

Abstract
Background/Aims
To date, it has been difficult to determine the optimal stenting duration of a fully covered self-expandable metal stent (FCSEMS) in a benign biliary stricture. The purpose of this study was to identify the histopathological changes in a bile duct resulting from long-term placement of a FCSEMS.
Methods
An FCSEMS was inserted into the common bile duct of 12 canines, and the animals were divided into four groups. Posteuthanasia, necropsy was performed to examine the histopathological changes in the bile ducts after 1, 3, 6, and 9 months.
Results
The results of necropsy showed that the covered membranes of the FCSEMSs were intact and easily removed from the bile ducts in 11 of the canines. Severe epithelial hyperplasia of the stented bile duct and epithelial ingrowth into the stent occurred in one animal (from the 3-month group). On histopathological examination, mild inflammatory changes were observed in the stented bile ducts, and there was no significant difference between the four groups. Among the 12 animals, five had de novo stricture.
Conclusions
An FCSEMS can be inserted into the bile duct without severe histopathological changes up until 9 months. However, a de novo stricture and severe epithelial hyperplasia relating to the stent insertion might occur.
Keywords: Stents; Common bile duct; Common bile duct disease; Cholangiopancreatography, endoscopic retrograde; Dogs
INTRODUCTION
A self-expandable metal stent (SEMS) has proven to be a useful palliative method in unresectable malignant biliary obstruction.1,2 In particular, the SEMS has been the preferred option for palliation of malignant biliary obstructions owing to its long patency duration compared with the plastic stent, especially in patients with longer predicted survival times.3-5 There are three different types of SEMS, namely an uncovered SEMS (UCSEMS), a partially covered SEMS (PCSEMS), and a fully covered SEMS (FCSEMS). Among these, a UCSEMS has the following disadvantages: occurrence of tumor ingrowth or epithelial hyperplasia in the bile duct between uncovered meshes, thereby creating possible stent occlusion, and difficulty in the removal of the stent once it has embedded in the bile duct.6-8 To overcome these disadvantages, an FCSEMS has been developed and used. An FCSEMS can prevent tumor ingrowth or epithelial hyperplasia as the covered membrane is made of polyurethane, silicone, or polytetrafluoroethylene, thereby extending the patency duration of the stent and facilitating removal of the stent if required. Therefore, it is now being used in disorders such as benign biliary strictures, bile leakages, and main pancreatic duct strictures accompanied by chronic pancreatitis.9-14 Sustained efficacy of an FCSEMS on benign obstructions generally requires a longer duration of stenting to induce sufficient remodeling. However, since there are few studies on the optimal duration of the placement of a stent for which an FCSEMS is efficiently maintained and safely removed, it has been difficult for an FCSEMS to be used in benign disease. As time goes by, the covered membrane of an FCSEMS begins to crack, and bile duct epithelial cells can then grow into the stent through this opening.15-17 As a result, an FCSEMS may become immovable from the bile duct because the stent is embedded in the bile duct. Surprisingly, there are few well-designed animal studies investigating the long-term use of an FCSEMS in the bile duct.18
The aim of this study was to examine the microscopic changes in the stented bile duct in a canine model and to establish the optimal duration of the temporary placement of an FCSEMS.
MATERIALS AND METHODS
Subjects
For this experiment, we used 12 mongrel dogs weighing about 20 to 25 kg each. In our study, dogs were chosen because the average size of the canine bile duct is within the range of the normal human bile duct. Moreover, animal handling and endoscopic intervention are usually easier in dogs than in pigs.19-21 All experimental procedures were performed in accordance with the National Institutes of Health guidelines for the humane handling of animals and were approved by the Committee on Animal Research at our institution.
Experiment method
Pretreatment
The animals were fed a soft liquid diet, starting from 48 hours before the procedures; then, food was withheld, except for only a small quantity of water, 24 hours before the procedures. Before the procedures, blood sampling was performed on all the animals to measure the baseline levels of aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, γ-glutamyl transferase, and total bilirubin. They were anesthetized with intramuscularly injected ketamine hydrochloride (Yuhan, Seoul, Korea) and atropine sulfate (Daewon, Seoul, Korea) before the procedures, and anesthesia was maintained throughout the procedures with intravenous ketamine hydrochloride. Each procedure was performed by placing the animal in the left lateral decubitus position.
