

Abstract
Taurodontism is a developmental disturbance of a tooth in which body is enlarged at the expense of the roots. An enlarged pulp chamber, apical displacement of the pulpal floor and lack of constriction at the cementoenamel junction are the characteristic features. It appears most frequently as an isolated anomaly. But its association with several syndromes and abnormalities has also been reported. Endodontic treatment of taurodont teeth is stated to be complex and difficult due to the complexity in the tooth morphology. This case report presents a case of taurodontism in permanent maxillary molars and their successful endodontic treatment.
Keywords: Bull tooth, karyotype, taurodontism
INTRODUCTION
Dental morphological triats are of particular importance in the study of phylogenetic relationships and the population offinities. One of the most important abnormalities in the tooth morphology is taurodontism. Taurodontism is a morpho-anatomical change in the shape of the tooth which usually occurs in the multirooted teeth. An enlarged body and the pulp chamber as well as apical displacement of the pulpal floor are the characteristic features.[1]
The term taurodontism comes from the Latin term tauros which means bull and the Greek term odus which means tooth (or) bull tooth. It was first described by Gorjanovic-Kramberger.[2] However, the term traurodontism was first introduced by Sir Arthur Keith in 1913 to describe molar teeth resembling those of ungulates particularly bulls. The etiology of taurodortism is unclear. It is thought to be caused by the failure of Hertwig's epithelial sheath diaphragm to invaginate at the proper horizontal level, resulting in a tooth with short root, enlarged body, an enlarged pulp and normal dentin.[1]
Previously, taurodontism was related to syndromes such as Klinefelter's and Down's. Today it is considered as an anatomic variance that could occur in a normal population. Taurodontism has been graded according to its severity as least pronounced (hypotaurodontism), moderate (mesotaurodontism) and most severe (hypertaurodontism). Shifman and Channel[3] also included an index to calculate the degree of taurondontism as shown radiographically [Figure 1].
Figure 1.
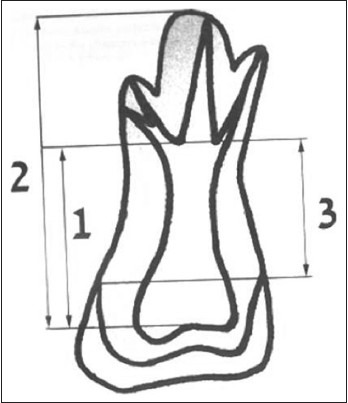
Taurodontism index: vertical height of the pulp chamber (1) distance between the lowest point of the roof of the pulp chamber to the apex of the longest root (2) and distance between the baseline connecting the two cement-enamel junction and the highest point in the floor of the pulp chamber (3). Establishment of a condition of taurodontism is made when1/2 multiplied by 100 is above 20, and 3 exceeds 2.5 mm: (1/2)* 100 > 20 and 3 > 2.5 mm. Taurodontic index (TI) = 1/2 × 100. In this case TI= 61 and 3= 8 mm, clearly indicating hypertaurodontism
Taurodontism although not common, a preoperative radiograph serve as an important tool for diagnosing the taurodontic condition and helps in preventing unexpected challenges while performing successful endodontic therapy.
The present case describes successful endodontic management of maxillary first molar with taurodontism.
CASE REPORT
A 25-year-old male patient was referred to Department of Conservative Dentistry and Endodontics, for the treatment of upper right and left first molar teeth. Intraoral examination revealed fracture of the palatal cusps with respect to 16 and buccal cusp fracture with respect to 26 [Figure 2]. At the time of examination, the teeth were asymptomatic. The teeth were not sensitive to percussion or palpation. Intraoral examination revealed a normal-shaped crown. Periodontal probing was within the normal range. Patient's medical history was noncontributory. Upon vitality testing, 26 showed positive response to thermal and electric pulp testing. The 16 showed no response to thermal and electric pulp testing indicating necrotic pulp. Intraoral periapical radiograph of 16 showed huge pulp chamber extending beyond the cervical area reaching the furcation in the apical third region [Figure 3]. Three short roots were seen at the furcation area in the apical third indicating hypertaurodontism. The intraoral periapical radiograph of contralateral 26 revealed similar findings [Figure 4]. The diagnosis of hypertaurodontism for the present case was made based on the radiographic finding and taurodont index as proposed by Shiffman and Chanannel [Figure 1].
Figure 2.

Palatal cusp fracture in relation to 16 and buccal cusp fracture in relation to 26
Figure 3.
