

Abstract
Objective. To assess the health-related quality of life (HRQoL) of student pharmacists and explore factors related to HRQoL outcomes of student pharmacists in a doctor of pharmacy (PharmD) program at a public university.
Methods. A survey instrument was administered to all student pharmacists in a PharmD program at a public university to evaluate differences and factors related to the HRQoL outcomes of first-year (P1), second-year (P2), third-year (P3), and fourth-year (P4) student pharmacists in the college. The survey instrument included attitudes and academic-related self-perception, a 12-item short form health survey, and personal information components.
Results. There were 304 students (68.6%) who completed the survey instrument. The average health state classification measure and mental health component scale (MCS-12) scores were significantly higher for P4 students when compared with the P1through P3 students. There was no difference observed in the physical component scale (PCS-12) scores among each of the 4 class years. Significant negative impact on HRQoL outcomes was observed in students with higher levels of confusion about how they should study (scale lack of regulation) and concern about not being negatively perceived by others (self-defeating ego orientation), while school satisfaction increased HRQoL outcomes (SF-6D, p<0.001; MCS-12, p=0.013). A greater desire to be judged capable (self-enhancing ego-orientation) and career satisfaction were positively associated with the PCS-12 scores (p<0.05).
Conclusion. Factors associated with the HRQoL of student pharmacists were confusion regarding how to study, ego orientation, satisfaction with the chosen college of pharmacy, and career satisfaction. First-year through third-year student pharmacists had lower HRQoL as compared with P4 students and the US general population. Support programs may be helpful for students to maintain or improve their mental and overall health.
Keywords: health-related quality of life, student pharmacists, perceived self-efficacy, ego-orientation
INTRODUCTION
Health-related quality of life is negatively associated with perceived stress among health professions students,1-6 with student pharmacists reporting higher psychological distress than nursing and medical students.7,8 Stress triggers reported by student pharmacists include academic workload and examinations, relationship problems, financial concerns, and difficulty of combining and organizing their study and leisure time.3,9,10 Some stressors are unavoidable because of the inherent nature of pharmacy education, and student pharmacists may experience sleep deprivation, decreased physical health and self-care, emotional exhaustion, burnout, and psychological morbidity.11-13 Students may not recognize the level of their elevated stress. Instead, they may dismiss it as a natural response to the rigors of academic life and avoid seeking appropriate help.14 Consequently, these stress triggers may contribute to diminished overall HRQoL and decreased academic performance.3
Students’ academic performance is affected by a multitude of factors that include attitude toward their educational program, perceived academic competence, self-driven regulation of learning, self-test directedness (willingness to test one’s own study ability), ego-orientation, and help-seeking behavior.15 When students feel unsure about their career choice or chosen college or school of pharmacy, they may not perform well or exert appropriate effort toward their academic goals. Perceived academic competence, self-driven regulation of learning, and self-test directedness contribute to a greater level of individual self-efficacy. Perceived self-efficacy is the belief in one’s competence to organize and execute the activities required to reach given attainments, such as managing the academic workload necessary to obtain a PharmD degree.16 Individuals with high perceived self-efficacy are more likely to deal with a challenging academic workload without feeling overwhelmed, confused, or stressed.17,18 Health-related quality of life is positively associated with high self-efficacy in health-related behavior literature.19-21 Interventions that increase self-efficacy may lead to improved HRQoL.22-24 Ego orientation (the perceived ability relative to others) is categorized as either self-defeating (performance avoidance goals) or self-enhancing (performance approach goals).25-27 Students with high levels of self-defeating ego orientation may experience more stress and avoid seeking help,15 which may lead to decreased HRQoL.
Our objective for this study was to measure the HRQoL of student pharmacists at the University of Arkansas for Medical Sciences College of Pharmacy (UAMSCOP) and explore the impact that factors such as perception toward pharmacy education, perceived self-efficacy, ego orientation, and academic help-seeking behaviors have on student pharmacist HRQoL. Identifying these associations will allow institutions to improve the health and wellness of their student pharmacists and, hopefully, improve student success in pharmacy programs. We previously reported factors associated with academic help-seeking behavior15 which was 1 of the 2 objectives of this project.
METHODS
Data were collected from student pharmacists aged 18 years or older enrolled in the UAMSCOP’s PharmD program. First-year through fourth-year student pharmacists were invited to participate in a cross-sectional survey. Survey instruments were distributed at the conclusion of the 2011 spring semester during the last required course of each P1, P2, and P3 class. The P4 students were asked to complete the survey instrument during the class meeting prior to graduation. Participation in this study was strictly voluntary and anonymous. Additional details concerning the data collection process are described in the paper on academic help-seeking behavior, the first phase of this research project.15 The study protocol was approved by the University of Arkansas for Medical Sciences Institution Review Board.
