

Abstract
Minimal tooth preparation is required for porcelain laminate veneers, but interim restorations are a must to protect their teeth against thermal insult, chemical irritation, and to provide aesthetics. Cement remaining after the removal of the provisional restoration can impair the etching quality of the tooth surface and fit and final bonding of the porcelain laminate veneer. This in vitro study examined the tooth surface for remaining debris of cement after removal of a provisional restoration. Determine the presence of cement debris on prepared tooth surface subsequent to the removal of provisional restoration. Determine the cement with the least residue following the cleansing procedures. Determine the effect of smear layer on the amount of residual luting cement. Eighty-four extracted natural anterior teeth were prepared for porcelain laminate veneers. For half of the teeth, the smear layer was removed before luting provisional restorations. Veneer provisional restorations were fabricated and luted to teeth with six bonding methods: varnish combined with glass ionomer cement (GIC), varnish combined with resin modified GIC, varnish, spot etching combined with dual-cure luting cement, adhesive combined with GIC, adhesive combined with resin modified GIC, and adhesive, spot etching combined with dual-cure luting cement. After removal of provisional restorations 1 week later, the tooth surface was examined for residual luting material with SEM. Traces of cement debris were found on all the prepared teeth surfaces for all six groups which were cemented with different methods. Cement debris was seen on teeth subsequent to the removal of provisional’s. Dual-cure cement had the least residue following the cleansing procedures. Presence of smear layer had no statistical significance in comparison with cement residue. With the use of adhesive the cement debris was always found to be more than with the use of varnish. GIC showed maximum residual cement followed by dual-cure.
Keywords: Porcelain laminates veneers, Luting cements, Scanning electron microscope (SEM)
Introduction
The introduction of porcelain laminates by Pincus in the 1930 s ushered a new era in the treatment of aesthetic restorations. Their present day applications have evolved greatly. Laminates are a conservative alternative to full coverage crowns for improving the appearance of an anterior tooth. The long time success of porcelain laminate veneers depends on careful case selection, design of and meticulous tooth preparation, laboratory fabrication and adhesive bonding procedures. The need for temporization of tooth preparation in porcelain laminate veneers is advocated for the unchanged patient appearance; and for the overall success of the restoration. Subsequent to the removal of provisional restorations, debris of the temporary cement remains on the prepared tooth surfaces. The presence of this debris hinders the maximum cementing ability of the final cement and hence there is always the need to find out the extent of cement left after the removal of the provisional restoration. There are few documented evidences which support the presence or absence of cement debris after removal of provisional restorations and have any effect on bonding of porcelain laminate veneers. Hence the present study was designed to analyze the prepared tooth surfaces and evaluate the presence of cement debris with the help of scanning electron microscope following the removal of the provisional restorations.
Methodology
Eighty-four intact human central incisors were individually mounted, to a level just below the cemento-enamel junction, in an acrylic base in an upright position. They were randomly divided into six groups, based on luting method, which has 14 teeth in each group, and each group will be further divided into sub-groups consisting of seven teeth in each sub-group.
Grouping is done based on the following criteria:
- Group 1 (A)
Prepared tooth surface treated with varnish and provisional cementation done using luting glass ionomer cement (GIC) with smear layer intact.
- Group 1 (B)
Prepared tooth surface treated with varnish and provisional cementation done using luting GIC after smear layer was removed.
- Group 2 (A)
Prepared tooth surface treated with varnish and provisional cementation done using resin modified GIC with smear layer intact.
- Group 2 (B)
Prepared tooth surface treated with varnish and provisional cementation done using resin modified GIC after smear layer was removed.
- Group 3 (A)
Prepared tooth surface treated with varnish and provisional cementation done using dual cure luting cement with smear layer intact.
- Group 3 (B)
Prepared tooth surface treated with varnish and provisional cementation done using dual cure luting cement after smear layer was removed.
- Group 4 (A)
Prepared tooth surface treated with adhesive and provisional cementation done using luting GIC with smear layer intact.
- Group 4 (B)
Prepared tooth surface treated with adhesive and provisional cementation done using luting GIC after smear layer was removed.
- Group 5 (A)
Prepared tooth surface treated with adhesive and provisional cementation done using resin modified GIC with smear layer intact.