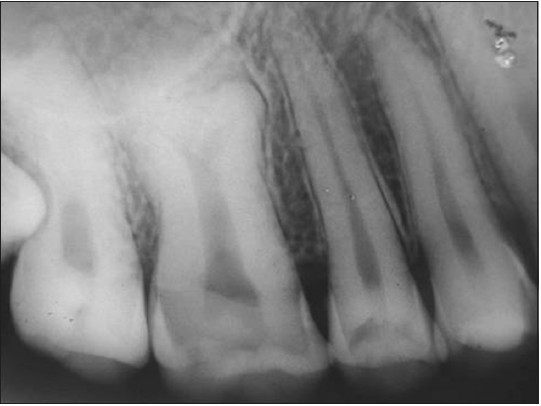
Preoperative radiograph of maxillary right first molar
Figure 4.
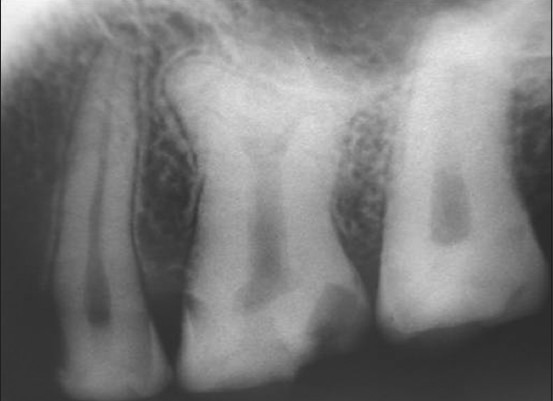
Radiograph of the contralateral maxillary left first molar
Endodontic management
The tooth was anesthetized with lidocaine 2% with epinephrine 1:1, 00,000 (Lignox 2% A Warren India). Magnifying loupes (Carl Zeiss, India) were used throughout the procedure to facilitate visualization. The tooth was isolated and access cavity prepared. The pulp tissue which was voluminous was extirpated. A total of 2.5% of sodium hypochlorite was used as irrigating solution. The furcation area was situated in the apical third region and three canal orifices were located at the furcation area; palatal, mesiobuccal and distobuccal.
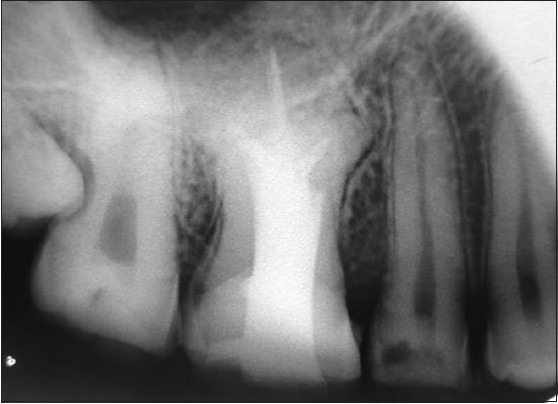
Working length determination was performed using electronic apex locator Propex II (Dentsply Maillefer, Switzerland, USA) and was confirmed with a radiograph [Figure 5]. After working length determination the instrumentation of the canals was done to size 40 for the palatal canal and up to size 30 for the mesial canals using RC prep (Premier, Ultradent, USA) as a lubricanting agent.
Figure 5.

Working length radiograph
A modified obturation technique was used because of complexity of inner root canal anatomy. This consisted of combined lateral condensation of the gutta percha in the apical part with vertical compaction of the remaining pulp chamber. AH-plus (Dentsply, Switzerland, USA) was used as a root canal sealer. The final radiograph confirmed well-obturated root canal system [Figure 6].
Figure 6.
Obturation radiograph
DISCUSSION
The taurodont tooth shows wide variation in the size of the pulp chamber, varying degrees of canal configuration like apically displaced furcation with a shorter root length and a less marked cervical constriction. The triat is usually seen in both permanent and primary teeth and is believed to be caused by failure of Hertwig's epithelial root sheath to invaginate at the proper horizontal level.[4] The reported rate of occurrence ranges from 0.57% to 4.37%. Taurodontism appears most frequently as an isolated anomaly; it has also been associated with several syndromes and anomalies including Klinefelter's, Down's, tricho-dento-osseous syndrome and others.
Taurodontism is a dental anamoly characterized by a distinct morphology.[6] In general, patient with more severe forms of the triat (meso or hyper) are more likely to have X-chromosomal aneuploidy. Varrela et al.,[5] supported the concept that prevalence of taurodontism increases as the number of X-chromosomes increases and also indicate that expression of the triat and the number of X-chromosomes may be positively correlated. They have further suggested that X-chromosomal gene influencing development of enamel may also be involved in the development of taurodontism.[5]
Gardner and Girgis recommend that patients with meso- or hypertaurodontic teeth who do not have a syndrome known to be associated with taurodontic teeth should be consulted for chromosome analysis, as there is a high association of taurodontic teeth with X-chromosome aneuploidy syndromes.[6]
In the present case, karyotype of the patient was studied to rule out the possibility of chromosomal aberrations. The results of the karyotype study showed no chromosomal aberrations [Figure 7].