Endoscopic procedure
As biliary strictures in dogs are uncommon, we used a normal biliary model. Stents were placed using an oral transpapillary approach via a 3.8-mm endoscope (ED-3630T video duodenoscope; Pentax, Tokyo, Japan). When an endoscope was extended to the major duodenal papilla, the bile duct was cannulated with a catheter, and a cholangiogram was obtained. The diameter and length of the FCSEMS were 8 mm and 4 to 5 cm, respectively. An FCSEMS is made of nitinol wire and is fully covered on both sides with a silicone membrane. Stents were deployed over a guidewire under endoscopic and fluoroscopic guidance. They were positioned proximal to the papilla to prevent distal stent migration during the study, and the correct position was confirmed by fluoroscopy (Fig. 1).
Fig. 1.

Stent deployment under fluoroscopic guidance. (A) Cholangiography of a normal canine bile duct. (B) Fluoroscopic image of a guidewire placed inside the bile duct. (C) The stent is placed above the papilla. (D) The stent is in place after withdrawal of the delivery catheter and guidewire.
Postprocedure follow-up
After the endoscopic procedure, the animals were monitored continuously until full recovery from the anesthesia. The animals were monitored daily by a veterinary technician. Clinical signs, including weight loss, pain, and jaundice, were monitored daily, as well as food intake, respiratory rate, and heart rate for the first week and weekly thereafter.
Necropsy
Blood sampling was carried out as a follow-up procedure before necropsy. We performed euthanasia and necropsy on the animals after 1 (dogs 1 to 3), 3 (dogs 4 to 6), 6 (dogs 7 to 9), and 9 months (dogs 10 to 12) from the date of the stent placement. The animals were euthanized with an overdose of xylazine hydrochloride (Rompun; Bayer, Seoul, Korea). Following euthanasia, the liver, common bile duct, gall bladder, and duodenum were removed, and between them, the common bile duct was carefully separated. Then, we incised the separated common bile duct longitudinally and carefully removed the FCSEMS from it. The FCSEMS and common bile duct were observed in their entirety to check for the presence of any de novo stricture of the bile duct, stent patency, and disruption of the covered membrane of the stent. Finally, the common bile duct was placed in a formalin solution.
