

Abstract
An important etiopathogenic component of cardiovascular disease is atherosclerosis, with inflammation being an essential event in the pathophysiology of all clinical pictures it comprises. In recent years, several molecules implicated in this process have been studied in order to assess cardiovascular risk in both primary and secondary prevention. C-reactive protein is a plasmatic protein of the pentraxin family and an acute phase reactant, very useful as a general inflammation marker. Currently, it is one of the most profoundly researched molecules in the cardiovascular field, yet its clinical applicability regarding cardiovascular risk remains an object of discussion, considered by some as a simple marker and by others as a true risk factor. In this sense, numerous studies propose its utilization as a predictor of cardiovascular risk through the use of high-sensitivity quantification methods for the detection of values <1 mg/L, following strict international guidelines. Increasing interest in these clinical findings has led to the creation of modified score systems including C-reactive protein concentrations, in order to enhance risk scores commonly used in clinical practice and offer improved care to patients with cardiovascular disease, which remains the first cause of mortality at the worldwide, national, and regional scenarios.
1. Introduction
Owing to profound research and identification of the etiopathogenic basis of cardiovascular disease (CVD), as well as the diverse mechanisms implicated in the onset and progression of atherosclerosis [1], current studies in this area focus in the characterization of biomarkers for the early detection of the inflammatory activation underlying this process. In turn, this has improved methods for the estimation of cardiovascular risk (CVR), atherosclerotic plaque rupture, and even subsequent ischemic events [2], by establishing revised initial management measures based on the newfound greater knowledge on this group of ailments. Likewise, these molecules may complement the predictive ability of many classic CVD risk factors and serve as valuable prognostic information for several associated adverse effects [3, 4].
The biomolecule with the greater body of research both from a molecular and epidemiological perspective is C-reactive protein (CRP), a plasma protein of the pentraxin family and an acute phase reactant, which displays high sensitivity as a general inflammation marker [5]. Numerous studies have demonstrated the active participation of this molecule in the atherogenic process [6], and due to the discovery of high-sensitivity techniques for its determination, its stable plasmatic concentrations, and its relatively low costs, it may be of great use in the identification of patients at high risk, as a prognostic indicator and even as a therapeutic target in large populations [7].
Studies surrounding this molecule started over a decade ago, statistically associating the onset of coronary events, such as myocardial infarction (MI) and angor pectoris, with elevated serum levels of this protein [8]. From this point, experimental and epidemiological research [9, 10] has aimed at the elucidation of the true effect and predictive power of CRP in CVD, for both primary and secondary prevention, as an element to consider in equations for the calculation of absolute CVR in specific populations and as a parameter to be evaluated in all patients with an acute coronary event and patients undergoing therapeutic procedures in this field [11].
In this scenario, it is necessary to consider the diverse perspectives outlined worldwide and assess opinions for and against this controversial protein, in order to ultimately analyze the inclusion of its routine determination as part of the diagnostic work-up in patients with CVD in our population.
2. Cardiovascular Risk: Current Tendencies
According to the Framingham Heart Study, CVD comprises a broad spectrum of pathologies including coronary disease (MI, coronary insufficiency, and angor pectoris), cerebrovascular disease (ischemic ictus, hemorrhagic ictus, and transient ischemic events), peripheral artery disease (intermittent claudication), and heart failure (HF) [12–14]. For the clinical-epidemiological assessment of CVD, several studies [15, 16] have proposed the implementation of concepts such as absolute cardiovascular risk (aCVR), also known as global or total risk, which represents the probability of developing one of these disorders in a given period of time [17], and relative cardiovascular risk (rCVR), which accounts for the probability of developing a cardiovascular event in subjects with certain risk factors compared with individuals of the same age and gender without such factors [12].
The first great-scale epidemiologic study for the determination of the main causes of CVD was the Framingham Heart Study [18]. The algorithms resulting from this research have been validated and widely utilized in clinical practice for the estimation of aCVR in various populations worldwide [12], since they allow for risk stratification. These equations are based in cardiovascular risk factors (CRF) such as hypertension (HT), diabetes mellitus (DM), and dyslipidemia, among others. Nevertheless, results obtained from the application of these equations are not applicable in certain demographies, such as Spain, Italy, China, and Chile [19–21], where the risk of developing CVD is relatively low.
Indeed, although scoring systems for the estimation of aCVR are important tools, they display several limitations: modifications in long-standing population-specific patterns of disease onset—upon which CVR is estimated—may distort their clinical application. Moreover, most of these algorithms do not evaluate CVD in a global manner, but they are formulated to predict specific isolated components of it, especially coronary disease (CD) [17, 22–25], in opposition to the multifactorial concept of the etiology to which these equations for estimated aCVR are geared for [12, 18].
3. Cardiovascular Risk Factors: Classic versus Novel (Table 1)
Table 1.
Risk factors for cardiovascular disease.
| Classic factors (reference) | Novel factors (reference) |
|---|---|
| (i) Age [26] | (i) C-reactive protein [27] |
| (ii) Family history [28] | (ii) Lipoprotein[a] [29] |
| (iii) Race [30] | (iii) Pentraxin 3 [31] |
| (iv) Arterial hypertension [32] | (iv) Leukocytes CD31+ [33] |
| (v) Diabetes mellitus [34] | (v) Homocysteine [35] |
| (vi) Smoking [36] | (vi) Fibrinogen [37] |
| (vii) Dyslipidemia [38] | (vii) Adiponectin [39] |
| (viii) Obesity [40] | (viii) Alcohol [41] |
| (ix) Sedentary lifestyle [42] |
A risk factor is a measurable element or characteristic that shares a causal relationship with an increment in the onset frequency of a given disease, constituting a significant independent predictive component for the risk of the developing this condition [18]. CRF have been described since the 1930s, reaching widespread notoriety in 1948 with the initiation of the Framingham Heart Study, which years later would define what are nowadays considered classic risk factors, in consonance and corroboration with other great epidemiologic studies [43, 44].
The most common classification of CRF labels them as either modifiable or nonmodifiable. Nonmodifiable CRF include age (men >45 years and women >55 years or menopausal), race (black), gender (male), and genetics (family history of CVD), while modifiable CRF cover obesity, HT, dyslipidemia, smoking, DM, and a sedentary lifestyle [22].
Throughout the years, interest has focused on the improvement of CVR assessment, given the rising incidence of CVD. This has led to the realization of numerous multidisciplinary studies linking the origin and evolution of CVD with new biochemical markers. These biomarkers have displayed an important predictive ability for the onset of cardiovascular events, as they have been shown to be closely related to the pathophysiological mechanisms of these diseases, with both local and systemic implications [45, 46]. Each of these molecules exhibits distinct biochemical features, including factors associated with low-grade inflammation (CRP, vascular adhesion molecules, interleukins, pentraxins, leukocytes, etc.) [31, 33, 47–49], components of the lipid profile (lipoprotein[a], apolipoproteins, triacylglycerides, etc.) [29, 50, 51], and elements linked to prothrombotic states (fibrinogen, homocysteine, D-dimer, etc.) [35, 37, 52].
