

Abstract
Objective
The present study aims at using trajectory analysis to measure labour market attachment (LMA) over 12 years and at examining whether labour market tracks relate to perceived health status.
Design
Data were retrieved from a 26-year prospective cohort study, the Northern Swedish Cohort.
Setting and participants
All ninth grade students (n=1083) within the municipality of Luleå in northern Sweden were included in the baseline investigation in 1981. The vast majority (94%) of the original cohort participated at the fourth follow-up. In this study, 969 participants were included.
Measures
Perceived health status (psychological distress and non-optimal self-rated health) at age 42 and the data obtained from questionnaires.
Results
We have identified four tracks in relation to LMA across the 12-year period: ‘permanent’, ‘high level’, ‘strengthening’ and ‘poor level’ of attachment. LMA history relates to psychological distress. High level (OR 1.55 (95% CI 1.06 to 2.27)), strengthening (OR 1.95 (95% CI 1.29 to 2.93)) and poor attachment (OR 3.14 (95% CI 2.10 to 4.70) involve higher OR for psychological distress compared with permanent attachment. The overall p value remained significant in the final model (p=0.001). Analyses regarding non-optimal self-rated health displayed a similar pattern but this was not significant in the final model.
Conclusions
Our results suggest that health status in mid-life, particularly psychological distress, is related to patterns of LMA history, to a large part independently of other social risk factors and previous health. Consideration of heterogeneity and time in LMA might be important when analysing associations with perceived health.
Keywords: Epidemiology, Occupational & Industrial Medicine, Public Health
Strengths and limitations of this study.
Using longitudinal data with exceptionally high response rate.
Applying trajectory analysis which only has previously been sparsely used in this field.
Provides a uniquely rich and detailed data on temporary contracts over a long period of time.
Relies on self-reported data.
Used a relatively small sample.
Introduction
During the past three decades or so, demands for a more flexible workforce have increased all over the world. Flexibility in the labour market is reflected, for example, in the proportion of temporary employees, which in recent years has varied between 13% and 15% of the total working population in Europe.1 To the individual, the consequence of flexible employment is that attachment to a workplace is weak and commonly interrupted by unemployment and other episodes out of work. In order to capture the total spectrum of employment relations, with regard to quality and quantity, we have chosen to work with the concept of ‘labour market attachment’ (LMA) in this study. In our definition of the LMA spectrum, we have included permanent, non-permanent employment, unemployment and those who are exempted from working.2–4
Some relations between labour market status and health status are widely accepted: permanent employment is considered beneficial to health, while unemployment is known to have adverse health effects5–7 and being out of the labour market in the long term is commonly due to poor health.8 But when it comes to the health implications of labour market status, between the extremes of the LMA spectrum, the evidence is much scarcer. Previous studies have proposed that temporary employment could be a risk of poor psychosocial work characteristics,9 with temporary employees more commonly experiencing job insecurity and having a low cash margin,10 which are some of the factors that can be potential pathways linking weak LMA to poor health. We have, for example, shown that long-term temporary employees often experience difficulties working full-time (underemployment) which influences their financial situation in a negative way11 and can thus be a source of worry.12 Poor health can also be mediated through job strain, although it seems as if this group is affected more by limited influence or control rather than high demands.13 Moderate LMA has been highlighted as potentially harmful for health status, but research on the topic is divergent.14 While some studies report worse self-rated health among temporary employees,15 a few studies even suggest better self-rated health among fixed-term employees.16 Some studies also indicate that deterioration in self-rated health may not be observable until the attachment is quite weak.17 A major answer to the mixed research results may lie in the inherent difficulty in capturing the changeable nature of employment. Measurement of the employment situation at one or a few points in time, as in most of the previous studies,18 19 may overlook the factual exposures to different positions. Health effects of temporary employment could surface after several years of accumulation, as we have shown in a previous report,20 or even when several years have passed after the exposure.21 Moreover, it is possible that it is the chain of passages in different employments, the trajectory of LMA, that contributes to health status; for example, becoming more strongly attached over time could contribute to health status differently than becoming less attached to the labour market even if the both groups hold same total exposure.
There are a lot of studies about particular labour market status as predictors of health. An inherent problem of such studies is the amount of exposure: cross-sectional information about status includes great variation, a variable based on the duration of the ongoing status is bound to use cross-sectional health data, and in prospective follow-up settings there may be periods in several status during the follow-up. The problem is of special importance in research on the health effects of atypical employment, as there are a wide range of status between permanent employment and overt unemployment. To address this topic, we have introduced a score that sums up the exposure to different types of non-permanent employment during the follow-up.20 The score, however, does not take into account the timing of the exposures. One way to capture the status chains, or the passages in and the transitions between different labour market positions, is provided by trajectory analysis. Applying this method with a four-class response variable (permanent employment, non-permanent employment, unemployment and out of the labour force), the members of the Northern Swedish Cohort have been clustered into six different ‘LMA tracks’.2 For the trajectory analysis of the present study, LMA was measured by a 10-class indicator, in order to articulate in more detail the trajectories of non-permanent employment and their association with health.
