

Abstract
Objective
To examine recent studies on the effect of mobile and electronic (ME)-health technology on adherence to acne treatment.
Background
With emerging use of ME-health technology, there is a growing interest in evaluating the effectiveness of the tools on medication adherence. Examples of ME-health technology-based tools include text message-based pill reminders and Web-based patient education.
Methods
MEDLINE, Cochrane Library, and Web of Science were searched for articles on adherence to acne treatment published through November 2013. A combination of search terms such as “acne” and “adherence” or “compliance” were used.
Results
Adherence to oral acne medication was higher than for topical acne medication. The frequency of office visits was also an influencing factor for acne treatment adherence. The telephone-based reminders on a daily basis did not improve acne patients’ medication adherence, whereas the Web-based educational tools on a weekly basis had a positive effect on medication adherence in acne treatment.
Conclusion
In using ME-health interventions, factors such as medication dosage forms, frequency of intervention, and patients’ preferences should be taken into consideration. Developing disease-specific text message reminders may be helpful to increase adherence rates. In addition, a combination of text message reminders with another type of intervention may improve medication adherence.
Keywords: acne vulgaris, medication adherence, compliance, mobile and electronic health technology, application software, telemedicine
Introduction
Acne vulgaris is a common skin disorder characterized by a multiple spectrum of lesions affecting different parts of the body.1 The disorder affects 45 million people in the United States, with over 85% of the affected population aged 15–24 years.2 Males typically have a higher prevalence and more severe form of the disorder than females. There are physical (eg, lesions, pain) as well as psychological (eg, depression) morbidities associated with acne. As for acne treatment, milder acne is typically treated with topical regimens, whereas severe acne is treated using systemic medications. Topical medications include retinoids, antibiotics, and benzoyl peroxide. Systemic agents include hormonal therapies, oral antibiotics, and oral isotretinoin.1
In many cases, acne treatment fails because of low medication adherence. Poor medication adherence may be associated with various factors such as medication dosage forms and adverse effects, costs of treatment, lack of education, and frustration with previous therapy failures.3 With emerging use of mobile and electronic (ME)-health technology (eg, text message-based pill reminders, Web-based patient education), there is a growing interest in evaluating the effectiveness of the tools on medication adherence. The purpose of this study is to examine recent studies on the effect of ME-health technology on adherence to acne treatment.
Methods
Search strategy
We searched MEDLINE, the Cochrane Library, and Web of Science for articles on adherence to acne treatment published from inception to November 2013. The search terms were a combination of the following: “acne” and “adherence” or “compliance”. In addition, we searched in the reference lists of these articles. The main search and screening of titles and abstracts was conducted independently by two authors. The search was restricted to articles published in English.
Inclusion criteria
Both published and presented studies were selected if they involved patients with acne, compared technology interventions and no interventions/other interventions, measured the outcome as medication adherence to acne treatment, and were published in English.
Data extraction
Both the main search and the screening of titles and abstracts were conducted independently by two authors (CP and GK).
Results
Study and patient characteristics
A total of 414 potentially relevant articles were identified with the keyword search. Through an independent review of these selected abstracts by two reviewers, eleven articles were retrieved for further evaluation. Among those, four articles examined the effect of technology on adherence for acne treatment.4–7 Figure 1 shows a flow diagram of the search strategy and review process.
Figure 1.
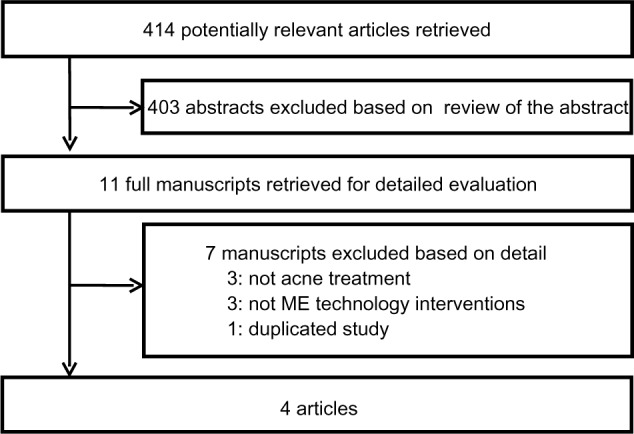
Flow diagram of search strategy.
Abbreviation: ME, mobile and electronic.