The self-administered, paper-and-pencil survey instrument took approximately 10 minutes to complete. It was divided into 4 sections, including attitudes and academic help-seeking behavior, health status, demographics, and an open section for any comments on school-related issues.
The attitudes and academic health-seeking behavior section comprised 9 domains: (1) perceptions of academic help-seeking as threatening, (2) perceptions of academic help-seeking behavior, (3) scale for lack of self-regulation and scale for self-test directedness, (4) ambivalence scale, (5) self-enhancing ego orientation, (6) self-defeating ego orientation, (7) perceived academic competence, (8) perceived faculty helpfulness, and (9) satisfaction towards career and school selection.15 The level of agreement for each statement in the survey instrument was determined using a 5-point Likert scale (1=disagree entirely; 2=disagree for the most part; 3=undecided or do not know; 4=agree for the most part; 5=agree entirely). All of the domains were valid and reliable in our sample.15 A summary score of each of the first 8 domains was calculated by summing all statements with higher summary scores representing stronger traits. Responses to satisfaction with chosen college of pharmacy and career satisfaction questions were coded again and listed separately to interpret results more easily (a higher score represented higher satisfaction). All of the domains were used to explore their associations with students’ HRQoL in the analyses.
The student pharmacists’ HRQoL was measured using the 12-item short-form healthy survey, version 2.0 (SF-12v2). The SF-12v2 is a multidimensional generic measure of HRQoL which is available as a self-administered instrument. It is widely used in clinical trials and routine outcome assessment because of its brevity and psychometric performance.28,29 The SF-12v2 produces several HRQoL components, including the PCS-12 and MCS-12, and 8 additional subscales (physical function, role physical limitation, bodily pain, general health, vitality, role emotional function, social functioning, and mental health). Scoring algorithms of the PCS-12, MCS-12, and 8 subscales were developed using factor weights obtained from principle component analysis with orthogonal practice experience from the US healthy population (mean age 50±10 years).30,31 Health state classifications can be obtained from the SF-12v2 using SF-6D scores derived from a standard gamble approach.32 The SF-6D scores are the estimation of overall health status in a continuous scale ranging from 0.35 (worst possible health) to 1.0 (perfect health). The average SF-6D score of the US population norm was 0.80.33 The scoring process for all HRQoL component scores was performed in SAS, version 9.3 (SAS Institute Inc, Cary, NC).
Participant demographics, and the attitudes and academic help-seeking behavior domain summary scores were analyzed using descriptive statistics. Demographic differences between the group of participants who reported earning a D or F and the group who did not were analyzed using t test (for continuous variables, including age and reported grade point average [GPA]) and chi-square statistics (for categorical variables including gender, race/ethnicity, and program year). Missing data on each domain of the attitudes and academic help-seeking behavior was imputed with a mean score of that domain.
Differences in the attitudes and academic help-seeking behavior domain summary scores between the group of participants who reported earning a D or F and the group who did not were analyzed using rank analysis of covariance (ANCOVA) controlled by age, gender, and ethnicity (Mantel-Haenszel test). The ANCOVA was further used to determine any HRQoL score differences among the 4 class years in the PharmD degree program, controlled for age, gender, and reported receipt of a D or F grade. The HRQoL of the participants was compared to the US population norm data using minimally clinically important difference (MCID), the smallest score differences that are clinically relevant, of SF-6D=0.04,34 and PCS-12 and MCS-12=5 points.31 Backward stepwise ordinary least squares (OLS) regression was used to explore which components in the attitudes and academic help-seeking behavior domains were related to HRQoL using a cutoff point of p>0.2 to delete variables from the model. Independent variables in the OLS models included all the domains on attitudes and academic help-seeking behavior section and demographics (self-reported current GPA, age, gender, race/ethnicity) of participants. All significant levels were set at a p value of 0.05. To perform all analyses, Stata/SE, version 12.1, software was used (StataCorp LP, College Station, TX).
