

Abstract
Background:
The incidence of subarachnoid hemorrhage (SAH) in young adults is relatively rare. Kawasaki disease is a systemic vasculopathy that is known to cause coronary artery aneurysms; however, its effect on cerebral arteries remains largely unclear.
Case Description:
We report the case of a 20-year-old male with a history of Kawasaki disease who presented with SAH caused by the rupture of a nonbranching middle cerebral artery aneurysm. This is the third report of SAH associated with Kawasaki disease. Preoperative echocardiography of the patient rejected the presence of bacterial endocarditis and other heart abnormalities. An emergency craniotomy and clip occlusion of the aneurysm was successfully performed without obstructing the parent artery. Two weeks later, the patient was discharged without any apparent neurological deficit. We also performed a circumstantial pathological study on specimens obtained from the aneurysm wall. Our histological findings suggest that the elastic lamina and tunica intima were completely destroyed during the acute vasculitis phase of Kawasaki disease, which possibly led to the aneurysmal formation.
Conclusions:
Lack of active inflammatory changes and atherosclerotic lesions may explain the chronic feature of Kawasaki disease, not a typical aneurysmal formation.
Keywords: Kawasaki disease, middle cerebral artery, nonbranching aneurysm, subarachnoid hemorrhage
INTRODUCTION
Subarachnoid hemorrhage (SAH) is rarely seen in young adults. In older patients, ruptured aneurysms at arterial bifurcation sites typically gives rise to SAH. Atherosclerosis induces inflammatory changes in these locations and damages the elastic lamina, which in turn can lead to an artery bifurcation aneurysm.
Kawasaki disease is an acute vasculitis that predominantly occurs during childhood. It is characterized by fever, bilateral nonexudative conjunctivitis, erythema of the lips and oral mucosa, changes in the extremities, rash, and cervical lymphadenopathy.[5] The major sequela of Kawasaki disease is coronary aneurysm. Although cerebral aneurysms can also occur, there are only two reported cases,[1,12] and the correlation between Kawasaki disease and cerebral artery aneurysms remains largely unclear.
Here, we describe the case of a 20-year-old male patient with a history of Kawasaki disease who presented with SAH caused by the rupture of a nonbranching aneurysm at a proximal segment of the middle cerebral artery (M2). The aneurysm was successfully clipped even though it had no obvious vascular wall and was very fragile. Besides Kawasaki disease, which is a known cause of aneurysms, the patient had no other notable medical history. This is the third report of SAH in association with Kawasaki disease, and the findings are discussed in relation to the previous reports.
CASE REPORT
History and examination
A 20-year-old male experienced a sudden onset of headache, nausea, and vomiting. He was brought to a nearby hospital, where a head computed tomographic (CT) scan revealed SAH. He was immediately transferred to our hospital for emergency treatment. He had a history of Kawasaki disease, which was believed to be cured. He had severe atopic dermatitis and was allergic to pollen, dogs, cats, and soba. There was no relevant family medical history and no previous history of forceps delivery, major head injury, and infectious or valvular disease. On arrival at our hospital, his Glasgow Coma Scale score was 14 points (E3V5M6). Physical and neurological examination revealed no specific abnormal deficits. Laboratory blood tests also revealed no abnormalities. Plain CT of the brain showed SAH, localized in the right sylvian fissure, and evidence of skull fracture [Figure 1]. Subsequent CT angiography indicated an aneurysm of the right M2, which was not at a bifurcation site [Figure 1]. Magentic resonance (MR) angiography revealed that the aneurysm had a stalk-like narrow neck. A pseudoaneurysm was suspected on the basis of the atypical location and shape of the aneurysm, his age, and his medical history of Kawasaki disease. Preoperative echocardiography rejected the presence of bacterial endocarditis and other heart abnormalities. As far as we could examine, there were no other vascular abnormal findings other than the aneurysm described here including aneurysms of other locations.
