

Abstract
Context:
Several classifications for pattern hair loss (PHL) have been used over the years. The Norwood-Hamilton classification for men and Ludwig's classification for women is used commonly, but they have their limitations.
Aims:
The objective of the following study is to evaluate the efficacy of the basic and specific (BASP) classification in Indian populations.
Subjects and Methods:
We used the BASP classification to classify the PHL in the patients visiting our out-patient department in the period from June 2012 to May 2013. 763 patients were classified out of which 313 were females and 450 were males.
Results:
The majority of the female patients were in the 3-5th decade of life and in males were in 4-6th decade.
Conclusions:
The BASP classification is, easily remembered, reproducible classification for the diagnosis and treatment for both male and female pattern alopecia.
Keywords: Basic and specific classification, Indian population, pattern hair loss
INTRODUCTION
Pattern hair loss (PHL) is the most common type of hair loss in men. In females, it is less common. Through the years, several classifications have been proposed, but the Norwood-Hamilton classification for men and Ludwig's classification for women are the most commonly used systems. In 1951, Hamilton proposed the first systemic classification for PHL. He classified the patterns based on fronto-parietal, frontal recession and vertex thinning.[1] Norwood, in 1975, put an emphasis on vertex only classification as an addition to the Hamilton classification.[2] Savin introduced a classification based on pictorial depiction of hair density as derived from midline scalp width.[3] Olsen proposed assigning different designations to the areas of the scalp (temporal, frontal, mid and vertex) as they bald at different rates in different individuals.[4,5] In an article in 1977, Ludwig presented a separate classification for women emphasizing on the preservation of the frontal hairline despite the loss of hair on the top of the scalp.[6] For surgical purposes, Bouhanna created a multifactorial classification of certain parameters such as fixed distances from the face, scalp mobility and thickness and covering power of hair, which can be quantified and computerized.[7] However, all of these have limitations such as Norwood-Hamilton is difficult to memorize and female pattern hair loss (FPHL) in men cannot be classified by this and Ludwig's classification cannot be used to classify male pattern hair loss in females. In addition, most of these classifications were based on Caucasians subjects and not Asians as in comparison with Caucasian patients, Asian patients with androgenetic alopecia (AGA) have different types of hair loss and family histories which may alter the treatment response. There was considerable overlap in types IV, V and VI in the Norwood classification with the ‘a’ variants further confusing the picture.[8] Thus a common classification system for men and women, which is easy to memorize and can be used for all races is required.
In an article in 2000, Koo et al. from Korea, classified male pattern alopecia into six types based on the English alphabetical letter shape of the hair loss area.[9]
The basic and specific (BASP) classification was designed by Lee et al.[10] This included four basic types and two specific types [Figure 1]. The basic type represents the shape of the anterior hairline and the specific type represents the density of hair on the frontal and vertex area. The final type is the combination of the basic and the specific type.[10]
Figure 1.
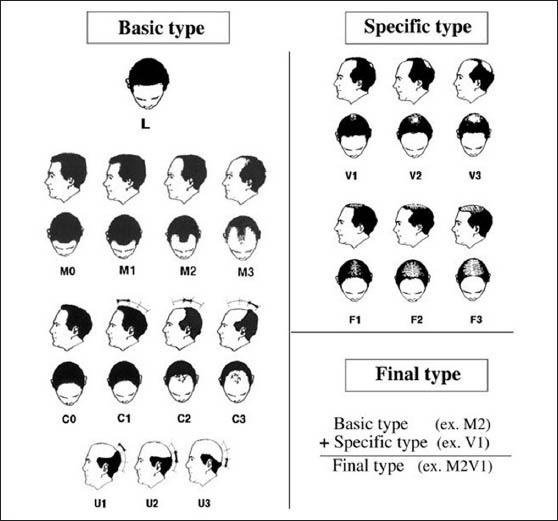
Basic and specific classification
SUBJECTS AND METHODS
Patients were classified according to the pattern of hair loss as per BASP classification as mentioned below. The patients enrolled were those who visited the out-patient department and inpatients who complained of hair loss. A detailed history regarding some of the etiological factors was elicited.
Inclusion criteria
All those who were classified as having PHL.
Exclusion criteria
All those who had diffuse hair loss, alopecia areata, any infection or inflammation of the scalp and hair, any drugs affecting hair growth or under stress.