RESULTS
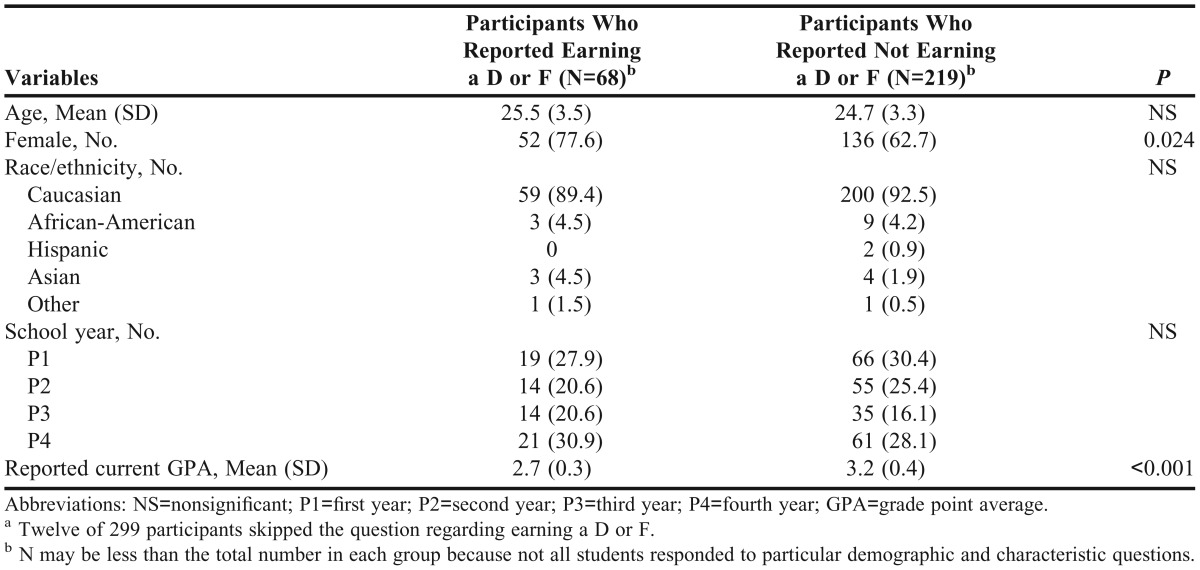
There were 304 (68.6%) students who participated in this study (mean age 25±3.4 years). Five of 304 survey instruments were omitted from the analyses because they were less than 50% complete. Most participants were Caucasian (92.4%) and female (64.5%). The overall self-reported current average GPA was 3.1±0.5 years About a quarter of participants (23.7%) reported earning at least 1 grade of D or F in the PharmD program.15 When dividing the participants according to whether they had received a D or F, a significant difference was observed in gender and GPA (Table 1). The proportion of female students in the group who had earned a D or F was higher than the group who did not (77.6% vs 62.7%; p=0.024). Participants who reported earning a D or F also reported having a significantly lower GPA (2.67±0.32) compared to that of students who did not (3.21±0.40; p<0.001).
Table 1.
Student Pharmacist Demographics and Characteristics Based on Self-Reported Earning at Least One D or F Grade During the Doctor of Pharmacy Program at a Public University (n=287)a
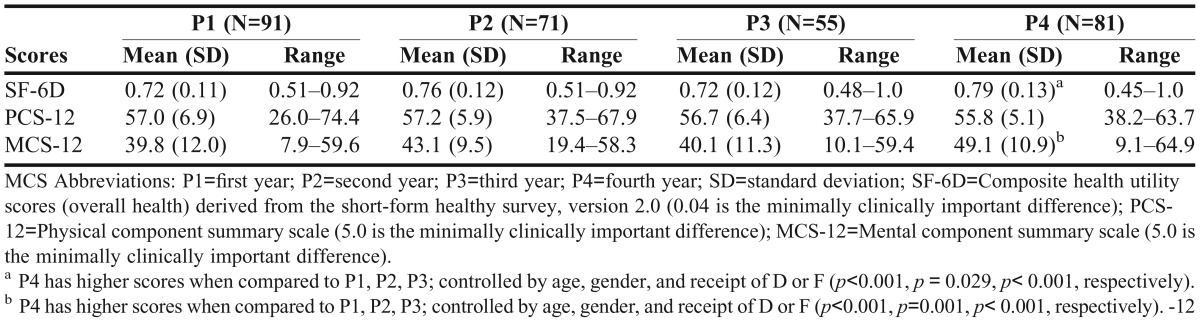
The SF-6D, PCS-12, and MCS-12 scores were calculated from the P1 through P4 students’ responses to the SF-12v2 health survey instrument (Table 2). Average SF-6D scores ranged from 0.71±0.11 for P3 students to 0.81±0.13 for P4 students. Average MCS-12 scores ranged from 40.1±11.3 for P3 students to 49.1±10.9 for P4 students. The average P4 students’ SF-6D and MCS-12 scores were significantly higher than the P1, P2, andP3 students’ average (p<0.05), after controlling for age, gender, and reported receipt of a D or F. No differences were detected in the average PCS-12 scores among the 4 pharmacy class years. When using the MCID of the SF-6D, PCS-12 and MCS-12, the P4 students had average SF-6D, PCS-12, and MCS-12 scores comparable to the US population norms. The MCS-12 scores of student pharmacists in the first 3 years of the program were significantly lower than those of the P4 students group (p<0.001, p=0.001, p<0.001, respectively). In addition, the P1, P2, and P3 students’ scores were more than 5 points lower than the US population norms, which exceeded the smallest score difference threshold for the MCID that is considered clinically relevant.31
Table 2.