The few available studies about labour market trajectories in the field of public health have measured LMA at a few time points, for example, between one time point and another9 and the goal has been descriptive rather than analytic.19 22 In the present study, we have applied a refined scale with regard to LMA. In the measure, we have included a spectrum of various types of employment situations and also covered a time-span of 12 years. The method, trajectory analysis,23 offers a novel way to identify differential tracks of LMA history in our population cohort. After obtaining a relevant set of tracks, our aim is to examine in which ways they relate to non-optimal self-rated health or perceived psychological distress.
Method
Population and procedures
The study was initiated in 1981 and included all pupils in their last year of compulsory school (n=1083), in the medium-sized industrial town of Luleå in northern Sweden (95% of the cohort were born in 1965). Since 1981 four additional follow-ups have been conducted.24 The attrition rate in the most recent follow-up from 2007 was low; 94% (n=1005) of the original cohort who were still alive (n=1071) participated. Comprehensive questionnaires, completed by the participants in 1981, 1983, 1986, 1995 and 2007, were used as the main assessment method. This paper is based on data from the 1995 and 2007 follow-ups. Procedures of data collection are described more extensively elsewhere.24 The study was approved by the Regional Ethical Review Board in Umeå, Sweden.
Measurements
LMA history
We name the response variable of the trajectory analysis as LMA. It aims to serve as a conceptual and empirical tool to sort the employment status of the postindustrial labour market along a continuum.25 26 Crudely, it ‘refers to whether or not people have continuous employment (eg, all year or only part of it) and whether or not they have periods of unemployment’27 At headline level28 there are four major classes of LMA: non-employment, unemployment, temporary employment and permanent employment. Within each class, several subclasses can be discerned. In the present study, the interest is focused on differential temporary employment. Seen through LMA, temporary employment covers a set of positions defined by formal job contracts, regardless of the psychological contract,29 job commitment30 or perceived job insecurity.31
Participants’ labour market position from 1996 to 2007 was measured with a matrix consisting of columns representing half-year periods and rows representing different labour market positions. With the instruction ‘During which periods have you been employed permanently or have had some type of temporary job contract or have been out of work?’ the respondents were prompted to choose among 11 response options for each 6-month period: ‘permanently employed’ (coded as 10), ‘entrepreneur’ (9), ‘employed in project’ (8), ‘substitute’ (7), ‘probationary employment’ (6), ‘on-demand worker’ (5), ‘seasonal worker’ (4), ‘temporary employee for other reasons’ (3), ‘in employment policy measure’ (2), ‘unemployed’ (2) and ‘out of the labour market’ (1). Unemployment and participation in policy measure were merged, and each option was coded to a variable that expressed the strength of LMA on a scale from 10 to 1. The ranking of contracts has been tested in previous research on the accumulation of temporary employment20 and was based on Aronsson's core–periphery model,32 which proposes that there is a health gradient in relation to the type of employment contract. The model ranks contracts based on duration, possibility of on-the-job training, autonomy and job security.32 However, we have extended the ranking by also including three labour market positions of non-employment. In the event of ‘out of labour market’, a continuum of five or more periods (ie, 2.5 years) was required: if there were fewer than five, all periods were coded according to the last labour market position, to purposely exclude those on parental leave or studying from this category. As the last category, ‘out of labour market’ was given the lowest score in relation to LMA. The intention for this group was that it was supposed to be contained by those mainly on sickness benefit (supported by analysis, data not shown), not those temporarily not working due to parental leave or education. These operations thus yielded a score of the strength of LMA for each of the 24 successive half-year periods. The scores served as the data for the trajectory analysis.
Indicators of health status
Psychological distress at ages 30 and 42 was measured with a question that inquired whether the respondent had experienced in the previous year any of the following symptoms: restlessness, concentration problems, being worried or anxious, palpitations, anxiety or panic or other nervous problems. Reporting one or more of the six symptoms was coded as 1 and none as 0, equalling a dichotomisation into the quartile with the most symptoms versus the rest. The question was derived from the ‘Survey of living conditions’.33
Non-optimal self-rated health at ages 30 and 42 was measured with one question, ‘How do you rate your general health?’, with response options: good, average or bad.33 The responses were dichotomised into the quartile with the worst health (average or bad) coded as 1, and the rest (good) coded as 0.10 34
Covariates
Socioeconomic position is a strong predictor of health.35–38 LMA has been shown to be related to occupational class.39 It is important to consider socioeconomic position as a possible confounder when studying the relationship between temporary employment and illness. In this study, socioeconomic position (SEP) in 2007 was based on one question about occupation, which was classified according to the Swedish socioeconomic classification of occupational categories.40 Upper white-collar and self-employed were coded as 0, lower white-collar workers were coded as 1 and blue-collar workers were coded as 2.
Partnership and parenthood are also important factors in relation to LMA as these two may be postponed due to insecure working arrangement,39 41 which could influence social aspects related to illness.39 Marriage or having a partner is also important to consider when studying LMA, as it can be beneficial to health and financial resources.42 Parental status in 2007 was coded as 0 for those having children and as 1 for the childless. Marital status in 2007 was measured with one question: ‘Are you married or co-habiting?’ yes was coded as 0 and no as 1.
More women than men have poor LMA in terms of temporary employment.43 Gender has been considered as an important factor in relation to poor LMA and illness, where women's health might be at greater risk.44 Women were coded as 0 and men as 1.