The effect of technology on medication adherence in patients with acne
Overall, we summarized the study methods and baseline patient characteristics of each study in Table 1. Among the four studies, interventions were categorized as telephone-based technology and Internet-based technology. To the best of our knowledge, research on evaluating interventions of smartphone application technology in this field has not been published. Three studies included mild to moderate acne patients,4,6,7 and one study included moderate to severe acne patients.5 Among the four studies, there were two studies in which the technology intervention groups were compared with no intervention groups,4,6 one study that directly compared the technology intervention group with different types of intervention groups,7 and one study that compared the technology group with either the intervention group or different types of intervention groups.5 All but one study reported the age of patients and included adolescent patients with acne.
Table 1.
Characteristics of randomized controlled trials included in the review
| Study and groups | Intervention | Number of participants | Age (range of years) |
Sex (% of male) |
Acne severity |
|---|---|---|---|---|---|
| Boker et al, 20124 | |||||
| Treatment | Text message reminders | 19 | 14–35 (mean, 22.8) | 52.6 | Mild to moderate |
| Control | None | 21 | 12–32 (mean, 22.5) | 71.4 | Mild to moderate |
| Yentzer et al, 20115 | |||||
| Treatment | Telephone call reminders | 15 | NA | NA | Moderate to severe |
| Control 1 | None | 16 | |||
| Control 2 | Frequent office visits | 15 | |||
| Control 3 | Parental reminders | 15 | |||
| Yentzer et al, 20116 | |||||
| Treatment | Internet-based | 10 | 13–18 | NA | Mild to moderate |
| Control | None | 10 | |||
| Wang et al, 20117 | |||||
| Treatment | Internet (acne-related questions) | 25 | 13–69 | NA | Mild to moderate |
| Control | Internet (nondermatologic-related questions) | 25 | |||
Abbreviation: NA, not applicable.
Table 2 shows the description of medication, technology-based intervention, and medication adherence measurement method of each study. In the two studies on telephone-based technology, one study used text messages and the other study used telephone calls as an intervention to improve acne medication adherence. Both studies used each intervention method to remind patients to apply topical medications.4,5 In contrast, two other studies used Internet-based interventions as education tools instead of reminders.6,7 Medication adherence rates by interventions among three studies are presented in Figure 2.4–6 The results from Wang et al7 were not included in this table because they did not report medication adherence rates by intervention.
Table 2.
Description of medication, technology-based intervention, and the medication adherence measure of randomized controlled trials included in the review
| Study | Medication | Intervention | Adherence |
|---|---|---|---|
| Boker et al, 20124 | • Topical medication (12 weeks) – Morning: OTC facial cleanser, followed by 3 pea-sized amounts of clindamycin/benzoyl peroxide 1%/5% topical gel – E vening: 1 pea-sized amount adapalene 0.3% gel |
• Type: text message reminder • Frequency: twice a day • Duration: 12 weeks |
• Measurement: MEMS cap • Calculation: actual number of correct MEMS cap opening/closing events for each tube divided by the expected number of opening/closing events |
| Yentzer et al, 20115 | • Topical medication (12 weeks): adapalene 0.1% gel once-daily | • Type: telephone call reminder • Frequency: once a day • Duration: 12 weeks |
• Measurement: MEMS cap • Calculation: not specified |
| Yentzer et al, 20116 | • Topical medication (12 weeks): benzoyl peroxide 5% gel once-daily | • Type: Internet-based communication: email containing a link to a survey assessing acne severity and treatment • Frequency: once a week • Duration: 12 weeks |
• Measurement: MEMS cap; patients’ report • Calculation: percentage of days the medication container was opened |
| Wang et al, 20117 | • Not specified | • Type: Internet-based interactive health care education tool • Frequency: once a week • Duration: 12 weeks |
• Measurement: clinical outcomes and quality of life |
Abbreviations: OTC, over-the-counter; MEMS, Medication Event Monitoring System.
Figure 2.
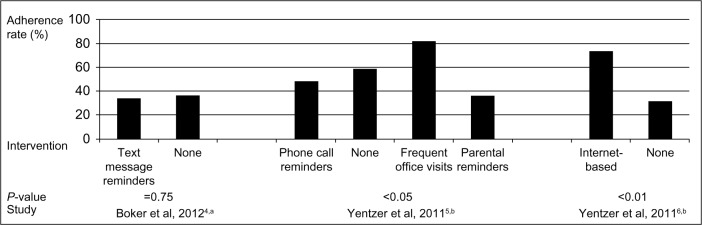
Medication adherence rates using electronic Medication Event Monitoring System cap over the course of 12 weeks.