Score Differences Derived From Short-Form Health Survey, Version 2.0, Responses by Student Pharmacists From 4 Class Years of a Doctor of Pharmacy Program
Among the 8 SF-12 subdomains (data not shown), the averages of general health and role emotional limitation scores of the P4 students were significantly higher than the average scores from the P1 and P3 students (p<0.05). Average vitality, social functioning, and mental health scores reported from P4 students were also significantly higher than those of P1, P2, and P3 students (p<0.05).
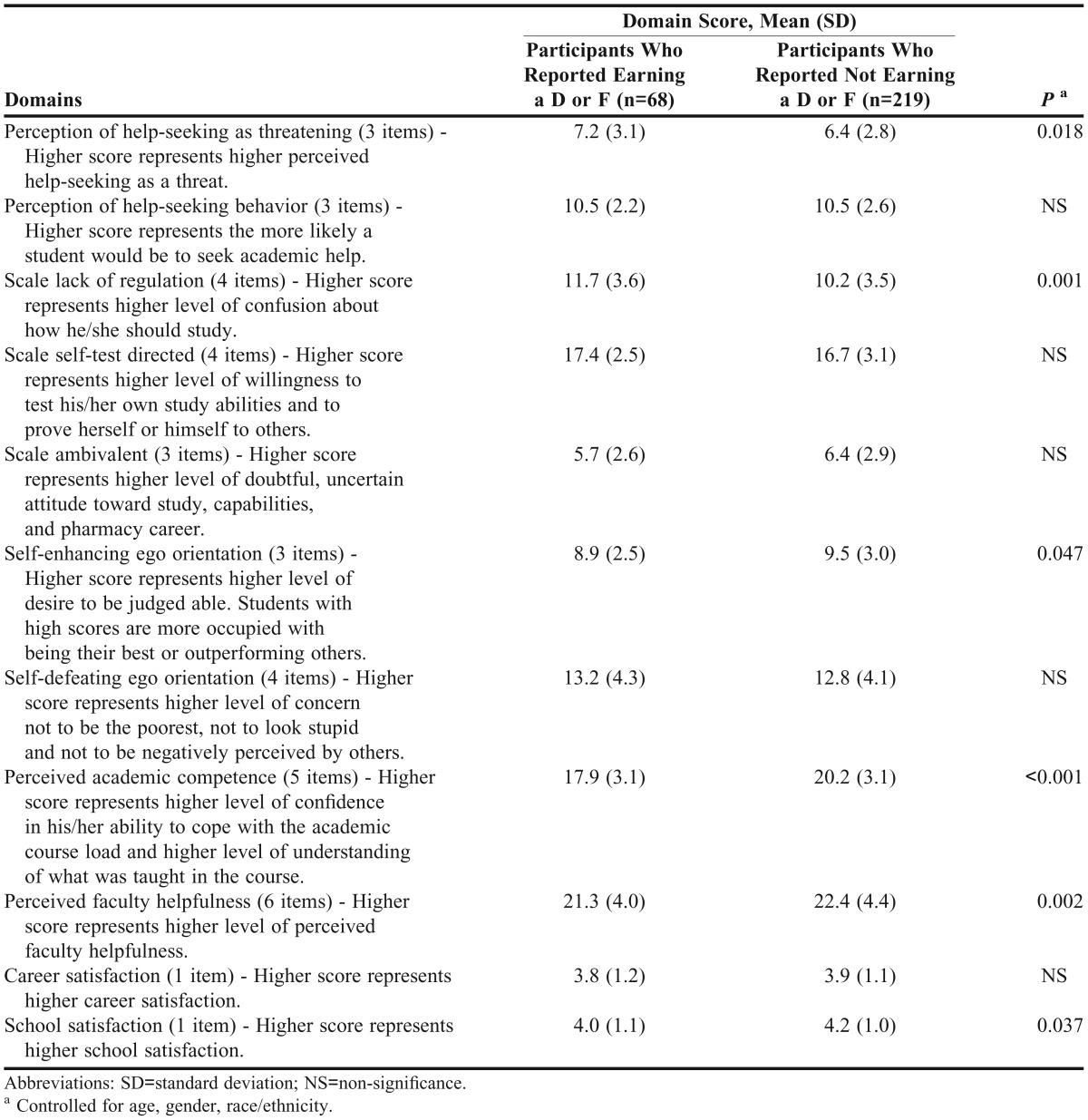
The summary scores of the attitudes and academic help-seeking behavior domains for the 2 subgroups (group that reported earning a D or F grade vs the group who did not) are presented in Table 3. Participants who reported earning a D or F had significantly higher scores on perception of help-seeking as threatening and scale of lack of regulation when compared to the participants who did not (p=0.018 and p=0.001, respectively). The participants who reported earning a D or F also reported significantly lower scores on self-enhancing ego orientation, perceived academic competence, and perceived faculty helpfulness (p=0.047, p<0.001, and p=0.002, respectively).
