

Abstract
Objective
This study explored the relationships among demographic (DVs) and clinical variables (CVs), neurocognitive (NOs) and functional outcome (FO) that could be used as prognostic factors for old aged patients with traumatic brain injury (TBI) undergoing or appointed disability evaluation (DE) after treatment.
Methods
A total of 162 subjects with TBI above the age of 55 years undergoing DE or appointed to do so after treatments were selected. The patients were divided into two subgroups according to age : a junior elderly group 55 to 64 years old and a senior elderly group over the age of 65. NOs and FO were evaluated using the Seoul Neuropsychological Screening Battery and Clinical Dementia Rating scale.
Results
Gender, age, and education level were shown to significantly impact the recovery of NOs after TBI. Other DVs and CVs such as area of residency, occupation, type of injury, or loss of consciousness were not found to significantly affect the recovery of NOs after TBI. Analysis of the relationships among DVs, CVs and NOs demonstrated that gender, age, and education level contributed to the variance of NOs. In FO, loss of consciousness (LOC) was included to prognostic factor.
Conclusion
Gender, age and education level significantly influence the NOs of elderly patients with TBI. LOC may also serve as a meaningful prognostic factor in FO. Unlike younger adult patients with TBI, old aged patients with TBI did not show global faking-bad or malingering attitudes to DE for compensation, but assume that they could faking their performance in a test set available visual feedback.
Keywords: Advanced age, Traumatic brain injury, Prognosis, Gender, Education
INTRODUCTION
Populations worldwide started to enjoy significantly longer life expectancies starting in the 20th century due to improved medical care and economic/social development. According to the Health and Affair Forum on "The Life Expectancy and Health-Adjusted Life Expectancy of Koreans"11), the life expectancy at birth in Korea was 80.7 years (76.8 years for males and 82.92 years for females), and 29.4% of individuals over 65 years old still maintain careers21). Given this aging revolution, it is fitting that the number of neurocognitive studies on elderly populations has increased greatly in the past decade14). However, brain injury or other physical trauma in old aged patients has not been the subject of disability evaluations or other forensic studies. Some studies have evaluated morbidity and mortality associated with brain injury in old aged populations and suggested that higher rates of mortality in older patients as well as neurologic deficits, even mild ones, result in poor prognosis18,19). Significant prognostic factors could serve as a gold standard for disability evaluations to determine indemnification or compensation. However, characteristics of brain injury in old aged Koreans have not been extensively studied, and advanced age is only part of a negative prognosis5). Furthermore, poorer outcomes of old aged patients with brain injury are not yet sufficiently explained by physiological monitoring data. In particular, reduced vascular versatility is likely to contribute to this occurrence6).
Studies of adult patients who have suffered brain injury or stroke demonstrated how age and injury severity are likely to interact given that increased age enhances the impact of injury severity. When injury severity is not taken into account, age alone does not appear to significantly impact the outcomes of young to middle aged patients14). In another study of prognostic factors for adults with brain injury, higher levels of education were found to be associated with good prognosis regardless of Glasgow Comma Scale (GCS) scores10). Additionally, they suggested that younger individuals showed better memory retention with the exception of patients who sustained severe traumatic brain injury (TBI), but in the severe TBI group, the meaningful effect of demographic variables was not noted by the cause of influence of severe brain injury. A systematic review of prognostic factors impacting the ability to return to work after sustaining brain injury provided strong evidence that the length of inpatient care is a negative prognostic factor while other factors do not appear to have any effect or have a minimal relationship with the overall prognosis23).
In a disability evaluation to determine indemnification or compensation for a loss, disability severity is based on patient status including demographic variables such as age, gender, education level, and career; clinical variables including GCS scores, radiological findings, physiological data collected just after brain injury, neurocognitive test results, and other functional datum on a status at now under disability evaluation. However, patient age is typically not considered for disability evaluation because age-matched individuals are compared in these types of assessments, thereby taking into account the normal aging process, particularly for older patients. In the present study, we evaluated neurocognitive and functional outcomes according to demographic and clinical variables as prognostic factors, and compared outcomes between junior and senior elderly patients for assess the effect of age old patients with TBI.
MATERIALS AND METHODS
Subject selection
A total of 506 patients above the age of 55 years who received hospital or ambulant treatment for a brain injury from April 2004 to August 2011 were recruited under an approved guideline for this retrospective study from the Institutional Review Board. From this group, 174 patients (34.0%) that had actually undergone disability evaluation, had been asked to this type of evaluation, or would do so in the future. Finally, seven patients (1.4%) with premorbid neurological abnormalities and five individuals (2.0%) who could not complete neurocognitive function tests due to a severe brain injury were excluded, leaving a total of 162 patients (32.0%) in the final study cohort.
Study procedure
The patients were divided into two groups based on age : a junior elderly (JE) group 55 to 64 years old and a senior elderly (SE) group over the age of 65 years. The relationship between neurocognitive and functional outcomes, demographic variables (including age, gender, educational levels, and occupation), and clinical variables (the cause of head injury, main types of head injury, loss of conscious, operation, comorbidity, hospitalization, and time between head injury and assessment) were evaluated. Furthermore, functional outcome was compared as same procedure, as also. Finally, we had assessed predicting values of all of variables for functional outcomes [Clinical Dementia Rating (CDR)-0--CDR-1 : most improved group vs. CDR-2--CDR-5 : mild improved group].
Neurocognitive outcomes were assessed using the Seoul Neuropsychological Screening Battery (SNSB) that includes standardized and validated tests for measuring a variety of cognitive functions12). The SNSB was administered in a standardized manner as part of a neurocognitive evaluation. Functional outcomes were evaluated using Korean Version of Expended CDR scale4). Testing was performed only when the participants were medically stable and could provide meaningful information. On average, testing was performed 20.90 (±34.92 standard deriation) months after injury.