Histology
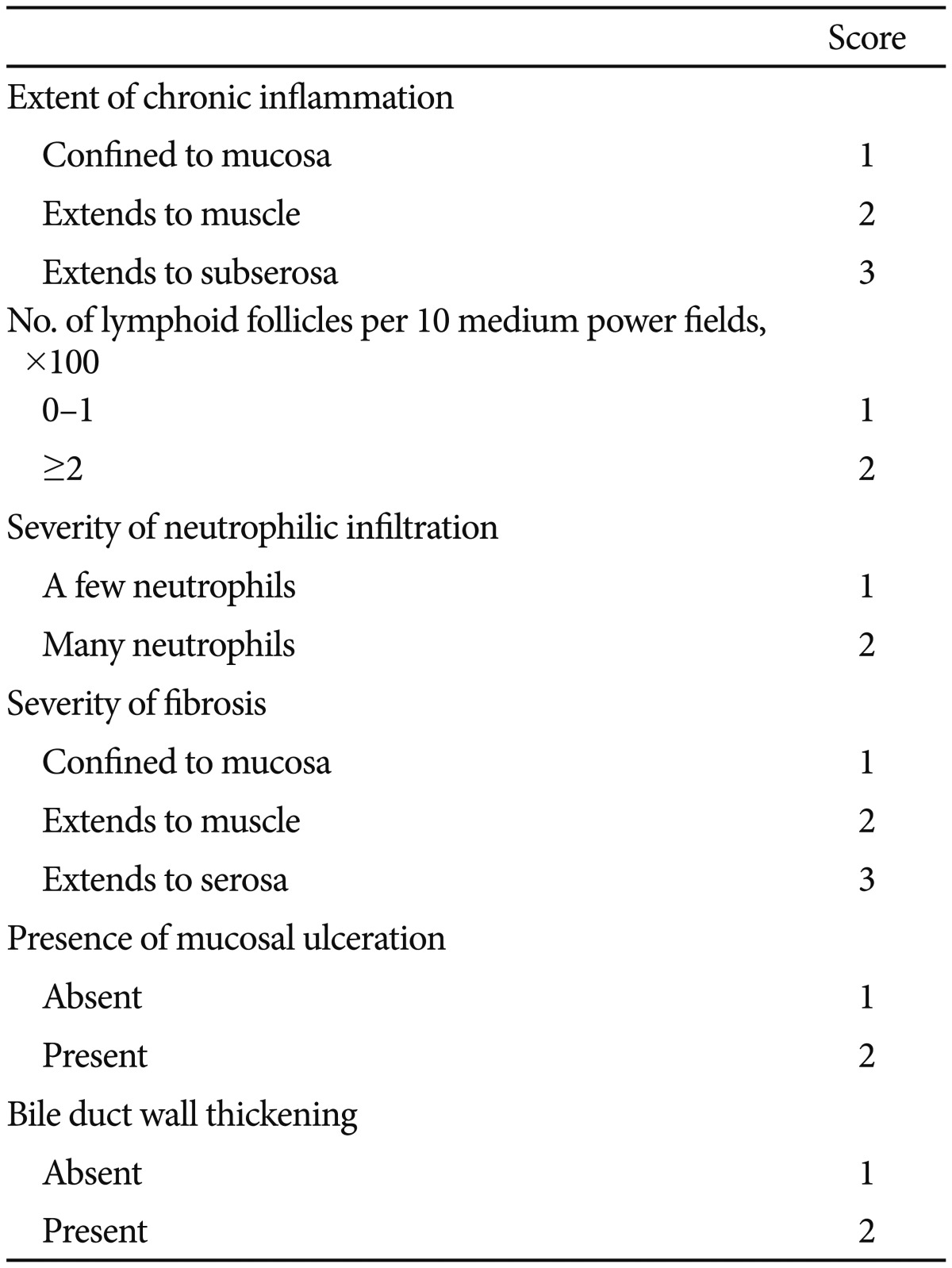
A histopathological examination was performed on the unstented bile duct, and on the proximal, middle, and distal portions of the stented bile duct (Fig. 2). The sections were examined with H&E and Masson trichome stainings for general histological features. A single pathologist (M. Joo) created the scoring system to determine the degree of inflammation, fibrosis, and epithelial injury, including the extent of chronic inflammation, number of lymphoid follicles, severity of neutrophilic infiltration, severity of fibrosis, presence of mucosal ulceration, and bile duct wall thickening. Each parameter is summarized in Table 1.
Fig. 2.
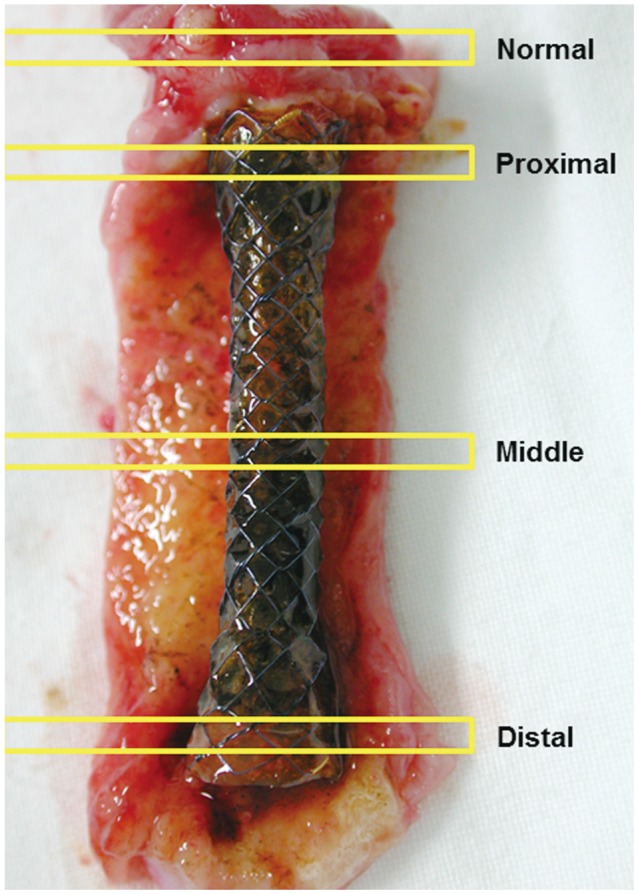
Four levels of histopathological examination. Cross section of an unstented (normal) bile duct, and the proximal, middle, and distal portions of the stented bile duct.
Table 1.
The Scoring System Used to Determine the Severity of Inflammation of the Stented Bile Duct
RESULTS
Initial stent placement
All the 12 animals had successful placement of an FCSEMS. No particular adverse events occurred during the stent insertion procedure in the 12 animals. After the insertion of the stent, we found no evidence of adverse events such as fever, jaundice, melena, and hematochezia, and all the animals ate food normally the day after the stent placement. During the follow-up period, all the animals showed appropriate weight gain, and there were no adverse events such as distal stent migration, cholecystitis, and pancreatitis.
Necropsy
The results of blood tests-including aspartate aminotransferase, alanine aminotransferase, alkaline phosphatase, γ-glutamyl transferase, and total bilirubin, which were performed before endoscopy and before necropsy-were all within reference range, and there was no significant difference between the two groups tests.