From this diverse assortment of candidates, CRP appears to be the most profoundly studied regarding inflammation in the cardiovascular field [53]. Not only has CRP been associated with the chain of events occurring at the endothelium within the atherosclerotic process [54, 55], but it has also been linked with a direct, independent association with future cardiovascular events in several great-scale epidemiologic reports [27, 56, 57], as well as with other disorders of metabolic origin, both in adult and pediatric populations [58, 59].
4. Clinical Applicability of C-Reactive Protein in Risk Assessment
4.1. C-Reactive Protein as a Cardiovascular Risk Factor
Kroop and Shackman [60] were the first to report alterations of CRP levels in patients with MI. Three years later, Gurevin and Kozonis [61] proposed this protein as a reflection of the natural history of this disorder, but it was only in the mid-1990s that research by Ridker et al. [62] suggested this molecule to acquire greater relevance within the group of novel risk factors, after closely linking it not only with MI but also with cerebrovascular events.
Currently, it is well known that CRP levels may rise due to a several processes of inflammatory etiology (Table 2). This lack of specificity may concern many physicians when assessing CRP in the clinical scenario. However, methods for the quantitative determination of this acute phase reactant have reached detection thresholds lower than 1 mg/L [63], with a mean serum concentration of 0.8 mg/L in young adults with no underlying inflammatory processes [5]. These newer quantification techniques have been dubbed “high-sensitivity” and are essential for the consideration of this protein as a CRF. Initially, high-sensitivity quantification methods were based on ELISA, utilized in several population studies despite its cumbersome routine use in clinical laboratories [64]. As a consequence, more accessible methods, such as immunonephelometric techniques [65] and, more recently, automatized immunoluminometry and immunoturbidimetry, have been implemented, improving the sensitivity of the quantification even in cases of very low concentrations [66]. Additionally, these are inexpensive techniques, an important aspect regarding its routine use in clinical practice [63].
Table 2.
C-Reactive Protein in certain pathologies.
| Acute phase response with high CRP release | |
|---|---|
| Infection | Bacteria, mycobacteria, viruses, and fungi |
| Postinfectious allergic complications | Rheumatoid arthritis and erythema nodosum |
| Inflammatory diseases | Crohn's disease, psoriatic arthritis, systemic vasculitis, and Reiter's disease |
| Necrosis | Myocardial infarction and acute pancreatitis |
| Trauma | Surgeries, fractures, and burns |
|
| |
| Acute phase response with low CRP release | |
|
| |
| Systemic lupus erythematosus, scleroderma, ulcerative colitis, and dermatomyositis | |
In light of these advantages and findings from several epidemiological studies, the Center for Disease Control and Prevention (CDC) and American Heart Association (AHA) established in 2003 the first guidelines for the interpretation of markers of CVR, with special emphasis on the use of CRP in primary prevention. In addition, the distribution of CRP serum concentrations in tertiles was presented: first tertile: <1 mg/L, second tertile: 1–3 mg/L, and third tertile: >3 mg/L. This model is widely accepted in clinical practice given that, after adjustment for other CRF, subjects with CRP levels between 1 and 3 mg/L had a 50% greater CVR than those with concentrations <1 mg/L. Likewise, individuals with levels >3 mg/L had a CVR approximately twice as high as those with values <1 mg/L. With this outline, the CDC designated subjects within the first tertile as low risk, those in the second tertile as average risk, and those in the third tertile as high risk of developing CVD [67, 68]. The utilization of CRP in the assessment of patients with CVD must be accompanied by a detailed clinical record and an adequate interpretation in order to avoid false positives. Measurement of CRP should be omitted if infection is suspected, or if there is history of a traumatic event within the previous 2 weeks. If concentrations >10 mg/L are obtained, the measurement should be repeated, and 2 subsequent determinations should be realized with an interval of 1 month, selecting the lowest value returned for the assessment of CVR [63, 68, 69]. Figure 1 displays the recommended scheme for the interpretation of CRP levels for CVR stratification.
Figure 1.
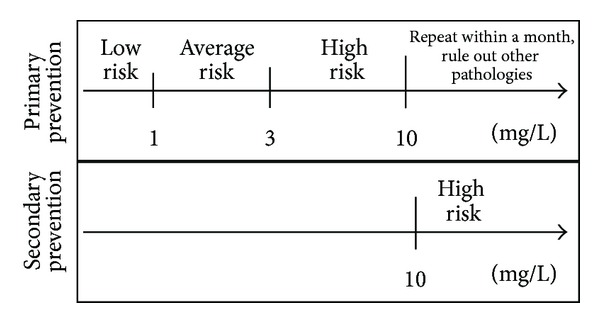
Use of high-sensitivity CRP levels for the stratification of cardiovascular risk (primary prevention) and as a prognostic factor in acute coronary syndrome (secondary prevention) [69, 70].
CRP cut-off values have been proposed for the evaluation of patients in 3 distinct clinical conditions: apparently healthy subjects, stable patients with CVR or diagnosed CVD, and patients with acute coronary syndrome (ACS) [2]. Nonetheless, the first scenario is particularly important, considering that the estimation of aCVR is pivotal for the initiation of preventive and therapeutic management. For example, individuals with a high risk as estimated by the equations from the Framingham Heart Study (entailing >20% risk of developing CD in 10 years) are indicated to receive intensive medical intervention and/or pharmacologic therapeutic management. The latest guidelines published by the National Academy of Clinical Biochemistry (NACB) recommend the quantification of CRP in patients with moderate risk (10–20% risk of developing CD in 10 years by the Framingham classification) and in patients that raise doubts regarding their management. These criteria allow for the evaluation of the application of intensive therapeutic measures including both lifestyle modifications and pharmacotherapy, with the quantification of CRP in primary attention being classified as a Class Ia indication [68, 70].
The importance of CRP assessment prompted Ridker et al. [74] to develop, validate, and demonstrate a project named the “Reynolds Risk Score,” a high-precision predictive model for CVR in 10 years, initially created for women and later for men [75], which included the use of high-sensitivity CRP and family history of CD within its clinical algorithm, along with traditional risk factors: age, blood pressure, smoking, total cholesterol, and HDL-C concentration, allowing for the reclassification of women and men in distinct CVR categories. A meta-analysis of over 50 studies realized by Kaptoge et al. [76] revealed CRP concentrations to have a strong association with mortality of vascular origin, as well as with risk of CD and ischemic ictus. Nevertheless, this association with ischemic vascular disease may depend fundamentally on conventional risk factors.
4.2. C-Reactive Protein in Acute Coronary Events
Similar to recommendations with respect to primary prevention, the AHA and CDC suggest the determination of high-sensitivity CRP serum concentrations in patients with SCA, with a cut-off of >10 mg/L as a predictive factor of subsequent acute events [68, 69]. Indeed, these standard have been recently ratified by several clinical guidelines and population studies [70, 78]. Figure 1 shows the CRP cut-off values used in both primary and secondary prevention.