Neurocognitive tests for evaluating neurocognitive outcomes
All patients underwent the SNSB to assess attention, language abilities, praxis, and the four elements of Gerstmann syndrome, calculation, body part identification, visuoconstructive function, verbal and visual memory, and frontal/executive functions. Subtests that provided numeric scores were also performed for comparison. These tests included the mini-mental status examination (MMSE) to calculate low and standard general mental state scores, a digit span test to measure attention span, the Korean version of the Boston naming test to obtain confrontational naming scores, the Rey-Osterrieth complex figure test to measure visuospatial functioning and visual memory, the Seoul verbal learning test to assess verbal memory abilities, a test of semantic fluency (animals and supermarket items), and the Stroop test (correct number of responses for reading words and naming the color of the font for 112 items during a 2-minute period). Age-, gender- and education-specific norms for each of the above tests based on assessments of 447 normal Korean participants were used for comparison12).
Korean version of Clinical Dementia Rating Scale
CDR is broadly accepted by clinicians as a staging measure for dementia, and although primarily developed for use in Alzheimer's disease, it has been employed for evaluation of non-Alzheimer dementias and as main index for functional impairments of old age with neurocognitive impairment in almost of disability evaluation8). CDR was developed at the Memory and Aging Project at Washington University School of Medicine in 1979 for the evaluation of staging severity of dementia and is a clinical staging instrument of dementia that combines 6 domains of cognitive and functional performance : memory, orientation, judgment and problem solving, community affairs, home and hobbies, and personal care15). We used Korean Version of Expanded CDR; CDR-0=none, CDR-0.5=questionable, CDR-1=mild, CDR-2=moderate, CDR-3=severe, CDR-4=profound, CDR-5=terminal4).
Statistical analysis
Descriptive statistics were calculated to determine the influence of different demographic variables on the recovery of neurocognitive functions following TBI. Two-way analysis of variances and a t-test were conducted to assess the overall differences between demographic and clinical variables, and result of the SNSB for each TBI subgroup. Multiple linear regression analyses were conducted to predicting the relationship between neurocognitive outcomes and demographic or clinical variables and the relationship between neurocognitive outcomes and functional outcome. Logistic regression analyses were conducted for functional outcomes by neurocognitive outcomes, demographic or clinical variables. p-values <0.05 were considered significant and data analysis was performed using SPSS version 20.0 (MS Windows Release 20.0)
RESULTS
Characteristics of demographic and clinical variables