Proximal or distal stent migration was not observed in any of the animals during the follow-up period. Apart from one animal, the FCSEMS was removed easily from the bile duct in the other animals at the time of necropsy-after 1, 3, 6, and 9 months-with no adhesion to the common bile duct. In these 11 animals, the silicone membrane of the removed FCSEMS was intact, and no disruption of the membrane was observed (Fig. 3). One animal (dog 4), in which a stent had been placed for 3 months, showed severe epithelial hyperplasia and strong adhesion between the stent and the bile duct, making removal of the FCSEMS very difficult. There was disruption of the covered membrane in this animal, and epithelial hyperplasia was observed inside the stent (Fig. 4). Complete stent obstruction was not found.
Fig. 3.

Macroscopic and microscopic findings of the stented bile duct (dog 6). (A) Macroscopic examination of the stented bile duct, showing superficial inflammation. (B) Chronic inflammation is confined to the mucosa (H&E stain, ×40). (C) There are a few neutrophils in the lamina propria (H&E stain, ×200). (D) Fibrosis extends to the muscle layer, but smooth muscle bundles are intact (red spindle cells; Masson trichrome stain, ×100).
Fig. 4.

Macroscopic and microscopic findings of the stented bile duct with severe inflammatory changes (dog 4). (A) A fully covered self-expandable metal stent became embedded in the bile duct owing to severe epithelial hyperplasia. (B) A low-magnification view reveals transmural inflammation and fibrosis (H&E stain, ×40). (C) Suppurative inflammation with many neutrophils is visible (H&E stain, ×200). (D) Masson trichome stain highlights extensive fibrosis (blue areas; H&E stain, ×100).
De novo stricture at the proximal or distal end of the stented bile duct was observed in five of the 12 animals (41.6%). These strictures were observed incidentally during necropsy because none of these five animals showed symptoms or signs of bile duct obstruction (Fig. 5).
Fig. 5.
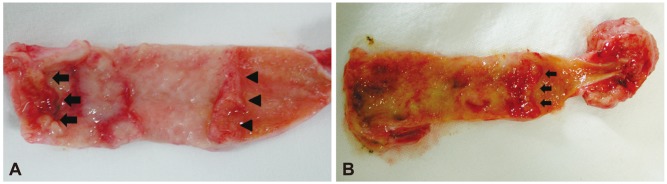
Macroscopic images of de novo stricture after removal of a fully covered self-expandable metal stent (FCSEMS). (A) De novo stricture occurred at both the proximal (arrows) and distal (arrowheads) portions of the bile ducts after placement of an FCSEMS for 9 months. (B) De novo stricture occurred at the distal portion of the bile duct after placement of an FCSEMS for 6 months (arrows).
Histology
The degree of chronic inflammation was mild to moderate, with no animal showing severe injury except for one (Fig. 3). One animal (dog 4), which had held an FCSEMS for 3 months, showed the most severe changes under histological examination, such as chronic inflammation, lymphoid follicle, neutrophilic infiltration, fibrosis, mucosal ulcer, and bile duct wall thickening (Fig. 4). On histological examination, we found no significant difference between the animals in terms of the length of time in which an FCSEMS remained in situ (1, 3, 6, or 9 months) (Table 2, Fig. 6).
Table 2.