Statistics
The participants were clustered according to the development of their LMA over the 12 years applying trajectory analysis.23 The method has been established as a way of studying individual developmental courses over age or time, and for identifying distinctive groups of individual trajectories within the population that emerge, instead of predefined criteria, from the data itself. Trajectory analysis consists of three steps. First, the appropriate probabilistic model is chosen for the response variable. The second step is to define the degree of the polynomial form of the trajectories. Finally, the number of the clusters is decided, employing the statistical information criteria and the ‘common sense criteria’ with respect to the substance and aims of the study. As a result, the developmental trajectories within clusters are as similar as possible, and trajectories between clusters are as different as possible.45 At individual level, cluster membership is dictated by the highest calculated posterior probability of belonging to a particular cluster.
Trajectory analyses were conducted with the Mplus program package. The analysis allowed for 12 time points, and the first and the second half of every second year were chosen in order to take into account the possible systematic seasonal variation of LMA.
We used logistic regression (OR and 95% CI) to test whether LMA history was associated with non-optimal self-rated health and psychological distress at age 42. Adjustments were made for the health indicator at age 30, gender, socioeconomic position, parental status and marital status. SPSS V.17 was used for the regression analyses. Women and men were analysed together to preserve power.
Results
The data consist of a 10-class ordinal indicator of LMA, and the form of probability distribution of longitudinal sequence of measurement for such variable is the multinomial distribution.
The adjusted Bayesian information criterion (BIC) value decreased from 17435.474 for the linear model to 16656.622 for the quadratic polynomial model, indicating that the latter can be preferred to the former. Other information criteria provided by the Mplus program likewise pointed in the same direction.
The optimal number of trajectories was searched by checking the solutions up to 1. The Adj. BIC was used for choosing the solution.46 The Adj. BIC value (as well as the other information criteria) decreased when the number of trajectories was increased, rapidly at the beginning and slower at the end. From seven-trajectory to eight-trajectory solution, the figure decreased from 17856.940 to 17606.402. Thereafter the decrease slowed down. We decided to continue with eight trajectories, as this solution provided, in addition to detailed depiction of differential LMA, the opportunity to exclude the cluster with 0 LMA that was outside our research interest.
Figure 1 illustrates the ‘labour market tracks’ based on means of the LMA scores at each time point of the individuals classified into each trajectory. Individuals on track 1 (3% of the cohort) also were excluded, as they were mainly disability pension recipients and their health was poor by definition. The track (6) of ‘permanent’ employment throughout the follow-up included more than half of the cohort, whereas the remaining six clusters were relatively small and there were relatively similar tracks. We collapsed these six clusters into three as follows. A considerable part (classes 2 and 3) maintained a continuously ‘high level’ of attachment, and about 12% (classes 5 and 7) displayed a ‘strengthening’ of attachment towards the end of the follow-up. The attachment was permanently weak in about 1 of 10 (class 8), and a small cluster with a U-shaped pattern (class 4) was also seen; we decided to collapse these clusters and defined their attachment as ‘poor’. In addition to being substantially grounded, this collapsing provided statistical power for subsequent analyses. Thus, we arrived at a four class ‘LMA history’ variable that comprised ‘permanent’ (class 6), ‘high level’ (classes 2 and 3), ‘strengthening’ (classes 5 and 7) and ‘poor’ (classes 4 and 8) LMA (figure 2).
Figure 1.
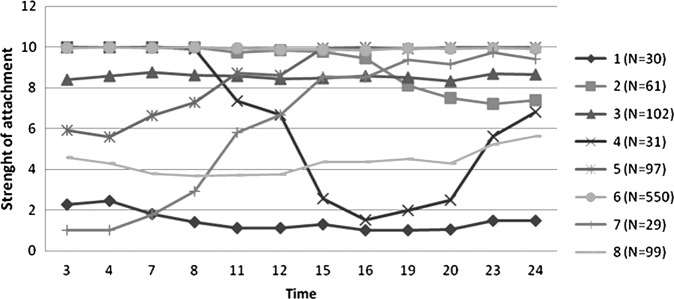
The number of cohort members clustered by trajectory analysis into eight tracks (curves based on means of the attachment at the time points).
Figure 2.

Collapsed tracks of labour market attachment history; permanent, high-level, strengthening and poor attachment.
Table 1 shows the distribution of the key variables by LMA history. In general, LMA history with less strong attachment entailed poorer health at age 42. Concerning covariates, similar patterns were seen for psychological distress and non-optimal self-rated health at age 30, thus indicating that health status differed between LMA history already at baseline. There were also significant differences with regard to socioeconomic position; the proportion of blue-collar workers was highest in the group with poor attachment to the labour market. The poor attachment group was also most likely to be living without a partner (p=0.010). Parental status did not differ between the groups. The proportion of women was higher in strengthening and poor-level attachment, whereas the permanent and high-level attachment were dominated by men (p=0.001).
Table 1.