Premorbid demographic characteristics of the two groups are presented in Table 1. No statistically significant differences were observed. The TBI patients (n=162) were predominantly male (71.0%) with a mean age of 65.02±6.34 years and an average of 6.01±4.54 years of education. The percentage of married participants was 86.4% and 52.5% resided in a rural area. Occupations at the time of injury were as follows : unskilled laborer/farmer (82.7%), merchants (6.2%), unemployed (7.4%), and clerical workers (3.7%). Over half (56.2%) of the patients had undergone a disability evaluation, and disability evaluation would be needed after treatment for the remainder.
Table 1.
Demographic data for the 162 subjects
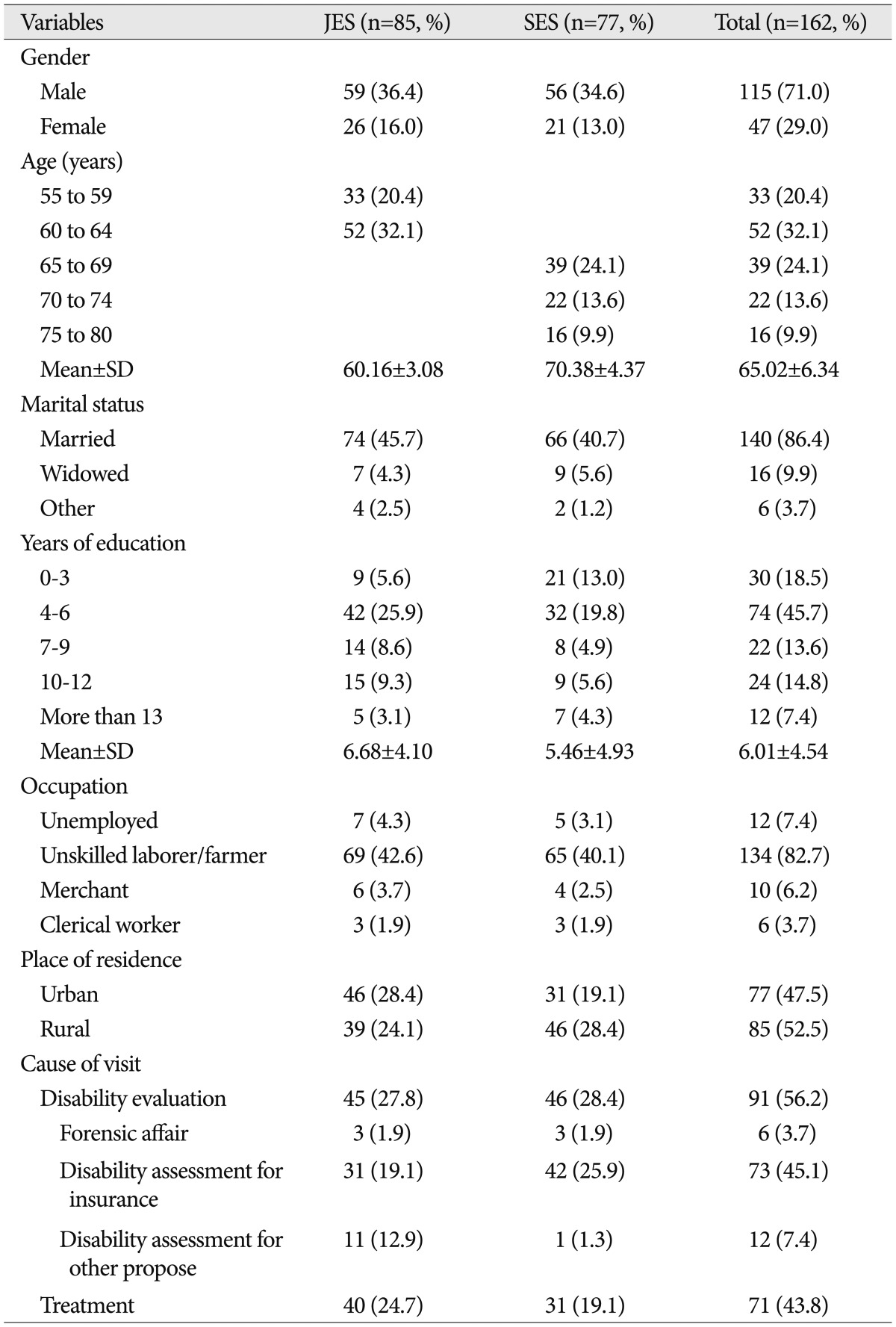
JES : junior elderly subjects, SES : senior elderly subjects, n : number of subjects, SD : standard deviation
Clinical characteristics of the TBI groups are presented in Table 2. The causes of TBI were traffic accidents as a pedestrian (54.3%), traffic accidents while in a car (33.2%), industry calamities (12.3%), and other occurrences (1.2%). The types of head trauma sustained included brain hemorrhage (95.2%), cerebral contusion (67.3%), cerebral hematoma (15.0%), diffuse axonal injury (11.8%), cerebral concussion (8.6%), and unknown injuries (15.8%). Loss of consciousness was experienced by 64.8% of the patients, 39.5% required an operation, 100.0% were hospitalized, and incidence of comorbidity due to the cause of TBI was 66.0%. The mean time interval between brain injury and assessment was 20.90±34.92 months.
Table 2.
Clinical characteristics of the 162 subjects
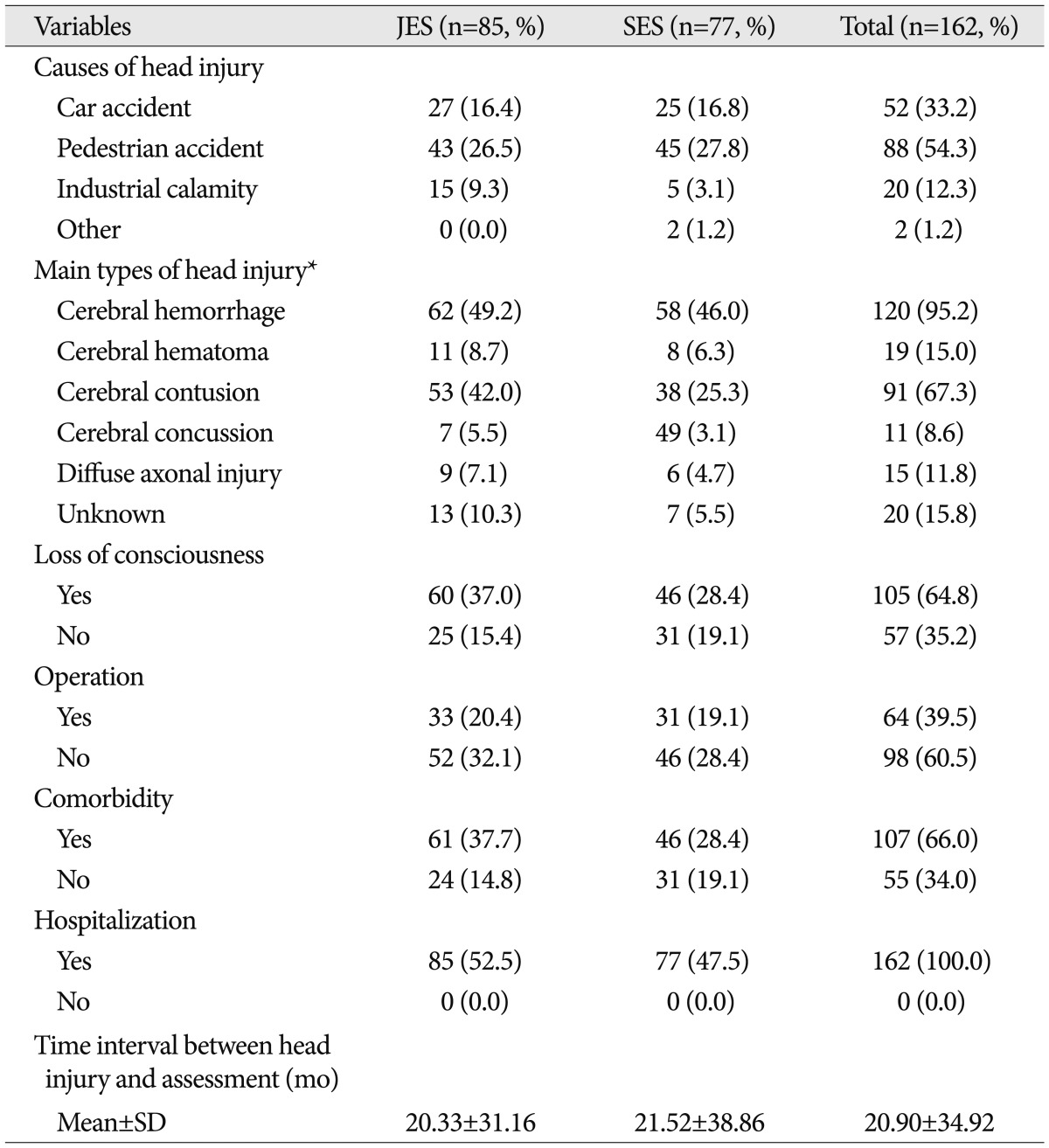
*Multiple counted ratio of main types of head injury. JES : junior elderly subjects, SES : senior elderly subjects, n : number of subjects, SD : standard deviation
Comparisons of neurocognitive outcomes between and among demographic variables
Comparisons between the junior elderly subjects (JES) and senior elderly subjects (SES) groups based on age did not show any significant differences for any of the neurocognitive outcomes and CDR score. Significant difference in low scores for MMSE (p<0.05), confrontational naming (p<0.01), and generative naming (p<0.05) were observed according to gender, but the interaction effects between gender and age group were not statistically significant (Table 3). Significant difference in standard scores for MMSE (p<0.01), attention (p<0.01), visuospatial functioning (p<0.01), and visual memory (p<0.05) were observed according to education level, but the interaction effects between gender and age were not statistically significant (Table 4). As shown in Fig. 1, low and standard scores changed according to educational level. In the JES group, low MMSE scores increased with the level of education, but standard MMSE scores decreased. In the SES group, the trends observed in the JES group were not found. Differences between area of residence and the interaction effect between residence and age were not statistically significant, and cause of visiting had not showed any statistical significance in any neurocognitive outcomes and CDR score.