Figure 7.
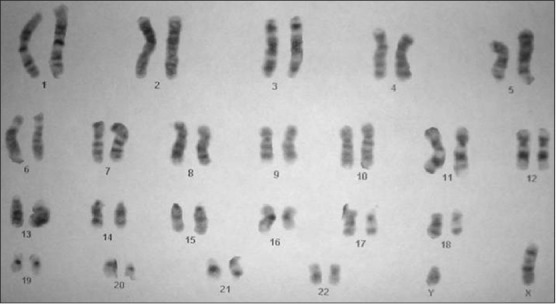
Karyotype from peripheral blood-Normal (46 XY)
The endodontic treatment in taurodont teeth has been described as complex and difficult. Durr et al.,[7] suggested that complexity in the morphology could hamper the location of the orifices thus creating difficulty in instrumentation and obturation.
The contributing factors for the successful endodontic treatment in such cases include careful exploration of the grooves between all the orifices particularly with magnification, ultrasonic irrigation and modified obturation techniques.[8]
In the present case also success in the root canal treatment was mainly attributed to use of magnifying loops for better visualization, use of 2.5% of sodium hypochlorite to dissolve the pulp tissue and was followed by modified obturation technique to achieve three-dimensional obturation of root canal system.
Another endodontic challenge related to taurodontism is intentional replantation. The extraction of taurodont tooth is usually complicated because of dilated apical third. In contrast, it has also been hypothesized that because of its large body, little surface area of the taurodont tooth is embedded in the alveolus. This feature would make extraction less difficult as long as roots are not widely divergent.[9]
From the periodontal stand point, taurodont teeth may in specific cases offer favorable prognosis. Here, the chances of furcation involvement are considerably less than those in normal teeth. Because taurodont teeth have to demonstrate significant periodontal destruction before the furcation involvement occurs.[10]
CONCLUSION
Although taurodontism is a dental rarity, this unusual radicular form showed merit circumspect consideration in treatment planning. The thorough knowledge of etiology, anatomic and radiographic features and its association with other syndromes of the dental rarity should be well-understood. Also, important consideration in performing endodontic treatment of such rarity is mandatory due to complexity of the root canal system.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Rajendran R. Shafer's Text Book of Oral Pathology. 7th ed. New Delhi (India): Elsevier ( Reed Elsevier India); 2009. Developmental disturbances of oral and paraoral structures; p. 45. [Google Scholar]
- 2.Gorjanovic-Kramberger K. On prismatic molar roots of recent and diluvial man. Anat Anz. 1908;32:401–13. [Google Scholar]
- 3.Shifman A, Chanannel I. Prevalence of taurodontism found in radiographic dental examination of 1,200 young adult Israeli patients. Community Dent Oral Epidemiol. 1978;6:200–3. doi: 10.1111/j.1600-0528.1978.tb01150.x. [DOI] [PubMed] [Google Scholar]
- 4.Bhatri R, Chandra A, Trikku AP, Wadhwani KK. “Taurodontism” and endodontic challenge: A case report. J Oral Sci. 2009;51:471–4. doi: 10.2334/josnusd.51.471. [DOI] [PubMed] [Google Scholar]
- 5.Yeh SC, Hsu TY. Endodontic treatment in taurodontism with Klinefelter's syndrome: A case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88:612–5. doi: 10.1016/s1079-2104(99)70094-6. [DOI] [PubMed] [Google Scholar]
- 6.Joseph M. Endodontic treatment in three taurodontic teeth associated with 48, XXXY Klinefeltors syndrome: A review and case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008;105:670–7. doi: 10.1016/j.tripleo.2007.11.015. [DOI] [PubMed] [Google Scholar]
- 7.Durr DP, Campos CA, Ayers CS. Clinical significance of taurodontism. J Am Dent Assoc. 1980;100:378–81. doi: 10.14219/jada.archive.1980.0100. [DOI] [PubMed] [Google Scholar]
- 8.Varrela J, Alvesalo L, Maghall J. Taurodontism in 45, X females. J Dent Res. 1990;69:494–5. doi: 10.1177/00220345900690021501. [DOI] [PubMed] [Google Scholar]
- 9.Varrela J, Alvesalo L. Taurodontism in 47, XXY males: An effect of the extra X chromosome on root development. J Dent Res. 1988;67:501–2. doi: 10.1177/00220345880670021401. [DOI] [PubMed] [Google Scholar]
- 10.Satyanarayanan R, Carounanidy U. Taurodontism–review and an Endodontic case report. Endodontology. 2001;13:8–10. [Google Scholar]