Indeed, research has covered the analysis of SCA patients both with and without ST segment elevation [79, 80], with the fundamental objective of identifying subjects at high risk for recurrence of these events and death [81]. On the other hand, its utilization has also been suggested as a prognostic marker in mid- and long-term after an acute event, independently of other markers such as troponins and B-type natriuretic peptide. In this sense, the joint analysis of Troponin-CRP is a very useful assessment method given the additive behavior of both biomarkers [82]. This practice would enhance the identification of patients with a high-risk prognosis and the necessity of intervention or “aggressive” monitoring [67]. Nonetheless, efforts are still directed to irrefutably demonstrate that this molecule improves risk estimation in all patients [83].
Therefore, novel research, such as that proposed by Schiele et al. [86], aims to determine the predictive value of the “Global Registry of Acute Coronary Events” (GRACE), a clinical scale designed for the estimation of mortality risk or HF risk in patients with SCA, with the inclusion of CRP serum concentrations in the model. Results have demonstrated that the addition of this molecule improves the classification of these patients in distinct risk categories [86]. Tables 3 and 4 summarize studies analyzing CRP for both primary and secondary prevention.
Table 3.
Studies on cardiovascular risk assessment utilizing C-reactive protein.
| Author (reference) | Sample | Results |
|---|---|---|
| Ridker et al. [62] | 543 apparently healthy men | Serum CRP levels predict MI and CVD: The quartile with the highest CRP levels had a greater risk of MI (RR: 2.9; P < 0.001) and CVD (RR: 1.9; P < 0.02) than the lowest quartile. |
|
| ||
| Ridker et al. [71] | 366 apparently healthy women (122 developed a cardiovascular event) | Serum CRP levels of patients who had a cardiovascular event were higher than control patients (P = 0.0001). Patients with the highest levels had a greater risk of developing MI or CVD (RR: 7.3; P = 0.0001). |
|
| ||
| Ridker et al. [72] | 27939 apparently healthy women | CRP is a more powerful predictor of cardiovascular events than LDL-C. The RR for a first cardiovascular event was, according to CRP quintiles: 1.4–1.6–2.0–2.3 (P < 0.001). |
|
| ||
| Cesari et al. [73] | 2225 participants aged 70–79 years without previously diagnosed cardiovascular disease | Inflammatory markers are predictors of cardiovascular events in elderly patients. CRP was associated with CHF (RR: 1.48; IC: 1.23–1.78). |
|
| ||
| Ridker et al. [74] | 24558 initially healthy women (≥45 years of age) | 2 new algorithms were developed for the calculation of global cardiovascular risk, reclassifying a great part of women with average risk according to conventional scoring systems. |
| Ridker et al. [75] | 10724 initially healthy women (≥50 years of age) | A new prediction model was developed for the calculation of global cardiovascular risk, including CRP and family history of cardiovascular events. Over 20.2% of the population was reclassified from the original distribution of conventional scoring systems. |
|
| ||
| Kaptoge et al. [76] | 160309 subjects without history of vascular disease (54 prospective studies) | The association of CRP with vascular disease depends on other inflammatory markers and classic risk factors. After multiple adjustments, the RR for coronary disease was (1.23; IC: 1.07–1.42), for CVD (1.32; IC: 1.18–1.49), and for vascular cause mortality (1.34; IC: 1.18–1.52). |
|
| ||
| Maiorana et al. [77] | 37 patients with 3 or more cardiovascular risk factors | 10 patients had LDL-C >100 mg/dL, fibrinogen >350 mg/dL, and CRP >2.6 mg/L; 6 of these patients presented a positive ischemia by exercise testing and coronary disease. |
CRP: C-reactive protein; MI: myocardial infarction; CVD: cerebrovascular disease; RR: relative risk; LDL-C: low-density lipoproteins; CHF: congestive heart failure; CI: confidence interval.
Table 4.
Studies on acute coronary syndrome prognosis utilizing C-reactive protein.
| Author (reference) | Sample | Results |
|---|---|---|
| Pietila et al. [84] | 188 patients with MI | Serum CRP levels in patients with MI predict mortality up to 6 months after the event. Highest levels were found between the 2nd and 4th days after infarction, the highest mean concentration being 65 mg/L; IC: 58–71 in patients who survived 24 months. |
|
| ||
| Gussekloo et al. [85] | 245 patients (80 deceased due to CVD after 5-year follow-up) | CRP is a powerful yet unspecific risk factor for CVD in the elderly. Serum CRP levels of those who died due to CVD were twice as high than those of control subjects (5.7 mg/L versus 2.7 mg/L; P < 0.005). |
|
| ||
| Mueller et al. [79] | 1042 ACS patients without ST segment elevation | CRP is an independent predictor of mortality short- and long-term in ACS patients without ST segment elevation who received early invasive treatment. In-hospital mortality was 1.2% in patients with (<3 mg/L), 0.8% (1–3 mg/L), and 3.7% (>10 mg/L), with RR = 4.2 for mortality. |
|
| ||
| Morrow et al. [78] | 3813 ACS patients | After multiple adjustments, patients with serum CRP levels 1–3 mg/L had a greater mortality risk (HR: 2.3; IC: 1.2–4.6) in comparison with those with levels <1 mg/L. The mortality risk for patients >3 mg/L was even higher (HR: 3.7; IC: 1.9–7.2). |
|
| ||
| Schiele et al. [86] | 1901 ACS patients | CRP is modest yet independent predictor of mortality within the first month after ACS. Subjects with levels >22 mg/L (4th quartile) had 4 times greater mortality risk within 30 days. |
|
| ||
| Caixeta et al. [80] | 2974 ACS patients | Patients with the highest serum CRP levels (4th quartile) presented a greater mortality risk within 30 days in comparison to the 1st quartile (2.3 versus 1.3%; P = 0.0004), as well as within a year after the event (5.5 versus 2.8%; P = 0.0003). |
CRP: C-reactive protein; MI: myocardial infarction; CI: confidence interval; CVD: cerebrovascular disease; ACS: acute coronary syndrome; RR: relative risk; HR: hazard ratios.
5. Is CRP a Risk Marker or a Risk Factor?
According to official definition of the United States National Institute of Health (NIH), a biomarker is “a characteristic that is objectively measured and evaluated as an indicator of normal biological processes, pathogenic processes, or pharmacologic responses to a therapeutic intervention” [87]. The association with any given disease may be exclusively statistical and it does not require an established causal relationship. Meanwhile, a risk factor is associated with a given pathology due to its participation in the etiopathogenic mechanisms triggered by itself [88] (Figure 2).
Figure 2.

Models used to ascertain the role of an inflammatory marker.