Distribution (%) of dependent and independent variables in relation to labour market attachment (LMA) history
| Permanent, n=550 | High level, n=163 | Strengthening, n=126 | Poor, n=130 | p Value (χ2 test) | |
|---|---|---|---|---|---|
| Track | 0 | 1 | 2 | 3 | |
| Dependent variables at age 42 | |||||
| Psychological distress | 26.3 | 35.7 | 41.0 | 52.8 | <0.001 |
| Non-optimal self-rated health | 29.1 | 36.2 | 39.2 | 48.1 | <0.001 |
| Independent variables | |||||
| Health status at age 30 | |||||
| Psychological distress | 19.4 | 27.3 | 36.3 | 31.9 | <0.001 |
| Non-optimal self-rated health | 16.8 | 29.4 | 26.6 | 33.3 | <0.001 |
| Sociodemographics | <0.001 | ||||
| Blue-collar worker | 33.5 | 25.8 | 35.7 | 47.7 | |
| Lower white-collar worker | 15.7 | 8.0 | 18.3 | 6.2 | |
| Upper white-collar worker | 50.8 | 66.3 | 46.0 | 46.2 | |
| Single marital status | 19.1 | 20.9 | 22.2 | 32.6 | 0.010 |
| No child as parental status | 17.3 | 16.6 | 15.1 | 19.4 | 0.831 |
| Women | 44.5 | 42.3 | 61.9 | 55.4 | 0.001 |
All values are displayed in per cent, except p values.
To analyse whether LMA history was related to poor health, self-rated health and psychological distress were regressed on LMA history with permanent attachment as the reference category, in multiple logistic regression models (table 2). The LMA history had a significant overall p value on both health outcomes. In unadjusted analyses with psychological distress, lower strength of attachment involved higher odds than the permanent one (table 2, model 0; LMA history p<0.001). In model 0, we found increased OR in relation to lower attachment to the labour market, ranging from high level OR 1.55 (95% CI 1.06 to 2.27), strengthening OR 1.95 (95% CI 1.29 to 2.93) and poor OR 3.14 (95% CI 2.10 to 4.70). Adjusting for covariates (sociodemographic and psychological distress at age 30, models 1 and 2, respectively) resulted in attenuation of the ORs for those with ‘strengthening’ and ‘poor’ attachment. Finally, in the fully adjusted models (model 3), only the high level and poor attachment were significantly related to psychological distress, with the ‘poorly’ attached displaying the numerically strongest association (OR=2.52 CI 1.59 to 3.98). Although borderline significant, the OR for the ‘strengthening’ (OR=1.57 (95% CI 0.99 to 2.49)) attachment was of comparable strength to the ‘high level’ attachment (OR=1.54 (95% CI 1.01 to 2.35)). While with a slight decrease in OR along with adjustments for sociodemographic factors and previous health, the same pattern is still evident in the final model, and the overall p value remained highly significant (p=0.001).
Table 2.
Logistic regression analyses for two outcomes at age 42 in relation to exposure to LMA history (OR (CI 95%))
| Trajectories | Model 0 | Model 1 | Model 2 | Model 3 |
|---|---|---|---|---|
| Psychological distress as outcome | ||||
| Permanent, n=550 | 1 | 1 | 1 | 1 |
| High level, n=163 | 1.55 (1.06 to 2.27) | 1.56 (1.06 to 2.30) | 1.50 (0.99 to 2.28) | 1.54 (1.01 to 2.35) |
| Strengthening, n=126 | 1.95 (1.29 to 2.93) | 1.77 (1.17 to 2.69) | 1.68 (1.07 to 2.66) | 1.57 (0.99 to 2.49) |
| Poor, n=130 | 3.14 (2.10 to 4.70) | 2.77 (1.83 to 4.19) | 2.87 (1.83 to 4.49) | 2.52 (1.59 to 3.98) |
| p Value for LMA | <0.001 | <0.001 | <0.001 | 0.001 |
| Non-optimal self-rated health as outcome | ||||
| Permanent, n=550 | 1 | 1 | 1 | 1 |
| High level, n=163 | 1.38 (0.96 to 2.00) | 1.46 (1.00 to 2.13) | 1.19 (0.81 to 1.76) | 1.26 (0.85 to 1.87) |
| Strengthening, n=126 | 1.57 (1.05 to 2.36) | 1.52 (1.00 to 2.29) | 1.44 (0.94 to 2.20) | 1.40 (0.91 to 2.16) |
| Poor, n=130 | 2.26 (1.53 to 3.34) | 2.00 (1.34 to 3.00) | 1.83 (1.21 to 2.77) | 1.65 (1.08 to 2.53) |
| p Value for LMA | <0.001 | 0.003 | 0.025 | 0.087 |
Model 0 crude ORs.
Model 1 ORs adjusted for sociodemographic variables (socioeconomic position, gender, marital status and parental status).
Model 2 ORs adjusted for health status at age 30.
Model 3 ORs adjusted for models 1+2.
Results for non-optimal self-rated health were slightly less prominent than for psychological distress but pointed in the same direction. Unadjusted models (table 2, model 0) showed a significant overall relationship between LMA history and self-rated health (p<0.001), and the LMA history with ‘strengthening’ (OR=1.57 95% CI 1.05 to 2.36) and ‘poor’ (OR=2.26 CI 1.53 to 3.34) attachment had higher odds of having non-optimal self-rated health. For those with ‘high level’ (OR=1.38 CI 0.96 to 2.00) of attachment, the risk was numerically higher, although not significantly, than for those with ‘permanent’ attachment. After adjustment for health status at age 30 (model 2), the results for the ‘strengthening’ group were attenuated below significance. In the final model, only the OR for the ‘poor’ attachment group was significantly high, while the overall p value for the association of LMA history with non-optimal health dropped to borderline significance (p=0.087).