- Group 5 (B)
Prepared tooth surface treated with adhesive and provisional cementation done using resin modified GIC after smear layer was removed.
- Group 6 (A)
Prepared tooth surfaces treated with adhesive and provisional cementation done using dual cure luting cement with smear layer intact.
- Group 6 (B)
Prepared tooth surface treated with adhesive and provisional cementation done using dual cure luting cement after smear layer was removed.
To evaluate whether the smear layer may have any influence on the remaining cement debris on the tooth surface, two sub-groups were formed for each method.
In sub-groups A the smear layer was not removed, in sub-groups B the smear layer was removed before luting the provisional restoration. To remove smear layer the prepared tooth was treated with cotton pellets soaked with EDTA–sodium salt solution (Nice Chemicals Pvt. Ltd.) for 60 s. All the six groups were assigned a standard tooth preparation for receiving porcelain laminate veneers.
Cementation
The teeth were taken out of distilled water at the time of provisional cementation and each provisional was cemented at a time.
For cementation of the provisional’s three different luting cements were used, GIC Type-I (Ketac Cem™, 3 M ESPE), resin modified cement (Rely X™ LUTE, 3 M ESPE), and dual cure composite (Calibra, Densply Caulk). All the teeth were grouped depending upon the removal and non-removal of smear layer, teeth treated with bifluoride-12 varnish (Voco, Germany) and bonding agent (adhesive) that has been used (Calibra, Densply Caulk).
The cementation was carried out using the manufacturer’s instruction in the following manner.
Group 1, 2, and 3 were treated with varnish and cemented with GIC Type-I, resin modified cement, and dual cure composite.
With the tooth in group 1 (A) following procedures were followed. The tooth surface was cleaned with the help of Pele Tim foam pellets, and bifluoride 12 resp was applied and allowed to soak in for 10–20 s. After the tooth surface was treated with varnish the recommended powder-to-liquid mixing ratio of 3.8:1 w/w, was used, and mixing was done under room temperature, and then provisional’s were loaded with cement that had to be cemented.
With the teeth in group 1 (B) the same above procedure was followed except the teeth were treated with EDTA to remove the smear layer before cementation.
With tooth in the group 2 (A) following procedures were followed. After the tooth was treated with varnish, the tooth was left to dry for 10–20 s. For cementation work, thin layer of cement was loaded into the provisional’s that had to be cemented and seated in place with light pressure. Excess cement was removed after 2 min.
With the teeth in group 2 (B) the same above procedures were followed except the teeth were treated with EDTA to remove the smear layer before cementation.
With tooth in group 3 (A) following procedures were followed, after the tooth was treated with varnish, the tooth was left to dry for 10–20 s. For cementation work, the internal surface of the provisional restoration was thoroughly cleaned with water spray and air dry and the coupling agent applied to the provisional restoration and the tooth surface on the incisal one third of the tooth, a spot with average diameter of 2.5 mm was etched for 30 s, with 37 % phosphoric acid gel and rinsed for 10 s and blot dried to keep away moisture. A dimple was created opposite to the etched spot in the veneer provisional restoration. The desired amount of the cement was dispensed on to the prepared provisional’s, and loaded in place. Excess cement was removed from gingival margin with a blunt instrument and only the gingival margin was light cured to tack the provisional restoration in place and then finally the provisional restoration on the whole was cured for 20 s each from facial, lingual, and proximal surfaces.
With the teeth in group 3 (B) the same above procedures were followed except that the teeth were treated with EDTA to remove smear layer before cementation.
The same procedure was used for the teeth in group 4, 5, and 6; that have been treated with adhesive. After the cementation procedure the teeth were stored in saline at a temperature of 37 °C. One week later, the provisional restorations were removed with an excavator; parts of temporary cement were visible on the tooth preparation surfaces of all teeth. However, these particles were partly removed with the excavator. According to the clinical procedures, specimens were polished with pumice until no cement particles were visible macroscopically. Teeth were gold coated in a sputter to make the specimens electrically conductive for scanning electron microscope examination and evaluated under 15×, 50×, and 100× levels of magnification.
Statistical Analysis
The hypothesis, whether there is an association between the methods group 1, 2, 3, 4, 5, 6, and the cement particles, was tested with the generalization of χ2 test (r × c test). In addition, to determine whether the distribution of samples within the sub-groups 1A and B, 2A and B, 3A and B, 4A and B, 5A and B, 6A and B was independent of cement debris, Fisher’s test was applied.