The Results of Microscopic Examination of the Stented Bile Duct
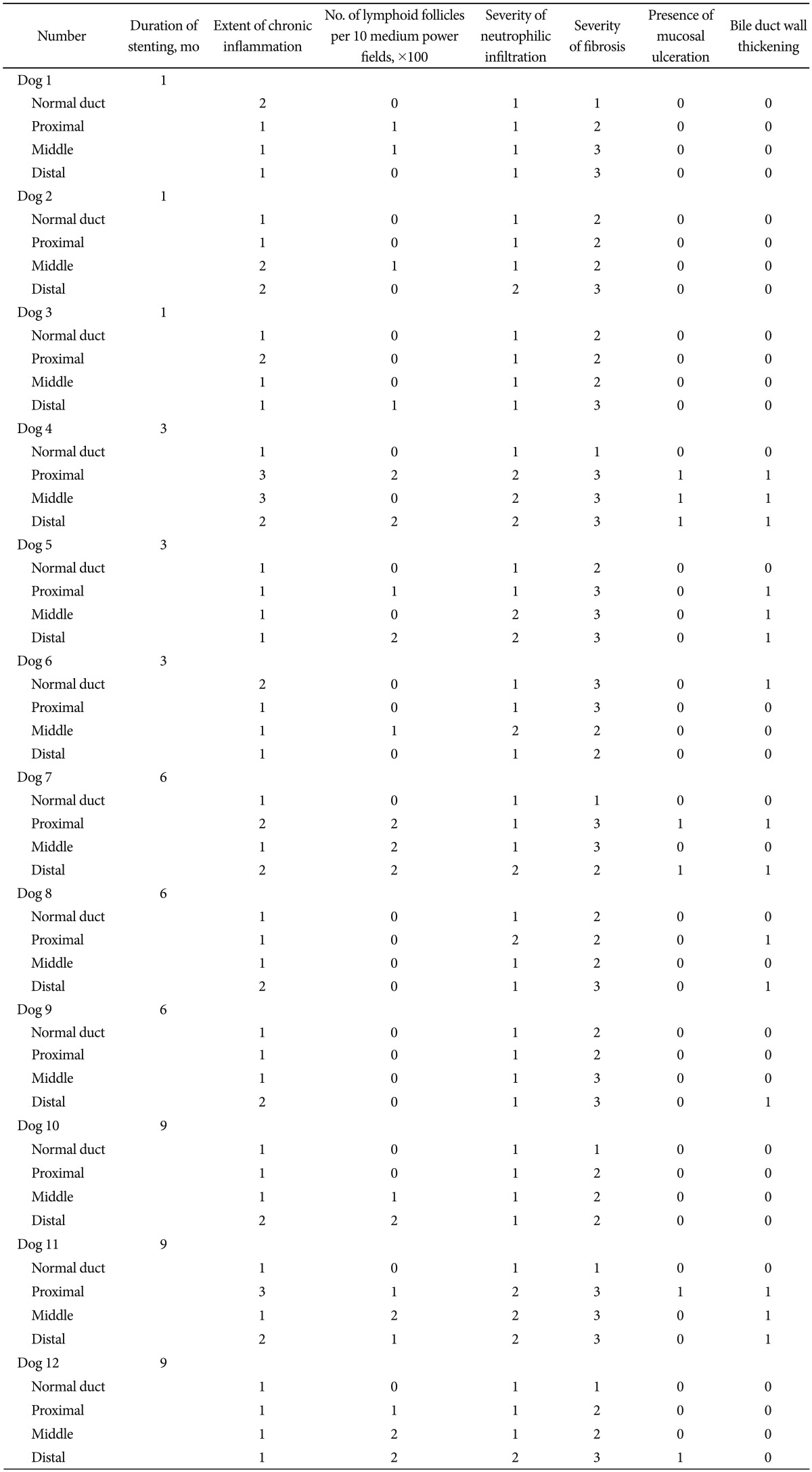
Fig. 6.

The results of microscopic examinations. (A) Microscopic examination of the normal (unstented) bile duct. (B) Microscopic examination of the proximal portion of the stented bile duct. (C) Microscopic examination of the middle portion of the stented bile duct. (D) Microscopic examination of the distal portion of the stented bile duct.
DISCUSSION
The results presented here provide valuable information on the histological changes in the bile duct in response to the long-term placement of an FCSEMS in a canine biliary model. In this study, when an FCSEMS was placed in the canine bile duct, stent patency was maintained for up to 9 months, and the inflammatory response of the bile duct to the FCSEMS was mild to moderate. Up until now, there have been few long-term and well-designed animal studies on the histological changes in the bile duct after an FCSEMS insertion. This study is significant because we observed changes in the bile duct in response to long-term placement of an FCSEMS for 9 months, which is a relatively long period.
As regards the choice of stent for biliary obstruction, it is known that bigger has been found to be better.22,23 Therefore, it can be advantageous to use a SEMS with a large diameter rather than using a plastic stent with a small diameter, not only in terms of long stent patency but also for adequate recanalization of the bile duct stricture. In particular, among SEMSs, an FCSEMS has been used for malignant biliary obstruction and for benign biliary disorders, such as benign biliary stricture or bile leakage, owing to its advantage of being removable via endoscopy.11-13,18,24 In the case of malignant biliary obstruction, it is very unusual to remove a stent after it has been inserted, while in the case of benign biliary disorders, a stent has to be removed at the appropriate time. Therefore, the use of an FCSEMS for benign indications in the bile duct raises questions regarding the optimal duration of stenting. However, there have been few studies on the optimal duration of stenting using an FCSEMS. Kuo et al.25 reported that after liver transplantation, an FCSEMS was inserted for bile duct stricture for a median of 32 days. In the study by Kahaleh et al.,13 an FCSEMS was inserted in 44 patients with benign biliary strictures and left in situ for a median of 3.3 months. Furthermore, Cahen et al.26 reported that an FCSEMS was placed for bile duct stricture due to chronic pancreatitis for 3 to 6 months. When an FCSEMS is used for benign biliary obstruction, it is important to determine the optimal time for the stent to remain in situ to minimize bile duct injury due to the stent while obtaining adequate remodeling and recanalization of the bile duct. Based on the results of this study, optimal results for benign biliary disease can be achieved by inserting an FCSEMS for up to 9 months.