Notes: Wang et al7 was not included because medication adherence rates were not reported. aMean adherence rates; bmedian adherence rates.
A study by Boker et al4 examined the effect of automated text messages on adherence to topical medications (clindamycin/benzoyl peroxide tube 1%/5% topical gel in the morning and adapalene 0.3% gel in the evening). In this study, patients in the intervention group received a customized text message reminder twice-daily over the course of 12 weeks. Medication adherence of those gels was measured using a customized electronic Medication Event Monitoring System (MEMS; Aardex Group, Sion, Switzerland) cap. This study defined medication adherence as the actual number of correct MEMS cap opening/closing events divided by the expected number of opening/closing events for each gel. This study did not find any significant effect of text message reminders on the medication adherence rate. Mean adherence rates were 33.9% for patients in the text message reminder group and 36.5% for patients in the no-intervention group (P=0.75). In addition, patients in the text message reminder group had similar clinical improvement of their acne and quality of life when compared with patients in the no-intervention group. The authors pointed out three main limitations that might have led to no differences being seen in adherence rate and clinical outcomes: small sample size, too-frequent text message reminders, and the differences between the actual study drug application and the opening/closing events of MEMS caps.
In the first study by Yentzer et al,5 the effect of the telephone call reminder intervention was compared not only with the no-intervention group but also with two other interventions (more frequent office visits and parental reminders). Although the other three studies included patients with mild to moderate acne, this study included patients with moderate to severe acne. All patients in the telephone call reminder group and the parental reminders group received a reminder once a day over the course of 12 weeks and made visits to their physicians during weeks 6 and 12, whereas patients in the frequent office group made visits to their physicians during weeks 1, 2, 4, 6, 8, and 12 without a reminder to improve medication adherence. This study also measured medication adherence to topical gels using the MEMS cap. Similar to the previous study by Boker et al,4 this study also did not demonstrate any effect of the telephone call reminder on improved medication adherence when compared with other interventions. The highest median medication adherence rate was shown in the frequent-visits group (82%), followed by the no-intervention group (59%), whereas the median medication adherence rates in the telephone call reminders group and parental reminders group were 48% and 36%, respectively. The authors also indicated small sample size as a limitation of the study.
In another study by Yentzer et al,6 the study objective was to determine whether the Internet-based intervention group increased adherence to topical acne therapy in teenagers. In this study, the Internet-based intervention group was compared with the no-intervention group. Interestingly, the intervention was not a reminder but a survey assessing acne severity and treatment to improve the adherence rate. The survey was sent out using e-mail to each patient once a week over the course of 12 weeks. Medication adherence was measured by two different methods: MEMS cap and patient-reported adherence. As a result, overall adherence rates ranged from 58% to 132% (adherence measured by MEMS caps in this study was defined as the percentage of days with the medication container opened; adherence rate could be over 100% if the medication container was opened more than once a day) in the Internet-based intervention group and from 4% to 80% the no-intervention group. Specifically, there was a statistically significant difference in adherence rates between the Internet-based intervention group (median, 74%) and the no-intervention group (median, 32%) (P<0.01). With regard to the measurement method of adherence, there was no significant difference between MEMS cap adherence rate and patient-reported adherence rate (P=0.11). This was the only study that showed the positive effect of the ME intervention on adherence rate.
The last study on the ME intervention used the Internet-based education tool.7 Although the purpose of the intervention in this study was to improve medication adherence, the outcome was measured by using clinical outcomes (ie, the numbers of inflammatory acne lesions and noninflammatory acne lesions) and health-related quality of life. Patients with mild to moderate acne received weekly emails with five multiple-choice questions, which were acne-related questions in the Internet-based intervention group and general health-related questions in the control group. The results showed that clinical outcomes and quality-of-life scores were better in the Internet-based intervention group than the control group, but these differences were not statistically significant. Similar to the limitations of other studies, the insignificant result could be a result of the small sample size (N=50).
In summary, among the four studies, the telephone-based reminders on a daily basis did not improve acne patients’ medication adherence, whereas the Internet-based educational tools on a weekly basis had a positive effect on better medication adherence in acne treatment.6 These results could be used as evidence to develop a future ME technology-related intervention in terms of the frequency of intervention or the technology type of intervention.
