

Abstract
Background. Amnestic Mild Cognitive Impairment (aMCI) often progresses to Alzheimer's disease. There are clinical markers and biomarkers to identify the degenerative process in the brain. Objectives. To obtain the diagnostic values of olfactory test, pupillary response to tropicamide 0.01%, BDNF plasma level, and APOE ε4 in diagnosing aMCI. Methods. Cross-sectional, comparative analysis. Results. There were 109 subjects enrolled (aMCI: 51, normal cognition: 58) with age 64 ± 5.54 years. For diagnosing aMCI, cut-off point for the olfactory score was <7 out of 10 and >22% for pupil dilatation response. Low BDNF plasma level was related significantly with olfactory deficits and aMCI (P < 0.05). Four of five subjects with homozygote e4 presented with multiple-domain aMCI. This group displayed the lowest means of olfactory score and the highest means of pupillary hypersensitivity response (P < 0.0001). Combination of olfactory deficit and pupillary hypersensitivity response in detection of aMCI was beneficial with Sp 91% and PPV 87%. In conjunction with clinical markers, BDNF plasma level and presence of APOE e4+ improved Sp and PPV. Conclusions. Combination of olfactory test and pupillary response test was useful as diagnostic tool in aMCI. In conjunction with clinical markers, low level of BDNF plasma and presence of APOE e4 improved the diagnostic value.
1. Introduction
Mild Cognitive Impairment (MCI) is a transitional state between normal cognitive function and dementia. It is predicted that 50–80% of patients with MCI will eventually develop dementia in the later stage of the disease [1]. The memory-predominant subtype, amnestic MCI (aMCI) conveys the highest risk of progressing to Alzheimer's dementia (AD) [2]. Neuropathologic study also has shown that aMCI seemed to be intermediate between the neurofibrillary changes of aging and the pathologic features of very early AD [3]. Dementia and MCI are clinical diagnosis based on psychometric evaluation. In spite of this evaluation being the gold standard, there are still limitations to its usage (e.g, illiterate patients, visual and hearing problems, and pseudoamnesia). There are clinical and biologic markers available to identify the degenerative process in the brain that have been studied, such as olfactory test [4–16], pupil dilatation response to tropicamide [17–26], APOE genotype [27–34], and brain derived neurotrophic factor (BDNF) plasma level [35–42].
Previous report has featured relationship between several markers with degenerative process and dementia such as olfactory deficits that is now being used as practice parameter in diagnosis of Parkinson disease [43]. Other studies published the presence of olfactory deficit in AD patients [13–16]. Studies performed in aMCI patients also revealed that patients with low olfactory scores were more likely to progress toward dementia [11].
Pupillary hypersensitivity response to tropicamide in dementia patients has been recorded in many studies. Scinto et al. reported a cut-off point of 13% in 30 minutes to differentiate dementia and normal cognition in the elderly using 0.01% tropicamide [17]. Another study published by Iijima et al. using 0.005% tropicamide showed hypersensitivity in pupil dilatation response in AD patients when compared with non-AD subjects [20].
Based on the former reports, olfactory test and pupil dilatation response to tropicamide could be the new potential markers in detecting aMCI. To our knowledge, there has not been a study combining the two factors for diagnostic purpose in aMCI patients. We are also aware of APOE and BDNF as markers of the degenerative process in the brain. Therefore, we want to investigate whether combination of olfactory test and pupillary response to tropicamide 0.01% has diagnosis value and whether presence of APOE ε4 and low BDNF plasma level can be useful to enhance diagnostic accuracy of aMCI.
2. Methods
This is a cross-sectional study, comparative analysis in elderly with normal cognition and those presenting with aMCI. The study consisted of all subjects participating in the baseline cognitive assessment of study on quality of life in elderly in Kali Anyar, West Jakarta, done by Center of Health Research Atma Jaya Catholic University of Indonesia, about 12 months prior to this study (between August 2011 and September 2011). Inclusion criteria are age ≥60 years old and being literate (reading and writing skills). Exclusion criteria are hearing problems, major psychiatric disorders, depression (Geriatric Depression Scale/GDS >4) [44, 45], history of cataract surgery, severe medical illness, past consumption of drugs affecting brain's function and structure, history of cerebrovascular disease, epilepsy, and diabetes mellitus (consumption of antiglycaemic drugs or fasting blood glucose ≥126 mg/dL) [46, 47].
Cognitive assessments were conducted and the results were compared with baseline data. Assessments were done using Forward Digit Span, Clock Drawing Test and MMSE, Verbal Fluency (VF), Boston Naming Test (BNT), Word List Memory Immediate Recall (WLM IR), World List Memory Delayed Recall (WLM DR), Recognition, and Constructional Praxis (CP) from CERAD (Consortium to Establish a Registry for Alzheimer's Disease) Neuropsychological Battery [48].
Diagnosis of MCI was based according to Consortium Criteria proposed by the International Working Group on MCI [49]. The criteria include (1) absence of dementia according to DSM IV or ICD-10, (2) evidence of cognitive decline overtime on objective cognitive task, and (3) preserved baseline activities of daily living or only minimal impairment in complex instrumental functions. Definition of cognitive decline is decrease ≥2 points/year in one cognitive instrument (MMSE/WLM IR/WLM DR) or decrease ≥1 point/year in at least 2 cognitive instruments (MMSE/WLM IR/WLM DR). Single-domain aMCI was diagnosed if subjects are showing deficit in memory task (Saving Score <65% or WLM IR (third repetition) <8), but not in any other area of cognitive domains. Multiple-domain aMCI was diagnosed if there was presence of memory deficit and also in other cognitive domains. Nonamnestic MCI (naMCI) was diagnosed if there was impairment in cognitive domains other than memory (we excluded naMCI in this study). The regional ethical committee approved the study and written informed consent was obtained from each individual.
2.1. Apolipoprotein E and BDNF Plasma Level
Blood samples (10 mL) were collected from each subject. Routine blood test was performed along with fasting blood glucose, lipid profile, APOE, and BDNF plasma level. APOE and BDNF were done blinded for all clinical data. APOE measurement was completed using Restriction Fragment Length Polymorphism (RFLP) method. In this study, we used High Pure Polymerase Chain Reaction (PCR) Template Preparation Kit for extraction and PCR was performed using FastStart Taq DNA Polymerase (Roche Applied Biosystem). BDNF was measured using ELISA kit from R&D Systems.
