

Abstract
Background:
Local reference data are needed in the screening of children for thyroid enlargement. We determined the thyroid gland volume using the ultrasonography (US) in schoolchildren of Isfahan, Iran.
Materials and Methods:
A total of 360 schoolchildren (59% girls) aged 8-15 years who met the study criteria were entered the study. Clinical grading of goiter was performed by an endocrinologist according to the World Health Organization (WHO) classification. Then, a single expert radiologist performed thyroid volume measurement using a portable ultrasound device. Urinary iodine (UI) concentration was checked in 36 randomly selected cases.
Results:
On physical examination, 327 (91%), 32 (8.8%) and 1 (0.2%) subjects were classified as normal, borderline and goiter Grade 2. Mean thyroid volume measured by US was 1.46 ± 0.70 ml. Thyroid volume in boys was significantly higher than girls (1.58 ± 0.67 ml vs. 1.38 ± 0.71 ml; P = 0.009). Thyroid volume was positively correlated with the clinical grade of the goiter (r = 0.30, P < 0.001) and with age (r = 0.25, P < 0.001). Both median and 95th percentile of thyroid volume of our subjects was lower than the reference values reported by WHO. Median of UI was 16.90 μg/dl. UI was not correlated with thyroid volume (r = 0.12, P = 0.46).
Conclusion:
The thyroid size in Isfahanian schoolchildren is lower than the reference values reported by WHO. These data could be used in determining local reference in the screening of children for thyroid enlargement.
Keywords: Goiter, Isfahan, thyroid, thyroid volume, ultrasound
INTRODUCTION
Thyroid diseases are among the most common endocrine disorders in children and adolescents. Iodine deficiency disorders (IDDs) are a global public health problem and is the leading preventable cause of mental impairment world-wide.[1,2]
According to the goiter prevalence, it is estimated that 750 million people world-wide are at risk of IDDs.[3] The median urinary iodine (UI) concentration is one of the most widely used indicators for assessing IDDs. Another important indicator of IDDs in a population is the enlargement of the thyroid gland, which is the most apparent manifestation of iodine deficiency.[4] Therefore, assessment of the size of thyroid gland is a useful method in the diagnosis and management of thyroid disorders.[2,5]
Inspection and palpation are two traditional methods that have been widely used to determine the thyroid volume. However, the clinical assessment of thyroid size has been shown to be imprecise and has relatively high inter-observer variation, especially when the goiter is small, i.e., Grade 1 or bordering on either Grade 0 or Grade 2.[6]
Thyroid ultrasonography (US) is a validated and recommended procedure for the quantitative assessment of the thyroid gland size.[7,8,9] US is a safe and noninvasive technique that provides a more accurate and objective method of thyroid volume measurement than inspection and palpation.[6] However, in order to use US method for determination of thyroid volume reliable reference data are necessary.[1]
Although normative values of thyroid volume measured by US has been described by international organizations, the pertinence of these international references for the assessment of IDD in other populations is unclear and needs further local investigations.[10,11,12] Moreover, previous studies have recommended the use of local reference in the screening of children for thyroid enlargement until the adoption of a new international reference for thyroid volume that is applicable for different countries.[11,12]
In light of the above, this study was aimed to determine the thyroid volume using US in schoolchildren of Isfahan, Iran. In addition, we compared the US values with the findings of clinical examination and evaluated the correlation between the thyroid volume and UI.
MATERIALS AND METHODS
After approval of the study by the Ethic Committee of Isfahan University of Medical Sciences and obtaining informed consent from parents, this cross-sectional study was performed on schoolchildren of Isfahan, Iran, between December 2011 and May 2012. The primary sampling unit consisted of elementary and secondary schools. Subjects were enrolled using a multistage cluster sampling procedure and then appropriate numbers of children were sampled randomly within selected clusters. Finally, a total of 360 schoolchildren of both genders aged 8-15 were entered the study. Subjects were excluded if they had a history of thyroid surgery or significant underlying disease such as cardiopulmonary, liver or renal problems. Available medical records of students and interviews with parents, teachers and participants were used to detect exclusion criteria.