Table 3.
Survey Instrument Domain Summary Scores for the Group of Student Pharmacists Who Self-Reported Earning a D or F and the Group of Student Pharmacists Who Did Not
The regression analyses showed that only scale lack of regulation and self-defeating ego orientation were negatively associated with SF-6D (p=0.001 and p=0.001, respectively) and MCS-12 scores (p=0.004 and p=0.004, respectively). In contrast, only school satisfaction was positively associated with SF-6D scores (p=0.009) and MCS-12 scores (p=0.013). Self-enhancing ego orientation and career satisfaction showed significant positive associations with PCS-12 scores (p=0.046 and p=0.046, respectively).
DISCUSSION
Colleges and schools of pharmacy attract students who are high academic achievers. When these students fail to earn their PharmD degree, it represents untapped potential and low return on their investment,35 considering the average student loan debt incurred (∼$123,000 in 2012).36 To help student pharmacists succeed, institutions must provide an excellent learning environment and have methods to assess and modify underlying causes of ineffective learning experiences.37 Students’ HRQoL is an important factor that contributes to academic success.
This study examined student pharmacists’ HRQoL across all 4 academic years of the PharmD program. It also analyzed the relationships with attitudes and perception toward pharmacy education, perceived self-efficacy, ego orientation, and academic help-seeking behaviors among student pharmacists. The P4 students had average SF-6D, PCS-12, and MCS-12 scores comparable to the US population in the age range of 18-34 years old.30,33 On the contrary, the average mental component summary scores of student pharmacists in the first 3 years of the program were lower than those for the US population and P4 students. Low HRQoL in our college of pharmacy’s P1, P2, and P3 student pharmacists, especially the mental component, is consistent with the results reported in medical and nursing students at similar chronological points of 3 degree programs prior to graduation.1,38,39
Several studies have found that a high level of stress was associated with low mental health. Marshall and colleagues examined perceived stress, HRQoL, and factors related to stress and found that P3 students had higher levels of stress and lower MCS-12 scores when compared with the US population norms.3 In our study, the average PCS-12 and MCS-12 scores of P3 students (56.7 and 40.1, respectively) were comparable with their results (55.4 and 40.6, respectively). Hirsch and colleagues detected significant differences in HRQoL, perceived stress, and coping skills in the mental component among the 3 preclinical years of student pharmacists.2 In addition, students in the 3 preclinical years had lower MCS-12 scores than the US population norms. The average PCS-12 scores of P1 through P3 students in our study were not different from Hirsch and colleagues, but the average MCS-12 scores of P2 students in our study were higher than those of students in Hirsch’s study. Gupchup and colleagues reported that the average mental component score of P3 students was significantly lower than that of P1 students.6 The average PCS-12 scores of P1through P3 students in our study were higher than those reported in Gupchup’s study. The average MCS-12 scores of P2 students in our study were higher than those reported by Gupchup. These discrepancies of HRQoL results between our study and the literature may result from many factors, such as dissimilar academic environments, differences in the institutions’ PharmD curricula, and timing of survey instrument administration within the academic year.
