

Dear Sir,
Tattoos and piercing have become relatively common and are often considered to be low risk, mainstream behaviours, although most countries have a donor deferral policy to address them. Temporary deferral is intended to delay donation from individuals in the early stages of infection (the window period) until detection by current assays is possible. Deferral for this reason is fairly common, and has a negative impact on the return of donors once eligible1. In Canada, where nucleic acid testing for human immunodeficiency virus (HIV), hepatitis C virus (HCV) and hepatitis B virus (HBV) is done on each donation, a 12-month deferral was originally applied for donors who had had tattoos or piercing as a precaution. This deferral period was reduced in 2005 to 6 months with no loss in safety2. In the USA the AABB standards do not require deferral for tattooing or body piercing if performed in a licensed establishment, but otherwise require a 12-month deferral, whereas the Council of Europe requires a 4-month deferral as long as HCV nucleic acid testing is performed, otherwise 12 months. It is largely presumed that donors comply with the policy and answer questions correctly, but donor disclosure of behaviours is complex and studies of donors with transmissible disease show that questions about high-risk behaviours are sometimes misinterpreted3. We have estimated the percentage of deferrable risk in donors using anonymous donor surveys and compared this with donor deferral records.
The Canadian Blood Services are responsible for the collection and distribution of blood products in all provinces except Québec. An anonymous questionnaire was mailed to a total of 40,000 whole blood donors with negative tests for infectious disease markers stratified by region and including all nine provinces from which the Canadian Blood Services collect blood with first-time donors over-sampled on a monthly basis (shortly after their donation) throughout 2006 and again in 2008 (80,000 donors in total) as described elsewhere4. Donors were asked if they had ever had a tattoo, ear or body piercing and if so, if it was in the last 6 months. They were also asked demographic questions. In total, 31,155 donors (48%) completed a survey questionnaire. Operational data include a single deferral code for percutaneous blood exposure. To quantify the number of deferrals for tattoo, ear and body piercing more accurately, donor records for on-site deferrals in Toronto and Ottawa, Ontario were accessed and reasons for deferral extracted manually for the period between 1 September 2005 and 31 December 2006 (16 months in total). These three risks accounted for 82% of all deferrals captured by the code. Because donors making appointments to donate are routinely asked about tattoos, ear and body piercing, telephone deferrals for these reasons are common. Telephone deferrals with the code that includes tattoo, ear and body piercing were adjusted using the manually extracted proportions for these specific reasons for deferral to obtain the total estimated deferrals and sorted by age group and sex. The proportions for each specific reason were calculated for each age and gender group from the on-site deferral data, and then applied to the telephone deferrals from donors with the same age and gender to estimate the total number of deferrals for each specific reason.
Our results from the national donor survey showed that the percentage of donors with a history of a tattoo was higher in female donors (18% vs 10%, p<0.0001, Figure 1a), peaking between the ages of 25 and 34 when about one third of females and about one fifth of males have had a tattoo. Ear and body piercing by age group is shown in Figure 1b. Nearly all female donors (92%) had their ears pierced, whereas far fewer males had (13%, p<0.0001). Body piercing was more common in females than in males (18% vs 3%, p<0.0001), especially in the 20–29 age group (43%).
Figure 1.
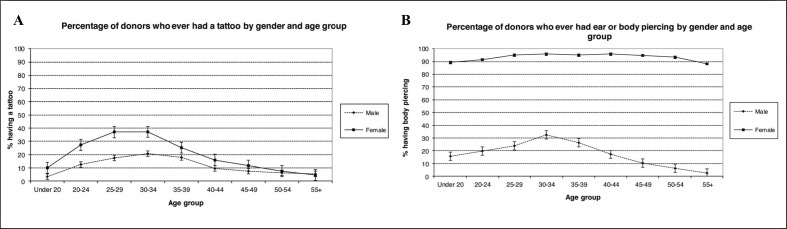
Percentage of donors who ever had a tattoo (A), ear or body piercing (B) by gender and age group.