Results
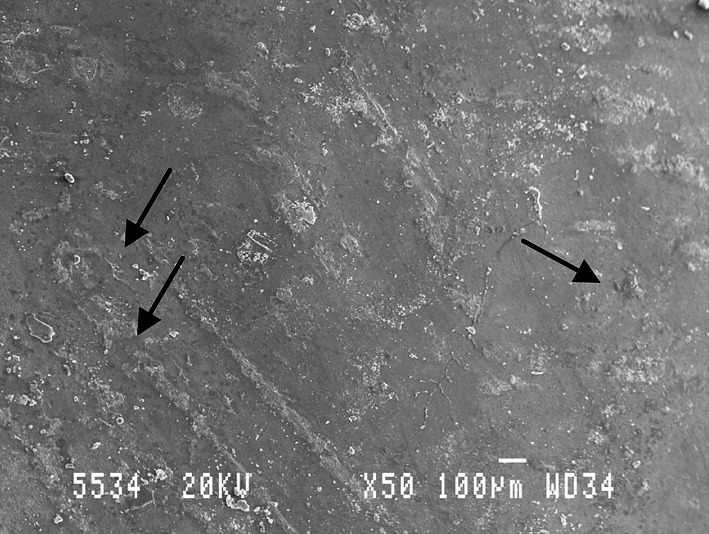
SEM examination revealed that for group 1 (varnish + GIC Type-I) 12 out of 14 specimens exhibit parts of cement that present over the prepared surface (Fig. 1a). The cement residual appeared flattened (Fig. 1b) as a result of polishing with pumice and water but were not completely removed. The resin modified GIC, cemented on the teeth (14) subjected to group 2; covered most of the tooth surface, 10 out of 14 teeth that were examined has shown the cement residual (Fig. 2). Of (14) specimens of group 3, out of 14 teeth only three teeth showed cement residual or varnish on the prepared tooth surface.(Figs. 3a, b) clean prepared tooth surface has been achieved.
Fig. 1.
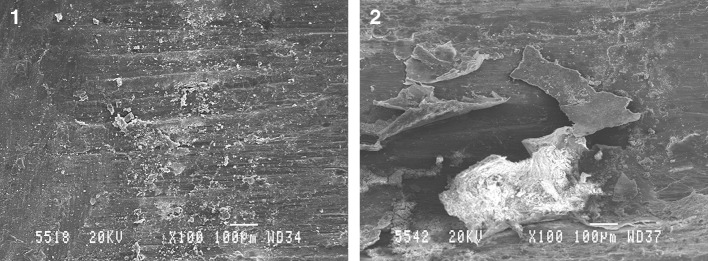
SEM picture showing residual cement, GIC Type-I group 1 (A, B)
Fig. 2.
SEM picture showing cement adhered in roughened areas in group 2 (A)
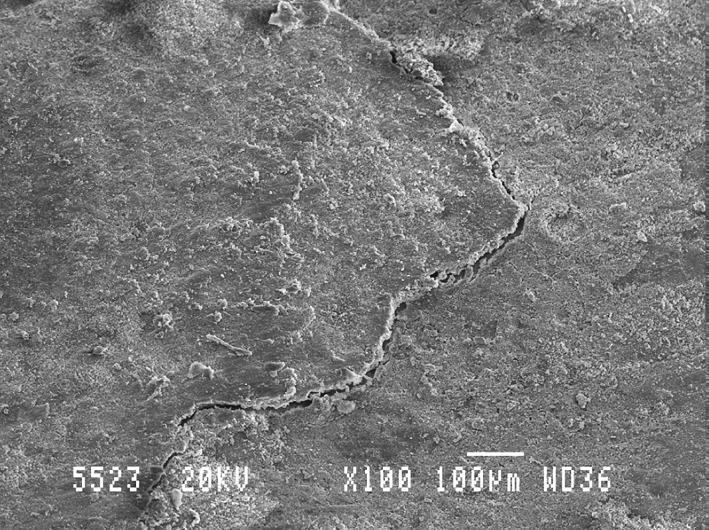
Fig. 3.