Figure 1.
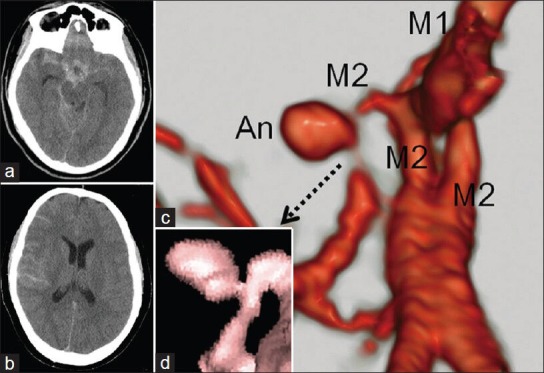
Computed tomography (CT) of the patient at admission showed a thick subarachnoid hemorrhage (SAH) predominantly in the basal cistern and right Sylvian fissure (a). The SAH was spreading to the peripheral subarachnoid space and the brain seemed really tight (b). Three-dimensional CT angiography revealed an aneurysm arising from a distal point of the right middle cerebral artery bifurcation (c). Magnetic resonance (MR) angiography shows a clear image of the stalk-like and narrow aneurysm neck (d)
Operation
The sylvian fissure was identified and opened to expose the two parallel M2 branches. The M1 and the parental artery were then subsequently secured. A thin-walled, pseudo-looking aneurysm was found buried in the frontal lobe, but it appeared to be clippable [Figure 2]. A 5-mm bayonet-type clip (Sugita 2, Mizuho) was chosen and several attempts were made to close the ruptured hole without narrowing the parental artery [Figure 2]. A doppler study confirmed good flow through the artery, and the aneurysm appeared to be completely obliterated. The thin aneurysm wall was partially trimmed for pathological analysis and Neoveil™ was wrapped around the neck. The aneurysm wall appeared extremely thin and fragile and was surrounded by some clots.
Figure 2.
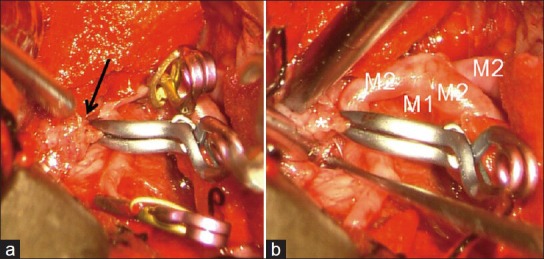
Operative pictures of the aneurysm clipping. (a) The aneurysm was buried into the right frontal lobe (arrow). With parent artery trapping, the aneurysm was tentatively clipped. (b) Final view of the clipping. The aneurysm was carefully resected. There was no obvious arterial wall (asterisk). The aneurysm was located distal to the right middle cerebral artery bifurcation without an adjacent artery
Pathological findings
Histopathological examination revealed that the aneurysm wall primarily consisted of thinkened tunica intima. Granulation tissue presented with edematous chronic inflammatory cell invasion and intermediate invasion of macrophages, fibroblasts, myofibroblasts, and vascular endothelial cells. There was mild invasion of lymphocytes and plasmacytes, but no neutrophils [Figure 3]. Lack of black Elastica van Gieson (EVG) staining demonstrated complete absence of elastic lamina. EVG staining, Masson's trichrome staining, and smooth muscle actin (SMA) immunohistochemistry also demonstrated the lack of smooth muscle cells in the tunica media. There was no atherosclerotic change in the tunica intima, which is usually observed in cerebral aneurysms [Figure 3].
Figure 3.