Regarding CRP, a controversial worldwide debate persists over its participation in CVD. Several retrospective and prospective studies, as well as meta-analyses, have described an association with MI [71, 72, 84, 89, 90], coronary insufficiency [4, 73, 91], cerebrovascular disease [85], and peripheral artery disease [92], behaving as an important mortality predictor [69]. As such, a large portion of scientific opinion supports CRP as a risk marker, in response to the inflammatory process within the atherosclerotic plaque and other previously established CRF [88]. Conversely, its role as a CRF is heavily debated [77, 93, 94]. Despite the large body of evidence associating CRP with atherosclerotic lesions, the lack of a direct correlation between its concentration and the extension of atherosclerosis as determined by imaging techniques constitutes one of the main arguments for those who oppose this much-disputed mechanism [88], along with its well-known associations with other risk factors included in the Framingham equations [95]. However, we consider there is sufficient evidence that shows an intimate association between this molecule and cardiovascular events, both at a clinical and molecular level, granting its consideration not only as a biomarker, but also as a true risk factor [96].
Likewise, various reports have demonstrated that initiation of pharmacologic treatment prompted by elevated CRP levels may lower the onset of coronary events both in primary and secondary prevention, as suggested by the AirForce/Texas Coronary Atherosclerosis Prevention Study (AFCAPS/TexCAPS), wherein the administration of lovastatin reduced the frequency of coronary events in patients under primary prevention with low/normal LDL-C levels and high CRP concentrations [97]. Similarly, secondary prevention studies such as the Reversal of Atherosclerosis with Aggressive Lipid Lowering (REVERSAL) study show the use of higher statin doses (Atorvastatin 80 mg versus Pravastatin 40 mg) to significantly lower both LDL-C and CRP levels after 18 months of therapy. Amelioration of atherosclerotic progression was also found as assessed by intravascular ultrasound, with a significant independent correlation between decreased CRP and atherosclerotic progression [98]. These results, in addition to others such as the JUPITER study [99], demonstrate the usefulness of CRP for the identification of subjects in risk, and they also hint towards its potential role as a therapeutic target in the atherosclerotic process [100]. Therefore, future research should continue to more thoroughly study the effects of the reduction of serum CRP levels.
6. Conclusions
Given the ever-increasing problematic that CVD represents nowadays worldwide, it is necessary to exhaustively evaluate all subjects who may develop them. This possibility may be measured or quantified through scoring systems created based on the Framingham Heart Study, which allows for the calculation of absolute risk of developing a cardiovascular event based on risk factors inherent to each studied individual. Traditional risk factors are proved predictive elements for the development of disease that share a causal relationship with it. In the case of CVD, these include age, gender, obesity, HT, dyslipidemia, smoking, DM, and a sedentary lifestyle, among others.
The designation of new risk factors stemming from advances in the comprehension of the inflammatory physiopathology of CVD has led research to try and elucidate which of these novel and emergent elements display all required criteria to be considered true risk factors, and which have solely exhibited a casual statistical association. C-reactive protein is one of the numerous molecules that fit this description, but its properties and features have led it to become one of the main targets for researchers worldwide. Its utilization in the clinical setting is still discussed by a myriad of organizations, as well as its role in CVD. In this aspect, CRP is more than a simple biomarker and current findings tightly link this protein with the atheromatous plaque. Its implementation is based on the guidelines suggested by the NACB, which delimit its application to a certain population at risk, and sets a cut-off point for its serum levels.
However, many aspects still remain to be elucidated, requiring the assessment of CRP behavior across ethnic groups (Asians, Africans, and Hispanics) since most studies have been limited to European and North American cohorts. Likewise, further research would clarify the true role of CRP in the development of CVD, establishing its relative importance regarding other CRF, which is a particularly relevant aspect given the potential benefit that may be rendered by broadening the spectrum of variables included in CVR-estimating calculation tools [101].
Furthermore, research should be expanded to further age groups, analyze the impact of CRP in coronary event prognosis, and decipher the phenomena linking it to the atherogenic process, in order to exploit its potential efficacy as a therapeutic target [102]. The answers to these matters would allow the confirmation of the feasibility of CRP quantification and the formulation of management guidelines for our patients, based in the measurement and the clinical picture of each individual.
It should be noted that despite the high prevalence of CVD in our population, CRP quantification remains a nonroutine procedure, neither in primary attention nor in specialist management. Therefore, raising awareness among all health personnel represents a fundamental basis for this kind of studies, which should be readily spread in order to offer a more efficient management to our patients. This is especially relevant for population reports such as our local study, which shows a particular behavior for CRP, with levels differing from those of most other worldwide studies—with lower average serum concentrations—as well as a close association with the metabolic syndrome, especially with high triacylglyceride levels and elevated waist circumference values (with cut-off points higher than those proposed by all current consensuses) [103]. These findings demonstrate the need to evaluate the behavior of these metabolic variables in each region in order to assess the comparative influence these cardiometabolic alterations exert over CVR and to set management guidelines adapted to each specific cohort.
Conflict of Interests
The authors declare that there is no conflict of interests regarding the publication of this paper.
References
- 1.Libby P, Ridker PM, Maseri A. Inflammation and atherosclerosis. Circulation. 2002;105(9):1135–1143. doi: 10.1161/hc0902.104353. [DOI] [PubMed] [Google Scholar]
- 2.Blankenberg S, Yusuf S. The inflammatory hypothesis: any progress in risk stratification and therapeutic targets? Circulation. 2006;114(15):1557–1560. doi: 10.1161/CIRCULATIONAHA.106.652081. [DOI] [PubMed] [Google Scholar]
- 3.Abbasi SH, Boroumand MA. Expanded network of inflammatory markers of atherogenesis: where are we now? Open Cardiovascular Medicine Journal. 2010;4(1):38–44. doi: 10.2174/1874192401004020038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Figueroa P, Hamad I, Pascual García FJ, Carazo Marín AF, Casado Almeida MA, García Forcada A. Proteína C reactiva en el pronóstico de la insuficiencia cardiaca. Revista Costarricense de Cardiologia. 2007;9:5–10. [Google Scholar]
- 5.Pepys MB, Hirschfield GM. C-reactive protein: a critical update. Journal of Clinical Investigation. 2003;111(12):1805–1812. doi: 10.1172/JCI18921. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bisoendial RJ, Boekholdt SM, Vergeer M, Stroes ESG, Kastelein JJP. C-reactive protein is a mediator of cardiovascular disease. European Heart Journal. 2010;31(17):2087–2095. doi: 10.1093/eurheartj/ehq238. [DOI] [PubMed] [Google Scholar]
- 7.Heres-Álvarez F, Peix-González A. La proteína C reactiva como blanco terapéutico en la prevención cardiovascular: ¿ficción o realidad? Revista Española de Cardiología. 2011;11(5):30–35. [Google Scholar]
- 8.Thompson SG, Kienast J, Pyke SDM, et al. Hemostatic factors and the risk of myocardial infarction or sudden death in patients with angina pectoris. The New England Journal of Medicine. 1995;332(10):635–641. doi: 10.1056/NEJM199503093321003. [DOI] [PubMed] [Google Scholar]
- 9.Turu MM, Slevin M, Matou S, et al. C-reactive protein exerts angiogenic effects on vascular endothelial cells and modulates associated signalling pathways and gene expression. BMC Cell Biology. 2008;9, article 47 doi: 10.1186/1471-2121-9-47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Ridker PM. C-reactive protein and the prediction of cardiovascular events among those at intermediate risk. moving an inflammatory hypothesis toward consensus. Journal of the American College of Cardiology. 2007;49(21):2129–2138. doi: 10.1016/j.jacc.2007.02.052. [DOI] [PubMed] [Google Scholar]
- 11.Yeh ETH. High-sensitivity C-reactive protein as a risk assessment tool for cardiovascular disease. Clinical Cardiology. 2005;28(9):408–412. doi: 10.1002/clc.4960280905. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Scottish Intercollegiate Guidelines Network, Risk estimation and the prevention of cardiovascular disease, A national clinical guideline, 2007.