The patients who fitted into the inclusion criteria and had no exclusion criteria were enrolled into the study after taking consent. Personal, drug and family history was elicited. Digital photographs were taken in four views.
The BASP classification
The basic and the specific type were further divided into three to four grades. One basic type is selected depending on the pattern and graded according to the extent of hair loss with regards to the reference points. The specific type may be selected wherever applicable and graded.
Basic type
The shape of the anterior hairline is divided into four basic types: L, M, C and U.
L - Linear line (no hair loss)
M - Shape of the hairline resembles the alphabet M
C - Shape of the hairline resembles the alphabet C
U - Shape of the hairline resembles the alphabet U.
The reference points are:
Original anterior hairline (anterior hairline at that time when baldness is not present)
The top of the vertex (highest point on the posterior crown)
The occipital protuberance.
Type L
“L” refers to linear line seen when there is no hair loss seen along the anterior border in the fronto-temporal region [Figure 2].
Figure 2.

Basic type L
Type M
Recession in the fronto-temporal hairline is more prominent than the mid-anterior hairline hence the hairline looks like the alphabet “M”.
Type M0
The original hairline is preserved. No hair loss is seen.
Type M1
Fronto-temporal recession is present but does not extend beyond the anterior one-third of the virtual line connecting the original hairline and the top of the vertex [Figure 3].
Figure 3.

Basic + specific M1F1
Type M2
Fronto-temporal recession extends further but not beyond the middle-third of the virtual line.
Type M3
Fronto-temporal recession extends further into the last one-third of the virtual line [Figure 4].
Figure 4.

Basic + specific type M3F3
Type C
Recession in the mid-anterior hairline is more prominent than the Fronto-temporal hairline. The entire anterior hairline regresses posteriorly in the shape of semi-circle resembling the letter “C”.
Type C0
The original hairline is preserved.
Type C1
The mid-anterior hairline recedes to the anterior 1/3rd of the virtual line connecting the original hairline and the top of the vertex.
Type C2
The mid-anterior hairline recedes to the middle 1/3rd of the virtual line.
Type C3
The mid-anterior hairline recedes to the posterior 1/3rd of the virtual line.
Type U
The anterior hairline recedes posteriorly beyond the vertex forming a horseshoe shape resembling the letter “U”. It is the most severe type of AGA.
Type U1
The anterior hairline recedes to lie within the superior 1/3rd of the virtual line connecting vertex and the posterior occipital protuberance.
Type U2
The anterior hairline recedes to lie within the middle 1/3rd of the virtual line connecting vertex and the posterior occipital protuberance.
Type U3
The anterior hairline recedes to lie within the inferior 1/3rd of the virtual line connecting vertex and the posterior occipital protuberance.
Specific type
The specific type may be included whenever necessary. There are two specific types: F and V.
Type F
It represents a general decrease in the density of hair over the entire top of the scalp, regardless of the anterior hairline.
Type F1
Thinning of the hair on the crown is perceptible (mild change) [Figures 3 and 5].
Figure 5.

Specific type F1
Type F2
Thinning of the hair on the crown is pronounced (moderate change).
Type F3
The hair on the crown is very sparse or absent (severe change) [Figure 4].
Type V
The hair around the vertex is notably sparser.
Type V1
Thinning of the hair around the vertex is perceptible (mild change).
Type V2
Thinning of the hair around the vertex is pronounced (moderate change).
Type V3
Thinning of the hair around the vertex is very sparse or absent (severe change).
RESULTS
The male patients were 450 and the number of female patients was 313. The majority of the patients were in the 3-5th decade in females and 4-6th decade in males [Table 1].
Table 1.