2.2. Olfactory Test
Examination of olfactory nerve function was performed using 10 odors commonly found in Indonesia: cajuput oil, coffee, jasmine, menthol, tobacco, kerosene, pandan, camphor, chocolate, and orange [50]. The odors were preserved in similar containers, sealed, and coded continuously. Subjects were allowed to smell the odors twice for 5 seconds before being asked to identify them. They were given a 30 sec break prior to identifying the next odor.
2.3. Pupillary Response to 0.01% Tropicamide
The examiner instilled a drop of 0.01% tropicamide on one subject's eye, while the other eye received saline as control. We measured pupil diameter at 30 minutes, 40 minutes, and 50 minutes [17] using Colvard pupillometry in a semidarkened room [51, 52]. Pupillary response was examined using Granholm et al. method by measuring anisocoria (percent difference between tropicamide and saline eyes at each time point). This method was preferred to reduce bias resulting from fatigue, stress, drugs, and others that might influence the pupil size [53].
2.4. Statistical Analysis
Differences in proportions were assessed by means of chi-square, Mann-Whitney tests, or Kruskall-Wallis tests. The tests were performed to compare the demographic and clinical factors between subjects with aMCI and cognitively normal individuals in both groups. Any significant items were then entered into a multivariate logistic regression to develop a model for predicting aMCI, using stepwise selection with an inclusion criteria of P < 0.05. Statistical analysis was performed using the SPSS 15.0 software (SPSS Inc., Chicago, IL, USA). The level of significance was set at P < 0.05 for all statistical analyses.
3. Results
There were 109 subjects enrolled in this study (normal cognition: 58, single-domain aMCI: 10, and multiple-domain aMCI: 41); 77 subjects were women (70.6%) and most of the subjects had <6 years of formal education (40%) (Table 1). Using ROC curve, we calculated the cut-off points to determine aMCI as follows: cut-off point for low BDNF plasma level ≤1314 pg/mL, less than 7 for olfactory deficit, and pupillary hypersensitivity response >22% (maximal peak diameter on 30 minutes) (Figures 1, 2, and 3).
Table 1.
Demographic and clinical status in elderly with aMCI and normal cognition.
| Variable | aMCI | Normal | P | Odds ratio | 95% CI |
|---|---|---|---|---|---|
| Age (years) | |||||
| (a) ≤65 | 36 (45.6%) | 43 (54.4%) | 0.84 | 0.84 | 0.36–1.94 |
| (b) >65 | 15 (50.0%) | 15 (50.0%) | |||
| Gender | |||||
| (a) Men | 16 (50.0%) | 16 (50.0%) | 0.82 | 1.20 | 0.53–2.74 |
| (b) Women | 35 (45.5%) | 42 (54.5%) | |||
| Years of education | |||||
| (a) <6 years | 20 (45.5%) | 24 (54.5%) | 0.97 | 0.91 | 0.42–1.97 |
| (b) ≥6 years | 31 (47.7%) | 34 (52.3%) | |||
| Body mass index (BMI) | |||||
| (a) Overweight (≥25.0 kg/m2) | 26 (48.1%) | 28 (51.9%) | 0.93 | 1.11 | 0.53–2.37 |
| (b) Normal (<25.0 kg/m2) | 25 (45.5%) | 30 (54.5%) | |||
| APOE genotype | |||||
| (a) ε4+ | 14 (46.7%) | 16 (53.3%) | 1.00 | 1.00 | 0.43–2.32 |
| (b) ε4− | 36 (46.8%) | 41 (53.2%) | |||
| BDNF level | |||||
| (a) Low (≤1314 pg/mL) | 26 (60.5%) | 17 (39.5%) | 0.04 | 2.51 | 1.14–5.52 |
| (b) High (>1314 pg/mL) | 25 (37.9%) | 41 (62.1%) | |||
| Olfactory deficit | |||||
| (a) Yes (Skor 0–6) | 37 (77.1%) | 11 (22.9%) | <0.0001 | 11.29 | 4.59–27.76 |
| (b) No (Skor 7–10) | 14 (23.0%) | 47 (77.0%) | |||
| Pupillary hypersensitivity to tropicamide | |||||
| (a) Yes (>22%) | 44 (77.2%) | 13 (22.8%) | <0.0001 | 21.76 | 7.94–59.65 |
| (b) No (≤22%) | 7 (13.5%) | 45 (86.5%) | |||
| Systolic BP | |||||
| (a) Hypertension (≥140 mmHg) | 23 (44.2%) | 29 (55.8%) | 0.75 | 0.82 | 0.39–1.75 |
| (b) Normal (<140 mmHg) | 28 (49.1%) | 29 (50.9%) | |||
| Diastolic BP | |||||
| (a) Hypertension (≥90 mmHg) | 29 (52.7%) | 26 (47.3%) | 0.29 | 1.62 | 0.76–3.46 |
| (b) Normal (<90 mmHg) | 22 (40.7%) | 32 (59.3%) | |||
| LDL | |||||
| (a) High (≥130 mg/dL) | 35 (52.2%) | 32 (47.8%) | 0.21 | 1.78 | 0.81–3.90 |
| (b) Normal (<130 mg/dL) | 16 (38.1%) | 26 (61.9%) | |||
| HDL | |||||
| (a) Low (<40 mg/dL for men, <50 mg/dL for women) | 18 (46.2%) | 21 (53.8%) | 1.00 | 0.96 | 0.44–2.11 |
| (b) Normal (≥40 mg/dL for men, ≥50 mg/dL for women) | 33 (47.1%) | 37 (52.9%) |
Figure 1.