- 13.Cupples LA, D’Agostino RB. Section 34: some risk factors related to the annual incidence of cardiovascular disease and death in pooled repeated biennial measurements. In: Kannel WB, Wolf PA, Garrison RJ, editors. Framingham Heart Study: 30 Year Follow-Up. Bethesda, Md, USA: Department of Health and Human Services; 1987. [Google Scholar]
- 14.D’Agostino RB, Sr., Vasan RS, Pencina MJ, et al. General cardiovascular risk profile for use in primary care: the framingham heart study. Circulation. 2008;117(6):743–753. doi: 10.1161/CIRCULATIONAHA.107.699579. [DOI] [PubMed] [Google Scholar]
- 15. National Vascular Disease Prevention Alliance, Guidelines for the assessment of absolute cardiovascular disease risk, 2009.
- 16.Spitalnic S. Risk Assessment I: Relative Risk and Absolute Risk Reduction. Hospital physician; 2005. [Google Scholar]
- 17.Amouyel P, Deverly A, Andrejak M, et al. Cardiovascular global risk: definition, evaluation and management strategies. Therapie. 2000;55(4):533–539. [PubMed] [Google Scholar]
- 18.Black HR. Cardiovascular risk factors. In: Zaret BL, Moser M, Cohen LS, editors. Yale University School of Medicine Heart Book. New York, NY, USA: Hearst Books; 1992. pp. 23–35. [Google Scholar]
- 19.Zannad F. Cardiovascular high-risk patients—treat to protect, but whom? Medscape General Medicine. 2008;10(supplement 2) [PMC free article] [PubMed] [Google Scholar]
- 20.Icaza G, Núñez L, Marrugat J, Mujica V, Escobar MC, et al. Estimación de riesgo de enfermedad coronaria mediante la función de Framingham adaptada para la población chilena. Revista Médica de Chile. 2009;137:1273–1282. [PubMed] [Google Scholar]
- 21.Liu J, Hong Y, D’Agostino RB, Sr., et al. Predictive value for the Chinese population of the Framingham CHD risk assessment tool compared with the Chinese multi-provincial cohort study. Journal of the American Medical Association. 2004;291(21):2591–2599. doi: 10.1001/jama.291.21.2591. [DOI] [PubMed] [Google Scholar]
- 22.Cleeman JI. Executive summary of the third report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III) Journal of the American Medical Association. 2001;285(19):2486–2497. doi: 10.1001/jama.285.19.2486. [DOI] [PubMed] [Google Scholar]
- 23.Assmann G, Cullen P, Schulte H. Simple scoring scheme for calculating the risk of acute coronary events based on the 10-year follow-up of the Prospective Cardiovascular Münster (PROCAM) study. Circulation. 2002;105(3):310–315. doi: 10.1161/hc0302.102575. [DOI] [PubMed] [Google Scholar]
- 24.Ferrario M, Chiodini P, Chambless LE, et al. Prediction of coronary events in a low incidence population: assessing accuracy of the CUORE Cohort Study prediction equation. International Journal of Epidemiology. 2005;34(2):413–421. doi: 10.1093/ije/dyh405. [DOI] [PubMed] [Google Scholar]
- 25.Zhang X-F, Attia J, D’Este C, Yu X-H, Wu X-G. A risk score predicted coronary heart disease and stroke in a Chinese cohort. Journal of Clinical Epidemiology. 2005;58(9):951–958. doi: 10.1016/j.jclinepi.2005.01.013. [DOI] [PubMed] [Google Scholar]
- 26.Jousilahti P, Vartiainen E, Tuomilehto J, Puska P. Sex, age, cardiovascular risk factors, and coronary heart disease: a prospective follow-up study of 14 786 middle-aged men and women in Finland. Circulation. 1999;99(9):1165–1172. doi: 10.1161/01.cir.99.9.1165. [DOI] [PubMed] [Google Scholar]
- 27.Ridker PM, Kastelein JJP, Genest J, Koenig W. C-reactive protein and cholesterol are equally strong predictors of cardiovascular risk and both are important for quality clinical care. European Heart Journal. 2013;34:1258–1261. doi: 10.1093/eurheartj/eht022. [DOI] [PubMed] [Google Scholar]
- 28.Šimon J, Rosolová H. Family history—and independent risk factors for coronary heart disease, it is time to be practical. European Heart Journal. 2002;23(21):1637–1638. doi: 10.1053/euhj.2002.3295. [DOI] [PubMed] [Google Scholar]
- 29.Nordestgaard BG, Chapman MJ, Ray K, et al. Lipoprotein(a) as a cardiovascular risk factor: current status. European Heart Journal. 2010;31(23):2844–2853. doi: 10.1093/eurheartj/ehq386. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Kurian AK, Cardarelli KM. Racial and ethnic differences in cardiovascular disease risk factors: a systematic review. Ethnicity and Disease. 2007;17(1):143–152. [PubMed] [Google Scholar]
- 31.Bonacina F, Baragetti A, Catapano AL, Norata GD. Long pentraxin 3: experimental and clinical relevance in cardiovascular diseases. Mediators of Inflammation. 2013;2013:10 pages. doi: 10.1155/2013/725102.725102 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Kannel WB. Blood pressure as a cardiovascular risk factor: prevention and treatment. Journal of the American Medical Association. 1996;275(20):1571–1576. [PubMed] [Google Scholar]
- 33.Ge Y, Cheng S, Larson MG, Ghorbani A, et al. Circulating CD31+ leukocyte frequency is associated with cardiovascular risk factors. Atherosclerosis. 2013;229:228–233. doi: 10.1016/j.atherosclerosis.2013.04.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Kannel WB, McGee DL. Diabetes and cardiovascular risk factors: the Framingham study. Circulation. 1979;59(1):8–13. doi: 10.1161/01.cir.59.1.8. [DOI] [PubMed] [Google Scholar]
- 35.Lentz SR, Haynes WG. Homocysteine: is it a clinically important cardiovascular risk factor? Cleveland Clinic Journal of Medicine. 2004;71(9):729–734. doi: 10.3949/ccjm.71.9.729. [DOI] [PubMed] [Google Scholar]
- 36.Price JF, Mowbray PI, Lee AJ, Rumley A, Lowe GDO, Fowkes FGR. Relationship between smoking and cardiovascular risk factors in the development of peripheral arterial disease and coronary artery disease: edinburgh artery study. European Heart Journal. 1999;20(5):344–353. doi: 10.1053/euhj.1998.1194. [DOI] [PubMed] [Google Scholar]