Table I lists the percentage of donors with a deferrable risk who had donated and the percentage of donors who were deferred and shows that these were rather similar. There are some limitations to quantifying deferrable risk not declared at the time of donation due to voluntary participation in surveys (thus potential for underestimating), and due to a delay of up to a few weeks between completion of the questionnaire post-donation so that some donors could have engaged in risk activities after donating (thus potential for overestimating risk). Furthermore, the percentage of donors deferred was based on data from only two centres, accounting for about one quarter of collections whereas the percentages of donors with deferrable risk were drawn from national data. Nevertheless, it appears that compliance with these criteria is poor.
Table I.
Comparison of estimated numbers and percentages of donors deferred for tattoos, ear or body piercing with donors with deferrable risk.
| Deferred* (N=408,864) | Deferrable risk (but donated) (N=31,155) | |||
|---|---|---|---|---|
|
| ||||
| Tattoo | ||||
|
| ||||
| Age (years) | Females (%) | Males (%) | Females (%) | Males (%) |
| <25 | 1.9 | 1.0 | 1.2 | 0.9 |
| 25–34 | 0.8 | 0.4 | 0.6 | 0.2 |
| 35–44 | 0.4 | 0.1 | 0.4 | 0.3 |
| ≥45 | 0.2 | 0.04 | 0.05 | 0.0 |
| Total | 0.61 | 0.21 | 0.49 | 0.24 |
|
| ||||
| Ear or body piercing | ||||
|
| ||||
| Age (years) | Females (%) | Males (%) | Females (%) | Males (%) |
| <25 | 4.8 | 2.2 | 3.5 | 1.1 |
| 25–34 | 1.9 | 0.7 | 1.1 | 0.5 |
| 35–44 | 0.9 | 0.2 | 0.9 | 0.3 |
| ≥45 | 0.3 | 0.09 | 0.7 | 0.1 |
| Total | 1.38 | 0.41 | 1.5 | 0.31 |
Deferral data obtained from blood centres in two locations, Toronto and Ottawa.
These behaviours were all extremely frequent in our donor population, particularly among young females, suggesting that they do not identify a population at high risk for hepatitis or HIV infection. Tattoos and piercing are not predictive of transmissible disease in our donors2,5 and the safety benefit of these deferral criteria in Canada is, therefore, questionable.
Footnotes
The Authors declare no conflicts of interest disclosure.
References
- 1.Custer B, Chinn A, Hirschler NV, et al. The consequences of temporary deferral on future whole blood donation. Transfusion. 2007;47:1514–23. doi: 10.1111/j.1537-2995.2007.01292.x. [DOI] [PubMed] [Google Scholar]
- 2.Goldman M, Xi G, Yi Q-L, et al. Reassessment of deferrals for tattooing and piercing. Transfusion. 2009;49:648–54. doi: 10.1111/j.1537-2995.2008.02037.x. [DOI] [PubMed] [Google Scholar]
- 3.O’Brien SF, Xi G, Yi Q-L, Goldman M. Understanding non-disclosure of deferrable risk: a study of blood donors with a history of intravenous drug use. Transfus Med. 2010;20:15–21. doi: 10.1111/j.1365-3148.2009.00969.x. [DOI] [PubMed] [Google Scholar]
- 4.O’Brien SF, Fan W, Xi G, et al. Declining hepatitis C rates in first time blood donors: insight from surveillance and case-control risk factor studies. Transfusion. 2008;48:902–9. doi: 10.1111/j.1537-2995.2007.01618.x. [DOI] [PubMed] [Google Scholar]
- 5.O’Brien SF, Xi G, Fan W, et al. Epidemiology of hepatitis B in Canadian blood donors. Transfusion. 2008;48:2323–30. doi: 10.1111/j.1537-2995.2008.01845.x. [DOI] [PubMed] [Google Scholar]