In this study, one animal showed severe epithelial hyperplasia, thereby making removal of the stent impossible because the stent was embedded in the bile duct. Such severe epithelial hyperplasia was shown to occur only in dog 4, which had held a stent for 3 months. On the other hand, severe epithelial hyperplasia was not observed in the animals that held a stent for 6 to 9 months. Therefore, severe epithelial hyperplasia in response to the placement of an FCSEMS might have been due to other intrinsic factors such as damage to the silicone membrane during stent deployment or stent expansion through folding, rather than solely to the duration of the stent placement. The covered membrane of an FCSEMS might be damaged by surrounding tissues when the stent expands in a severe stricture. These factors should be further explored in future research.
In this study, although only one animal showed severe inflammatory change in the stented bile duct and the other animals showed mild to moderate inflammatory changes, five animals showed de novo stricture at the end portion of the stented bile duct. Two animals among the ones that held a stent for six months showed de novo stricture in both the proximal and distal portions of the bile duct, as did two animals among the ones that held a stent for 9 months. One animal that held a stent for 3 months showed de novo stricture in the proximal portion of the bile duct. In those cases where de novo stricture was found in the distal portion of the stented bile duct, it was assumed that this was because of excessive outward radial pressure at both ends of the stent used in this study, which was expanded with a flare shape at both ends.9,24 Moreover, since the average diameter of the common bile duct in mongrel dogs is about 4 mm, the 8-mm-wide metal stents that were used in this study were relatively large.19 It was found that such de novo stricture was generated in proportion to the duration of the stent placement. In particular, de novo stricture most frequently occurred when an FCSEMS was inserted for more than 6 months. Unlike malignant biliary obstruction, a patient with benign biliary disease has a long life expectancy, so quality of life for those who have benign biliary disease can be seriously impaired if bile duct injury due to a stent occurs.24 Therefore, when an FCSEMS is selected for benign biliary disease, an FCSEMS of an appropriate diameter should be selected by considering the diameters of the proximal and distal portions of the bile duct. Also, when de novo stricture is expected to occur frequently, it would be prudent to keep the duration of the stent placement to a minimum. Finally, it is necessary to develop an FCSEMS that reduces the radial force at both ends of the stent.
There were limitations to our study. First, our test used a normal bile duct model rather than a stricture bile duct model. This is because the average diameter of the common bile duct in mongrel dogs is much smaller than that of the metal stents that were used in this study. Therefore, we assume that our test results would be similar to those using a stricture model. Although we used a normal bile duct model, we assumed this to be sufficient to detect histological changes in the bile duct following long-term placement of an FCSEMS. Second, since the bile duct was examined immediately after necropsy and removal of the stent, there was no follow-up result for the bile duct after stent removal. For follow-up results, it is necessary to perform further animal tests using the stricture model. Third, the FCSEMS was surgically removed during necropsy in our study. However, the study would have been more ideal if the stent had been removed through an endoscope after tying a silk thread to the stent to see how easily it could be removed before observing the bile duct. Finally, there were too few experimental animals available to allow us to generalize these results. The results of this experiment may not be sufficient to determine the optimal duration of placement of a FCSEMS on account of the different clinical condition that exists between animals and humans; that is, patients with tight biliary strictures usually have the FCSEMS placed at the distal tip of their duodenum.
Theoretically, an FCSEMS has many advantages not only for palliative treatment of malignant biliary obstruction but also for benign biliary disorders such as benign biliary stricture or bile leakage, which explains its clinical use. However, it is necessary to provide guidelines regarding the length of time a stent should be placed and then removed. In this study, we demonstrated that a bile duct in which an FCSEMS was placed for 9 months had no severe inflammatory changes, showing that an FCSEMS can be held safely in the bile duct for 9 months. It also provided a firm basis for clinical trials of an FCSEMS in benign biliary disease in humans. However, it should be noted that de novo strictures can occur in proportion to the duration of stent placement and that a newly designed FCSEMS should be developed to reduce de novo strictures. Furthermore, additional studies on factors that influence severe epithelial hyperplasia are necessary because severe epithelial hyperplasia was generated regardless of the duration of stent placement, which can make removal of a stent impossible. Needless to say, further randomized controlled trials are needed to determine the optimal duration of an FCSEMS stent placement in benign biliary disease in humans.