- 37.Stec JJ, Silbershatz H, Tofler GH, et al. Association of fibrinogen with cardiovascular risk factors and cardiovascluar disease the Framingham offspring population. Circulation. 2000;102(14):1634–1638. doi: 10.1161/01.cir.102.14.1634. [DOI] [PubMed] [Google Scholar]
- 38.Anderson KM, Castelli WP, Levy D. Cholesterol and mortality. 30 years of follow-up from the Framingham Study. Journal of the American Medical Association. 1987;257(16):2176–2180. doi: 10.1001/jama.257.16.2176. [DOI] [PubMed] [Google Scholar]
- 39.Barrios V, Gomez-Huelgas R, Rodríguez R, Pablos-Velasco P. Adiponectina, un factor de riesgo cardiovascular emergente. Estudio REFERENCE. Revista Española de Cardiología. 2008;61:1159–1167. [PubMed] [Google Scholar]
- 40.Sowers JR. Obesity as a cardiovascular risk factor. The American Journal of Medicine. 2003;115(supplement 8A):37S–41S. doi: 10.1016/j.amjmed.2003.08.012. [DOI] [PubMed] [Google Scholar]
- 41.Puddey IB, Rakic V, Dimmitt SB, Beilin LJ. Influence of pattern of drinking on cardiovascular disease and cardiovascular risk factors—a review. Addiction. 1999;94(5):649–663. doi: 10.1046/j.1360-0443.1999.9456493.x. [DOI] [PubMed] [Google Scholar]
- 42.Bijnen FCH, Caspersen CJ, Mosterd WL. Physical inactivity as a risk factor for coronary heart disease: a WHO and International Society and Federation of cardiology position statement. Bulletin of the World Health Organization. 1994;72(1):1–4. [PMC free article] [PubMed] [Google Scholar]
- 43.Anderson KM, Castelli WP, Levy D. Cholesterol and mortality. 30 years of follow-up from the Framingham Study. Journal of the American Medical Association. 1987;257(16):2176–2180. doi: 10.1001/jama.257.16.2176. [DOI] [PubMed] [Google Scholar]
- 44.Kagan A, Harris BR, Winkelstein W., Jr. Epidemiologic studies of coronary heart disease and stroke in Japanese men living in Japan, Hawaii and California: demographic, physical, dietary and biochemical characteristics. Journal of Chronic Diseases. 1974;27(7-8):345–364. doi: 10.1016/0021-9681(74)90014-9. [DOI] [PubMed] [Google Scholar]
- 45.Ge Y, Wang TJ. Identifying novel biomarkers for cardiovascular disease risk prediction. Journal of Internal Medicine. 2012;272(5):430–439. doi: 10.1111/j.1365-2796.2012.02589.x. [DOI] [PubMed] [Google Scholar]
- 46.Montgomery JE, Brown JR. Metabolic biomarkers for predicting cardiovascular disease. Vascular Health and Risk Management. 2013;9:37–45. doi: 10.2147/VHRM.S30378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Wilson PWF. Assessing coronary heart disease risk with traditional and novel risk factors. Clinical Cardiology. 2004;27(6) supplement 3:III7–III11. doi: 10.1002/clc.4960271504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Peter K, Nawroth P, Conradt C, et al. Circulating vascular cell adhesion molecule-1 correlates with the extent of human atherosclerosis in contrast to circulating intercellular adhesion molecule-1, E-selectin, P-selectin, and thrombomodulin. Arteriosclerosis, Thrombosis, and Vascular Biology. 1997;17(3):505–512. doi: 10.1161/01.atv.17.3.505. [DOI] [PubMed] [Google Scholar]
- 49.Su D, Li Z, Li X, Chen Y, Zhang Y, et al. Association between serum interleukin-6 concentration and mortality in patients with coronary artery disease. Mediators of Inflammation. 2013;2013:7 pages. doi: 10.1155/2013/726178.726178 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Forti N, Diament J. Apolipoprotein B and A-I: cardiovascular risk factor? Revista da Associacao Medica Brasileira. 2007;53(3):276–282. doi: 10.1590/s0104-42302007000300029. [DOI] [PubMed] [Google Scholar]
- 51.Jones A. Triglycerides and cardiovascular risk. Heart. 2013;99:1–2. doi: 10.1136/heartjnl-2012-302968. [DOI] [PubMed] [Google Scholar]
- 52.Willeit P, Thompson A, Aspelund T, et al. Hemostatic factors and risk of coronary heart disease in general populations: new prospective study and updated meta-analyses. PLoS ONE. 2013;8 doi: 10.1371/journal.pone.0055175.e55175 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Manzur F, Alvear Ciro, Alayon AN. Papel de la proteína c reactiva en las enfermedades cardiovasculares. Revista Colombiana de Cardiología. 2011;18:273–278. [Google Scholar]
- 54.Shih HH, Zhang S, Cao W, et al. CRP is a novel ligand for the oxidized LDL receptor LOX-1. American Journal of Physiology. 2009;296(5):H1643–H1650. doi: 10.1152/ajpheart.00938.2008. [DOI] [PubMed] [Google Scholar]
- 55.Frostegård J. Immunity, atherosclerosis and cardiovascular disease. BMC Medicine. 2013;11, article 117 doi: 10.1186/1741-7015-11-117. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Flores M, Barquera S, Carrión C, et al. Concentraciones de proteína C reactiva en adultos mexicanos: alta prevalencia de un factor de riesgo cardiovascular. Salud Pública de México. 2007;49:s348–s360. [Google Scholar]
- 57.Jeemon P, Prabhakaran D, Ramakrishnan L, et al. Association of high sensitive C-Reactive Protein (hsCRP) with established cardiovascular risk factors in the Indian population. Nutrition and Metabolism. 2011;8, article 19 doi: 10.1186/1743-7075-8-19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Razavi A, Baghshani MR, Rahsepar AA, et al. Association between C-reactive protein, pro-oxidant-antioxidant balance and traditional cardiovascular risk factors in an Iranian population. Annals of Clinical Biochemistry. 2013;50:115–121. doi: 10.1258/acb.2012.012104. [DOI] [PubMed] [Google Scholar]
- 59.Acevedo M, Arnáiz P, Barja S, et al. Relationship of C-reactive protein to adiposity, cardiovascular risk factors and subclinical atherosclerosis in healthy children. Revista Espanola de Cardiologia. 2007;60(10):1051–1058. doi: 10.1157/13111237. [DOI] [PubMed] [Google Scholar]
- 60.Kroop IG, Shackman NH. Level of C-reactive protein as a measure of acute myocardial infarction. Proceedings of the Society for Experimental Biology and Medicine. 1954;86(1):95–97. doi: 10.3181/00379727-86-21019. [DOI] [PubMed] [Google Scholar]