Table 3.
Comparison of neurocognitive outcomes between groups according to gender
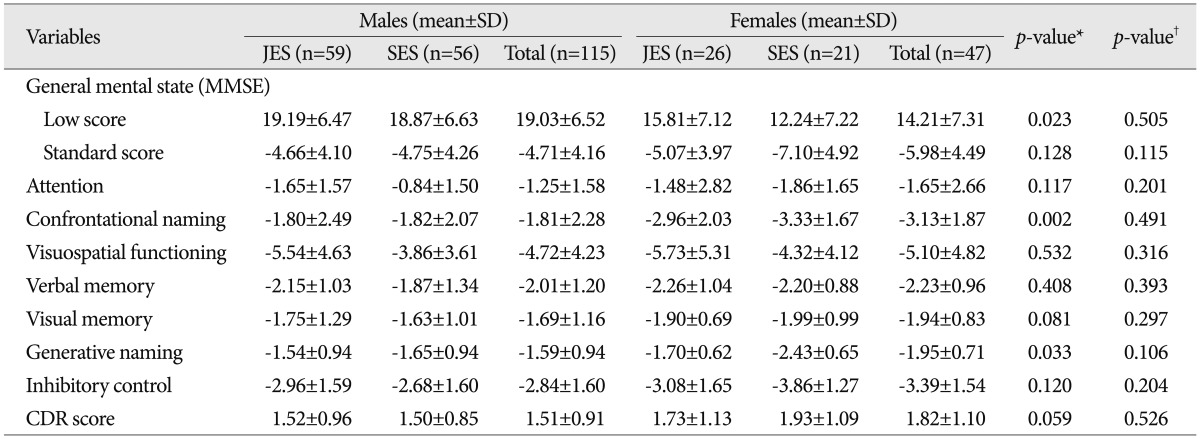
*p-value for main effect between gender, †p-value for interaction effect between age group and gender. CDR : Clinical Dementia Rating, JES : junior elderly subjects, SES : senior elderly subjects, n : number of subjects, SD : standard deviation, MMSE : Mini Mental State Examination
Table 4.
Comparison of neurocognitive outcomes between groups according to education level
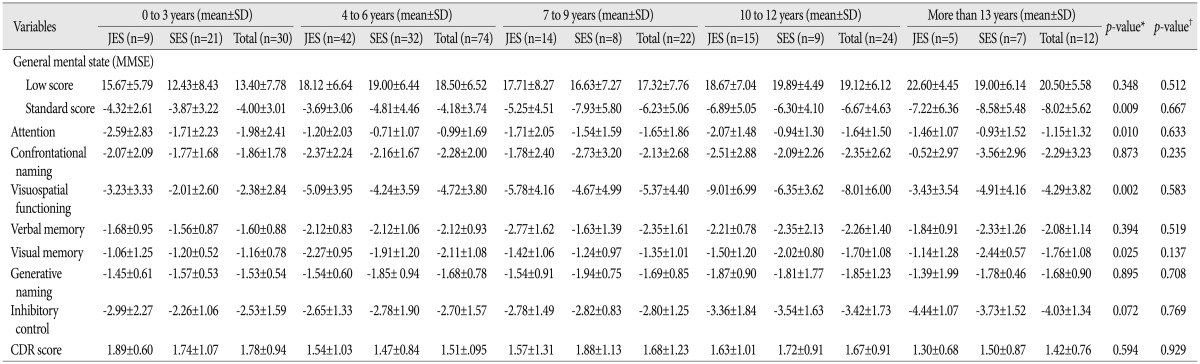
*p-value for main effect between gender, †p-value for interaction effect between age group and education period. JES : junior elderly subjects, SES : senior elderly subjects, n : number of subjects, SD : standard deviation, MMSE : Mini Mental State Examination, CDR : Clinical Dementia Rating
Fig. 1.

Distribution of MMSE low and standard scores according to years of education. JES : junior elderly subjects, SES : senior elderly subjects, MMSE : Mini Mental State Examination.
Relationships of neurocognitive outcomes between and among clinical variables
Loss of consciousness had not shown any statistical significance in any neurocognitive outcomes, and the interaction effects between loss of conscious and age were not statistically significant. Operated patients had shown poorer performance than not operated patents at confrontational naming (p<0.05), but the interaction effects between operations and age were not statistically significant. Comorbidity had not shown any statistical significance in any neurocognitive outcomes, and the interaction effects between loss of conscious and age were not statistically significant.