Discussion
In this study, we have identified four tracks of LMA history over 12 years: permanent, high level, strengthening and poor. Compared with the cohort with ‘permanent’ attachment, we found a higher probability of psychological distress among three cohorts with non-permanent LMA. The differences were partially attributed to previous health and to some extent also to sociodemographic variables; nevertheless, the overall contribution of LMA history remained significant in the fully adjusted model. The results for non-optimal self-rated health were similar but somewhat weaker.
Much of the previous research has suggested that temporary employment is a stepping stone towards more stable employment.47 In the present study, we found that, although the greater part of the sample already had a fairly strong attachment or were moving towards stronger attachment, one track remained poorly attached to the labour market over the 12 years. Thus, while the stepping stone hypothesis might be correct for the majority, a substantial minority appears to be trapped in an employment situation of permanent temporariness. Further, we found more women than men in this least favourable situation. This is probably explained by the widespread use of ‘on-demand employment contracts’ in women-dominated sectors of business43 such as care and welfare and education48 which are two industries which together stand for 33% of all temporary contracts in Sweden.11 These results can be interpreted as showing that, even though Sweden is considered one of the top-ranked gender-equal countries with regard to high labour market participation among women, the internal labour market is still gender-segregated.
Our findings importantly suggest that, in addition to the present LMA, the LMA history is important for health. In line with previous research, we found that the group with least attachment had the worst health status.15 17 As in our previous report showing a cumulative effect of temporary employment on health status,20 the present report further corroborates that employment history impacts on health status. However, a more nuanced picture emerged when the separate labour market tracks were considered.
First, even those with ‘high-level’ attachment experienced psychological distress more commonly than those with ‘permanent’ attachment. Thus, it appears that even marginal exposure to what could be labelled ‘LMA stress’ can contribute to psychological distress over time.
Second, the group with ‘strengthening’ attachment still experienced poor health more commonly than those with permanent attachment, even after adjustments for sociodemographic variables. This result suggests that earlier suboptimal attachment has a potentially ‘scarring’ effect. It is important to point out that in cross-sectional or short-term longitudinal designs, the ‘strengthening’ group would have been regarded as having a fairly favourable LMA. This particular finding, therefore, stresses the importance of taking the specific patterns of the long-term labour market history into account when examining associations with health status.
Third, among those poorly attached to the labour market is where we found the highest ORs for poor health. The poorly attached workers were also more likely to have other risk factors for psychological distress, which seemed to partly account for the association. For example, being single involves a lower average household income and decreases the level of control,49 and poor previous health could also contribute to difficulties in getting a stable attachment to the labour market, as those with health troubles could be less employable, particularly for blue-collar occupations.50 The poorly attached workers are also those with most experience of unemployment, which previously has been connected to mortality and morbidity.5 51 Thus, the poor mental health in this group seems to be a result not only of their enduringly unfavourable LMA history, but also of a range of coexisting burdensome life circumstances. As described in the introduction, job insecurity, financial stress, lack of reciprocity, uncertainty and lack of autonomy are some of the broad range of potential pathways linking temporary employment to poor health in previous studies.9 10 15 52–54 Although mediating mechanisms has not been within the scope of this article, our results can be understood in the light of potential pathways presented in previous research.
Methodological considerations
Our study relies on trajectory analysis, a method that became available in the beginning of the 2000s, largely by virtue of increased computing power. Instead of prefixing alternative developments, the analysis is seeking developmental trajectories that emerge from the data itself.17 It gives each individual posterior probability values for each trajectory, and allocates them according to the highest probability into groups or categories so that individuals within a group are more similar than individuals between groups.55 To our knowledge, trajectory analysis has been used only sparsely in previous studies about LMA.56 Our previous research using a core–periphery structure has only yielded a measure summarising the total accumulation of peripheral employment over 12 years,20 whereas this study has added new knowledge to the field by showing when exposure takes place and has provided patterns of labour market history, and this specific knowledge has hinted about potential scarring effects of poor LMA (seen in the strengthening group), knowledge that has previously been hidden due to methodological limitations. In general, this study represents novel methodological ideas in a research area that has been obscured by the practice of measuring the labour market position cross-sectionally or with short-term transitions between labour market positions.
The longitudinal design of this study has been an asset, as it made it possible to adjust for previous health, and thereby reduced the possibility of reverse causation, and especially as the attrition rate was kept low. Concerning the generalisability of this study, this cohort has been shown by a previous assessment to be representative of Sweden as a whole with respect to demographic data.24 It is plausible that health effects of poor LMA operate depending on the social context. For example, health implications might be more or less evident depending on structural factors such as national labour market policies, education system and legislation.57 Sweden is part of the Scandinavian welfare regimes which are considered to have strong Social Democratic values and government-funded benefits during episodes of unemployment. The welfare state Sweden could, therefore, possibly reduce negative health effects of flexible employment,58 which is in contrast to the results in our study. However, Swedish unions have criticised the current labour market regulations for being too liberal regarding temporary employment. With current regulations, it is possible to hire a substitute for up to 2 years and after that hire the same person on a general temporary employment contract for up to 2 years. This causes a situation where people are at risk of becoming long-term temporary.59 As a result of this, approximately 10% of all temporary employees have been employed by the same employer for 5 years or more. The Swedish labour market regulation could, therefore, be a reason for the noticeable finding in this study, where a substantial part of the workers followed remained poorly attached over the 12 years which were examined. Long-term temporary employment could be a future problem, and also a relevant group to study further in future research.