- 61.Gurevin I, Kozonis MC. The value of the C-reactive protein determination in coronary artery disease. Annals of Internal Medicine. 1957;46(1):79–85. doi: 10.7326/0003-4819-46-1-79. [DOI] [PubMed] [Google Scholar]
- 62.Ridker PM, Cushman M, Stampfer MJ, Tracy RP, Hennekens CH. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men. The New England Journal of Medicine. 1997;336(14):973–979. doi: 10.1056/NEJM199704033361401. [DOI] [PubMed] [Google Scholar]
- 63.Ferrer JI. Proteína C Reactiva (PCR) y ateroesclerosis. CENIC Ciencias Biológicas. 2005;36:79–84. [Google Scholar]
- 64.Tracy RP, Lemaitre RN, Psaty BM, et al. Relationship of C-reactive protein to risk of cardiovascular disease in the elderly: results from the cardiovascular health study and the rural health promotion project. Arteriosclerosis, Thrombosis, and Vascular Biology. 1997;17(6):1121–1127. doi: 10.1161/01.atv.17.6.1121. [DOI] [PubMed] [Google Scholar]
- 65.Ledue TB, Weiner DL, Sipe JD, Poulin SE, Collins MF, Rifai N. Analytical evaluation of particle-enhanced immunonephelometric assays for C-reactive protein, serum amyloid A and mannose-binding protein in human serum. Annals of Clinical Biochemistry. 1998;35(6):745–753. doi: 10.1177/000456329803500607. [DOI] [PubMed] [Google Scholar]
- 66.Roberts WL, Moulton L, Law TC, et al. Evaluation of nine automated high-sensitivity C-reactive protein methods: implications for clinical and epidemiological applications. Part 2. Clinical Chemistry. 2001;47(3):418–425. [PubMed] [Google Scholar]
- 67.Yeh ETH, Willerson JT. Coming of age of C-reactive protein: using inflammation markers in cardiology. Circulation. 2003;107(3):370–372. doi: 10.1161/01.cir.0000053731.05365.5a. [DOI] [PubMed] [Google Scholar]
- 68.Pearson TA, Mensah GA, Alexander RW, et al. Markers of inflammation and cardiovascular disease: application to clinical and public health practice: a statement for healthcare professionals from the centers for disease control and prevention and the American Heart Association. Circulation. 2003;107(3):499–511. doi: 10.1161/01.cir.0000052939.59093.45. [DOI] [PubMed] [Google Scholar]
- 69.Jellinger PS, Smith DA, Mehta AE, et al. American association of clinical endocrinologists’ guidelines for management of dyslipidemia and prevention of atherosclerosis. Endocrine Practice. 2012;18(1):1–78. doi: 10.4158/ep.18.s1.1. [DOI] [PubMed] [Google Scholar]
- 70.Myers GL, Christenson RHM, Cushman M, et al. National academy of clinical biochemistry laboratory medicine practice guidelines: emerging biomarkers for primary prevention of cardiovascular disease. Clinical Chemistry. 2009;55(2):378–384. doi: 10.1373/clinchem.2008.115899. [DOI] [PubMed] [Google Scholar]
- 71.Ridker PM, Buring JE, Shih J, Matias M, Hennekens CH. Prospective study of C-reactive protein and the risk of future cardiovascular events among apparently healthy women. Circulation. 1998;98(8):731–733. doi: 10.1161/01.cir.98.8.731. [DOI] [PubMed] [Google Scholar]
- 72.Ridker PM, Rifai N, Rose L, Buring JE, Cook NR. Comparison of C-reactive protein and low-density lipoprotein cholesterol levels in the prediction of first cardiovascular events. The New England Journal of Medicine. 2002;347(20):1557–1565. doi: 10.1056/NEJMoa021993. [DOI] [PubMed] [Google Scholar]
- 73.Cesari M, Penninx BWJH, Newman AB, et al. Inflammatory markers and onset of cardiovascular events: results from the Health ABC Study. Circulation. 2003;108(19):2317–2322. doi: 10.1161/01.CIR.0000097109.90783.FC. [DOI] [PubMed] [Google Scholar]
- 74.Ridker PM, Buring JE, Rifai N, Cook NR. Development and validation of improved algorithms for the assessment of global cardiovascular risk in women: the reynolds risk score. Journal of the American Medical Association. 2007;297(6):611–619. doi: 10.1001/jama.297.6.611. [DOI] [PubMed] [Google Scholar]
- 75.Ridker PM, Paynter NP, Rifai N, Gaziano JM, Cook NR. C-reactive protein and parental history improve global cardiovascular risk prediction: the reynolds risk score for men. Circulation. 2008;118(22):2243–2251. doi: 10.1161/CIRCULATIONAHA.108.814251. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Kaptoge S, Di Angelantonio E, Lowe G, et al. The emerging risk factors collaboration. C-reactive protein concentration and risk of coronary heart disease, stroke, and mortality: an individual participant meta-analysis. The Lancet. 2010;375:132–140. doi: 10.1016/S0140-6736(09)61717-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Maiorana C, Duque J, Pellino M, et al. Más allá de la prevención primaria: utilidad de la Proteína C Reactiva Ultra sensible (PCRus), como herramienta en el diagnóstico de enfermedad arterial coronaria. Síndrome Cardiometabólico. 2011;1:40–44. [Google Scholar]
- 78.Morrow DA, de Lemos JA, Sabatine MS, et al. Clinical relevance of C-reactive protein during follow-up of patients with acute coronary syndromes in the Aggrastat-to-Zocor Trial. Circulation. 2006;114(4):281–288. doi: 10.1161/CIRCULATIONAHA.106.628909. [DOI] [PubMed] [Google Scholar]
- 79.Mueller C, Buettner HJ, Hodgson JM, et al. Inflammation and long-term mortality after non-ST elevation acute coronary syndrome treated with a very early invasive strategy in 1042 consecutive patients. Circulation. 2002;105(12):1412–1415. doi: 10.1161/01.cir.0000012625.02748.62. [DOI] [PubMed] [Google Scholar]
- 80.Caixeta A, Stone GW, Mehran R, et al. Predictive value of C-reactive protein on 30-day and 1-year mortality in acute coronary syndromes: an analysis from the ACUITY trial. Journal of Thrombosis and Thrombolysis. 2011;31(2):154–164. doi: 10.1007/s11239-010-0516-y. [DOI] [PubMed] [Google Scholar]
- 81.Arroyo-Espleguiro R, Avanzas P, Kaski JC. Enfermedad cardiovascular aterosclerótica: la utilidad de la proteína C reactiva en la identificación de la placa “vulnerable” y del paciente ‘vulnerable’. Revista Española de Cardiología. 2004;57:375–378. [PubMed] [Google Scholar]