Acknowledgments
This study was supported by a 2010 Weolbong grant from the Korean Gastrointestinal Endoscopy Research Foundation (2010 Investigation Grant).
Footnotes
The authors have no financial conflicts of interest.
References
- 1.Smith AC, Dowsett JF, Russell RC, Hatfield AR, Cotton PB. Randomised trial of endoscopic stenting versus surgical bypass in malignant low bileduct obstruction. Lancet. 1994;344:1655–1660. doi: 10.1016/s0140-6736(94)90455-3. [DOI] [PubMed] [Google Scholar]
- 2.Andersen JR, Sørensen SM, Kruse A, Rokkjaer M, Matzen P. Randomised trial of endoscopic endoprosthesis versus operative bypass in malignant obstructive jaundice. Gut. 1989;30:1132–1135. doi: 10.1136/gut.30.8.1132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kaassis M, Boyer J, Dumas R, et al. Plastic or metal stents for malignant stricture of the common bile duct? Results of a randomized prospective study. Gastrointest Endosc. 2003;57:178–182. doi: 10.1067/mge.2003.66. [DOI] [PubMed] [Google Scholar]
- 4.Perdue DG, Freeman ML, DiSario JA, et al. Plastic versus self-expanding metallic stents for malignant hilar biliary obstruction: a prospective multicenter observational cohort study. J Clin Gastroenterol. 2008;42:1040–1046. doi: 10.1097/MCG.0b013e31815853e0. [DOI] [PubMed] [Google Scholar]
- 5.Soderlund C, Linder S. Covered metal versus plastic stents for malignant common bile duct stenosis: a prospective, randomized, controlled trial. Gastrointest Endosc. 2006;63:986–995. doi: 10.1016/j.gie.2005.11.052. [DOI] [PubMed] [Google Scholar]
- 6.Hausegger KA, Kleinert R, Lammer J, Klein GE, Fluckiger F. Malignant biliary obstruction: histologic findings after treatment with self-expandable stents. Radiology. 1992;185:461–464. doi: 10.1148/radiology.185.2.1410354. [DOI] [PubMed] [Google Scholar]
- 7.Lee MJ, Dawson SL, Mueller PR, Krebs TL, Saini S, Hahn PF. Palliation of malignant bile duct obstruction with metallic biliary endoprostheses: technique, results, and complications. J Vasc Interv Radiol. 1992;3:665–671. doi: 10.1016/s1051-0443(92)72920-0. [DOI] [PubMed] [Google Scholar]
- 8.van Berkel AM, Cahen DL, van Westerloo DJ, Rauws EA, Huibregtse K, Bruno MJ. Self-expanding metal stents in benign biliary strictures due to chronic pancreatitis. Endoscopy. 2004;36:381–384. doi: 10.1055/s-2004-814319. [DOI] [PubMed] [Google Scholar]
- 9.Moon SH, Kim MH, Park do H, et al. Modified fully covered self-expandable metal stents with antimigration features for benign pancreatic-duct strictures in advanced chronic pancreatitis, with a focus on the safety profile and reducing migration. Gastrointest Endosc. 2010;72:86–91. doi: 10.1016/j.gie.2010.01.063. [DOI] [PubMed] [Google Scholar]
- 10.Park do H, Kim MH, Moon SH, Lee SS, Seo DW, Lee SK. Feasibility and safety of placement of a newly designed, fully covered self-expandable metal stent for refractory benign pancreatic ductal strictures: a pilot study (with video) Gastrointest Endosc. 2008;68:1182–1189. doi: 10.1016/j.gie.2008.07.027. [DOI] [PubMed] [Google Scholar]
- 11.Behm B, Brock A, Clarke BW, et al. Partially covered self-expandable metallic stents for benign biliary strictures due to chronic pancreatitis. Endoscopy. 2009;41:547–551. doi: 10.1055/s-0029-1214708. [DOI] [PubMed] [Google Scholar]
- 12.Judah JR, Draganov PV. Endoscopic therapy of benign biliary strictures. World J Gastroenterol. 2007;13:3531–3539. doi: 10.3748/wjg.v13.i26.3531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kahaleh M, Behm B, Clarke BW, et al. Temporary placement of covered self-expandable metal stents in benign biliary strictures: a new paradigm? (with video) Gastrointest Endosc. 2008;67:446–454. doi: 10.1016/j.gie.2007.06.057. [DOI] [PubMed] [Google Scholar]