Discussion
Medication adherence in patients with acne
There is no gold standard for measuring medication adherence, and measurement methods for medication adherence are generally categorized into the following: direct methods (eg, directly observed therapy; biological markers [blood or urine] using drug levels; and use of drug markers with the target medication) and indirect methods (eg, electronic monitoring devices, medication measurement [pill counts], review of prescription refill records, and self-reporting).8,9 To date, research on medication adherence to acne treatment has focused on indirect methods.
Self-reporting is one of the most commonly used methods to measure acne medication. One study measured the adherence of both oral acne medication (isotretinoin) and topical acne medication.10 This study found that the medication adherence of the oral medication was better than that of the topical medication. In addition to questionnaire methods, several studies used patients’ diaries to measure adherence in acne medication.11,12 When using patients’ diary methods, most patients report higher topical medication adherence rates. Those studies also demonstrated that medication adherence rates in the once-daily treatment group were higher than those in the twice-daily treatment group.
Another frequently used measurement method is pill counts. One study reported that medication adherence rate of isotretinoin (71.4%) was higher when compared with topical medication and oral medication other than isotretinoin (35.2%).13
Alternatively, prescription refill records can also be used to measure medication adherence. Previous research found that when patients refilled their acne medications more frequently, they had a better acne outcome.14 As such, adherence to acne medications is an important factor of better acne outcome.
Finally, electronic monitoring has also been used in recently published studies. For many acne medications that are formulated as a gel, MEMS caps are frequently used to measure adherence. MEMS caps record the date and time each time the medication containers are opened or closed. A study using MEMS caps to measure the adherence of topical benzoyl peroxide found that adherence decreased when the time between office visits was expanded.15 This implies that frequent office visits are a critical factor in acne treatment adherence.
On the basis of the previous research, we found a couple of common trends. First, oral medication, especially isotretinoin, showed better adherence trends when compared with topical medication. Second, the frequency of office visits is also an influencing factor for acne treatment adherence.
Mobile and electronic health technology use in multiple disease states
With emerging technologies, ME-health tools are providing patients with various options outside the typical in-office physician visits to manage their health. These tools aim to offer different aspects of health management, including providing health care information, behavioral support, and behavioral intervention. Mobile telephone-based tools (eg, text messages, applications) serve multiple functions such as that of medical information provider, medication-taking aid tool (eg, pill reminder, medication and dosage guidance, data collection for medication adverse effect response), and health monitoring manager (eg, monitoring of vital health signs).16 Examples of Internet-based tools include online-based home monitoring from a health center, interactive communication between patient and health care provider via email, and a Web-based educational program. Although ME-health technology intends to improve multiple patient outcomes, medication adherence is one main area of focus. Several studies examined the effectiveness of ME-health interventions on medication adherence.
A few studies evaluated the effect of mobile telephone-based interventions on medication adherence.17–20 Two randomized controlled trials demonstrated that integration of mobile telephone intervention into antiretroviral therapy management improved patients’ adherence to therapy. In the first study, patients communicated with health care professionals via weekly text messages, replying back and forth to questions regarding their health condition. The self-reported medication adherence for the text message group was significantly higher than in the control group (62% versus 50%; P=0.006).17 In the second study, patients received a one-way text message as a reminder to take their medications. During the study period of 48 weeks, 53% of the text message group were adherent, whereas 40% of the control group were adherent (P=0.03).18 In a pilot study that examined the use of daily text messages as a medication reminder and educational tool for 12 weeks in psoriasis patients, medication adherence increased from 3.86 days per week to 6.46 days per week.19 There is currently an ongoing trial that aims to evaluate the effect of mobile telephone-based interventions on adherence to naltrexone among treatment-seeking heavy drinkers. The subjects will receive text messages as medication reminders at a frequency that is tailored to their adherence. The mobile telephone is further used to keep daily records of alcohol use and medication adverse effects.20