Age wise distribution of individual types
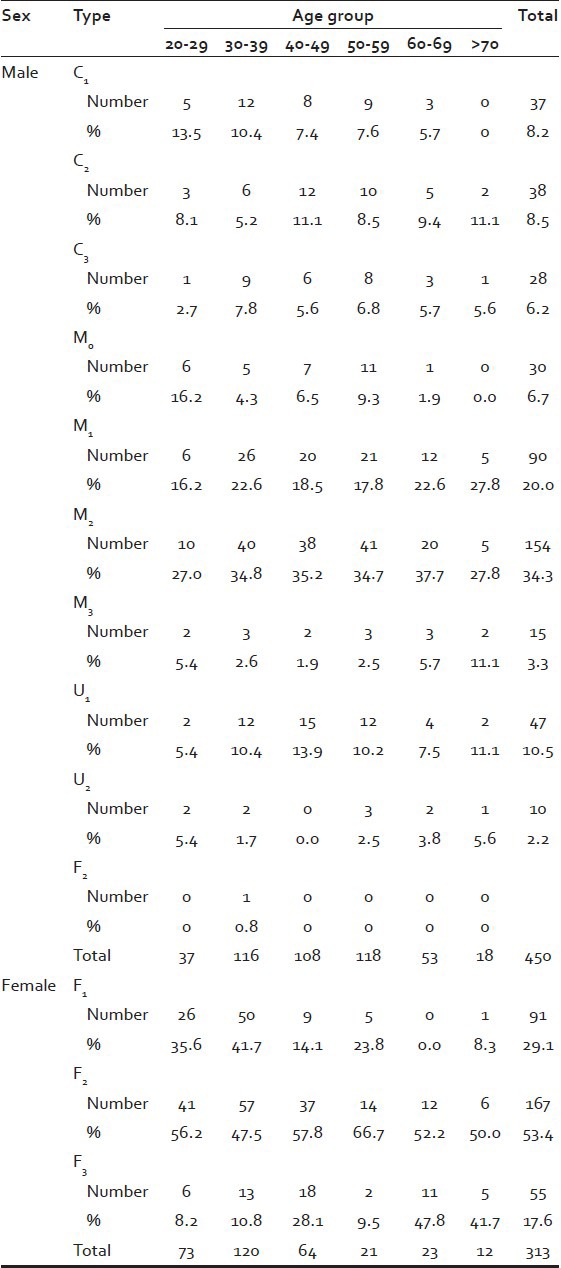
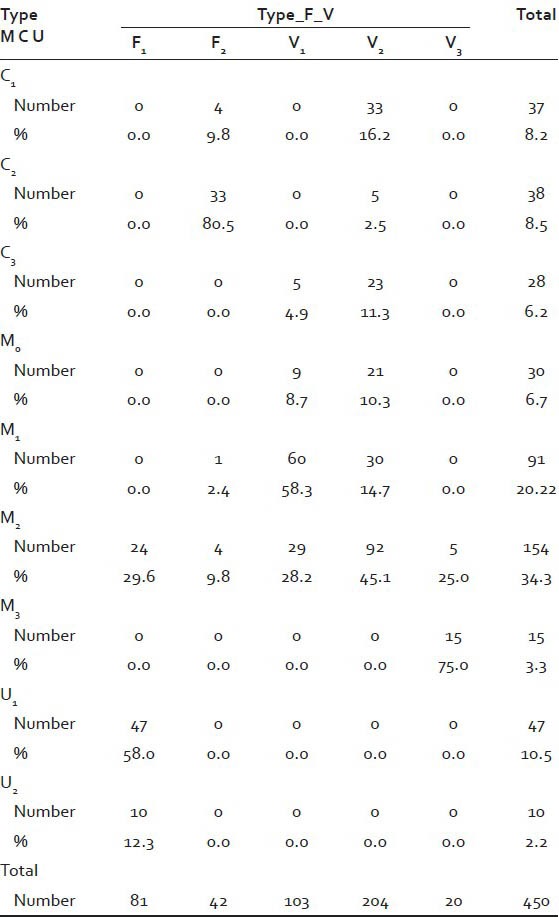
In men, majority (63%) were diagnosed with M type, with M2 being most common (34%). One of the males was diagnosed with female pattern alopecia [Table 2].
Table 2.
Sex wise distribution of final type (males)
All women were diagnosed with F type with F1 (87%) being most common and none of them were diagnosed with male pattern alopecia. As the age increased, the grading downgraded from F1 to F3.
Nearly 48% men gave a history of having similar hair loss on their paternal side of the family, 1% gave a history of having similar history on the maternal side of the family and 51% gave negative history of similar complaints.
Almost 42% women gave a history of similar complaints on the maternal side, none had similar complaints on the paternal side and 58% had no family history of similar complaints.
It was observed that the basic type of Hair loss had paternal inheritance and the specific type had maternal inheritance.