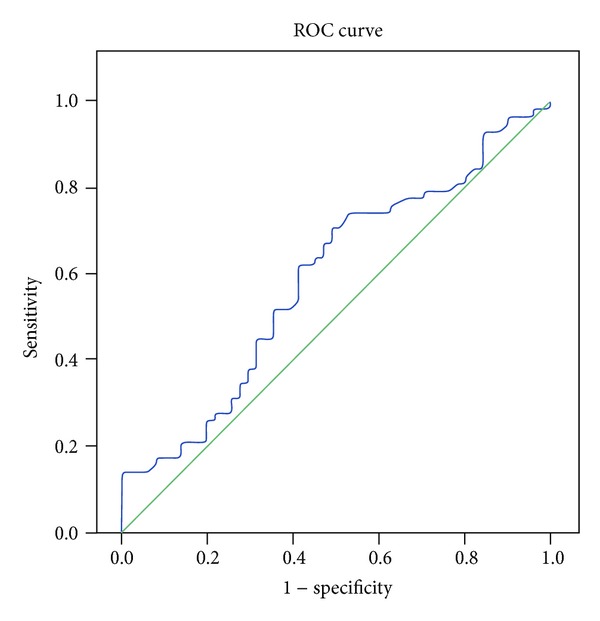
The ROC curve of BDNF plasma level and aMCI.
Figure 2.
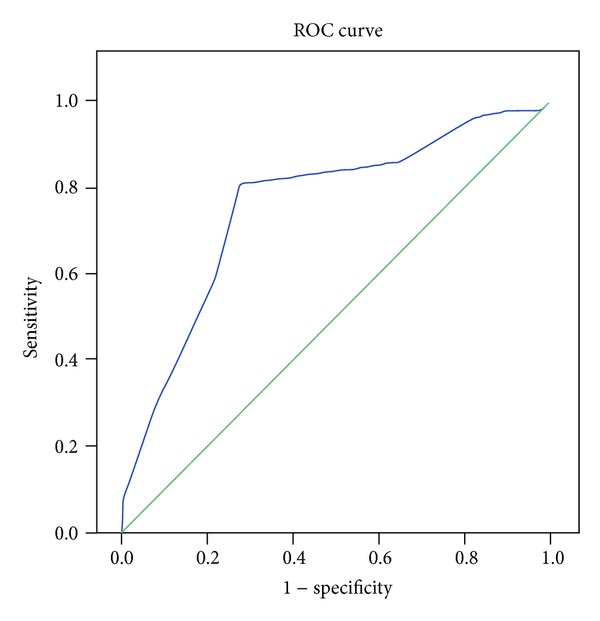
The ROC curve of olfactory deficit and aMCI.
Figure 3.
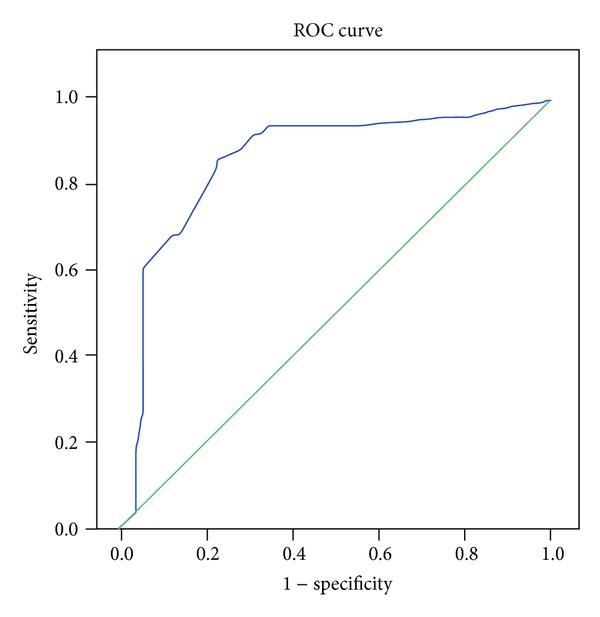
The ROC curve of pupillary response and aMCI.
The majority of subjects had multiple-domain aMCI (35%). There was no significant relationship between aMCI and APOE ε4 genotype. However, four of five subjects with ε4 homozygote also showed multiple-domain aMCI. Group with multiple-domain aMCI had the lowest means of olfactory score and the highest means of pupillary hypersensitivity response (P < 0.0001) (Table 2).
Table 2.
Pupillary response and olfactory score in elderly with aMCI and normal cognition.
| Variable | aMCI | Normal |
P* | |
|---|---|---|---|---|
| Single domain | Multiple domain | |||
| Pupillary response (%) | 30.4 ± 9.30 | 36.06 ± 15.85 | 17.20 ± 13.81 | <0.0001 |
| Olfactory score | 6.10 ± 1.60 | 5.80 ± 1.89 | 7.53 ± 1.68 | <0.0001 |
*Kruskal-Wallis test.
After performing chi-square test, we identified three variables with P < 0.05: pupillary response to tropicamide, olfactory nerve deficit, and BDNF plasma level (Table 1). We further analyzed using logistic regression test and found significant relationship between pupillary hypersensitivity response (OR = 13.69) and olfactory nerve deficit (OR = 5.99) with aMCI.
There was no significant relationship between ε4 genotype with olfactory scores and pupillary response (P > 0.05). However, we observed that subjects with ε4/ε4 genotypes scored the lowest in olfactory test and had the highest pupillary response. There was also significant relationship between low BDNF plasma level with lower olfactory scores (P = 0.012).
Combination of olfactory nerve deficit and pupillary hypersensitivity response generated good values of specificity/Sp 91%, positive predictive value/PPV 87%, and negative predictive value/NPV 75% when differentiating aMCI from those with normal cognition. In conjunction with clinical markers, low BDNF plasma level and presence of ε4+ substantially increased specificity and PPV (Table 3).
Table 3.
