture of the ceramic head would seem unlikely.
Case presentation
A 68-year-old man was referred to the orthopaedic team at a tertiary referral centre with a history of sudden onset of increasing pain in his right hip with a hybrid total hip arthroplasty in situ.
In 1995, at the age of 50, the patient underwent a primary total hip replacement (THR) through a posterior approach. The arthroplasty was a hybrid, cemented femoral stem, uncemented acetabular shell with a cobalt-chrome femoral head articulating with a UHMWPE liner. His postoperative course was uneventful. A year later, he underwent a similar arthroplasty of his left hip, again with no problems.
In 1999, the patient developed increasing pain in his right hip that was associated with a grinding feeling. The radiograph of his hip demonstrated the cause of his symptoms as wear of the UHMWPE liner. The patient was scheduled for revision surgery where in a single operation the implants were removed and replaced. The implants used following removal were a 58 mm outer diameter Zimmer (Warsaw, Indiana, USA) Harris/Galante uncemented acetabular shell with a 28 mm inner diameter UHMWPE liner. The femoral components were a Zimmer CPT size 3 stem that was inserted using a cement-in-cement technique with a 28 mm Zimmer zirconium oxide ceramic femoral head (6° taper, 7 mm neck length). The patient made a good recovery with decreased pain and improved mobility.
Forty-eight hours prior to the recent admission in 2013, the patient reported acute onset of pain in the right hip on standing first thing in the morning. There was no associated trauma reported with normal daily activities being conducted pain free the previous day. He works as a sheep farmer and uses a stick for walking only on uneven ground. After presenting to his general practitioner, he was referred to the orthopaedic team for management. On arrival to the department, he was comfortable at rest, non-feverish and had no neurovascular compromise but experienced pain on internal and external rotation as well as flexion past 90° of the hip. The radiograph of both hips taken on admission (figure 1) showed an acute fracture of the ceramic femoral head with osteolysis present behind the acetabular shell; the femoral stem, however, appeared well fixed. The patient was prepared for an urgent revision surgery of the right hip.
Figure 1.

Anteroposterior radiograph of the hips showing a fracture of the ceramic femoral head in the right hip.
Treatment
A single-stage revision arthroplasty of the right hip was undertaken. The fractured femoral head (figures 2 and 3) was removed as four main fragments. Copious saline was used to remove all the ceramic particles. The acetabular liner was loose and was easily removed. After the acetabular shell was removed, large areas of osteolysis were noted, requiring bone grafting before a replacement shell could be implanted. The femoral stem was knocked out of the cement mantle, which was intact, showing no signs of loosening. The well-fixed stem was removed due to trunnion damage, which if retained could cause damage to the replacement ceramic femoral head which would be unacceptable. Reimplantation of a Zimmer Continuum 60 mm outer diameter acetabular shell with a Continuum BIOLOX 36 mm inner diameter alumina ceramic liner was performed. A size 1 Zimmer CPT femoral stem was cemented in place using a cement-in-cement technique and a 36 mm alumina ceramic head. The postoperative radiograph showed a well-implanted total hip arthroplasty (figure 4). The patient made an uneventful recovery and was discharged on the third postoperative day.
Figure 2.