The sample size was limited in this study, which is a pointer for potential future research, which would benefit from analysing datasets with a larger sample size. Such studies would be able to stratify analyses of gender or socioeconomic position, which could enrich the understanding of the field of LMA and illness. In this study, we have focused on poor LMA as a risk factor for poor health, but there are a range of other circumstances relating to precarious employment which could explain the results, such as vulnerability, lack of benefits, low wages and disempowerment.44 Therefore, we would recommend future research to elaborate on other aspects of precariousness linked to poor LMA, as well as exploring the validity of the phenomena in a different context, for example, countries with different social and labour policies.
This study is based on self-reported data. Equivalent measures of self-rated health and psychological distress have displayed good validity by predicting future mortality and morbidity60 even after adjustments for known health risks.61 Furthermore, using retrospective measurement of LMA history could lead to recall bias. Nevertheless, retrospective questions about occupational history have been shown to maintain good quality in terms of agreement with census data.62
Further, the fact that we combined tracks could be seen as a limitation of this study. However, in our understanding, some of the tracks could be combined depending on their similar movement in the labour market. We first analysed each of the eight tracks separately in relation to the outcome, to make sure that none of the combinations resulted in blurring of the results (data not shown). One limitation regarding the method was that, due to features of the programme, only half of the time points (12 of 24 possible time points) could be included in the trajectory analysis. However, we used the first and second half of every second year to reduce the possibility of systematic error due to seasonal variations in employment status.
The structure behind the conceptualisation of LMA needs consideration. The LMA structure is based on the idea that there is a gradient in the labour market, with some positions being more strongly attached to the labour market than others. We have used a modified version of Aronsson's core periphery model32 to order the type of employment contract/situation, from the most attached to the least attached to labour market. Our structure is, indeed, a simplification of a more complex reality; this should be considered when interpreting the results. The LMA variable and socioeconomic position are partly overlapping, as the group of entrepreneurs is part of the SEP classification and the LMA variable. This overlap could cause over-adjustment in the logistic regression analysis. As these two variables partly measure the same phenomenon, adjusting for socioeconomic position could adjust for part of the true effect of LMA.
Conclusions
Policymakers frequently promote flexible employment contracts. However, this study shows that those with the most favourable but long-term high-level attachment suffer from worse health than those permanently attached. Further, despite a development towards favourable employment circumstances, health discrepancies can endure, suggesting a potentially ‘scarring’ effect. Finally, those poorly attached display the worst health situation, which is partly due to coexisting burdensome life circumstances. We firmly suggest that policymakers should consider the results of this study and take responsibility for creating employment opportunities suitable for maintaining a healthy working life, rather than promoting employment contracts characterised by poor attachment to the labour market.
Supplementary Material
Acknowledgments
The authors would like to thank all the participants in the Northern Swedish Cohort. Liudmila Lipiäinen and Tapio Nummi are thanked for contributing to this paper with regard to the trajectory analysis. The authors also thank Alan Crozier for professional language editing.
Footnotes
Collaborators: Liudmila Lipiainen; Tapio Nummi.
Contributors: AH, PEG, PV and A-KW have substantially contributed to conception and design. A-KW and PEG have contributed to analysis and interpretation of data. A-KW, AH, PV and PEG have drafted the article and revised it critically for important intellectual content. All authors have given their final approval of the version to be published.
Funding: This work was supported by Swedish Council for Working Life and Social Research [2006-0950] the Medical Faculty at Umeå University and the Academy of Finland [grant number 132668 to PV]. The study has been financed by The Swedish Research Council for Environment, Agricultural Sciences and Spatial Planning dnr 259-2012-37.
Competing interests: None.
Ethics approval: Regional Ethical Review board in Umeå, Sweden.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data sharing statement: The Northern Swedish Cohort is not freely available. Researchers who interested in collaboration should get into contact with the Principal Investigator, Anne Hammarström; anne.hammarstrom@umu.se
Contributor Information
Collaborators: Liudmila Lipiainen and Tapio Nummi
References
- 1.OECD Labour and Social Affairs. Incidence of temporary employment: OECD Online OECD Employment database [cited 12 December 2012]. 2012. http://www.oecd.org/employment/database