Approximately one-fourth of students in our study reported that they had earned at least 1 grade of D or F during the PharmD degree program. The students who reported earning a D or F were more likely to perceive help-seeking behavior as a threat. They also reported more confusion regarding how they should study (scale lack of regulation), compared to students who reported not earning a D or F. In addition, they scored lower in their desire to be judged able (self-enhancing ego orientation) and their perceived academic competence domain than students who reported not earning a grade of D or F. In our previous study, academic competence positively influenced self-enhancing ego orientation and perceived faculty helpfulness.15 Therefore, students who reported earning a D or F may have a lower desire to be judged able (self-enhancing ego orientation) and may feel less positive towards faculty members (perceived faculty helpfulness). Because this was a cross-sectional study, we cannot conclude that earning D or F grades led to different perceptions. Research using a longitudinal design to explore these relationships is necessary to gain a fuller understanding and develop strategies to enhance student academic performance.
Students’ perceptions of how they should study (scale lack of regulation) and their self-defeating ego orientation were negatively related to their overall health (SF-6D) and mental health (MCS-12). A high level of school satisfaction was associated with increased HRQoL of student pharmacists. Individuals’ concepts of ability affect thought processes and performance through the self-efficacy mechanism.18,40 For example, the higher students perceive their ability to manage their studies, the better they use their cognitive capabilities. In contrast, a low sense of self-efficacy relates to depression and anxiety which lead to poor mental component summary scale scores for HRQoL.16 Our study facilitates the understanding of how attitudes and perceptions toward pharmacy education are associated with the HRQoL of student pharmacists. Our study also provides information for colleges and schools of pharmacy to identify potential interventions and strategies to improve the HRQoL of students and their academic success. Using the attitudes and academic help-seeking behavior survey instrument to determine student level of self-efficacy may be useful in helping students make positive changes. In addition, supporting students in maintaining good mental and overall health and modeling successful achievement by their peers may improve students’ self-efficacy.16
Although we carefully examined the associations between different factors and the HRQoL of student pharmacists, our study had some limitations. This study was conducted at only 1 public college of pharmacy in the southern United States, which may somewhat limit its generalizability to other colleges and schools of pharmacy. Additionally, because this study was strictly voluntary and anonymous, we do not know the accuracy of students’ self-reported grades. However, the participants had little motivation to answer dishonestly. The study was a cross-sectional survey and, therefore, a causality of low HRQoL among pharmacy students cannot be concluded. Longitudinal research that includes a baseline at admission with periodic assessment over the course of the program concluding at or near graduation is worth pursuing in future studies.
CONCLUSION
Confusion regarding how to study, ego orientation, and level of satisfaction towards a chosen college or school of pharmacy and a career in pharmacy are factors associated with HRQoL of student pharmacists. The HRQoL scores of our P1 through P3 student pharmacists at our institution were lower than those of P4 students and the US population. This could reflect stress associated with heavy academic course loads, student loan debt, or other personal or health-related factors. However, this study does not establish causal associations and longitudinal research on the HRQoL of student pharmacists throughout pharmacy programs is needed. Support programs such as stress management and hotlines for mental health consultation may be helpful for students to maintain or improve their mental and overall health. Group study sessions or a tutor program should include guidance on effective studying.
ACKNOWLEDGEMENT