Combination of olfactory deficit, pupillary hypersensitivity response, APOE ε4, and BDNF plasma level in elderly with aMCI and normal cognition.
| aMCI | Normal | Sv (%) | Sp (%) | PPV (%) | NPV (%) | OR (95% CI) | P | |
|---|---|---|---|---|---|---|---|---|
| Olfactory deficit | ||||||||
| (a) Yes | 37 (77.1%) | 11 (22.9%) | 72.6 | 81.0 | 77.1 | 77.1 | 11.29 (4.59–27.76) | <0.0001 |
| (b) No | 14 (23.0%) | 47 (77.0%) | ||||||
| Pupillary hypersensitivity response | ||||||||
| (a) Yes | 44 (77.2%) | 13 (22.8%) | 86.3 | 77.6 | 77.2 | 86.5 | 21.76 (7.94–59.65) | <0.0001 |
| (b) No | 7 (13.5%) | 45 (86.5%) | ||||||
| Olfactory deficit and APOE ε4* | ||||||||
| (a) Yes | 13 (92.9%) | 1 (7.1%) | 26.0 | 98.3 | 92.9 | 60.2 | 19.68 (2.47–156.85) | 0.01 |
| (b) No | 37 (39.8%) | 56 (60.2%) | ||||||
| Olfactory deficit and low BDNF plasma level | ||||||||
| (a) Yes | 22 (84.6%) | 4 (15.4%) | 43.1 | 93.1 | 84.6 | 65.1 | 10.24 (3.22–32.57) | <0.0001 |
| (b) No | 29 (34.9%) | 54 (65.1%) | ||||||
| Pupillary hypersensitivity response and APOE ε4* | ||||||||
| (a) Yes | 13 (76.5%) | 4 (23.5%) | 26.0 | 92.9 | 76.5 | 58.9 | 4.66 (1.41–15.41) | 0.016 |
| (b) No | 37 (41.1%) | 53 (58.9%) | ||||||
| Pupillary hypersensitivity response and low BDNF plasma level | ||||||||
| (a) Yes | 20 (79.9%) | 6 (23.1%) | 39.2 | 89.7 | 76.9 | 62.7 | 5.59 (2.03–15.43) | 0.001 |
| (b) No | 31 (37.3%) | 52 (62.7%) | ||||||
| Olfactory deficit and pupillary hypersensitivity response | ||||||||
| (a) Yes | 33 (86.8%) | 5 (13.2%) | 64.7 | 91.4 | 86.8 | 74.7 | 19.43 (6.59–57.34) | <0.0001 |
| (b) No | 18 (25.4%) | 53 (74.6%) |
Note. *APOE ε2/ε4 genotype is not included.
In the end of the study, we replicated the test on different group (30 subjects) and the results were almost identical. Combination of olfactory deficit and pupillary hypersensitivity response in differentiating aMCI from normal cognitive function yielded Sv 70%, Sp 95%, PPV 88%, and NPV 86%.
4. Discussion
The majority of the subjects in this study came from low educational background. This finding is similar to other study of the elderly population in Indonesia [44]. This may also explain the high prevalence of aMCI (43%) found in our study. The prevalence is higher compared to a study by Luck et al. that stated that the prevalence of aMCI was 17% among elderly aged >65 years old [54].
Four of five subjects with ε4+/+ also showed multiple-domain aMCI. Blom et al. reported that seven of eight aMCI patients with ε4+/+ genotypes eventually progressed to dementia [55]. We found significant difference in pupillary response and olfactory scores for each type of MCI. Pupil dilatation response in those with multiple-domain aMCI was higher in comparison with normal cognition (P < 0.0001). Arai et al. stated that elderly with AD demonstrated pupil dilatation up to 43% when compared to 15.6% in those with normal cognition [56]. In this study, multiple-domain aMCI subjects scored the lowest olfactory score compared to those with single-domain aMCI and normal cognition (Table 3). It has been widely known that multiple-domain aMCI has the worst outcome and a predisposing factor toward dementia [57].
Higuchi et al. reported a significant relationship between ε4+ and pupil hypersensitivity response [21]. In a study by Wang et al., they demonstrated the difference between subjects with and without ε4 allele in identifying the odors [9]. In our study, subjects with ε4 homozygote significantly demonstrated the lowest olfactory scores and highest pupillary hypersensitivity response.
We did not find a significant relationship between APOE and aMCI. Due to the multifactorial nature, APOE solely could not be held responsible for the disease. Despite the fact that APOE ε4 genotype is a risk factor that accelerates degenerative process in the brain (AD), ε4 carrier status alone could not be accountable for cognitive decline or dementia [58].
The peak dilatation response to 0.01% tropicamide was about 30 min in this study which was similar to other reports [17, 25, 56, 59, 60]. Pupillary response to tropicamide was previously studied to expose degenerative process in Edinger Westphal nucleus. This area demonstrated degeneration in early stage of AD [61]. Pupillary response is an objective test that does not require neuropsychological examination/interview. This can be beneficial in special cases where patients are not able to participate in neuropsychological test. However, this test is not suitable for those with eye disorders such as history of cataract surgery and in diabetes mellitus patients (in whom autonomy nervous system has been compromised).
In our study, the cut-off point for pupil dilatation is >22% for differentiating elderly with aMCI. There are various cut-off points in other publications that may due be to different patients criteria, different age group, and concentration of tropicamide being administered. Scinto et al. reported a cut-off point of 13% in 30 minutes to differentiate dementia and normal cognition in the elderly using 0.01% tropicamide [17]. Another report by Iijima et al. used a cut-off point of 14.5% in 60 minutes using less concentrated tropicamide (0.005%) [20].
In our study, we established the cut-off point <7 for olfactory score to diagnose aMCI in elderly. Eibenstein et al. set a higher cut-off point ≥10 (out of 12) to differentiate elderly with normal cognition and aMCI and stated that scores ≤6 were anosmic [7]. A study by Tabert et al. using 10 different odors set a cut-off point ≤7 in differentiating DA with aMCI [8]. Olfactory test is not similar with cognitive assessment because the former is not influenced by educational level nor depression; hence, it is suitable to use in elderly patients with low level of education and depression [4].
Lower level of BDNF was observed in aMCI group than elderly with normal cognition (P = 0.04). This is supported by a study by Lee et al., where they observed low level of BDNF in MCI and dementia patients [40].
High LDL level is undoubtedly a risk factor for vascular disease but its connection with cognitive dysfunction has not yet been established. Yasuno et al. declared no relationship between level of LDL, triglycerides, and total cholesterol with cognitive scores [62]. Another study by Elias et al. also showed no relationship between aMCI and cholesterol, specifically between total cholesterol and memory domain [63]. Reitz et al. stated that plasma lipid levels in the elderly are not associated with the risk of MCI [64]. The relationship between HDL and cognitive function is still inconclusive. Van Exel et al. stated that low HDL level was related to low MMSE scores and these low scores of MMSE did not result from the atherosclerosis process [65]. In contrary, Gillum and Obisesan did not find any significant relationship between HDL level and cognitive function [66].