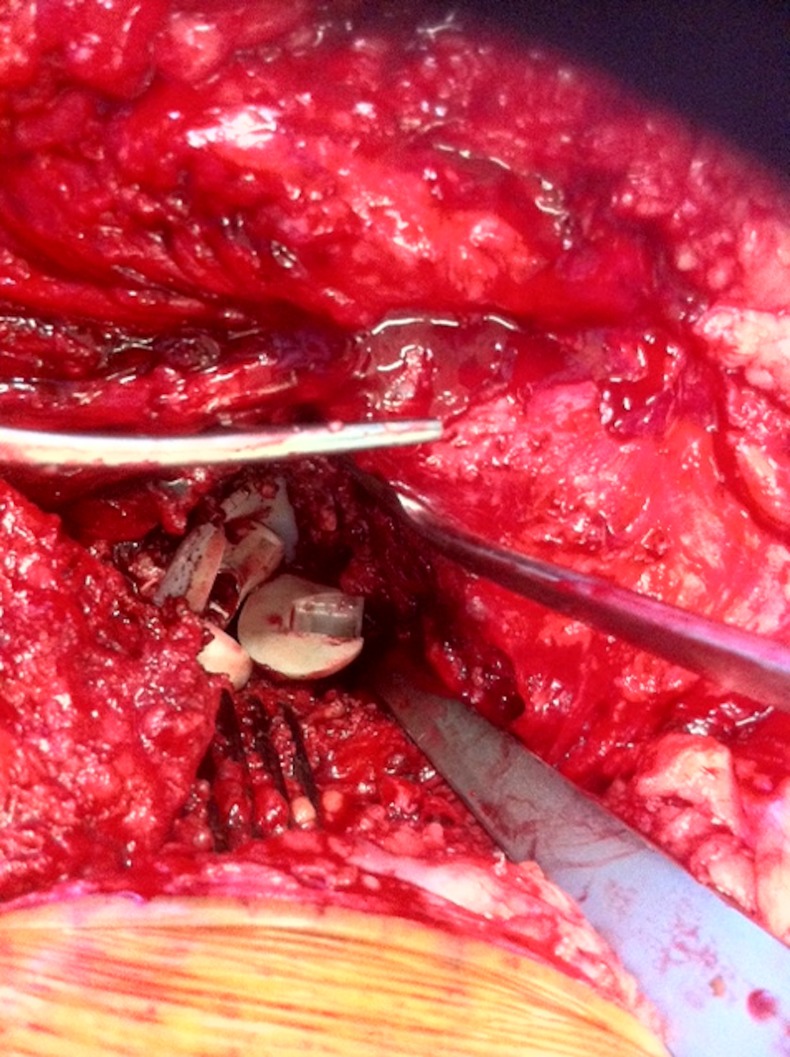
Intraoperative findings of fractured ceramic bearing in situ.
Figure 3.

The explanted implants including the femoral stem, polyethylene acetabular liner and fractured ceramic femoral head.
Figure 4.

Postoperative radiograph depicting the revised right total hip replacement in situ.
Discussion
The perfect bearing surface remains the ‘holy grail’ of arthroplasty surgery. At present, there are three categories of bearing surfaces available to the arthroplasty surgeon, namely metal, ceramic and UHMWPE. Owing to the forces acting upon the hip joint, the prosthetic femoral head has historically been made from a hard material. Metals and ceramics are hard materials but they differ in an important area—ductility. Ductility of a material refers to the amount of plastic deformation a material undergoes before it fails.4 A ductile material undergoes plastic deformation before failure and depending on how long this takes can be identified before failure occurs. A material that has no ductility is said to be brittle and undergoes little or no plastic deformation before failure and failing at a more rapid rate than ductile materials. Failure of these brittle materials typically begins with a flaw in the material such as a crack or pore which then propagates to fracture. Ceramics are a brittle material with failure occurring rapidly resulting in fracturing of the material, while metals are more ductile and deform over a period of time which leads to ultimate failure of the material.5
Primary spontaneous ceramic head fracture where no underlying cause is found is extremely rare and would constitute a manufacturing fault. Fracturing of a ceramic femoral head due to flaws arising in the material secondary to insults occurring during or after implantation are more common than spontaneous fractures but thankfully remains a rare event,6 7 constituting an indication for revision arthroplasty in less than 1% of all revision cases in one series.8 Surgeons and assistants take particular care not to damage the ceramic during implantation, handling the implant carefully and preventing other hard materials from coming into contact with the brittle ceramic, especially during the final reduction manoeuvre. The ceramic head can be damaged even after implantation and closure of the hip joint, primarily from the other hard components of a hip arthroplasty. In a normally functioning THR, the femoral head is in contact with two surfaces, the tapered trunnion of the femoral stem and the acetabular-bearing surface. If a ceramic femoral head comes into contact with any other surface or if there is any movement at the neck–head interface, which is an abnormal situation, will result in failure of the prosthesis. Contact with other hard surfaces can occur as a result of wear or loosening of the acetabular liner—which occurs more frequently in a soft UHMWPE liner—exposing the underlying metal shell or if the shell itself loosens from its attachment to the pelvis in a process called osteolysis. Under normal conditions, there is no movement between the tapered trunnion and the head, if for some reason movement can occur, this would cause imperfections and flaws to occur on the inside of the ceramic head providing yet another mode of ceramic damage. Movement between the trunnion and the femoral head is increased in situations where the trunnion itself is damaged, hence the revision of the well-fixed stem following identification of trunnion damage in this case.