We would like to thank the University of Arkansas for Medical Sciences College of Pharmacy, Department of Pharmacy Practice for funding support for this research project. We also thank our students for completing the survey instrument. We thank Dr. Jan Vermunt for permission to adapt items from the Inventory of Learning Styles questionnaire.41
REFERENCES
- 1.Paro HB, Morales NM, Silva CH, et al. Health-related quality of life of medical students. Med Educ. 2010;44(3):227–235. doi: 10.1111/j.1365-2923.2009.03587.x. [DOI] [PubMed] [Google Scholar]
- 2.Hirsch JD, Do AH, Hollenbach KA, Manoguerra AS, Adler DS. Students' health-related quality of life across the preclinical pharmacy curriculum. Am J Pharm Educ. 2009;73(8):Article 147. doi: 10.5688/aj7308147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Marshall LL, Allison A, Nykamp D, Lanke S. Perceived stress and quality of life among doctor of pharmacy students. Am J Pharm Educ. 2008;72(6):Article 137. doi: 10.5688/aj7206137. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Pau A, Rowland ML, Naidoo S, et al. Emotional intelligence and perceived stress in dental undergraduates: a multinational survey. J Dent Educ. 2007;71(2):197–204. [PubMed] [Google Scholar]
- 5.Beck DL, Hackett MB, Srivastava R, McKim E, Rockwell B. Perceived level and sources of stress in university professional schools. J Nurs Educ. 1997;36(4):180–186. doi: 10.3928/0148-4834-19970401-08. [DOI] [PubMed] [Google Scholar]
- 6.Gupchup G, Borrego M, Konduri N. The impact of student life stress on health related quality of life among doctor of pharmacy students. Coll Stud J. 2004;38(2):292–301. [Google Scholar]
- 7.Sansgiry SS, Sail K. Effect of students' perceptions of course load on test anxiety. Am J Pharm Educ. 2006;70(2):Article 26. doi: 10.5688/aj700226. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Henning K, Ey S, Shaw D. Perfectionism, the impostor phenomenon and psychological adjustment in medical, dental, nursing and pharmacy students. Med Educ. 1998;32(5):456–464. doi: 10.1046/j.1365-2923.1998.00234.x. [DOI] [PubMed] [Google Scholar]
- 9.Beck DL, Hackett MB, Srivastava R, McKim E, Rockwell B. Perceived level and sources of stress in university professional schools. J Nurs Educ. 1997;36(4):180–186. doi: 10.3928/0148-4834-19970401-08. [DOI] [PubMed] [Google Scholar]
- 10.Sansgiry SS, Bhosle M, Sail K. Factors that affect academic performance among pharmacy students. Am J Pharm Educ. 2006;70(5):Article 104. doi: 10.5688/aj7005104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Watson R, Deary I, Thompson D, Li G. A study of stress and burnout in nursing students in Hong Kong: a questionnaire survey. Int J Nurs Stud. 2008;45(10):1534–1542. doi: 10.1016/j.ijnurstu.2007.11.003. [DOI] [PubMed] [Google Scholar]
- 12.Dyrbye LN, Thomas MR, Shanafelt TD. Systematic review of depression, anxiety, and other indicators of psychological distress among U.S. and Canadian medical students. Acad Med. 2006;81(4):354–373. doi: 10.1097/00001888-200604000-00009. [DOI] [PubMed] [Google Scholar]
- 13.Henning M, Krageloh C, Hawken S, Zhao Y, Doherty I. Quality of life and motivation to learn: a study of meidcal students. Issues Educ Res. 2010;20(3):244–256. [Google Scholar]
- 14.Eisenberg D, Golberstein E, Gollust SE. Help-seeking and access to mental health care in a university student population. Med Care. 2007;45(7):594–601. doi: 10.1097/MLR.0b013e31803bb4c1. [DOI] [PubMed] [Google Scholar]
- 15.Payakachat N, Gubbins PO, Ragland D, et al. Academic help-seeking behavior among student pharmacists. Am J Pharm Educ. 2013;77(1):Article 7. doi: 10.5688/ajpe7717. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bandura A. Perceived self-efficacy in cognitive development and functioning. Educ Psychol. 1993;28(2):117–148. [Google Scholar]
- 17.Bandura A. The explanantory and predictive scope of self-efficacy theory. J Soc Clin Psychol. 1986;4(3):359–373. [Google Scholar]
- 18.Wood R, Bandura A. Impact of conceptions of ability on self-regulatory mechanisms and complex decision making. J Pers Soc Psychol. 1989;56(3):407–415. doi: 10.1037//0022-3514.56.3.407. [DOI] [PubMed] [Google Scholar]
- 19.Khan F, Pallant J, Brand C. Caregiver strain and factors associated with caregiver self-efficacy and quality of life in a community cohort with multiple sclerosis. Disabil Rehabil. 2007;29(16):1241–1250. doi: 10.1080/01443610600964141. [DOI] [PubMed] [Google Scholar]
- 20.Weng LC, Dai YT, Huang HL, Chiang YJ. Self-efficacy, self-care behaviours and quality of life of kidney transplant recipients. J Adv Nurs. 2010;66(4):828–838. doi: 10.1111/j.1365-2648.2009.05243.x. [DOI] [PubMed] [Google Scholar]