There was no significant relationship between systolic and diastolic hypertension with aMCI in our study. The issue of hypertension and aMCI and dementia remains controversial. Vascular disease is a risk factor for developing MCI in some studies [67, 68]. Farmer et al. stated that there was no relationship between hypertension and cognitive dysfunction [69]. In another research conducted in Jakarta involving 1001 elderly patients with mean age 68 ± 7 years old, there was no relationship between recall memory and total MMSE scores with hypertension [70]. A different finding is shown by Reitz et al. using 918 subjects, followed for mean of 4.7 years where they found hypertension as a risk factor for nonamnestic MCI (naMCI) not for aMCI [71].
In this study, 13 of 14 subjects with olfactory deficit and ε4+ genotypes presented with aMCI (OR = 20). Graves et al. stated that subjects with olfactory deficit and ε4+ genotype were 4.9 times likely to suffer from cognitive decline compared to those without olfactory deficit and ε4– [10]. We also observed subjects with pupillary hypersensitivity and having ε4+ genotype was 4.7 times likely to have aMCI. Hence, presence of ε4+ genotype may substantially increase specificity and positive predictive value toward aMCI. In addition, our study showed that 22 out of 26 patients with olfactory deficit and low BDNF plasma level had aMCI (OR = 10).
Based on the findings in our study, biological markers, such as APOE and BDNF, when used in conjunction with clinical markers of pupillary response or olfactory test can increase positive predictive value (PPV) toward aMCI diagnosis. Our findings supported the statement by Lautenschlager et al. that combination of biological and clinical markers is essential to increase PPV in MCI diagnosis [72].
Multivariate analysis in our study revealed that olfactory deficit and pupillary response were related significantly to aMCI. We also found that combination of olfactory test and pupillary response to tropicamide was the best model when considering Sp and PPV (Sv 64,7%, Sp 91,4%, and PPV 86,8%) in comparison to the other combination. We do acknowledge the limitation of our study that we did not perform analysis for combinations of three or more variables due to sample size. To our knowledge, this is the first research combining the two variables at one time. Taking into consideration that the two markers can aid the psychometric evaluation for diagnosis (not for screening purpose), hence, higher specificity is more important than sensitivity.
When we replicated the test on different group (30 subjects), the results for diagnostic values of olfactory deficit and pupillary response were almost identical. The combination of two clinical markers can increase the specificity up to 95% and PPV up to 88%. This shows that the diagnostic values of pupillary response to tropicamide and olfactory deficit in diagnosing aMCI were consistent.
We share optimism that, in the future, combination of these two clinical markers (olfactory test and pupillary response to tropicamide) can be widely implemented together with cognitive assessment. Hence, clinicians can perform early diagnosis of the degenerative process in the brain using various alternatives and institute proper treatment for a better quality of life in the elderly.
Conflict of Interests
The authors do not have any direct financial relation with the trademarks mentioned in the paper that might lead to a conflict of interests for any of the authors. The authors declare no potential conflict of interests.
References
- 1.Petersen RC, Smith GE, Waring SC, Ivnik RJ, Tangalos EG, Kokmen E. Mild cognitive impairment: clinical characterization and outcome. Archives of Neurology. 1999;56(3):303–308. doi: 10.1001/archneur.56.3.303. [DOI] [PubMed] [Google Scholar]
- 2.Schmidtke K, Hermeneit S. High rate of conversion to Alzheimer’s disease in a cohort of amnestic MCI patients. International Psychogeriatrics. 2008;20(1):96–108. doi: 10.1017/S1041610207005509. [DOI] [PubMed] [Google Scholar]
- 3.Petersen RC, Parisi JE, Dickson DW, et al. Neuropathologic features of amnestic mild cognitive impairment. Archives of Neurology. 2006;63(5):665–672. doi: 10.1001/archneur.63.5.665. [DOI] [PubMed] [Google Scholar]
- 4.McCaffrey RJ, Duff K, Solomon GS. Olfactory dysfunction discriminates probable Alzheimer’s dementia from major depression: a cross-validation and extension. Journal of Neuropsychiatry and Clinical Neurosciences. 2000;12(1):29–33. doi: 10.1176/jnp.12.1.29. [DOI] [PubMed] [Google Scholar]
- 5.Serby M, Larson P, Kalkstein D. The nature and course of olfactory deficits in Alzheimer’s disease. The American Journal of Psychiatry. 1991;148(3):357–360. doi: 10.1176/ajp.148.3.357. [DOI] [PubMed] [Google Scholar]
- 6.Doty RL, Marcus A, Lee WW. Development of the 12 item cross cultural smell identification test (CC-SIT) Laryngoscope. 1996;106(3):353–356. doi: 10.1097/00005537-199603000-00021. [DOI] [PubMed] [Google Scholar]
- 7.Eibenstein A, Fioretti AB, Simaskou MN, et al. Olfactory screening test in mild cognitive impairment. Neurological Sciences. 2005;26(3):156–160. doi: 10.1007/s10072-005-0453-2. [DOI] [PubMed] [Google Scholar]
- 8.Tabert MH, Liu X, Doty RL, et al. A 10-item smell identification scale related to risk for Alzheimer’s disease. Annals of Neurology. 2005;58(1):155–160. doi: 10.1002/ana.20533. [DOI] [PubMed] [Google Scholar]