- 14.Mahajan A, Ho H, Sauer B, et al. Temporary placement of fully covered self-expandable metal stents in benign biliary strictures: midterm evaluation (with video) Gastrointest Endosc. 2009;70:303–309. doi: 10.1016/j.gie.2008.11.029. [DOI] [PubMed] [Google Scholar]
- 15.Khan I, Smith N, Jones E, Finch DS, Cameron RE. Analysis and evaluation of a biomedical polycarbonate urethane tested in an in vitro study and an ovine arthroplasty model. Part II: in vivo investigation. Biomaterials. 2005;26:633–643. doi: 10.1016/j.biomaterials.2004.02.064. [DOI] [PubMed] [Google Scholar]
- 16.Kim JH, Song HY, Shin JH, et al. Membrane degradation of covered stents in the upper gastrointestinal tract: frequency and clinical significance. J Vasc Interv Radiol. 2008;19(2 Pt 1):220–224. doi: 10.1016/j.jvir.2007.09.023. [DOI] [PubMed] [Google Scholar]
- 17.Song TJ, Lee SS, Yun SC, et al. Paclitaxel-eluting covered metal stents versus covered metal stents for distal malignant biliary obstruction: a prospective comparative pilot study. Gastrointest Endosc. 2011;73:727–733. doi: 10.1016/j.gie.2010.11.048. [DOI] [PubMed] [Google Scholar]
- 18.Bakhru MR, Foley PL, Gatesman J, Schmitt T, Moskaluk CA, Kahaleh M. Fully covered self-expanding metal stents placed temporarily in the bile duct: safety profile and histologic classification in a porcine model. BMC Gastroenterol. 2011;11:76. doi: 10.1186/1471-230X-11-76. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lee SS, Shin JH, Han JM, et al. Histologic influence of paclitaxel-eluting covered metallic stents in a canine biliary model. Gastrointest Endosc. 2009;69:1140–1147. doi: 10.1016/j.gie.2008.08.005. [DOI] [PubMed] [Google Scholar]
- 20.Silvis SE, Sievert CE, Jr, Vennes JA, Abeyta BK, Brennecke LH. Comparison of covered versus uncovered wire mesh stents in the canine biliary tract. Gastrointest Endosc. 1994;40:17–21. doi: 10.1016/s0016-5107(94)70004-4. [DOI] [PubMed] [Google Scholar]
- 21.Yasumori K, Mahmoudi N, Wright KC, Wallace S, Gianturco C. Placement of covered self-expanding metallic stents in the common bile duct: a feasibility study. J Vasc Interv Radiol. 1993;4:773–778. doi: 10.1016/s1051-0443(93)71971-5. [DOI] [PubMed] [Google Scholar]
- 22.Costamagna G, Pandolfi M, Mutignani M, Spada C, Perri V. Long-term results of endoscopic management of postoperative bile duct strictures with increasing numbers of stents. Gastrointest Endosc. 2001;54:162–168. doi: 10.1067/mge.2001.116876. [DOI] [PubMed] [Google Scholar]
- 23.Binmoeller KF. Fully covered metal stents in the pancreatic duct: balancing trade-offs. Gastrointest Endosc. 2010;72:92–94. doi: 10.1016/j.gie.2010.03.1064. [DOI] [PubMed] [Google Scholar]
- 24.Moon JH, Choi HJ, Koo HC, et al. Feasibility of placing a modified fully covered self-expandable metal stent above the papilla to minimize stent-induced bile duct injury in patients with refractory benign biliary strictures (with videos) Gastrointest Endosc. 2012;75:1080–1085. doi: 10.1016/j.gie.2012.01.016. [DOI] [PubMed] [Google Scholar]
- 25.Kuo MD, Lopresti DC, Gover DD, Hall LD, Ferrara SL. Intentional retrieval of viabil stent-grafts from the biliary system. J Vasc Interv Radiol. 2006;17(2 Pt 1):389–397. doi: 10.1097/01.RVI.0000194867.86371.0B. [DOI] [PubMed] [Google Scholar]
- 26.Cahen DL, Rauws EA, Gouma DJ, Fockens P, Bruno MJ. Removable fully covered self-expandable metal stents in the treatment of common bile duct strictures due to chronic pancreatitis: a case series. Endoscopy. 2008;40:697–700. doi: 10.1055/s-2008-1077353. [DOI] [PubMed] [Google Scholar]