First, all demographic data (sex, age, weight and height) were recorded in a questionnaire. Then, an Endocrinologist examined all children and performed goiter grading according to World Health Organization (WHO) classification. Children were classified into three groups (Grades 0, 1 and 2) with respect to goiter grading: Grade 0 — the thyroid impalpable and invisible; Grade 1 — neck thickening is present in the result of enlarged thyroid, palpable, however, not visible in normal position of the neck (the thickened mass moves upwards during swallowing); Grade 2 — neck swelling, visible when the neck is in normal position, corresponding to enlarged thyroid — found in palpation.[13] Afterward, a single expert radiologist performed thyroid volume measurement using a portable ultrasound device, SSD-500 with a 5-MHz linear transducer (Aloka Co. Ltd., Tokyo, Japan). The volume of each lobe was calculated, using the formula: V (ml) = width × length × thickness (cm) × 0·479.[14] Then, mean of the volume of right and left lobes were calculated and recorded. Ten percent of the participants (36 children) were randomly selected and were referred to a single laboratory to check UI level.
Data were analyzed by the statistical package for the social sciences (SPSS) 20.0 (SPSS Inc., Chicago, IL, USA). Independent t-test, one-way ANOVA, Spearman correlation, Pearson correlation and Chi-square were used when appropriate. P values less than 0.05 were considered as statistically significant.
RESULTS
Baseline characteristics
This study consisted of 147 (41%) boys and 213 (59%) girls. The baseline characteristics of the 360 investigated schoolchildren aged 8-15 years are listed in Table 1.
Table 1.
Comparison of baseline characteristics between boys and girls

Relative frequency of different clinical grades of goiter
According to the clinical grading of goiter, 327 subjects (91%) were classified as normal (Grade 0), 32 subjects (8.8%) had borderline goiter size (between Grade 0 and Grade 1) and 1 participant (0.2%) had goiter Grade 2. None of the patients had goiter 1. There was no significant difference between boys and girls in relative frequency of different clinical grades of goiter [Table 2].
Table 2.
Comparison of relative frequency of different clinical grades of goiter between boys and girls

Mean volume of the thyroid gland
The mean volume of the thyroid gland measured by US was 1.46 ± 0.70 ml. The difference in the thyroid gland volume between boys and girls was statistically significant (1.58 ± 0.67 ml vs. 1.38 ± 0.71 ml respectively; P = 0.009).
Furthermore, patients with different clinical grades of goiter were significantly different regarding the mean volume of the thyroid gland [Table 3].
Table 3.
Comparison of mean of thyroid gland volume in patient with different clinical grades of goiter
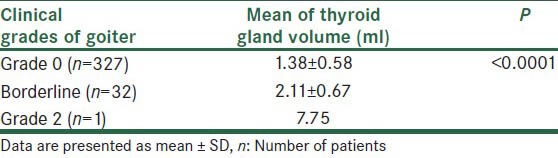
Using Spearman's correlation, mean of the thyroid gland volume was positively correlated with the clinical grade of the goiter (r = 0.30, P < 0.001).
Mean of the thyroid gland volume was positively correlated with the age of participants (r = 0.25, P < 0.001). Age and sex specific median and 95th percentile are presented in Table 4. Figures 1–4 represent comparison of thyroid volume of Isfahanian boys and girls in different ages with those reported by WHO.
Table 4.
Median and 95th percentile thyroid volume by sex and age

Figure 1.

Comparison of median of thyroid volume of Isfahanian boys in different ages with those reported by World Health Organization
Figure 4.

Comparison of 95th percentile of thyroid volume of Isfahanian girls in different ages with 97th percentile of boys reported by World Health Organization
Figure 2.

Comparison of 95th percentile of thyroid volume of Isfahanian boys in different ages with 97th percentile of boys reported by World Health Organization
Figure 3.