- 9.Wang Q-S, Tian L, Huang Y-L, Qin S, He L-Q, Zhou J-N. Olfactory identification and apolipoprotein E ε4 allele in mild cognitive impairment. Brain Research. 2002;951(1):77–81. doi: 10.1016/s0006-8993(02)03137-2. [DOI] [PubMed] [Google Scholar]
- 10.Graves AB, Bowen JD, Rajaram L, et al. Impaired olfaction as a marker for cognitive decline: interaction with apolipoprotein E ε4. Neurology. 1999;53(7):1480–1487. doi: 10.1212/wnl.53.7.1480. [DOI] [PubMed] [Google Scholar]
- 11.Devanand DP, Michaels-Marston KS, Liu X, et al. Olfactory deficits in patients with mild cognitive impairment predict Alzheimer’s disease at follow-up. The American Journal of Psychiatry. 2000;157(9):1399–1405. doi: 10.1176/appi.ajp.157.9.1399. [DOI] [PubMed] [Google Scholar]
- 12.Murphy C, Jernigan TL, Fennema-Notestine C. Left hippocampal volume loss in Alzheimer’s disease is reflected in performance on odor identification: a structural MRI study. Journal of the International Neuropsychological Society. 2003;9(3):459–471. doi: 10.1017/S1355617703930116. [DOI] [PubMed] [Google Scholar]
- 13.Warner MD, Peabody CA, Flattery JJ, Tinklenberg JR. Olfactory deficits and Alzheimer’s disease. Biological Psychiatry. 1986;21(1):116–118. doi: 10.1016/0006-3223(86)90013-2. [DOI] [PubMed] [Google Scholar]
- 14.Koss E. Olfactory dysfunction in Alzheimer’s disease. Developmental Neuropsychology. 1986;2(2):89–99. [Google Scholar]
- 15.Doty RL, Reyes PF, Gregor T. Presence of both odor identification and detection deficits in Alzheimer’s disease. Brain Research Bulletin. 1987;18(5):597–600. doi: 10.1016/0361-9230(87)90129-8. [DOI] [PubMed] [Google Scholar]
- 16.Koss E, Weiffenbach JM, Haxby JV, Friedland RP. Olfactory detection and identification performance are dissociated in early Alzheimer’s disease. Neurology. 1988;38(8):1228–1232. doi: 10.1212/wnl.38.8.1228. [DOI] [PubMed] [Google Scholar]
- 17.Scinto LFM, Daffner KR, Dressler D, et al. A potential noninvasive neurobiological test for Alzheimer’s disease. Science. 1994;266(5187):1051–1054. doi: 10.1126/science.7973660. [DOI] [PubMed] [Google Scholar]
- 18.Grünberger J, Linzmayer L, Walter H, et al. Receptor test (pupillary dilatation after application of 0.01% tropicamide solution) and determination of central nervous activation (Fourier analysis of pupillary oscillations) in patients with Alzheimer’s disease. Neuropsychobiology. 1999;40(1):40–46. doi: 10.1159/000026595. [DOI] [PubMed] [Google Scholar]
- 19.Fourie J. Age dependent pupillary and cognitive responses to cholinergic drugs as a model for identification of future biological markers for Alzheimer disease [Ph.D. thesis] Toronto, Canada: University of Toronto; 1999. [Google Scholar]
- 20.Iijima A, Haida M, Ishikawa N, Ueno A, Minamitani H, Shinohara Y. Re-evaluation of tropicamide in the pupillary response test for Alzheimer’s disease. Neurobiology of Aging. 2003;24(6):789–796. doi: 10.1016/s0197-4580(02)00235-x. [DOI] [PubMed] [Google Scholar]
- 21.Higuchi S, Matsushita S, Hasegawa Y, Muramatsu T, Arai H, Hayashida M. Apolipoprotein E ε4 allele and pupillary response to tropicamide. The American Journal of Psychiatry. 1997;154(5):694–696. doi: 10.1176/ajp.154.5.694. [DOI] [PubMed] [Google Scholar]
- 22.Gómez-Tortosa E, del Barrio A, Jiménez-Alfaro I. Pupil response to tropicamide in Alzheimer’s disease and other neurodegenerative disorders. Acta Neurologica Scandinavica. 1996;94(2):104–109. doi: 10.1111/j.1600-0404.1996.tb07038.x. [DOI] [PubMed] [Google Scholar]
- 23.Higuchi S, Matsushita S, Hasegawa Y, Muramatsu T, Arai H. Pupillary response to tropicamide in Japanese patients with alcoholic dementia, Alzheimer’s disease, and vascular dementia. Experimental Neurology. 1997;144(1):199–201. doi: 10.1006/exnr.1997.6417. [DOI] [PubMed] [Google Scholar]
- 24.Imamura Y, Kojima H, Haraoka K. Pupil dilatation response to the acethylcholine receptor antagonist tropicamide in normal aged and senile dementia subjects. Neurobiology of Aging. 1996;17(4, supplement 1):p. S165. [Google Scholar]
- 25.Kálmán J, Kanka A, Maglóczky E, Szóke A, Járdánházy T, Janka Z. Increased mydriatic response to tropicamide is a sign of cholinergic hypersensitivity but not specific to late-onset sporadic type of Alzheimer’s dementia. Biological Psychiatry. 1997;41(8):909–911. doi: 10.1016/S0006-3223(97)00021-8. [DOI] [PubMed] [Google Scholar]
- 26.Matsushita S, Arai H, Hasegawa Y, et al. Apolipoprotein Ee4 allele and pupillary response to tropicamide in Alzheimer’s disease and cognitively normal subjects. Neurobiology of Aging. 1996;17(4, supplement 1):p. S164. [Google Scholar]
- 27.Titus AM, Revest P, Shortland P. The Nervous System, Basic Science and Clinical Conditions. New York, NY, USA: Elseiver; 2007. [Google Scholar]
- 28.Ertekin-Taner N. Genetics of Alzheimer’s disease: a centennial review. Neurologic Clinics. 2007;25(3):611–667. doi: 10.1016/j.ncl.2007.03.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Polvikoski T, Sulkava R, Haltia M, et al. Apolipoprotein E, dementia, and cortical deposition of β-amyloid protein. The New England Journal of Medicine. 1995;333(19):1242–1247. doi: 10.1056/NEJM199511093331902. [DOI] [PubMed] [Google Scholar]
- 30.Petersen RC, Smith GE, Ivnik RJ, et al. The APOE ε4 status as a predictor of the developmental of Alzheimer’s disease in memory impaired individuals. The Journal of the American Medical Association. 1995;273(16):1274–1278. [PubMed] [Google Scholar]