In addition, a few other studies examined the effectiveness of using Internet-based and electronic device-based interventions on different patient outcomes, including medication adherence. In a 12-week randomized controlled trial of 120 pediatric patients with asthma, the Internet-based intervention group decreased in adherence to inhaled corticosteroids during the study period but had significantly higher adherence than the control group at the end of the study period. Although the control group underwent traditional asthma care, the intervention group participated in regular self-monitoring of asthma status via the Internet and an interactive program that offered asthma education and a management plan.21 In the other randomized controlled trial, the combined use of Web-based intervention and telephone nurse case management was shown to improve pediatric asthma control compared with the control group, but not significantly in the composite adherence scores (P=0.76).22 Elkjaer et al23 showed that with the use of an Internet-based program, there was a significant improvement in adherence to 4 weeks of acute treatment (increased by 31% in Denmark and 44% in Ireland, respectively, to control group) in mild to moderate ulcerative colitis patients receiving 5-aminosalicylate acid treatment. At 12 months of follow-up, however, there was no significant difference in refilling their prescriptions (68% of the Web-based group versus 69% of the control group refilled at least 80% of medications). During the Internet-based intervention, patients had to visit the Internet-based program to record their disease activity score and could contact the Web doctor regarding their disease.23 A study by Frangou et al24 demonstrated that when compared with the control and pill counting group, the electronic monitoring group had significantly higher medication adherence among patients with schizophrenia during a study period of 8 weeks. Although the control group received standard treatment from mental health services and the pill-counting group was involved in counting their medication pills at each pharmacy visit, the electronic monitoring group used an electronic medication dispenser that issued alerts if less than half of a medication was taken on a weekly basis.24
Overall, there were inconsistent findings in the effect of ME technology on medication adherence across multiple disease states.17–24 In the three studies that used mobile telephone-based interventions, text messages were the primary source of intervention. Although the studies were conducted using different content and frequency of text messages, as well as different study periods, all of them showed significant improvement in medication adherence.17–19 In contrast, among the studies that used Internet-based interventions,21–23 only one of three studies reported significant improvement in medication adherence.23 These studies also varied in the content of intervention and study periods. Medication adherence was shown to improve in the other study on electronic monitoring-based intervention.24
Future directions for mobile and electronic health technology in acne treatment
The goal of this study was to summarize the effect of ME-health interventions on medication adherence to acne treatment. To accomplish this goal, we searched for previous studies on the factors that are associated with medication adherence among acne patients and current technology-related interventions across different disease types. Through a substantial literature review, we found several common results on technology-based interventions to acne treatment. In addition, these results could provide evidence to enhance ME-health interventions for better medication adherence to acne treatment in the future.
First, we found that the effect of text message reminders was inconsistent across different disease types. Specifically, mobile telephone intervention improved patients’ adherence rates in antiretroviral therapy management,17,18 however, we failed to find a significant relationship between text reminders and improved adherence to acne treatment.4,5 Thus, developing disease-specific text message remainders could be helpful to increase adherence rates. For example, sending personalized text messages to teenaged acne patients might be more effective than sending a generic text message to all acne patients.
Second, the dosage regimen of acne treatment was related to medication adherence rates. In general, topical medications are the first-line therapy for mild to moderate acne patients, whereas oral antibiotics or isotretinoin are the first-line therapy for severe cystic acne.3 Several studies found that patients receiving oral acne medication showed generally better adherence trends compared with those receiving topical acne medication, including gel-type medications.10,13 These results suggest that future ME-health interventions should differentiate between dosage forms, which are often related to acne severity.
Third, the frequency of ME-health interventions might be a critical factor for the improvement of medication adherence. It is clearly shown that although ME-health intervention on a daily basis was not effective, intervention on a weekly basis showed a positive association between intervention and medication adherence in acne treatment. In addition, in one study that used twice-daily text messaging, the authors mentioned a possibility that this frequency of reminders was too high and suggested that less-frequent text messaging reminders may be more influential.4 Thus, it may be of importance to investigate the appropriate frequency of ME-health intervention, which can motivate the patient to apply or take medications.
Fourth, we found that sending text message reminders alone might not guarantee the improvement of medication adherence. Rather, there is a possibility that a combination of text message reminders with another type of intervention could be a more effective way to improve medication adherence rate. For example, a smartphone application that has an alarm function for medication reminders and educational tools might be a promising intervention. In addition, text message reminders with a clinician-provided intervention could be effective.