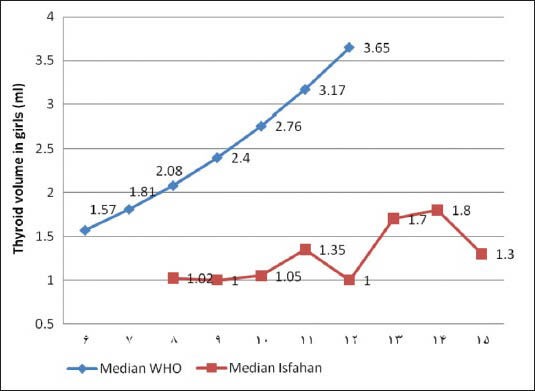
Comparison of median of thyroid volume of Isfahanian girls in different ages with those reported by World Health Organization
UI
Median of UI was 16.90 μg/dl and there was no significant correlation between UI and mean of the thyroid gland volume (r = 0.12, P = 0.460).
DISCUSSION
After the implementation of the national salt-iodization program, iodine deficiency was resolved in Isfahan[15] and the prevalence of goiter decreased significantly. However, the prevalence of goiter is still high in Isfahan schoolchildren.[16] Although thyroid palpation has been considered as the standard method for determining thyroid size, it has been found to be inadequate for evaluation of mild thyroid enlargement in schoolchildren.[17] Thyroid US is recommended whenever possible as a validated procedure for the quantitative assessment of the thyroid gland size.[17,18,19,20]
In the present study, we represented the thyroid volume measured by US in 8-15-year-old schoolchildren from Isfahan. We have only investigated schoolchildren living in the urban area of Isfahan. To the best of our knowledge, this is the first study that has measured the thyroid gland volume US in Isfahan schoolchildren. We measured the median and 95th percentile of thyroid volume for different sex and ages. However, due to the relatively sample size, we were not able to determine these values for all age/sex groups.
In general, the median and 95th percentile of thyroid volume from Isfahanian children were lower than the corresponding references reported by WHO as normative values.[21] This finding is consistent with a previous study in Tehran, Iran, conducted by Azizi et al. They reported that the thyroid volume from Tehranian children were lower than the reference values reported by the WHO.[12] Similarly, a study on schoolchildren in Philippines by Kim et al. demonstrated that the median thyroid volumes of schoolchildren of Philippines were generally low compared with international reference data by age group.[1]
The mean volume of the thyroid gland was significantly correlated with age and body mass index (BMI). Kim et al. have also reported similar correlations in schoolchildren from Philippines. They have demonstrated a significant association between the thyroid size and age, weight and height.[1] Azizi et al. also reported a significant correlation between the thyroid volume and height and weight in Tehranian schoolchildren.[12] Our findings revealed significantly higher thyroid size in boys. Given the significantly higher BMI in boys and the significant correlation between BMI and thyroid size, this significant difference between thyroid size in boys and girls could be attributed to the difference of BMI between two genders. A study performed by Azizi et al. on schoolchildren of Emirates also revealed a significant difference between boys and girls regarding the thyroid size.[22]
Median of UI in our population was 16.90 μg/dl. Although this value is less than the median of UI reported for schoolchildren of Tehran (median UI of 21.2 μg/dl), it is still within the normal range. According to the WHO report, the normal range of median UI concentrations in schoolchildren of iodine sufficient areas is 11.8-28.8 μg/dl.[21] The median of UI in the present study is higher than that of schoolchildren of the Emirates reported by Azizi et al.[22]
We also found no significant correlation between UI and thyroid size. Busnardo et al. who also conducted a study to determine the normal values for thyroid US, goiter prevalence and UI concentration in schoolchildren in Italy did not find a significant correlation between thyroid volume by US and UI.[23] However, Delange et al. reported an inverse relationship between UI and thyroid volume in schoolchildren in Europe.[18]
This study has some limitations. First, we have investigated relatively small sample size. In addition, we only included children living in the urban area of Isfahan. Furthermore, UI was evaluated in only 10% of participants. Hence, further studies with larger sample size are required in this regard.