- 31.Small BJ, Rosnick CB, Fratiglioni L, Bäckman L. APOE ε4 and cognitive performance: a metaanalysis. Psychology and Aging. 2004;19(4):592–600. doi: 10.1037/0882-7974.19.4.592. [DOI] [PubMed] [Google Scholar]
- 32.van der Vlies AE, Pijnenburg YAL, Koene T, et al. Cognitive impairment in Alzheimer’s disease is modified by APOE genotype. Dementia and Geriatric Cognitive Disorders. 2007;24(2):98–103. doi: 10.1159/000104467. [DOI] [PubMed] [Google Scholar]
- 33.Ramakers IHGB, Visser PJ, Aalten P, et al. The association between APOE genotype and memory dysfunction in subjects with mild cognitive impairment is related to age and Alzheimer pathology. Dementia and Geriatric Cognitive Disorders. 2008;26(2):101–108. doi: 10.1159/000144072. [DOI] [PubMed] [Google Scholar]
- 34.Boyle PA, Buchman AS, Wilson RS, Kelly JF, Bennett DA. The APOE ε4 allele is associated with incident mild cognitive impairment among community-dwelling older persons. Neuroepidemiology. 2010;34(1):43–49. doi: 10.1159/000256662. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Cunha C, Brambilla R, Thomas KL. A simple role for BDNF in learning and memory? Frontiers in Molecular Neuroscience. 2010;3:1–14. doi: 10.3389/neuro.02.001.2010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Laske C, Stransky E, Leyhe T, et al. BDNF serum and CSF concentrations in Alzheimer’s disease, normal pressure hydrocephalus and healthy controls. Journal of Psychiatric Research. 2007;41(5):387–394. doi: 10.1016/j.jpsychires.2006.01.014. [DOI] [PubMed] [Google Scholar]
- 37.Pan W, Banks WA, Fasold MB, Blunth J, Katin AJ. Transport of BDNF across the BBB. Neuropharmacology. 2006;37(12):1553–1561. doi: 10.1016/s0028-3908(98)00141-5. [DOI] [PubMed] [Google Scholar]
- 38.Dogliotti G, Galliera E, Licastro F, Corsi MM. Age-related changes in plasma levels of BDNF in Down syndrome patients. Immunity and Ageing. 2010;7, article 2 doi: 10.1186/1742-4933-7-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Yu H, Zhang Z, Shi Y, et al. Association study of the decreased serum BDNF concentrations in amnestic mild cognitive impairment and the Val66Met polymorphism in Chinese han. Journal of Clinical Psychiatry. 2008;69(7):1104–1111. doi: 10.4088/jcp.v69n0710. [DOI] [PubMed] [Google Scholar]
- 40.Lee JG, Shin BS, You YS, et al. Decreased serum brain-derived neurotrophic factor levels in elderly Korean with dementia. Psychiatry Investigation. 2009;6(4):299–305. doi: 10.4306/pi.2009.6.4.299. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Hwang KS, Gylys K, Taylor K, et al. Plasma BDNF associations with cortical thickness in normal controls and mild cognitive impairment. Alzheimer's & Dementia. 2011;7(4, supplement):p. S319. [Google Scholar]
- 42.von Bohlen O, Halbach Involvement of BDNF in age-dependent alterations in the hippocampus. Frontiers in Aging Neuroscience. 2010;2:1–11. doi: 10.3389/fnagi.2010.00036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Suchowersky O, Reich S, Perlmutter J, Zesiewicz T, Gronseth G, Weiner WJ. Practice parameter: diagnosis and prognosis of new onset Parkinson disease (an evidence-based review): report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2006;66(7):968–975. doi: 10.1212/01.wnl.0000215437.80053.d0. [DOI] [PubMed] [Google Scholar]
- 44.Handajani YS. Disability measurement index and prediction of the life quality of the elderly in DKI Jakarta [Ph.D. thesis] Depok, Indonesia: University of Indonesia; 2006. [Google Scholar]
- 45.Yesavage JA, Brink TL, Rose TL, et al. Development and validation of a geriatric depression screening scale: a preliminary report. Journal of Psychiatric Research. 1983;17(1):37–49. doi: 10.1016/0022-3956(82)90033-4. [DOI] [PubMed] [Google Scholar]
- 46.American Diabetes Association. Standard of medical care in diabetes 2012. Diabetes Care. 2012;35:S11–S63. doi: 10.2337/dc12-s011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Asian-Pacific Type 2 Diabetes Policy Group. Type 2 Diabetes: Practical Targets and Treatments. 3rd edition. Melbourne, Australia: 2002. [Google Scholar]
- 48.Welsh KA, Butters N, Mohs RC, et al. The Consortium to Establish a Registry for Alzheimer’s Disease (CERAD). Part V. A normative study of the neuropsychological battery. Neurology. 1994;44(4):609–614. doi: 10.1212/wnl.44.4.609. [DOI] [PubMed] [Google Scholar]
- 49.Winblad B, Palmer K, Kivipelto M, et al. Mild cognitive impairment—beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment. Journal of Internal Medicine. 2004;256(3):240–246. doi: 10.1111/j.1365-2796.2004.01380.x. [DOI] [PubMed] [Google Scholar]
- 50.Luhur JJ, Mirsha, Handajani YS, Turana Y. Determination of familiar odors for standard examination of olfactory function of the elderly in Jakarta. Neurona. 2012;29:7–13. [Google Scholar]
- 51.Yoon MK, Schmidt G, Lietman T, McLeod SD. Interexaminer and intraexaminer reliability of pupil diameter measurement using the colvard pupillometer. Investigative Ophthalmology and Visual Science. 2003;44 [Google Scholar]
- 52.Bootsma S, Tahzib N, Eggink F, de Brabander J, Nuijts RMMA. Comparison of two pupillometers in determining pupil size for refractive surgery. Acta Ophthalmologica Scandinavica. 2007;85(3):324–328. doi: 10.1111/j.1600-0420.2006.00823.x. [DOI] [PubMed] [Google Scholar]