- 2.Virtanen P, Lipiäinen L, Hammarström Aet al. Tracks of labour market attachment in early middle age: a trajectory analysis over 12years. Adv Life Course Res 2011;16:55–64 [Google Scholar]
- 3.Furåker B, Berglund T. Changes of Employer, Employment Protection Legislation and Labour Market Attachment. 6th Conference in Memory of Professor Marco Biagi Modena, Italy 2008 [Google Scholar]
- 4.Department for Transport Data Sources for the Appraisal of Regeneration Impacts: TAG Unit 3.5.13. http://www.dft.gov.uk/webtag/documents/expert/pdf/unit3.5.13.pdf (accessed 18 Nov 2013). Government of the United Kingdom 2011
- 5.Dooley D, Fielding J, Levi L. Health and unemployment. Anu Rev Publ Health 1996;17:449–65 [DOI] [PubMed] [Google Scholar]
- 6.Hammarström A. Youth unemployment and ill health: results from a two-year follow-up study [in Swedish, summary in English]. Solna: Karolinska Institutet, 1986 [Google Scholar]
- 7.McKee-Ryan FM, Song ZL, Wanberg CRet al. Psychological and physical well-being during unemployment: a meta-analytic study. J Appl Psychol 2005;90:53–76 [DOI] [PubMed] [Google Scholar]
- 8.Brenner H, Ahern W. Sickness absence and early retirement on health grounds in the construction industry in Ireland. Occup Environ Med 2000;57:615–20 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Mauno S, De Cuyper N, Kinnunen Uet al. Work characteristics in long-term temporary workers and temporary-to-permanent workers: a prospective study among Finnish health care personnel. Econ Ind Democracy 2012;33:357–77 [Google Scholar]
- 10.Waenerlund AK, Virtanen P, Hammarström A. Is temporary employment related to health status? Analysis of the Northern Swedish Cohort. Scand J Public Health 2011;39:533–9 [DOI] [PubMed] [Google Scholar]
- 11.Waenerlund A-K. Temporary employment and illness. Department of public health and clinical medicine. Umeå: Umeå University, 2013 [Google Scholar]
- 12.Aronsson G, Dallner M, Lindh Tet al. Flexible pay but fixed expenses: personal financial strain among on-call employees. Int J Health Serv 2005;35:499–28 [DOI] [PubMed] [Google Scholar]
- 13.Parker SK, Griffin MA, Sprigg CAet al. Effect of temporary contracts on perceived work characteristics and job strain: a longitudinal study. Pers Psychol 2002;55:689–719 [Google Scholar]
- 14.Ferrie JE, Westerlund H, Virtanen Met al. Flexible labor markets and employee health. Scand J Work Environ Health 2008:98–10 [Google Scholar]
- 15.Kim MH, Kim CY, Park JKet al. Is precarious employment damaging to self-rated health? Results of propensity score matching methods, using longitudinal data in South Korea. Soc Sci Med 2008;67:1982–94 [DOI] [PubMed] [Google Scholar]
- 16.Virtanen P, Vahtera J, Kivimaki Met al. Employment security and health. J Epidemiol Community Health 2002;56:569–74 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Virtanen P, Liukkonen V, Vahtera Jet al. Health inequalities in the workforce: the labour market core-periphery structure. Int J Epidemiol 2003;32:1015–21 [DOI] [PubMed] [Google Scholar]
- 18.Bardasi E, Francesconi M. The impact of atypical employment on individual wellbeing: evidence from a panel of British workers. Soc Sci Med 2004;58:1671–88 [DOI] [PubMed] [Google Scholar]
- 19.Virtanen P, Vahtera J, Kivimaki Met al. Labor market trajectories and health: a four-year follow-up study of initially fixed-term employees. Am J Epidemiol 2005;161:840–6 [DOI] [PubMed] [Google Scholar]
- 20.Waenerlund AK, Gustafsson PE, Virtanen Pet al. Is the core-periphery labour market structure related to perceived health? Findings of the Northern Swedish Cohort. BMC Public Health 2011;11:10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Broughton A, Biletta I, Kullander M. Flexible forms of work: ‘very atypical’ contractual arrangements. European Foundation for the Improvement of Living and Working Conditions, 2010 [Google Scholar]
- 22.Liukkonen V, Virtanen P, Vahtera Jet al. Employment trajectories and changes in sense of coherence. Eur J Public Health 2010;20:293–8 [DOI] [PubMed] [Google Scholar]
- 23.Nagin DS. Analyzing developmental trajectories: a semiparametric, group-based approach. Psychol Methods 1999;4:139–57 [DOI] [PubMed] [Google Scholar]
- 24.Hammarström A, Janlert U. Cohort profile: the Northern Swedish Cohort. Int J Epidemiol 2012;41:1545.– [DOI] [PubMed] [Google Scholar]
- 25.Jones SRG, Riddell WC. Unemployment and nonemployment: heterogeneities in labor market states. Rev Econ Stat 2006;88:314–23 [Google Scholar]
- 26.Grzywacz JG, Dooley D. “Good jobs” to “bad jobs”: replicated evidence of an employment continuum from two large surveys. Soc Sci Med 2003;56:1749–60 [DOI] [PubMed] [Google Scholar]
- 27.Furåker B, Berglund T. Changes of employer, employment protection and labour market attachment: an analysis of Swedish data from 1972–1998. Gothenburg: University of Gothenburg, 2008 [Google Scholar]
- 28.Laux R. Measuring labour market attachment using the Labour Force Survey. Labour Market Trends [1361–4819] 1997;105:407 [Google Scholar]
- 29.Rousseau D. ed Psychological contracts in organizations: understanding written and unwritten agreements. Thousand Oaks, CA: Sage, 1995 [Google Scholar]
- 30.Meyer J, Paunonen S, Gellatly I, et al. Organizational commitment and job performance: it's the nature of commitment that counts. J Appl Psychol 1989;74:152–6 [Google Scholar]
- 31.Greenhalgh L, Rosenblatt Z. Job insecurity: toward conceptual clarity. Acad Manage Rev 1984;9:438–48 [Google Scholar]