CONCLUSION
In summary, the thyroid size in Isfahanian schoolchildren is lower than the reference values reported by WHO. These data could be used in determining local reference in the screening of children for thyroid enlargement. Further studies on a larger sample sizes on both rural and urban areas are recommended to achieve more accurate results.
ACKNOWLEDGEMENTS
This study was supported by the Isfahan University of Medical Sciences. We are thankful to Dr. Ali Gholamrezaei who edited this report.
Footnotes
Source of Support: This study was supported by the Isfahan University of Medical Sciences.
Conflict of Interest: None declared.
REFERENCES
- 1.Kim BK, Choi YS, Oak CH, Park YH, Kim JH, Park DJ, et al. Determination of thyroid volume by ultrasonography among schoolchildren in Philippines. Int J Endocrinol 2012. 2012 doi: 10.1155/2012/387971. 387971. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Xu F, Sullivan K, Houston R, Zhao J, May W, Maberly G. Thyroid volumes in US and Bangladeshi schoolchildren: Comparison with European schoolchildren. Eur J Endocrinol. 1999;140:498–504. doi: 10.1530/eje.0.1400498. [DOI] [PubMed] [Google Scholar]
- 3.Siavash Dastjerdi M, Hashemipour M, Rezvanian H, Kazemi F, Najafian A, Mohammady M, et al. Iron deficiency in goitrous schoolchildren of Semirom, Iran. Horm Res. 2006;66:45–50. doi: 10.1159/000093473. [DOI] [PubMed] [Google Scholar]
- 4.Hess SY, Zimmermann MB. Thyroid volumes in a national sample of iodine-sufficient Swiss school children: Comparison with the World Health Organization/International Council for the control of iodine deficiency disorders normative thyroid volume criteria. Eur J Endocrinol. 2000;142:599–603. doi: 10.1530/eje.0.1420599. [DOI] [PubMed] [Google Scholar]
- 5.Ying M, Sin MH, Pang SF. Sonographic measurement of thyroid gland volume: A comparison of 2D and 3D ultrasound. Radiography. 2005;11:242–8. [Google Scholar]
- 6.Recommended normative values for thyroid volume in children aged 6-15 years. World Health Organization & International Council for Control of Iodine Deficiency Disorders. Bull World Health Organ. 1997;75:95–7. [PMC free article] [PubMed] [Google Scholar]
- 7.Berghout A, Wiersinga WM, Smits NJ, Touber JL. Determinants of thyroid volume as measured by ultrasonography in healthy adults in a non-iodine deficient area. Clin Endocrinol (Oxf) 1987;26:273–80. doi: 10.1111/j.1365-2265.1987.tb00784.x. [DOI] [PubMed] [Google Scholar]
- 8.Hegedüs L, Perrild H, Poulsen LR, Andersen JR, Holm B, Schnohr P, et al. The determination of thyroid volume by ultrasound and its relationship to body weight, age, and sex in normal subjects. J Clin Endocrinol Metab. 1983;56:260–3. doi: 10.1210/jcem-56-2-260. [DOI] [PubMed] [Google Scholar]
- 9.Rasmussen SN, Hjorth L. Determination of thyroid volume by ultrasonic scanning. J Clin Ultrasound. 1974;2:143–7. doi: 10.1002/jcu.1870020211. [DOI] [PubMed] [Google Scholar]
- 10.Wiersinga WM, Podoba J, Srbecky M, van Vessem M, van Beeren HC, Platvoet-Ter Schiphorst MC. A survey of iodine intake and thyroid volume in Dutch schoolchildren: Reference values in an iodine-sufficient area and the effect of puberty. Eur J Endocrinol. 2001;144:595–603. doi: 10.1530/eje.0.1440595. [DOI] [PubMed] [Google Scholar]
- 11.Foo LC, Zulfiqar A, Nafikudin M, Fadzil MT, Asmah AS. Local versus WHO/International council for control of iodine deficiency disorders-recommended thyroid volume reference in the assessment of iodine deficiency disorders. Eur J Endocrinol. 1999;140:491–7. doi: 10.1530/eje.0.1400491. [DOI] [PubMed] [Google Scholar]