- 21.Robinson-Smith G, Johnston MV, Allen J. Self-care self-efficacy, quality of life, and depression after stroke. Arch Phys Med Rehabil. 2000;81(4):460–464. doi: 10.1053/mr.2000.3863. [DOI] [PubMed] [Google Scholar]
- 22.Wu HK, Chau JP, Twinn S. Self-efficacy and quality of life among stoma patients in Hong Kong. Cancer Nurs. 2007;30(3):186–193. doi: 10.1097/01.NCC.0000270704.34296.86. [DOI] [PubMed] [Google Scholar]
- 23.Sherina MS, Rampal L, Kaneson N. Psychological stress among undergraduate medical students. Med J Malaysia. 2004;59(2):207–211. [PubMed] [Google Scholar]
- 24.Joekes K, Van ET, Schreurs K. Self-efficacy and overprotection are related to quality of life, psychological well-being and self-management in cardiac patients. J Health Psychol. 2007;12(1):4–16. doi: 10.1177/1359105306069096. [DOI] [PubMed] [Google Scholar]
- 25.Elliot A, Church M. A hierarchical model of approach and avoidance achievement motivation. J Pers Soc Psychol. 1997;72(1):218–232. doi: 10.1037//0022-3514.76.4.628. [DOI] [PubMed] [Google Scholar]
- 26.Nicholls J. Conceptions of ability and achievement motivation: a theory and its implications for education. In: Paris S, Olsen GM, Stevenson H, editors. Learning and Motivation in the Classroom. Hillsdale, NJ: Lawrence Erlbaum Association; 1983. pp. 211–237. [Google Scholar]
- 27.Skaalvik EM. Self-enhancing and self-defeating ego orientation: relations with task and avoidance orientation, achievement, self-perceptions, and anxiety. J Educ Psychol. 1997;89(1):71–81. [Google Scholar]
- 28.Ware JE, Kosinski M, Keller SD. A 12-item short form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34:220–233. doi: 10.1097/00005650-199603000-00003. [DOI] [PubMed] [Google Scholar]
- 29.Cheak-Zamora N, Wyrwich K, McBride T. Reliability and validity of the SF-12v2 in the medical expenditure panel survey. Qual Life Res. 2009;18(6):727–735. doi: 10.1007/s11136-009-9483-1. [DOI] [PubMed] [Google Scholar]
- 30.Ware J. U.S population norms. http://www.sf-36.org/research/sf98norms.pdf. Accessed April 12, 2013.
- 31.Ware JE, Kolinski M, Keller SD. How to score the SF-12 Physical and mental health summaries: a user's manual. Boston, MA: The Health Institute, New England Medical Centre; 1995. [Google Scholar]
- 32.Brazier JE, Roberts J. The estimation of a preference-based measure of health from the SF-12. Med Care. 2004;42(9):851–859. doi: 10.1097/01.mlr.0000135827.18610.0d. [DOI] [PubMed] [Google Scholar]
- 33.Fryback DG, Dunham NC, Palta M, et al. US norms for six generic health-related quality-of-life indexes from the National Health Measurement study. Med Care. 2007;45(12):1162–1170. doi: 10.1097/MLR.0b013e31814848f1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Walters SJ, Brazier JE. Comparison of the minimally important difference for two health state utility measures: EQ-5D and SF-6D. Qual Life Res. 2005;14(16):1523–1532. doi: 10.1007/s11136-004-7713-0. [DOI] [PubMed] [Google Scholar]
- 35.Jaeger D, Page M. Degrees matter: New evidence on sheepskin effects in the returns to education. Rev Econ Stat. 1996;78(4):733–740. [Google Scholar]
- 36.Brown DL. A looming joblessness crisis for new pharmacy graduates and the implication it holds for the academy. Am J Pharm Educ. 2013;77(5) doi: 10.5688/ajpe77590. Article 90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Accreditation Council for Pharmacy Education. Accreditation standards and guidelines for the professional program in pharmacy leading to the doctor of pharmacy degree. Guideline 2.0. https://www.acpe-accredit.org/pdf/S2007Guidelines2.0_ChangesIdentifiedInRed.pdf. Accessed August 24, 2011.
- 38.Voltmer E, Rosta J, Aasland OG, Spahn C. Study-related health and behavior patterns of medical students: a longitudinal study. Med Teach. 2010;32(10):e422–e428. doi: 10.3109/0142159X.2010.496008. [DOI] [PubMed] [Google Scholar]
- 39.Souza IMDM, Paro HBMD, Morales RR, Pinto RDC, da Silva CHM. Health-related quality of life and depressive symptoms in undergraduate nursing students. Rev Lat Am Enfermagem. 2012;20(4):736–743. doi: 10.1590/s0104-11692012000400014. [DOI] [PubMed] [Google Scholar]
- 40.Zajacova A, Lynch S, Espenshade T. Self-efficacy, stress, and academic success in college. Res High Educ. 2005;46(6):677–706. [Google Scholar]
- 41.Vermunt JD. Relations between student learning patterns and personal and contextual factors and academic performance. High Educ. 2005;49(3):205–234. [Google Scholar]