SEM picture showing cement reminents present only in area where the tooth preparations are rough in group 3 (A, B)
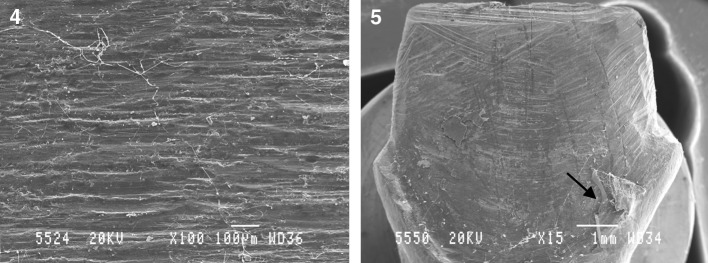
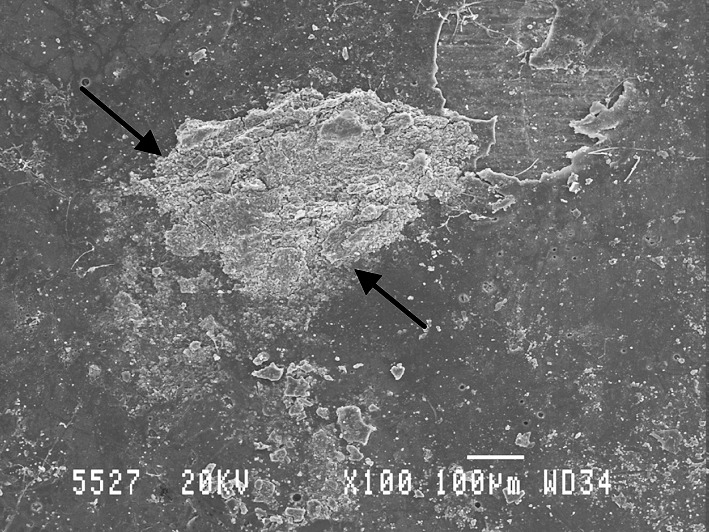
For group 4 (adhesive + GIC Type-I) 13 of 14 specimens showed cement residual on the tooth surface, the specimens showed flattened remains (Fig. 4) as a result of cleansing procedures that had been carried out, but complete removal of the cement was not achieved. In the group 5, specimens (adhesive + resin modified GIC) which covered most of the prepared tooth surface, 11 of 14 specimens showed a significant amount of remains of adhesive that adhered only to the roughened tooth preparation. On the other hand i.e., the specimens in the group 2, showed no remains of varnish on the prepared tooth surface, and in the last and final group 6 (adhesive + dual cure composite) only 5 specimens out of 14 examined showed minute remains of adhesive that adhered only to the surface were the surface was roughened while tooth cutting (Fig. 5). However, these areas could not be detected on the smoothened margins of the tooth preparation. On the contrary, in the group 3, the specimens did not show any varnish or composite on the prepared tooth surface (Fig. 3a).
Fig. 4.
SEM picture showing bulk of cement present in some areas even after the cleansing procedures were carried out in group 4 (A)
Fig. 5.
SEM picture showing areas of adhesive in group 6, visible as black spots on the roughened areas of prepared surfaces
Tables 1 and 2 presents the results of the study. A total of 56 specimens (66.67 %) exhibited residual luting material, whereas 28 specimens (33.33 %) showed no traces of luting material.
Table 1.
Fisher exact test
| Class 1 | Class 2 | Total | |
|---|---|---|---|
| Sample 1 | A | B | a + b |
| Sample 2 | C | D | c + d |
| Total | a + c | b + d | n |
Table 2.
Comparison of remaining of cement between 6 groups
| Groups | Total | Remaining of cement | 95 % CI (No) | |
|---|---|---|---|---|
| Present | Absent | |||
| Group 1 | 14 | 12 (85.7 %) | 2 (14.3 %) | 4.01–39.94 |
| Group 2 | 14 | 10 (71.4 %) | 4 (28.7 %) | 11.72–54.55 |
| Group 3 | 14 | 3 (21.4 %) | 11 (78.6 %) | 52.41–92.43 |
| Group 4 | 14 | 13 (92.9 %) | 1 (7.1 %) | 1.27–31.47 |
| Group 5 | 14 | 11 (78.6 %) | 3 (21.4 %) | 7.57–47.59 |
| Group 6 | 14 | 5 (35.7 %) | 9 (64.3 %) | 38.76–83.67 |
| Inference | Group 3 (varnish + dual cure) had significantly more number of specimens with out cement debris compared to other groups, varnish and adhesive (P < 0.001) | |||
Statistical Methods
95 % confidence interval has been used to find the significance of proportion of remaining cement ‘No’, χ2/Fisher exact test has been used to find the significance of proportion of remaining of cement between the sub groups.