- 53.Granholm E, Morris S, Galasko D, Shults C, Rogers E, Vukov B. Tropicamide effects on pupil size and pupillary light reflexes in Alzheimer’s and Parkinson’s disease. International Journal of Psychophysiology. 2003;47(2):95–115. doi: 10.1016/s0167-8760(02)00122-8. [DOI] [PubMed] [Google Scholar]
- 54.Luck T, Riedel-Heller SG, Kaduszkiewicz H, et al. Mild cognitive impairment in general practice: age-specific prevalence and correlate results from the German study on ageing, cognition and dementia in primary care patients (AgeCoDe) Dementia and Geriatric Cognitive Disorders. 2007;24(4):307–316. doi: 10.1159/000108099. [DOI] [PubMed] [Google Scholar]
- 55.Blom ES, Giedraitis V, Zetterberg H, et al. Rapid progression from mild cognitive impairment to alzheimer’s disease in subjects with elevated levels of tau in cerebrospinal fluid and the Apoe ε4/ε4 genotype. Dementia and Geriatric Cognitive Disorders. 2009;27(5):458–464. doi: 10.1159/000216841. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Arai H, Terajima M, Nakagawa T, Higuchi S, Mochizuki H, Sasaki H. Pupil dilatation assay by tropicamide is modulated by apolipoprotein e ∈4 allele dosage in Alzheimer’s disease. NeuroReport. 1996;7(4):918–920. doi: 10.1097/00001756-199603220-00017. [DOI] [PubMed] [Google Scholar]
- 57.Petersen RC, Stevens JC, Ganguli M, Tangalos EG, Cummings JL, DeKosky ST. Practice parameter: early detection of dementia: mild cognitive impairment (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2001;56(9):1133–1142. doi: 10.1212/wnl.56.9.1133. [DOI] [PubMed] [Google Scholar]
- 58.Devanand DP, Pelton GH, Zamora D, et al. Predictive utility of apolipoprotein E genotype for Alzheimer disease in outpatients with mild cognitive impairment. Archives of Neurology. 2005;62(6):975–980. doi: 10.1001/archneur.62.6.975. [DOI] [PubMed] [Google Scholar]
- 59.Fridh M, Havelius U, Elofsson G, Hindfelt B. The pupillary response to tropicamide in Alzheimer’s disease. Acta Ophthalmologica Scandinavica. 1996;74(3):276–279. doi: 10.1111/j.1600-0420.1996.tb00091.x. [DOI] [PubMed] [Google Scholar]
- 60.Kurz A, Marquard R, Fremke S, Leipert KP. Pupil dilation response to tropicamide: a biological test for Alzheimer’s disease? Pharmacopsychiatry. 1997;30(1):12–15. doi: 10.1055/s-2007-979476. [DOI] [PubMed] [Google Scholar]
- 61.Scinto LFM, Frosch M, Wu CK, Daffner KR, Gedi N, Geula C. Selective cell loss in Edinger-Westphal in asymptomatic elders and Alzheimer’s patients. Neurobiology of Aging. 2001;22(5):729–736. doi: 10.1016/s0197-4580(01)00235-4. [DOI] [PubMed] [Google Scholar]
- 62.Yasuno F, Tanimukai S, Sasaki M, et al. Association between cognitive function and plasma lipids of the elderly after controlling for apolipoprotein E genotype. American Journal of Geriatric Psychiatry. 2012;20:574–583. doi: 10.1097/JGP.0b013e318211819b. [DOI] [PubMed] [Google Scholar]
- 63.Elias PK, Elias MF, D’Agostino RB, Sullivan LM, Wolf PA. Serum cholesterol and cognitive performance in the Framingham Heart Study. Psychosomatic Medicine. 2005;67(1):24–30. doi: 10.1097/01.psy.0000151745.67285.c2. [DOI] [PubMed] [Google Scholar]
- 64.Reitz C, Tang M-X, Manly J, Schupf N, Mayeux R, Luchsinger JA. Plasma lipid levels in the elderly are not associated with the risk of mild cognitive impairment. Dementia and Geriatric Cognitive Disorders. 2008;25(3):232–237. doi: 10.1159/000115847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.van Exel E, de Craen AJM, Gussekloo J, et al. Association between high-density lipoprotein and cognitive impairment in the oldest old. Annals of Neurology. 2002;51(6):716–721. doi: 10.1002/ana.10220. [DOI] [PubMed] [Google Scholar]
- 66.Gillum RF, Obisesan TO. High-density lipoprotein cholesterol, cognitive function and mortality in a U.S. national cohort. Lipids in Health and Disease. 2011;10, article 26 doi: 10.1186/1476-511X-10-26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Lopez OL, Jagust WJ, Dulberg C, et al. Risk factors for mild cognitive impairment in the cardiovascular health study cognition study. Archives of Neurology. 2003;60(10):1394–1399. doi: 10.1001/archneur.60.10.1394. [DOI] [PubMed] [Google Scholar]
- 68.Tervo S, Kivipelto M, Hänninen T, et al. Incidence and risk factors for mild cognitive impairment: a population-based three-year follow-up study of cognitively healthy elderly subjects. Dementia and Geriatric Cognitive Disorders. 2004;17(3):196–203. doi: 10.1159/000076356. [DOI] [PubMed] [Google Scholar]
- 69.Farmer ME, Kittner SJ, Abbott RD, Wolz MM, Wolf PA, White LR. Longitudinally measured blood pressure, antihypertensive medication use, and cognitive performance: The Framingham Study. Journal of Clinical Epidemiology. 1990;43(5):475–480. doi: 10.1016/0895-4356(90)90136-d. [DOI] [PubMed] [Google Scholar]
- 70.Turana Y, Handayani YS. Relationship between vascular risk factors and physical exercise with cognitive function of the elderly in Jakarta. Proceedings of the INASH Scientific Meeting; February 2010. [Google Scholar]
- 71.Reitz C, Tang M-X, Manly J, Mayeux R, Luchsinger JA. Hypertension and the risk of mild cognitive impairment. Archives of Neurology. 2007;64(12):1734–1740. doi: 10.1001/archneur.64.12.1734. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Lautenschlager NT, Flicker L, Vasikaran S, Leedman P, Almeida OP. Subjective memory complaints with and without objective memory impairment: relationship with risk factors for dementia. American Journal of Geriatric Psychiatry. 2005;13(8):731–734. doi: 10.1176/appi.ajgp.13.8.731. [DOI] [PubMed] [Google Scholar]