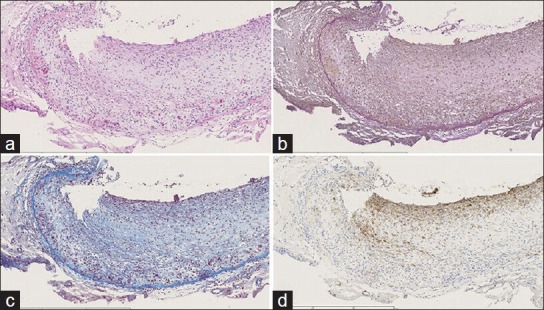
Histopathological studies of the surgical specimen. (a) Hematoxylin and eosin (H and E) staining. The upper side is the vascular lumen. Atherosclerotic change was not observed. (b) Elastica van Gieson (EVG) staining shows thickened intima and mild invasion of inflammatory cells. (c) Masson's trichrome staining. (d) SMA (smooth muscle actin) immunohistochemistry. Staining reveals lack of smooth muscle cells in the tunica media. Scale bar: 600 μm
Postoperative course
After surgery, the patient regained consciousness and exhibited a full postoperative recovery. Two weeks later, CT angiography showed complete amelioration of the aneurysm and normal flow of the parent artery [Figure 4]. Plain CT after sugery also confirmed an intact brain [Figure 4]. His postoperative course was uneventful without any neurological deficits, and he was discharged 2 weeks after admission.
Figure 4.
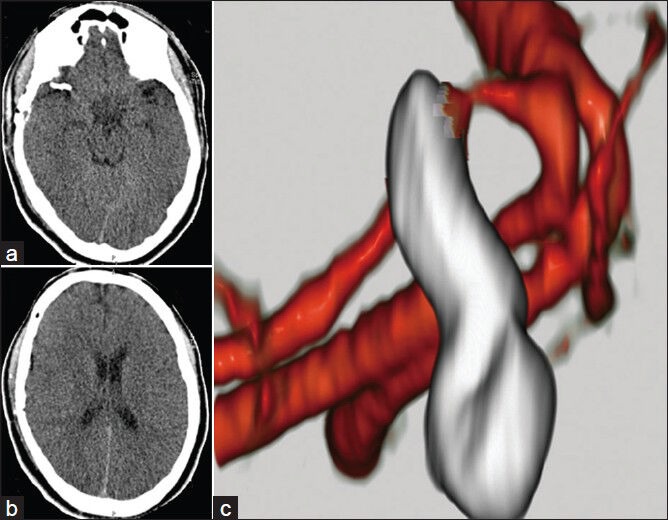
Computed tomography (CT) image acquired on the day of discharge showed an intact brain with a clip (a,b) CT angiography after 2 weeks showed obliteration of the aneurysm and ideal flow of the parent artery (c)
DISCUSSION
The incidence of SAH in young adults is very rare, accounting for 1% of individuals younger than 20 years of age.[3,7] Traumatic and infectious aneurysms are more prevalent in children and adolescents than in adults.[2,6,13] The cause of most childhood aneurysms is unexplained and theories remain controversial.[6] In the present case, there was no history of unusual delivery, recent head injury, or infectious disease. Preoperative echocardiography rejected the presence of bacterial endocarditis and other heart abnormalities.
Kawasaki disease is a condition that causes inflammation in the walls of small- and medium-sized arteries throughout the body, including the coronary arteries.[11] Kawasaki disease is also called mucocutaneous lymph node syndrome because it affects lymph nodes, skin, and the mucous membranes inside the mouth, nose, and throat. Symptoms of Kawasaki disease such as high fever and peeling skin can be frightening. Among different pathologies of Kawasaki disease, elastic and musculoelastic arteries typically demonstrate a high incidence of arteritic changes. In general, lesions are mild to moderate with the exception of the iliac artery; severe changes and necrotizing panarteritis of the iliac artery are often associated with aneurysm formation. A high incidence of arteritic changes, mainly necrotizing panarteritis, has been observed in extravisceral middle-sized arteries. In particular, this has been noted in the coronary artery and is often accompanied by aneurysms, some of which can rupture. Coronary artery aneurysms or ectasias develop in approximately 15-25% of untreated children with Kawasaki disease and may lead to ischemic heart disease or sudden death.[9] Pathological studies of aneurysm specimens obtained from patients with Kawasaki disease have revealed arteritic changes in the intravisceral arteries in addition to coronary arteries. Thus, aneurysmal changes may arise from medium-sized cerebral arteries.