1. χ2 test
-
where Oi is observed frequency and Ei is expected frequency
2. Fisher Exact Test
Fisher exact test statistic =

3. 95 % Confidence Interval, P ± 1.96* SE (P), where SE (P) is the standard error of proportion =
4. Significant figures
+Suggestive significance 0.05 < P < 0.10
* Moderately significant 0.01 < P ≤ 0.05
** Strongly significant P ≤ 0.01
Statistical Software
The statistical software namely SPSS 11.0 and Systat 8.0 were used for the analysis of the data and Microsoft word and Excel have been used to generate graphs, tables, etc.
Study Design
A comparative study with 84 teeth divided into six groups, each with 14 teeth is undertaken to study the significance of remaining of cement.
Discussion
The use of porcelain laminate veneers for conservative esthetic restorations of anterior teeth is a new treatment option. Porcelain veneers are claimed to be durable restorations with superior esthetic properties for appropriate indications and for adequately selected patients.
The success of porcelain veneers is greatly determined by the strength and durability of the formed bond between three different components of the bond veneer complex, namely the tooth surface, the luting agent, and the porcelain veneer.
Dumfahrt [1] proposed that many patients treated with porcelain laminate veneers expect to receive interim restorations that provide acceptable esthetics, comfort, and protection. This demand can only be met by provisional restorations that adhere to the prepared teeth by cement because no primary retention form is achieved during tooth preparation. The cementation technique of provisional restoration can affect the quality of the final bonding of porcelain laminate veneers.
There have been few studies accounting for the temporary cementation techniques and fabrication of provisionals [2–4] some on effects of using dentin desensitizers, and adhesives for cementation [5, 6] and few studies on retention of provisional crowns fabricated with different materials with use of different luting cements [7], but few documented evidence is present for the effects of provisional restoration techniques on the final bonding of the porcelain laminate veneers. Hence this study is designed to study the effects of different cements and cementation techniques on the bonding of porcelain laminate veneers. This study also determines and compares the amount of cement debris present on the prepared tooth surface after the provisional were removed followed by cleansing techniques and which cement has least residual left on the prepared tooth surface.
Statistical differences were analyzed by using 95 % confidence interval and Fisher exact test. 95 % confidence interval is used to find out the upper and lower limits of the interval that has to be estimated. They are called confidence interval because they are determined in accordance with a specified or conventional level of confidence, that these limits will infact include the parameter being estimated. There fore in general, after we do a significance test and reject null hypothesis that a mean is really the same as an expected mean, we then wish to estimate confidence interval for the true value. Some times we have data that can be summarized in a 2×2 contingency table, but these data are derived from very small samples. The χ2 test is not an appropriate method of analysis if minimum expected frequency requirements are not met. A test that may be used when the size requirements of the χ2 test are not met, the test is called as Fisher exact test. It is called exact because, if desired, it permits us to calculate the exact probability of obtaining the observed results or results that are more extreme.
Eighty-four intact human central incisors were individually mounted, to a level just below the cemento-enamel junction, in an acrylic base in an upright position. They were randomly divided into six groups, based on luting method, which has fourteen teeth in each group, and each group will be further divided into sub-groups consisting of seven teeth in each sub-group. A standard veneer preparations were made on the labial surfaces of all the teeth, and once the preparation got over the teeth were treated with varnish that is in group 1, 2, and 3 and cemented with GIC Type-I, resin modified GIC, and dual-cure simultaneously. Teeth in groups 4, 5, and 6 were treated with adhesive which is also a dentin protector and cemented with the luting cements used in this study and were stored in saline for 1 week, the provisionals were removed and cleansing procedures were carried out to make sure that all the cement debris is removed macroscopically and then were examined under SEM. The amount of cement residual left over on the prepared tooth surface in subsequent to the removal of provisional restorations were observed and determined which cement left least residual on the tooth surface and whether the presence or absence of smear layer had any significance.