Predicting value of demographic and clinical variables for neurocognitive and functional outcomes
Multiple regression analyses among neurocognitive outcomes, demographic, and clinical variables showed some statistical significant results as shown in Table 5. At low score of MMSE, 13.5% of variance was explained by the gender (p<0.01) and 16.5% of variance at standard score of MMSE was explained by the gender and education (p<0.001). A 14.8% of variance at confrontational naming variable was explained by the gender and education (p<0.01), and 16.8% of variance at visuospatial functioning variable was explained by education (p<0.001). In memory ability, 11.8% of variance of verbal memory was age, education, comorbidity (p<0.05) and 10.4% of variance at visual memory variable was explained by cause of visit (p<0.05).
Table 5.
Multiple linear regression analysis for neurocognitive and functional outcomes
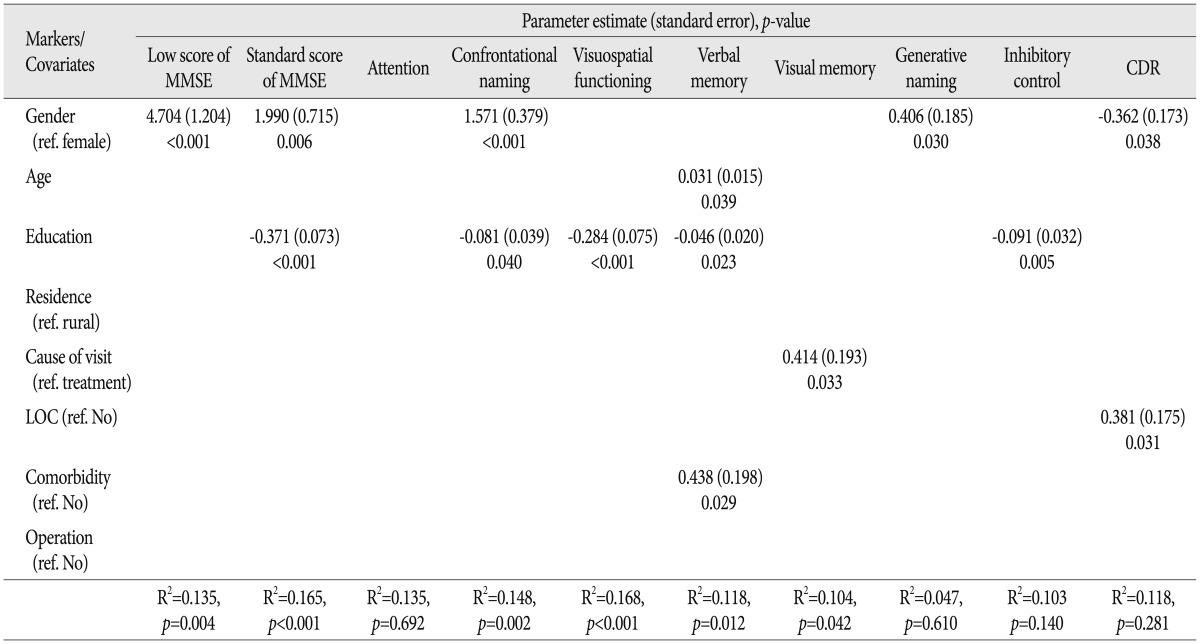
MMSE : Mini Mental State Examination, LOC : loss of consciousness, CDR : Clinical Dementia Rating
Logistic regression analysis for functional outcome by demographic, clinical variables and neurocognitive outcomes showed some statistical significant results as shown in Table 6, and education (odd ratio=0.781, 0.663-0.921, p<0.01), standard score of MMSE (odd ratio=0.701, 0.551-0.893, p<0.01), and visuospatial functioning (odd ratio=0.776, 0.616-0.978, p<0.05) showed statistically significant results.
Table 6.