Therefore, it is clear that although ceramics typically fail quickly and catastrophically, there is usually a preceding failure of the arthroplasty that begins the process of ceramic failure. For this reason, an active surveillance of all patients undergoing hip replacements is important as early identification of problems may prevent catastrophic failures, as in this case, as well as decreasing the morbidity associated with revision arthroplasties in general.9–11
Learning points.
Bearing surfaces in total hip arthroplasty consist of three materials: metal (cobalt-chrome), ceramic (alumina and zirconia) and polymers (UHMWPE).
Brittle materials such as ceramics undergo no plastic deformation before failing, rather defects such as cracks or pores in the material caused by damage propagate rapidly which causes the material to fracture.
Damage to ceramics in hip arthroplasty can occur intraoperatively via poor operative technique or postoperatively when the other components of the arthroplasty begin to fail.
Fracturing of ceramic bearings is an uncommon but serious indication for revision hip arthroplasty. Appreciation of the importance of regular follow-up in all patients undergoing a joint replacement is essential as early identification of complications reduces overall morbidity.
Footnotes
Contributors: Both authors have made substantial contributions to the conception, drafting, revision and final approval of the manuscript.
Competing interests: None.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Learmonth ID, Young C, Rorabeck C. The operation of the century: total hip replacement. Lancet 2007;370:1508–19 [DOI] [PubMed] [Google Scholar]
- 2.Zywiel MG, Sayeed SA, Johnson AJ, et al. Survival of hard-on-hard bearings in total hip arthroplasty: a systematic review. Clin Orthop Relat Res 2011;469:1536–46 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Lusty PJ, Tai CC, Sew-Hoy RP, et al. Third-generation alumina-on-alumina ceramic bearings in cementless total hip arthroplasty. J Bone Joint Surg Am 2007;89:2676–83 [DOI] [PubMed] [Google Scholar]
- 4.Green SM. Deformation of materials. Curr Orthop 2006;20:9–15 [Google Scholar]
- 5.Krikler S, Schatzker J. Ceramic head failure. J Arthroplasty 1995;10:860–2 [DOI] [PubMed] [Google Scholar]
- 6.Callaway GH, Flynn W, Ranawat CS, et al. Fracture of the femoral head after ceramic-on-polyethylene total hip arthroplasty. J Arthroplasty 1995;10:855–9 [DOI] [PubMed] [Google Scholar]
- 7.Michaud RJ, Rashad SY. Spontaneous fracture of the ceramic ball in a ceramic-polyethylene total hip arthroplasty. J Arthroplasty 1995;10:863–7 [DOI] [PubMed] [Google Scholar]
- 8.Lee Y-K. Alumina-on-alumina total hip arthroplasty: a concise follow-up, at a minimum of ten years, of a previous report. J Bone Joint Surg Am 2010;92:1715. [DOI] [PubMed] [Google Scholar]
- 9.BOA Blue Book Primary Total Hip Replacement: a guide to good practise, Nov 2012. http://www.boa.ac.uk/Publications/Documents/blue_book_hip_1-1.pdf
- 10.Havelin LI, Engesæter LB, Espehaug B, et al. The Norwegian arthroplasty register: 11 years and 73 000 arthroplasties. Acta Orthop 2000;71:337–53 [DOI] [PubMed] [Google Scholar]
- 11.Sharma V, Ranawat AS, Rasquinha VJ, et al. Revision total hip arthroplasty for ceramic head fracture. J Arthroplasty 2010;25:342–7 [DOI] [PubMed] [Google Scholar]