In the present study, it is seen that all the luting cements used left cement residual on the tooth surface no matter whether smear layer was removed or left intact. These results are in agreement with the study made by Herbert Dumfahrt and Georg Gobel [1]. Where they stated that traces of cement debris were found in provisionally prepared teeth for all the three methods used and the presence of smear layer caused less distinction between the methods. Sufficient adhesion of provisional restorations can be achieved initially but minute debris that persisted after polishing, documented by SEM, can impair etching and final bonding of the porcelain laminate veneers. Clinical experience has shown that provisional restorations may debond because of solubility and the opacity of cement and compromise esthetics.
The results from the present study showed application of provisional restoration with GIC, showed cement residual on the prepared tooth surface even after polishing, documented by scanning electron microscope. (Table 3; Graph 3) But GIC when exposed to water in the initial stages of setting reaction the cement gets eroded because of water absorption. Water changes the setting reaction of the GIC forming cations are washed out and water is absorbed, leading to erosion. In this study all precaution were taken while seating the provisional restorations. Removal of smear layer showed a difference in the specimens which had cement residual on them. Specimens in which smear layer is intact, showed less amount of cement residual on the tooth surface when compared with those in which smear layer has been removed and when confidence interval used to find out significance of presence or absence of smear layer it shows removal and non-removal of smear layer had no significance. Luting of provisional’s with GIC along with adhesive showed more specimens with cement residual than those treated with varnish (group 1). Even in group 2 the presence or removal of smear layer had made no much difference.
Table 3.
Comparison of residual cement between 6 sub-groups
| Groups | Subgroups | Total | Remaining of cement | P value | |
|---|---|---|---|---|---|
| Present | Absent | ||||
| Group 1 | A | 7 | 5 (71.47 %) | 2 (28.6) | 0.462 |
| B | 7 | 7 (100.0 %) | 0 | ||
| Group 2 | A | 7 | 6 (85.7 %) | 1 (14.3 %) | 0.559 |
| B | 7 | 4 (57.1 %) | 3 (42.9 %) | ||
| Group 3 | A | 7 | 1 (14.3 %) | 6 (85.7 %) | 0.867 |
| B | 7 | 2 (28.6 %) | 5 (71.4 %) | ||
| Group 4 | A | 7 | 7 (100.0 %) | 0 | 0.909 |
| B | 7 | 6 (85.7 %) | 1 (14.3 %) | ||
| Group 5 | A | 7 | 6 (85.7 %) | 1 (14.3 %) | 0.867 |
| B | 7 | 5 (71.4 %) | 2 (28.6 %) | ||
| Group 6 | A | 7 | 4 (57.1 %) | 3 (42.9 %) | 0.266 |
| B | 7 | 1 (14.3 %) | 6 (85.7 %) | ||
Graph 3.

Showing the percentage distribution of residual of cement ‘No’ [10, 11]
Varnishes are primarily used to protect the pulp from chemical irritation by reducing the permeability of the exposed dentine. Irritations may come directly from the luting material as with luting agents. Varnishes aids in reduction of post operative sensitivity when applied to dentinal surfaces under newly inserted restorations. Varnishes are most popular because they are convenient to use. They can be applied rapidly and they dry instantly. In addition they are applied in thin coat and therefore do not affect the structural strength of the restoration [5]. Bi-fluoride 12 varnish was used in this study, it is fast drying which adheres well to the dry tooth enamel and dentine and can form a water light protective film insulating against thermal and chemical influences. Obviously, the result of this study cannot accurately predict the in vivo performances of the varnish because of the complexity of the actual conditions in the mouth. But the testing methods, however; hoped that the conclusions drawn could still be closely related to actual clinical performances.