- 32.Aronsson G, Gustafsson K, Dallner M. Forms of employment, work environment and health in to a centre—periphery perspective. Arbete och Hälsa (Work and Health). Stockholm: National Institute for Working Life, 2000 [Google Scholar]
- 33.Statistics Sweden Undersökning om levnadsförhållande [In English: Survey of living conditions]. Stockholm: Statistics Sweden, 1980 [Google Scholar]
- 34.Hammarström A, Virtanen P, Janlert U. Are the health consequences of temporary employment worse among low educated than among high educated? Eur J Public Health 2011;21:756.– [DOI] [PubMed] [Google Scholar]
- 35.Siegrist J, Marmot M. Health inequalities and the psychosocial environment—two scientific challenges. Soc Sci Med 2004;58:1463–73 [DOI] [PubMed] [Google Scholar]
- 36.Black D, Morris JN, Townsend Pet al. Inequalities in health. Report of a research working group. London: Department of Health and Social Security, 1980 [Google Scholar]
- 37.Marmot M, Allen J, Goldblatt Pet al. Fair society, healthy lives: strategic review of health inequalities in England post-2010 (the Marmot review). London: UCL, 2010 [Google Scholar]
- 38.Lynch J, Kaplan G. Socioeconomic position. In: Berkman LF, Kawachi I. eds Social epidemiology. New York: Oxford University Press, 2000:13–35 [Google Scholar]
- 39.Artazcoz L, Benach J, Borrell Cet al. Social inequalities in the impact of flexible employment on different domains of psychosocial health. J Epidemiol Community Health 2005;59:761–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Statistics Sweden Socioeconomisk indelning (SEI). Meddelande i samordningsfrågor 1982:4 (Swedish Socioeconomic Classification). Stockholm: Statistics Sweden, 1983 [Google Scholar]
- 41.Golsch K. Employment flexibility in Spain and its impact on transitions to adulthood. Work Employ Soc 2003;17:691–718 [Google Scholar]
- 42.Waldron I, Weiss CC, Hughes ME. Interacting effects of multiple roles on women's health. J Health Soc Behav 1998;39:216–36 [PubMed] [Google Scholar]
- 43.Aronsson G, Gustafsson K, Dallner M. Work environment and health in different types of temporary jobs. Eur J Work Organ Psy 2002;11:151–75 [Google Scholar]
- 44.Vives A, Amable M, Ferrer M, et al. Employment precariousness and poor mental health: evidence from Spain on a new social determinant of health. J Environ Public Health 2013;2013: 978656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Muthén B, Muthén L. Integrating person-centered and variable-centered analyses: growth mixture modeling with latent trajectory classes. Alcohol Clin Exp Res 2000;24:882–91 [PubMed] [Google Scholar]
- 46.Tolvanen A. Latent growth mixture modelling: a simulation study. Department of mathematics and statistics. Finland: University of Jyväskylä, 2007 [Google Scholar]
- 47.Cockx B, Picchio M. Are short-lived jobs stepping stones to long-lasting jobs? Oxf Bull Econ Stat 2012;74:646–75 [Google Scholar]
- 48.Statistics Sweden Women and men in Sweden 2012. Örebro: Statistics Sweden, 2012 [Google Scholar]
- 49.Mirowsky J, Ross C. Social causes of psychological distress. New York: Aldine De Gruyter, 2003 [Google Scholar]
- 50.Strully KW. Job loss and health in the US labour market. Demography 2009;46:221–46 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Bartley M. Unemployment and ill health—understanding the relationship. J Epidemiol Community Health 1994;48:333–7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Ferrie JE. Is job insecurity harmful to health? J R Soc Med 2001;94:71–6 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Tompa E, Scott-Marshall H, Dolinschi R, et al. Precarious employment experiences and their health consequences: towards a theoretical framework. Work 2007;28:209–24 [PubMed] [Google Scholar]
- 54.Facey ME, Eakin JM. Contingent work and ill-health: conceptualizing the links. Soc Theory Health 2010;8:326–49 [Google Scholar]
- 55.Jung T, Wickrama KAS. An introduction to latent class growth analysis and growth mixture modeling. Soc Pers Psychol Compass 2008;2:302–17 [Google Scholar]
- 56.Hynes K, Clarkberg M. Women's employment patterns during early parenthood: a group-based trajectory analysis. J Marriage Fam 2005;67:222–39 [Google Scholar]
- 57.Guest DE, Isaksson K, De Witte H, et al. Employment contracts, psychological contracts, and worker well-being: an international study. Oxford: Oxford University Press, 2010 [Google Scholar]
- 58.Kim IH, Muntaner C, Shahidi FVet al. Welfare states, flexible employment, and health: a critical review. Health Policy 2012;104:99–127 [DOI] [PubMed] [Google Scholar]
- 59.TCO Additional comment from TCO regarding infringement procedure 2007/4835 against Sweden. Stockholm the Swedish Confederation for professional employees. 2013. http://www.tco.se/Documents/Additionalcomments.pdf
- 60.Weitoft GR, Rosén M. Is perceived nervousness and anxiety a predictor of premature mortality and severe morbidity? A longitudinal follow up of the Swedish survey of living conditions. J Epidemiol Community Health 2005;59:794–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Idler EL, Benyamini Y. Self-rated health and mortality: a review of twenty-seven community studies. J Health Soc Behav 1997;38:21–37 [PubMed] [Google Scholar]
- 62.Wärneryd B, Thorslund M, Östlin P. The quality of retrospective questions about occupational history—a comparison between survey and census data. Scand J Soc Med 1991;19:7–13 [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.