In a previous study, noninvasive multislice spiral computed tomography (MSCT) was performed in adolescents and young adults with Kawasaki disease to assess coronary artery abnormalities; all young adults older than 20 years still had coronary artery aneurysms.[4] We were unable to examine the coronary artery of our patient in detail because an emergency surgery was necessary. Furthermore, since he recovered without any neurological deficit, he and his family would not agree to further invasive angiography. Thus, we cannot say definitively if the patient also possessed a coronary artery lesion similar to the cerebral artery abnormality.
There are only two other reports that discuss the relationship between Kawasaki disease and cerebral aneurysm.[1,12] Both of them described a saccular aneurysm at the bifurcation of major arteries. In our case, the aneurysm was located at the trunk of the middle cerebral artery, where no branch existed. In contrast to a usual bifurcation aneurysm, a nonbifurcation aneurysm is less associated with atherosclerosis and degeneration of the internal elastic lamina.[8,14] Its dome is composed of a fragile outer membrane and connective tissue that ruptures before the aneurysm becomes relatively large.[8] Interestingly, coronary aneurysms in Kawasaki disease also arise from where no branch exists. In this case, the aneurysm had a stalk-like narrow neck. Park reported that basal rupture is likely to happen in this type of aneurysm.[10] In our case, the dome was found buried in the frontal lobe; however, CT revealed no intracerebral hemorrhage other than SAH. Therefore, basal rupture of the aneurysm was the likely cause of SAH.
Histopathological examinations carried out in previous reports should be discussed here. In the 13-month-old case, the specimen was too small to examine appropriately and no inflammatory changes of the aneurysm wall could be observed.[1] In contrast, histopathological findings of a 12-year-old case revealed thickening of the endothelial inner wall due to hypertrophy and invasion of inflammatory cells, including granulocytes, into the wall of the dome,[12] and they concluded that their findings seemed to mimic the acute inflammatory changes observed in coronary arteries in Kawasaki disease. In our case, we performed a circumstantial histopathological study and compared our findings to the previous reports. All of the vasculitis changes in our specimen occurred during infancy. Elastic lamina and tunica intima were completely destroyed during the acute phase, which caused the aneurysmal formation. Lack of elastic lamina and tunica media led us to consider the possibility of a pseudoaneurysm. However, the whole vascular wall had enlarged, and thus, it could be classified as a true aneurysm. Nevertheless, distinction between pseudo and true aneurysm is not relevant in this case. In summary, from a pathological point of view, the aneurysmal lesion occurred as a result of acute vasculitis associated with Kawasaki disease.
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2014/5/1/5/125285
Contributor Information
Atsushi Ishida, Email: v2danyon@gmail.com.
Seigo Matsuo, Email: sergio5679@gmail.com.
Shunji Kawamura, Email: shunji@tymc.twmu.ac.jp.
Toshio Nishikawa, Email: nishikawat@twmu.ac.jp.