In this study, the teeth in group 2 and 5, were cemented with resin modified GIC, the only difference in the properties between GIC and a resin modified GIC is the micro mechanical adhesion with the under laying tooth structure and that is achieved following etching. For the better adhesion between the luting cement and the tooth surface it is suggested to remove smear layer, which in turn develop maximum ion-exchange adhesion, that helps to expose dentinal tubules and remove dentine plugs that are obliterating lumen, but when cementation of the crown possibilities of developing hydraulic pressure, which may allow penetration of polyacrylate acid into the tubules, leading to undue irritation to the pulp tissue and post insertion sensitivity. So it is desirable to seal the dentine surface rather than removing the smear layer. But in the present study, surface treated with varnish and intact smear layer showed more number of specimens with residual cement and it was more in group 5 when compared, in which the surface was treated with adhesive (Graph 2), but the presence or removal of smear layer had shown no much significant difference on the presence or absence of residual cement. (Table 3; Graph 3)
Graph 2.

Shows cement residual percentage between varnish and adhesive treated teeth with three different luting cements
In the present study, the results indicate that there were no significant difference in retention obtained with the luting agents and this was tested by removing the provisional restorations only with the help of an excavator. That means the amount of cement residual on the tooth surface can effect the final cementation of porcelain laminate veneers. In a well designed study, Lepe et al. [7] compared the retention properties of two provisional resin materials and four temporary luting agents, at 24 h. The marginal fit of composite provisional restoration is superior to that of poly methyl methacrylate, but also stated that, it was not the only factor affecting the retention of the crown. Because of amount of polymerization shrinkage, provisional restorations made with poly methyl methacrylate resin may have tighter fit than those made with composite. Because the shrinkage is volumetric, it may influence over all fit of the restoration on the axial walls. The powder/liquid ratio of the cement mix effects the physical properties of the set cement, in particular, its compressive strength, which in most situations will result in increase cement retention.
The permeability of dentine to adhesive agents is of crucial importance in obtaining good dentinal bonding. In those systems that remove the smear layer, the opportunity exists for resin to infiltrate both tubules and inter tubular dentine. Resin penetration into tubules can effectively seal the tubules and can contribute to bond strength if the resin bonds to the tubule wall. Adhesive restorations better transmit and distribute functional stresses across the bonding interface to the tooth, with the potential to reinforce weakened tooth structure.
In direct restorative procedures usually require temporary restoration for protection of the pulp and for restoring the patient aesthetics and functional needs. Acid etched technique, composite luted indirect provisional restoration [8] resulted in composite bulk adhering to etched enamel. This bulk can be removed only by instrumentation with great force or with the use of a bur [9]. Kurtz [9] described porcelain laminate veneers provisional restoration fabricated directly on the prepared tooth and etched enamel that were fractured from the teeth during removal. This approach risked enamel or tooth fracture and should be avoided.
In the present study, the provisional’s which were made indirectly were seated with dual-cure composite in groups 3 and 6, which showed significantly less residual cement than the other groups. This result was worse when the smear layer was removed before cementation procedures [1], traces of adhesive discovered on six specimens (85 %) of group 6 (B) indicating that this material can adhere to rough surfaces of prepared teeth if the smear layer is removed. (Tables 2, 3; Graphs 1, 3) In group 6 (A), where the smear layer was not removed, bonding of adhesive to the prepared tooth surface was not as strong as to the group 6 (B). The provisional restorations subjected to teeth that are treated with varnish and cemented with dual-cure cement were removed in bulk, which left a clean preparation for 11 of 14 teeth.
Graph 1.

Showing the percentage distribution of residual of cement between six groups
Smear layer produced by instrumentation should be removed, because bacteria may have dentinal tubules. Smear layer constitutes a negative influence as the sealing ability of the obturated tubules, since it is porous and weakly adherent interface between the luting material and dentinal wall. Takeda et al. [12], made a comparative study of removal of smear layer by three endodontic irrigants and two types of laser. When compared to laser, EDTA was not effective in removing smear layer but when compared to other irrigants, EDTA was affective in removal of smear layer. Guerisoli et al. [13], evaluated of smear layer removal by EDTAC and sodium hypochlorite with ultrasonic agitation. In which ultrasonic agitation, sodium hypochlorite associated with EDTAC removed the smear layer effectively. In the present study, comparing with all the groups in which smear layer was intact and in which smear layer was removed had made no significant difference, because all the groups showed cement residual whether it might be treated with varnish or with adhesive. (Table 2; Graph 3) comparing with all the groups that have been examined the group which showed least cement debris is group 3 and followed by group 6. (Table 1; Graphs 1, 2).