Finally, there is a possibility that better medication adherence rates might be related to patients having a more favorable opinion of the intervention. Conversely, if patients admitted to disliking any of the interventions, the adherence rates might not be improved or may even decrease. One study demonstrated that parental reminders resulted in lower medication adherence.5 When considering the characteristics of teenagers, such as oppositional and defiant behavior, parents should be cautious when reminding their teenagers to take or apply medications. In this context, developing future ME-health interventions for acne treatment should take into account the potential negative effects of parent related interventions.
Limitations of the studies included in the review
Overall, previous studies on ME-health interventions for acne treatment have several common limitations. First, the study period of four included studies was 12 weeks. This may not be enough time to improve adherence rates by changing patients’ behavior. As such, some of these studies might not show significant relationships between technology-based interventions and medication adherence rate. Thus, if future studies expand the study period, a positive relationship between technology-based intervention and acne medication adherence might be suggested. Second, small sample sizes could lead to lack of a significant association between ME-based intervention and better medication adherence. The sample size in four of the studies ranged from 20 to 61, and the number of each group within these studies ranged from 10 to 25. Because of this small sample size, although the medication adherence rates between the intervention group and the control group might be different, it is difficult to demonstrate a statistically significant difference. Third, to measure adherence of patients using topical medications, MEMS caps were used. In future studies, other methods, such as prescription refill records, could be considered to evaluate general trends within large sample sizes.
Conclusion
This review study summarizes the effect of ME-health interventions on acne medication adherence. To the best of our knowledge, this is the first systematic review on this topic. In conclusion, it is suggested that sending only text message reminders might not be an effective method for improving medication adherence. In the future, to use ME-health interventions more effectively, these technologies should be developed in combination with other types of interventions, including educational tools and interventions provided by clinicians.
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Dawson AL, Dellavalle RP. Acne vulgaris. BMJ. 2013;346:f2634. doi: 10.1136/bmj.f2634. [DOI] [PubMed] [Google Scholar]
- 2.Agency for Healthcare Research and Quality Management of acne. [Accessed on Jan 31, 2014]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK11955/
- 3.Lott R, Taylor SL, O’Neill JL, Krowchuk DP, Feldman SR. Medication adherence among acne patients: a review. J Cosmet Dermatol. 2010;9(2):160–166. doi: 10.1111/j.1473-2165.2010.00490.x. [DOI] [PubMed] [Google Scholar]
- 4.Boker A, Feetham HJ, Armstrong A, Purcell P, Jacobe H. Do automated text messages increase adherence to acne therapy? Results of a randomized, controlled trial. J Am Acad Dermatol. 2012;67(6):1136–1142. doi: 10.1016/j.jaad.2012.02.031. [DOI] [PubMed] [Google Scholar]
- 5.Yentzer BA, Gosnell AL, Clark AR, et al. A randomized controlled pilot study of strategies to increase adherence in teenagers with acne vulgaris. J Am Acad Dermatol. 2011;64(4):793–795. doi: 10.1016/j.jaad.2010.05.008. [DOI] [PubMed] [Google Scholar]
- 6.Yentzer BA, Wood AA, Sagransky MJ, et al. An Internet-based survey and improvement of acne treatment outcomes. Arch Dermatol. 2011;147(10):1223–1224. doi: 10.1001/archdermatol.2011.277. [DOI] [PubMed] [Google Scholar]
- 7.Wang A, Armstrong A, Schupp CW, Wu J. Randomized controlled trial examining effectiveness of a novel personalized interactive health care education tool for acne patients (MyPACE) J Am Acad Dermatol. 2013;4(1):AB18. [Google Scholar]
- 8.Farmer KC. Methods for measuring and monitoring medication regimen adherence in clinical trials and clinical practice. Clin Ther. 1999;21(6):1074–1090. doi: 10.1016/S0149-2918(99)80026-5. [DOI] [PubMed] [Google Scholar]