Odds ratios for functional outcome
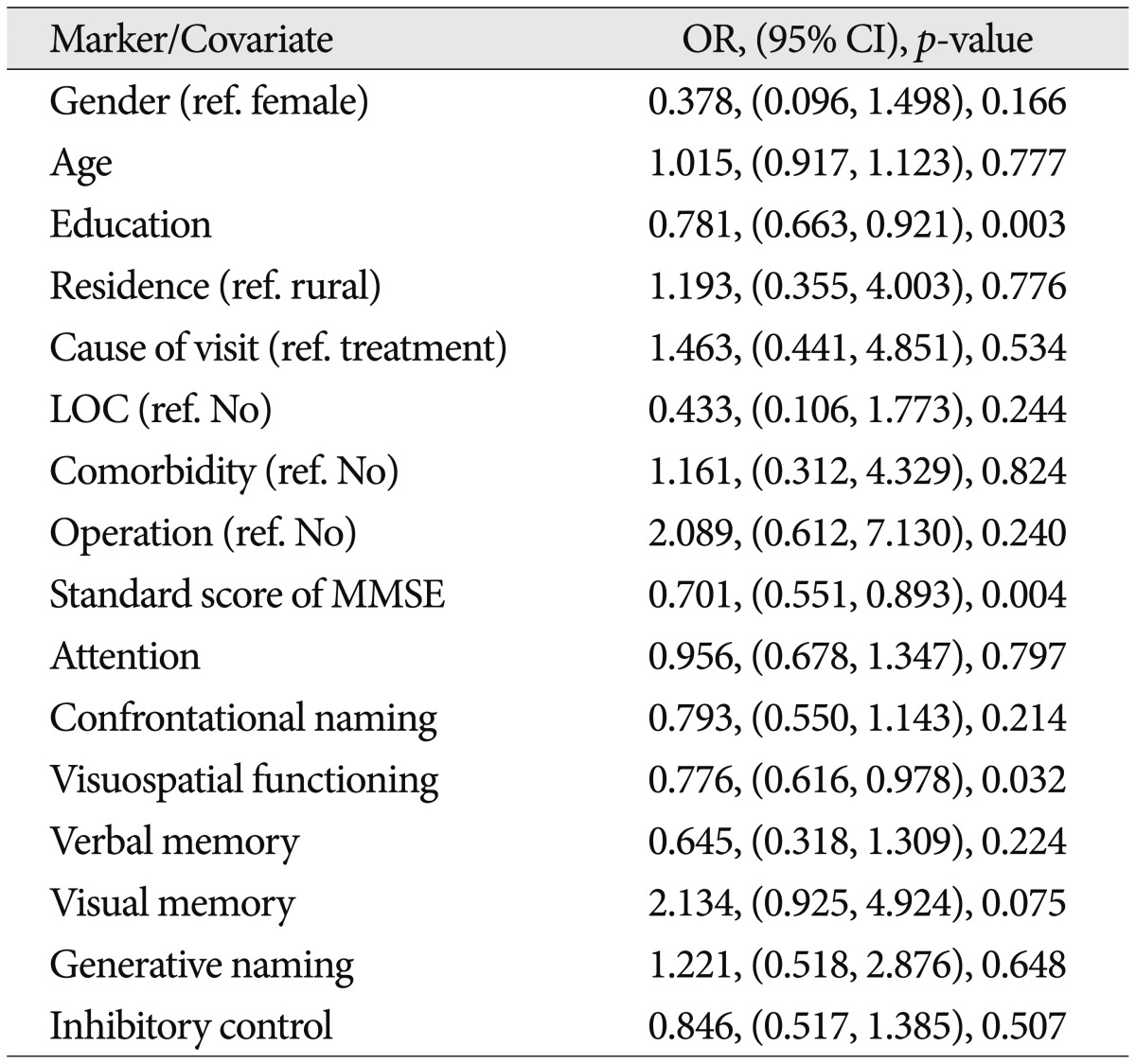
Values in the parentheses are 95% confidence interval (CI). OR : odds ratio, LOC : loss of consciousness, MMSE : Mini Mental State Examination
DISCUSSION
Clinicians treating patients often make therapeutic decisions based on their assessment of prognosis. An accurate prognostic evaluation is important when selecting specific methods of treatment, deciding whether or not to discontinue treatment, and when counseling patients and relatives16). For disability evaluation to determine indemnification or compensation for a loss, widely accepted prognostic factors for TBI treatment could be a gold standard for making a decision acceptable and fair to all interested parties. However, there is wide variety of opinions and research findings about prognosis after TBI as well as great variability in the quality of research2). These include patient age, clinical findings indicating the severity of brain injury (e.g., the depth and duration of coma or other neurological abnormalities), and the results of investigative and imaging studies, particularly intracranial pressure and computed tomography scanning, which disclose the nature of the brain injury and its effects on intracranial dynamics. Even though there is little doubt regarding the importance of these features, there are still debates about the precise nature of their relationships and exactly how these different factors should be assessed, categorized, and utilized3).
The most widely used variables or demographic characteristics of patients with TBI are age, gender, race and culture, premorbid mental abilities, education level, and premorbid personality and social adjustment. In particular, older adult show less improvement 1 year after TBI than younger ones, have a greater number of complications including subdural hematomas, and are less likely to survive a severe injury14). Although advanced age at the onset of TBI is a severe risk factor, it does not significantly affect some areas of disability evaluation. Decrements or impairment of neurocognitive outcomes in old aged patients with TBI are evaluated in the context of normal neurocognitive aging processes by comparison to healthy individuals in the same age range. Consequently, clinician should concerned to not a onset age of TBI but a difference from a normal neurocognitive aging process of old aged patient with TBI when performing a disability evaluation.
In the present study, we compared junior elderly and senior elderly patient with TBI to explore the effects of normal aging. The age of 55-65 years may be a starting point of normal neurocognitive aging given that most neurocognitive functions of individuals this age are poorer than those of young adults. Results of the comparison between junior and senior elderly patients in the present study did not show significant differences among neurocognitive outcomes even for low MMSE scores. Almost all (92.6%) of the recruited patients were employed and would therefore need to undergo evaluation to determine how much compensation they would receive for their disability. Since premorbid unhealthy patients were excluded from our study, individuals undergoing disability evaluation were more active and healthy than most people of the same age. Furthermore, relationship between neurocognitive outcome and age were significant minimally, and verbal memory was affected or decreased by the onset age of TBI. Thus, though the evaluation of neurocognitive outcome was administrated and interpreted based on patient age or using age corrected norms, the onset age of TBI should be disregarded partially for old aged individuals.
Gender-related differences between the groups were identified for the low MMSE scores as well as the standard scores for confrontational naming and generative naming. Altogether, above 10% of the variance in neurocognitive functions was associated with gender, and male patients scored higher in these areas. Functional outcome using CDR showed similar results. The results of TBI outcomes are reported according to gender in only a small percentage of the published literature, but a quantitative review of those studies revealed that worse outcomes are observed in women after TBI7).
Standard MMSE scores corrected for age, gender, and education level did not show any significant difference. Thus, differences in low MMSE scores between genders was not a prognostic factor for recovery after TBI unlike gender difference in normal aging1,9). However, differences between genders in verbal abilities assessed by confrontational and generative naming could be considered a prognostic factor unlike a common sense about gender difference. Gender-associated differences and individual test performances in the context of neurocognitive differences between the genders must nevertheless be interpreted with caution14).