Summary and Conclusion
After the samples which were stored in saline for 1 week, the provisional’s were removed and cleansing procedures were carried out to make sure that all the cement debris is removed macroscopically and then were examined under SEM. The amount of cement residual left over on the prepared tooth surface in subsequent to the removal of provisional restorations were observed and determined which cement left least residual on the tooth surface and whether the presence or absence of smear layer had any significance. Within the limitations of the study the following conclusions could be derived:
Cement debris were seen on all prepared teeth subsequent to the removal of provisional’s.
Dual-cure cement had the least residue following the cleansing procedures.
Presence of smear layer had no statistical significance in comparison with cement residue.
With the use of adhesive the cement debris was always found to be more than with the use of varnish.
GIC showed maximum residual cement followed by dual-cure.
Contributor Information
G. Vinod Kumar, Phone: +919000160808, Email: valcun23@yahoo.com
T. Soorya Poduval, Phone: +919845034664
Bipin Reddy, Phone: +919845034664.
P. Shesha Reddy, Phone: +919845034664
References
- 1.Dumfahrt H, Gobel G. Bonding porcelain laminate veneer provisional restorations: an experimental study. J Prosthet Dent. 1999;82:281–285. doi: 10.1016/S0022-3913(99)70081-8. [DOI] [PubMed] [Google Scholar]
- 2.Rosenstiel SF, Gegauff AG. Effect of provisional cementing agents on provisional resins. J Prosthet Dent. 1988;59:29–33. doi: 10.1016/0022-3913(88)90102-3. [DOI] [PubMed] [Google Scholar]
- 3.Elledge DA, Hart JK, Schorr BL. A provisional restoration technique for laminate veneer preparation. J Prosthet Dent. 1989;62:139–142. doi: 10.1016/0022-3913(89)90299-0. [DOI] [PubMed] [Google Scholar]
- 4.Rada RE, Jankowski BJ. Porcelain laminate veneer provisionalization using visible light-curing acrylic resin. Quintessence Int. 1991;22:291–293. [PubMed] [Google Scholar]
- 5.Tjan AHL, Grant BE, Nemetz H. The efficacy of resin-compatible cavity varnishes in reducing dentin permeability to free monomer. J Prosthet Dent. 1987;57:179–185. doi: 10.1016/0022-3913(87)90143-0. [DOI] [PubMed] [Google Scholar]
- 6.Lewinstein I, Fuhrer N, Ganor Y. Effect of a fluoride varnish on the margin leakage and retention of luted provisional crowns. J Prosthet Dent. 2003;89:70–75. doi: 10.1067/mpr.2003.2. [DOI] [PubMed] [Google Scholar]
- 7.Lepe X, Bales J. D and Johnson G. H. Retention of provisional crowns fabricated from two materials with the use of four temporary cements. J Prosthet Dent. 1999;81:469–475. doi: 10.1016/S0022-3913(99)80016-X. [DOI] [PubMed] [Google Scholar]
- 8.Zalkind M, Hochman N. Laminate veneer provisional restorations: a clinical report. J Prosthet Dent. 1997;77:109–110. doi: 10.1016/S0022-3913(97)70220-8. [DOI] [PubMed] [Google Scholar]
- 9.Kurtz KS. Constructing direct porcelain laminate veneers provisionals. J Am Dent Assoc. 1995;126:653–656. doi: 10.14219/jada.archive.1995.0245. [DOI] [PubMed] [Google Scholar]
- 10.Rosner B (2000), Fundamentals of biostatistics, 5th edn, Duxbury
- 11.Reddy MV. Statistics for mental health care research. Bangalore: NIMHANS Publication; 2002. [Google Scholar]
- 12.Takeda FH, Harashima T, Kimura Y, Matsumoto K. A comparative study of the removal of smear layer by three endodontic irrigants and two types of laser. Int Endo J. 1999;32:32–39. doi: 10.1046/j.1365-2591.1999.00182.x. [DOI] [PubMed] [Google Scholar]
- 13.Guerisoli DMZ, Marchesan MA, Walmsley AD, Lumley PJ, Pecora JD. Evaluation of smear layer removal by EDTAC and sodium hypochlorite with ultrasonic agitation. Int Endo J. 2002;35:418–421. doi: 10.1046/j.1365-2591.2002.00488.x. [DOI] [PubMed] [Google Scholar]