- 12.Azizi F, Delshad H, Mehrabi Y. Thyroid volumes in schoolchildren of Tehran: Comparison with European schoolchildren. J Endocrinol Invest. 2001;24:756–62. doi: 10.1007/BF03343924. [DOI] [PubMed] [Google Scholar]
- 13.Geneva: WHO; 2001. World Health Organization. United Nations Children's Fund and International Council for the Control of Iodine Deficiency Disorders. Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination, WHO/NHD/01.1. [Google Scholar]
- 14.Brunn J, Block U, Ruf G, Bos I, Kunze WP, Scriba PC. Volumetric analysis of thyroid lobes by real-time ultrasound (author's transl) Dtsch Med Wochenschr. 1981;106:1338–40. doi: 10.1055/s-2008-1070506. [DOI] [PubMed] [Google Scholar]
- 15.Aminorroaya A, Amini M, Hovsepian S. Prevalence of goitre in Isfahan, Iran, fifteen years after initiation of universal salt iodization. J Health Popul Nutr. 2010;28:351–8. doi: 10.3329/jhpn.v28i4.6041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Keshteli AH, Hashemipour M, Siavash M, Kelishadi R, Amini M. High prevalence of goiter in schoolchildren in Isfahan; zinc deficiency does not play a role. Endokrynol Pol. 2010;61:287–90. [PubMed] [Google Scholar]
- 17.Marwaha RK, Tandon N, Ashraf GM, Ganguly SK, Batra A, Aggarwal R, et al. Ultrasound evaluation of thyroid size: A large nationwide study of schoolchildren in India. Natl Med J India. 2008;21:69–74. [PubMed] [Google Scholar]
- 18.Delange F, Benker G, Caron P, Eber O, Ott W, Peter F, et al. Thyroid volume and urinary iodine in European schoolchildren: Standardization of values for assessment of iodine deficiency. Eur J Endocrinol. 1997;136:180–7. doi: 10.1530/eje.0.1360180. [DOI] [PubMed] [Google Scholar]
- 19.Knudsen N, Bols B, Bülow I, Jørgensen T, Perrild H, Ovesen L, et al. Validation of ultrasonography of the thyroid gland for epidemiological purposes. Thyroid. 1999;9:1069–74. doi: 10.1089/thy.1999.9.1069. [DOI] [PubMed] [Google Scholar]
- 20.Vitti P, Martino E, Aghini-Lombardi F, Rago T, Antonangeli L, Maccherini D, et al. Thyroid volume measurement by ultrasound in children as a tool for the assessment of mild iodine deficiency. J Clin Endocrinol Metab. 1994;79:600–3. doi: 10.1210/jcem.79.2.8045982. [DOI] [PubMed] [Google Scholar]
- 21.Zimmermann MB, Hess SY, Molinari L, De Benoist B, Delange F, Braverman LE, et al. New reference values for thyroid volume by ultrasound in iodine-sufficient schoolchildren: A World Health Organization/Nutrition for Health and Development Iodine Deficiency Study Group Report. Am J Clin Nutr. 2004;79:231–7. doi: 10.1093/ajcn/79.2.231. [DOI] [PubMed] [Google Scholar]
- 22.Azizi F, Mehran L, Sheikholeslam R, Ordookhani A, Naghavi M, Hedayati M, et al. Sustainability of a well-monitored salt iodization program in Iran: Marked reduction in goiter prevalence and eventual normalization of urinary iodine concentrations without alteration in iodine content of salt. J Endocrinol Invest. 2008;31:422–31. doi: 10.1007/BF03346386. [DOI] [PubMed] [Google Scholar]
- 23.Busnardo B, Nacamulli D, Frigato F, Vianello-Dri A, De Vido D, Mian C, et al. Normal values for thyroid ultrasonography, goiter prevalence and urinary iodine concentration in schoolchildren of the Veneto Region, Italy. J Endocrinol Invest. 2003;26:991–6. doi: 10.1007/BF03348197. [DOI] [PubMed] [Google Scholar]