Next to age, the most widely accepted prognostic factor is education level. Higher levels of education are associated with greater cognitive functioning and decreased susceptibility to dementia24). But almost of criteria for dementia or dementia status in South Korea have not used statistically standardized comparison norms considering gender and education level. Low MMSE scores did not show any significant difference among educational levels, but significant differences in standard MMSE scores were observed, had significant trends with higher at education level, and old aged patients with higher education level showed lower standard score at same a low score. Furthermore, significant differences in attention, visuospatial functioning, and visual memory were observed according education level and almost of neurocognitive functions were affected by education level. Those results had replicated the prognostic value of education level about adult study10).
Another demographic factor did not show any congruently significant differences or relationship. The cause of visit (disability evaluation group versus disability evaluation appointed group after treatment) did now show significant difference each other, but explained some variances of visual memory performance. Adult patients that had undergone disability evaluation after TBI showed differences in neurocognitive outcomes according to the cause of visit, and showed lower performance than the treatment group (patients who were scheduled to undergo disability evaluation after recovering from TBI). This suggested that disability evaluation process has an effect on the test-taking attitude or will affect the attitude of the clinician administering the test or the patient actually taking the test intentionally or unintentionally20). Therefore, clinicians should not assume that old aged patients with TBI are "faking" their symptoms or injuries as adult patients with TBI, but assume that they could faking their performance in a test set available visual feedback.
An examination of head injury causes with respect to age demonstrated that there were an increased proportion of injuries secondary to falls and pedestrian accidents with advanced age. The primary etiology of TBI among old aged patients was falling. Certain age-related medical conditions may predispose individuals to falling. Cognitive impairment is also a significant risk factor for falls. This may be due to both decreased safety awareness and increased use of psychotropic medications13). In a prospective study of the Traumatic Coma Data Bank3), motor-vehicle accidents were the cause of injury in 55% of patients 15-25 years old whereas only about 5% suffered falls. In contrast, 45% of patients over 55 years old suffered falls and only about 15% were in motor-vehicle accidents. However, falling as a mode of injury did not appear to be an independent predictor of poor outcomes. Older patients have poor outcomes compared to younger individuals regardless of the cause of injury. However, in our study 87.5% of head injuries were caused by 'car accidents (33.2%)' or 'pedestrian accidents (54.3%)'. Subjects of our study had an occupation and had undergone disability evaluation or were appointed to do so. Therefore, the cause of head injury does not appear to be a suitable prognostic factor for the disability evaluation process of old aged patients with TBI.
Utilization of clinical prognostic factors such as the type of brain injury, GCS scores, or other characteristics is limited for old aged patients. The GCS was developed by Teasdale and Jennett22) in 1974 as an objective measure of the level of consciousness. Since then, a number of studies have confirmed a fairly high degree of inter- and intra-rater reliability of the GCS among observers with a wide variety of experience levels3). Classical clinical features with prognostic significance for patients with TBI include age, GCS scores, pupil reactivity, brainstem reflexes, and the presence of post-traumatic hypotension. Many patients today arrive at the hospital already intubated, paralyzed, and ventilated. An accurate estimation of changes in GCS scores during the initial hours after trauma is therefore often difficult to obtain. In a survey of patients with severe and moderate head injuries conducted by the European Brain Injury Consortium, the full GCS scores were only testable for 56% of patients upon admission to neurosurgery17). In our study, 64.8% of subjects had a loss of consciousness, 66.0% of subjects had comorbidity, but they did not showed any significant difference at neurocognitive outcomes. In 39.5% of subjects with operation, they had showed lower performance at confrontational naming, only than had not operated. Functional outcome of old aged patient with TBI were assessed by intensive interviews based on evaluated neurocognitive outcomes as CDR and lead to a final decision of disability evaluation compromising all of data acquired in evaluation process. In those final process, gender, LOC, standard score of MMSE, education and visuospatial function were adopted by critical marker.
CONCLUSION
The present study showed a relationship among demographic, clinical variables, neurocognitive outcomes, and functional outcomes as prognosis factors for old aged patients with TBI undergoing or directed to undergo disability evaluation after treatment. Gender, LOC, and education level were found have a significant impact on determining the prognosis of these individuals. Gender should also be carefully considered as a meaningful prognostic factor. Furthermore, onset age of old aged patients with TBI should be disregarded partially for old aged individual using age corrected norms. Unlike adult patients with TBI under disability evaluation, old aged patients with TBI had not affected by disability evaluation itself for compensation, but assume that they could faking their performance in a test set available visual feedback. In a previous study of adult patients with TBI10) comparisons were made according to TBI severity based on the GCS. For old aged individuals, comparison of GCS scores and other clinical variables was limited because the caregivers or guardians of these patients were also old aged and could not provide an accurate medical history. Therefore, further studies should be conducted to identify prognostic features based on the results of medical examinations such as CT scanning, information with important therapeutic implications for operative intervention, and indications for intracranial pressure monitoring would include for providing information concerning prognostic significance.
Acknowledgements
This Work was supported by the 2010 Yeungnam University Research Grant.