REFERENCES
- 1.Ahn JH, Phi JH, Kang HS, Wang KC, Cho BK, Lee JY, et al. A ruptured middle cerebral artery aneurysm in a 13-month-old boy with Kawasaki disease. J Neurosurg Pediatr. 2010;6:150–3. doi: 10.3171/2010.5.PEDS1012. [DOI] [PubMed] [Google Scholar]
- 2.Honda M, Nagamine T, Yamashiro K, Shimoji T. An intracranial pseudoaneurysm in the distal middle cerebral artery in a child. Pediatr Neurosurg. 2008;44:426–9. doi: 10.1159/000149914. [DOI] [PubMed] [Google Scholar]
- 3.Ikawa F, Ohbayashi N, Imada Y, Matsushige T, Kajihara Y, Inagawa T, et al. Analysis of subarachnoid hemorrhage according to the Japanese Standard Stroke Registry Study-incidence, outcome, and comparison with the International Subarachnoid Aneurysm Trial. Neurol Med Chir (Tokyo) 2004;44:275–6. doi: 10.2176/nmc.44.275. [DOI] [PubMed] [Google Scholar]
- 4.Kanamaru H, Sato Y, Takayama T, Ayusawa M, Karasawa K, Sumitomo N, et al. Assessment of coronary artery abnormalities by multislice spiral computed tomography in adolescents and young adults with Kawasaki disease. Am J Cardiol. 2005;95:522–5. doi: 10.1016/j.amjcard.2004.10.011. [DOI] [PubMed] [Google Scholar]
- 5.Kawasaki T. Kawasaki disease. Mucocutaneous lymph node syndrome or MCLS. Acta Pathol Jpn. 1982;32:63–72. [PubMed] [Google Scholar]
- 6.Lasjaunias P, Wuppalapati S, Alvarez H, Rodesch G, Ozanne A. Intracranial aneurysms in children aged under 15 years: Review of 59 consecutive children with 75 aneurysms. Childs Nerv Syst. 2005;21:437–50. doi: 10.1007/s00381-004-1125-x. [DOI] [PubMed] [Google Scholar]
- 7.Locksley HB. Natural history of subarachnoid hemorrhage, intracranial aneurysms and arteriovenous malformations. J Neurosurg. 1966;25:321–68. doi: 10.3171/jns.1966.25.3.0321. [DOI] [PubMed] [Google Scholar]
- 8.Mizutani T, Miki Y, Kojima H, Suzuki H. Proposed classification of nonatherosclerotic cerebral fusiform and dissecting aneurysms. Neurosurgery. 1999;45:253–9. doi: 10.1097/00006123-199908000-00010. [DOI] [PubMed] [Google Scholar]
- 9.Newburger JW, Takahashi M, Gerber MA, Gewitz MH, Tani LY, Burns JC, et al. Diagnosis, treatment, and long-term management of Kawasaki disease: A statement for health professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Pediatrics. 2004;114:1708–33. doi: 10.1542/peds.2004-2182. [DOI] [PubMed] [Google Scholar]
- 10.Park J. Saccular aneurysm with basal rupture angiographically depicted as an aneurysm with stalk-like narrow neck. J Neurosurg. 2011;114:1065–8. doi: 10.3171/2010.6.JNS1086. [DOI] [PubMed] [Google Scholar]
- 11.Pinna GS, Kafetzis DA, Tselkas OI, Skevaki CL. Kawasaki disease: An overview. Curr Opin Infect Dis. 2008;21:263–70. doi: 10.1097/QCO.0b013e3282fbf9cd. [DOI] [PubMed] [Google Scholar]
- 12.Tanaka S, Sagiuchi T, Kobayashi I. Ruptured pediatric posterior cerebral artery aneurysm 9 years after the onset of Kawasaki disease: A case report. Childs Nerv Syst. 2007;23:701–6. doi: 10.1007/s00381-006-0263-8. [DOI] [PubMed] [Google Scholar]
- 13.Yi HJ, Kim KM, Ko Y, Kim YS, Oh SJ, Oh SH. Giant pseudoaneurysm in adolescent. Childs Nerv Syst. 2006;22:8–12. doi: 10.1007/s00381-005-1214-5. [DOI] [PubMed] [Google Scholar]
- 14.Yoshimoto Y, Ochiai C, Nagai M. Cerebral aneurysms unrelated to arterial bifurcations. Acta Neurochir (Wien) 1996;138:958–63. doi: 10.1007/BF01411285. [DOI] [PubMed] [Google Scholar]