- 82.Bodi V, Sanchís J. La proteína C reactiva en el síndrome coronario agudo. Una mirada atrás para seguir avanzando. Revista Española de Cardiología. 2006;59:418–420. [PubMed] [Google Scholar]
- 83.Kaski JC, Fernández-Bergés D. Proteína C reactiva en el servicio de urgencias: ‘ha encontrado una aplicación clínica? Revista Española de Cardiología. 2007;60:797–800. [PubMed] [Google Scholar]
- 84.Pietila KO, Harmoinen AP, Jokiniitty J, Pasternack AI. Serum C-reactive protein concentration in acute myocardial infarction and its relationship to mortality during 24 months of follow-up in patients under thrombolytic treatment. European Heart Journal. 1996;17(9):1345–1349. doi: 10.1093/oxfordjournals.eurheartj.a015068. [DOI] [PubMed] [Google Scholar]
- 85.Gussekloo J, Schaap MCL, Frölich M, Blauw GJ, Westendorp RGJ. C-reactive protein is a strong but nonspecific risk factor of fatal stroke in elderly persons. Arteriosclerosis, Thrombosis, and Vascular Biology. 2000;20(4):1047–1051. doi: 10.1161/01.atv.20.4.1047. [DOI] [PubMed] [Google Scholar]
- 86.Schiele F, Meneveau N, Seronde MF, et al. C-reactive protein improves risk prediction in patients with acute coronary syndromes. European Heart Journal. 2010;31(3):290–297. doi: 10.1093/eurheartj/ehp273. [DOI] [PubMed] [Google Scholar]
- 87.Atkinson A.J. J, Colburn WA, DeGruttola VG, et al. Biomarkers and surrogate endpoints: preferred definitions and conceptual framework. Clinical Pharmacology and Therapeutics. 2001;69(3):89–95. doi: 10.1067/mcp.2001.113989. [DOI] [PubMed] [Google Scholar]
- 88.van der Bom J, Cramer MJ. C-reactive protein as a prognostic tool in cardiovascular practices: should CRP testing be ordered along with lipid profiles? Netherlands Heart Journal. 2003;11:265–267. [PMC free article] [PubMed] [Google Scholar]
- 89.Ueda S, Ikeda U, Yamamoto K, et al. C-reactive protein as a predictor of cardiac rupture after acute myocardial infarction. American Heart Journal. 1996;131(5):857–860. doi: 10.1016/s0002-8703(96)90164-7. [DOI] [PubMed] [Google Scholar]
- 90.Boekholdt SM, Hack CE, Sandhu MS, et al. C-reactive protein levels and coronary artery disease incidence and mortality in apparently healthy men and women: the EPIC-Norfolk prospective population study 1993–2003. Atherosclerosis. 2006;187(2):415–422. doi: 10.1016/j.atherosclerosis.2005.09.023. [DOI] [PubMed] [Google Scholar]
- 91.Vasan RS, Sullivan LM, Roubenoff R, et al. Inflammatory markers and risk of heart failure in elderly subjects without prior myocardial infarction: the Framingham Heart Study. Circulation. 2003;107(11):1486–1491. doi: 10.1161/01.cir.0000057810.48709.f6. [DOI] [PubMed] [Google Scholar]
- 92.Ridker PM, Stampfer MJ, Rifai N. Novel risk factors for systemic atherosclerosis: a comparison of C-reactive protein, fibrinogen, homocysteine, lipoprotein(a), and standard cholesterol screening as predictors of peripheral arterial disease. Journal of the American Medical Association. 2001;285(19):2481–2485. doi: 10.1001/jama.285.19.2481. [DOI] [PubMed] [Google Scholar]
- 93.Ridker PM. C-Reactive protein: eighty years from discovery to emergence as a major risk marker for cardiovascular disease. Clinical Chemistry. 2009;55(2):209–215. doi: 10.1373/clinchem.2008.119214. [DOI] [PubMed] [Google Scholar]
- 94.Kraus VB, Jordan JM. Serum C-Reactive Protein (CRP), target for therapy or trouble? Biomarker Insights. 2006;1:77–80. [PMC free article] [PubMed] [Google Scholar]
- 95.Hingorani AD, Shah T, Casas JP, Humphries SE, Talmud PJ. C-Reactive protein and coronary heart disease: predictive test or therapeutic target? Clinical Chemistry. 2009;55(2):239–255. doi: 10.1373/clinchem.2008.115923. [DOI] [PubMed] [Google Scholar]
- 96.Buckley DI, Fu R, Freeman M, Rogers K, Helfand M. C-reactive protein as a risk factor for coronary heart disease: a systematic review and meta-analyses for the U.S. preventive services task force. Annals of Internal Medicine. 2009;151(7):483–495. doi: 10.7326/0003-4819-151-7-200910060-00009. [DOI] [PubMed] [Google Scholar]
- 97.Ridker PM, Rifai N, Clearfield M, et al. Measurement of C-reactive protein for the targeting of statin therapy in the primary prevention of acute coronary events. The New England Journal of Medicine. 2001;344(26):1959–1965. doi: 10.1056/NEJM200106283442601. [DOI] [PubMed] [Google Scholar]
- 98.Nissen SE, Tuzcu EM, Schoenhagen P, et al. Effect of intensive compared with moderate lipid-lowering therapy on progression of coronary atherosclerosis: a randomized controlled trial. Journal of the American Medical Association. 2004;291(9):1071–1080. doi: 10.1001/jama.291.9.1071. [DOI] [PubMed] [Google Scholar]
- 99.Ridker PM, Danielson E, Fonseca FA, et al. Reduction in C-reactive protein and LDL cholesterol and cardiovascular event rates after initiation of rosuvastatin: a prospective study of the JUPITER trial. The Lancet. 2009;373(9670):1175–1182. doi: 10.1016/S0140-6736(09)60447-5. [DOI] [PubMed] [Google Scholar]
- 100.Oh J, Teoh H, Leiter LA. Should C-reactive protein be a target of therapy? Diabetes Care. 2011;34(2):S155–S160. doi: 10.2337/dc11-s211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 101.Bermúdez V, Rojas E, Salazar JJ, et al. Coronary risk estimation according to the framingham-wilson score: epidemiologic behavior of innovative cardio metabolic risk factors in the maracaibo city. International Journal of Cardiovascular Research. 2013;2, article 4 [Google Scholar]
- 102.Ong KL, Allison MA, Cheung BM, et al. Trends in C-reactive protein levels in US adults From 1999 to 2010. American Journal of Epidemiology. 2013;177:1430–1442. doi: 10.1093/aje/kws443. [DOI] [PubMed] [Google Scholar]
- 103.Bermúdez V, Cabrera M, Mendoza L, et al. High-sensitivity C-Reactive Protein epidemiological behavior in adult individuals from Maracaibo, Venezuela. Revista Latinoamericana de Hipertension. 2013;8(1):22–29. [Google Scholar]