References
- 1.Albert M, Duffy FH, Naeser M. Nonlinear changes in cognition with age and their neuropsychologic correlates. Can J Psychol. 1987;41:141–157. [PubMed] [Google Scholar]
- 2.Carroll LJ, Cassidy JD, Peloso PM, Borg J, von Holst H, Holm L, et al. Prognosis for mild traumatic brain injury : results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J Rehabil Med. 2004;(43 Suppl):84–105. doi: 10.1080/16501960410023859. [DOI] [PubMed] [Google Scholar]
- 3.Chesnust RM, Ghajar J, Maas AIR, Marion DW, Servadei R, Teasdale GM, et al. Brain Trauma Foundation, American Association of Neurological Surgeons, editors. Management and Prognosis of Severe Traumatic Brain Injury. New York: Brain Trauma Foundaion; 2000. Early indicators of prognosis in severe traumatic brain injury; pp. 1–116. [Google Scholar]
- 4.Choi SH, Na DL, Lee BH, Hahm DS, Jeong JH, Yoon SJ, et al. Estimating the validity of the Korean version of expanded clinical dementia rating (CDR) scale. J Korean Neurol Assoc. 2001;19:585–591. [Google Scholar]
- 5.Choi SW, Koh HS, Yeom JY, Kim SH, Song SH, Kim Y. Clinical analysis of the risk factors and prognostic factors of delayed deterioration following mild head injury. J Korean Neurosurg Soc. 1999;28:1316–1323. [Google Scholar]
- 6.Depreitere B, Meyfroidt G, Roosen G, Ceuppens J, Grandas FG. Traumatic brain injury in the elderly : a significant phenomenon. Acta Neurochir Suppl. 2012;114:289–294. doi: 10.1007/978-3-7091-0956-4_56. [DOI] [PubMed] [Google Scholar]
- 7.Farace E, Alves WM. Do women fare worse? A metaanalysis of gender differences in outcome after traumatic brain injury. Neurosurg Focus. 2000;8:e6. doi: 10.3171/foc.2000.8.1.152. [DOI] [PubMed] [Google Scholar]
- 8.Fillenbaum GG, Peterson B, Morris JC. Estimating the validity of the clinical Dementia Rating Scale : the CERAD experience. Consortium to Establish a Registry for Alzheimer's Disease. Aging (Milano) 1996;8:379–385. doi: 10.1007/BF03339599. [DOI] [PubMed] [Google Scholar]
- 9.Hyde JS, Linn MC. Gender differences in verbal ability : a meta-analysis. Psychol Bull. 1988;104:53–69. [Google Scholar]
- 10.Jeon IC, Kim OL, Kim MS, Kim SH, Chang CH, Bai DS. The effect of premorbid demographic factors on the recovery of neurocognitive function in traumatic brain injury patients. J Korean Neurosurg Soc. 2008;44:295–302. doi: 10.3340/jkns.2008.44.5.295. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Jeung YH. The Life Expectancy and Health-Adjusted Life Expectancy of Koreans. Health Welf Policy Forum. 2012;193:5–18. [Google Scholar]
- 12.Kang YU, Na DL. Seoul neuropsychological screening battery. Incheon: Human Brain Research & Consulting Co; 2003. [Google Scholar]
- 13.Kim E. Elderly. In: Silver JM, McAllister TW, Yudofsky SC, editors. Textbook of Traumatic Brain Injury. Arlington: American Psychiatric Publishing, Inc.; 2005. pp. 495–508. [Google Scholar]
- 14.Lezak MD, Howieson DB, Bigler ED, Tranel D. Neuropsychological Assessment. ed 5. New York: Oxford University Press; 2012. pp. 354–361. [Google Scholar]
- 15.Morris JC. The Clinical Dementia Rating (CDR) : current version and scoring rules. Neurology. 1993;43:2412–2414. doi: 10.1212/wnl.43.11.2412-a. [DOI] [PubMed] [Google Scholar]
- 16.MRC CRASH Trial Collaborators. Perel P, Arango M, Clayton T, Edwards P, Komolafe E, et al. Predicting outcome after traumatic brain injury : practical prognostic models based on large cohort of international patients. BMJ. 2008;336:425–429. doi: 10.1136/bmj.39461.643438.25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Murray GD, Teasdale GM, Braakman R, Cohadon F, Dearden M, Iannotti F, et al. The European Brain Injury Consortium survey of head injuries. Acta Neurochir (Wien) 1999;141:223–236. doi: 10.1007/s007010050292. [DOI] [PubMed] [Google Scholar]
- 18.O'Neill S, Brady RR, Kerssens JJ, Parks RW. Mortality associated with traumatic injuries in the elderly : a population based study. Arch Gerontol Geriatr. 2012;54:e426–e430. doi: 10.1016/j.archger.2012.01.007. [DOI] [PubMed] [Google Scholar]
- 19.Park YS, Kim HJ, Whang K, Pyen JS, Hu C, Hong SK. Clinical characteristics and prognosis of mild head injury in the elderly. J Korean Neurosurg Soc. 2002;31:564–568. [Google Scholar]
- 20.Shin TH, Gong CB, Kim MS, Kim JS, Bai DS, Kim OL. Development of a cognitive level explanation model in brain injury : comparisons between disability and non-disability evaluation groups. J Korean Neurosurg Soc. 2010;48:506–517. doi: 10.3340/jkns.2010.48.6.506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Statistics Korea. Press materials : Statistics of old ages at 2011. Seoul: Statistics Korea; 2012. [Google Scholar]
- 22.Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet. 1974;2:81–84. doi: 10.1016/s0140-6736(74)91639-0. [DOI] [PubMed] [Google Scholar]
- 23.van Velzen JM, van Bennekom CA, Edelaar MJ, Sluiter JK, Frings-Dresen MH. Prognostic factors of return to work after acquired brain injury : a systematic review. Brain Inj. 2009;23:385–395. doi: 10.1080/02699050902838165. [DOI] [PubMed] [Google Scholar]
- 24.Wilson RS, Hebert LE, Scherr PA, Barnes LL, Mendes de Leon CF, Evans DA. Educational attainment and cognitive decline in old age. Neurology. 2009;72:460–465. doi: 10.1212/01.wnl.0000341782.71418.6c. [DOI] [PMC free article] [PubMed] [Google Scholar]