DISCUSSION
The study by Hong et al. conducted a comparative study consisting of eight dermatological specialists, 17 dermatological residents and 15 general physicians who classified PHL in 100 sets of photographs using both the BASP and Norwood-Hamilton classifications. They found that BASP classification not only distinguishes all kinds of hair loss patterns, but also has better reproducibility and repeatability than the Norwood-Hamilton classification.[11] The prevalence of FPHL (Ludwig grade >I) for all ages was 11.8%, increasing with advancing age.[12] The Asian Consensus Committee for AGA developed an algorithmic guideline, based on the BASP classification since the pre-existing classifications of AGA cannot easily classify the patterns of AGA that are more frequently seen in Asians.[13]
Limitations
When fronto-parietal and vertex regions of alopecia have become confluent, type F2 and F3 can be confused with type V.
The subjects were mostly out-patients so it is not indicative of the prevalence and the types of PHL in the general populations.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Hamilton JB. Patterned loss of hair in man; types and incidence. Ann N Y Acad Sci. 1951;53:708–28. doi: 10.1111/j.1749-6632.1951.tb31971.x. [DOI] [PubMed] [Google Scholar]
- 2.Norwood OT. Male pattern baldness: Classification and incidence. South Med J. 1975;68:1359–65. doi: 10.1097/00007611-197511000-00009. [DOI] [PubMed] [Google Scholar]
- 3.Savin RC. A method for visually describing and quantitating hair loss in male pattern baldness. J Invest Dermatol. 1992;98:604. [Google Scholar]
- 4.Olsen EA. Female pattern hair loss. J Am Acad Dermatol. 2001;45:570–80. doi: 10.1067/mjd.2001.117426. [DOI] [PubMed] [Google Scholar]
- 5.Olsen EA. Current and novel methods for assessing efficacy of hair growth promoters in pattern hair loss. J Am Acad Dermatol. 2003;48:253–62. doi: 10.1067/mjd.2003.81. [DOI] [PubMed] [Google Scholar]
- 6.Ludwig E. Classification of the types of androgenetic alopecia (common baldness) occurring in the female sex. Br J Dermatol. 1977;97:247–54. doi: 10.1111/j.1365-2133.1977.tb15179.x. [DOI] [PubMed] [Google Scholar]
- 7.Ekmekci TR, Sakiz D, Koslu A. Occipital involvement in female pattern hair loss: Histopathological evidences. J Eur Acad Dermatol Venereol. 2010;24:299–301. doi: 10.1111/j.1468-3083.2009.03411.x. [DOI] [PubMed] [Google Scholar]
- 8.Sehgal VN, Kak R, Aggarwal A, Srivastava G, Rajput P. Male pattern androgenetic alopecia in an Indian context: A perspective study. J Eur Acad Dermatol Venereol. 2007;21:473–9. doi: 10.1111/j.1468-3083.2006.01920.x. [DOI] [PubMed] [Google Scholar]
- 9.Koo SH, Chung HS, Yoon ES, Park SH. A new classification of male pattern baldness and a clinical study of the anterior hairline. Aesthetic Plast Surg. 2000;24:46–51. doi: 10.1007/s002669910009. [DOI] [PubMed] [Google Scholar]
- 10.Lee WS, Ro BI, Hong SP, Bak H, Sim WY, Kim do W, et al. A new classification of pattern hair loss that is universal for men and women: Basic and specific (BASP) classification. J Am Acad Dermatol. 2007;57:37–46. doi: 10.1016/j.jaad.2006.12.029. [DOI] [PubMed] [Google Scholar]
- 11.Hong H, Ji JH, Lee Y, Kang H, Choi GS, Lee WS. Reliability of the pattern hair loss classifications: A comparison of the basic and specific and Norwood-Hamilton classifications. J Dermatol. 2013;40:102–6. doi: 10.1111/1346-8138.12024. [DOI] [PubMed] [Google Scholar]
- 12.Su LH, Chen LS, Chen HH. Factors associated with female pattern hair loss and its prevalence in Taiwanese women: A community-based survey. J Am Acad Dermatol. 2013;69:e69–77. doi: 10.1016/j.jaad.2012.09.046. [DOI] [PubMed] [Google Scholar]
- 13.Lee WS, Lee HJ, Choi GS, Cheong WK, Chow SK, Gabriel MT, et al. Guidelines for management of androgenetic alopecia based on BASP classification – The Asian Consensus Committee guideline. J Eur Acad Dermatol Venereol. 2013;27:1026–34. doi: 10.1111/jdv.12034. [DOI] [PubMed] [Google Scholar]