- 9.MacLaughlin EJ, Raehl CL, Treadway AK, Sterling TL, Zoller DP, Bond CA. Assessing medication adherence in the elderly: which tools to use in clinical practice? Drugs Aging. 2005;22(3):231–255. doi: 10.2165/00002512-200522030-00005. [DOI] [PubMed] [Google Scholar]
- 10.Pawin H, Beylot C, Chivot M, et al. Creation of a tool to assess adherence to treatments for acne. Dermatology. 2009;218(1):26–32. doi: 10.1159/000165628. [DOI] [PubMed] [Google Scholar]
- 11.Marazzi P, Boorman GC, Donald AE, Davies HD. Clinical evaluation of Double Strength Isotrexin versus Benzamycin in the topical treatment of mild to moderate acne vulgaris. J Dermatolog Treat. 2002;13(3):111–117. doi: 10.1080/09546630260199460. [DOI] [PubMed] [Google Scholar]
- 12.Cunliffe WJ, Fernandez C, Bojar R, Kanis R, West F, Zindaclin Clinical Study Group An observer-blind parallel-group, randomized, multicentre clinical and microbiological study of a topical clindamycin/zinc gel and a topical clindamycin lotion in patients with mild/moderate acne. J Dermatolog Treat. 2005;16(4):213–218. doi: 10.1080/09546630500281957. [DOI] [PubMed] [Google Scholar]
- 13.Zaghloul SS, Cunliffe WJ, Goodfield MJ. Objective assessment of compliance with treatments in acne. Br J Dermatol. 2005;152(5):1015–1021. doi: 10.1111/j.1365-2133.2005.06357.x. [DOI] [PubMed] [Google Scholar]
- 14.Balkrishnan R, Kulkarni AS, Cayce K, Feldman SR. Predictors of healthcare outcomes and costs related to medication use in patients with acne in the United States. Cutis. 2006;77(4):251–255. [PubMed] [Google Scholar]
- 15.Yentzer BA, Alikhan A, Teuschler H, et al. An exploratory study of adherence to topical benzoyl peroxide in patients with acne vulgaris. J Am Acad Dermatol. 2009;60(5):879–880. doi: 10.1016/j.jaad.2008.11.019. [DOI] [PubMed] [Google Scholar]
- 16.Qudah I, Leijdekkers P, Gay V. Using mobile phones to improve medication compliance and awareness for cardiac patients; Proceedings of the 3rd International Conference on Pervasive Technologies Related to Assistive Environments, PETRA 2010; Samos, Greece. June 23–25 2010. [Google Scholar]
- 17.Lester RT, Ritvo P, Mills EJ, et al. Effects of a mobile phone short message service on antiretroviral treatment adherence in Kenya (WelTel Kenya1): a randomised trial. Lancet. 2010;376(9755):1838–1845. doi: 10.1016/S0140-6736(10)61997-6. [DOI] [PubMed] [Google Scholar]
- 18.Pop-Eleches C, Thirumurthy H, Habyarimana JP, et al. Mobile phone technologies improve adherence to antiretroviral treatment in a resource-limited setting: a randomized controlled trial of text message reminders. AIDS. 2011;25(6):825–834. doi: 10.1097/QAD.0b013e32834380c1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Balato N, Megna M, Di Costanzo L, Balato A, Ayala F. Educational and motivational support service: a pilot study for mobile-phone-based interventions in patients with psoriasis. Br J Dermatol. 2013;168(1):201–205. doi: 10.1111/j.1365-2133.2012.11205.x. [DOI] [PubMed] [Google Scholar]
- 20.Stoner SA, Hendershot CS. A randomized trial evaluating an mHealth system to monitor and enhance adherence to pharmacotherapy for alcohol use disorders. Addict Sci Clin Pract. 2012;7(1):9. doi: 10.1186/1940-0640-7-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Jan RL, Wang JY, Huang MC, Tseng SM, Su HJ, Liu LF. An internet-based interactive telemonitoring system for improving childhood asthma outcomes in Taiwan. Telemed J E Health. 2007;13(3):257–268. doi: 10.1089/tmj.2006.0053. [DOI] [PubMed] [Google Scholar]
- 22.Gustafson D, Wise M, Bhattacharya A, et al. The effects of combining Web-based eHealth with telephone nurse case management for pediatric asthma control: a randomized controlled trial. J Med Internet Res. 2012;14(4):e101. doi: 10.2196/jmir.1964. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Elkjaer M, Shuhaibar M, Burisch J, et al. E-health empowers patients with ulcerative colitis: a randomised controlled trial of the web-guided ‘Constant-care’ approach. Gut. 2010;59(12):1652–1661. doi: 10.1136/gut.2010.220160. [DOI] [PubMed] [Google Scholar]
- 24.Frangou S, Sachpazidis I, Stassinakis A, Sakas G. Telemonitoring of medication adherence in patients with schizophrenia. Telemed J E Health. 2005;11(6):675–683. doi: 10.1089/tmj.2005.11.675. [DOI] [PubMed] [Google Scholar]