

Abstract
Purpose
To assess the pain intensity of patients administered midazolam and fentanyl citrate before undergoing transrectal ultrasound-guided prostate biopsy.
Materials and Methods
This was a study in patients with different indications for prostate biopsy in whom 5 mg of midazolam and 50 µg of fentanyl citrate was administered intravenously 3 minutes before the procedure. After biopsy, pain was assessed by use of a visual analogue scale (VAS) in three stages: VAS 1, during probe introduction; VAS 2, during needle penetration into prostate tissue; and VAS 3, in the weeks following the exam. Pain intensity at these different times was tested with stratification by age, race, education, prostate volume, rebiopsy, and anxiety before biopsy. Pain was ranked according to the following scores: 0 (no pain), 1-3 (mild pain), 4-7 (moderate pain), and 8-10 (severe pain). Statistical analysis was performed by using Kruskal-Wallis and Wilcoxon two-tailed tests with a significance of 5%.
Results
Pain intensity was not influenced by any risk factors. The mean VAS 1 score was 1.95±1.98, the mean VAS 2 score was 2.73±2.55, and the mean VAS 3 score was 0.3±0.9, showing greater pain at the time of needle penetration than in other situations (VAS 2>VAS 1>VAS 3, p=0.0013, p=0.0001, respectively). Seventy-five percent of patients reported a VAS pain scale of less than 3.1 or mild pain.
Conclusions
Intravenous sedation and analgesia with midazolam and fentanyl citrate is a good method for reducing pain caused by prostate biopsy, even during probe insertion.
Keywords: Anesthesia and analgesia, Needle biopsy, Pain measurement, Prostate
INTRODUCTION
Prostate cancer is the most common solid tumor in men and is the second leading cause of death among cancers [1]. Diagnosis is performed through fragments obtained by ultrasound-guided transrectal prostate biopsy, which is usually performed on an outpatient basis. Many patients consider the procedure uncomfortable and painful; about 65% to 90% of patients report moderate to severe pain and 20% would not repeat the procedure [2]. Some of the factors that can cause pain during biopsy are anal discomfort generated by transducer insertion and needle penetration in the rectal wall, periprostatic tissue, and prostatic capsule [3]. The best means of analgesia for prostate biopsy has not yet been defined, and several techniques have been described, such as intrarectal lidocaine gel, anti-inflammatory drugs, periprostatic nerve block (PPNB), and sedoanalgesia [4-19].
Sedation and anesthetic agents are a good method for relieving pain during prostate biopsy. The drug used should preferably be rapidly metabolized, have few side effects, and, if necessary, be easily reversed. Anal distension during the introduction of the transducer is an important component in the mechanism of pain generated by the procedure. Other pain-relieving techniques do not act on this mechanism, thus justifying the use of sedation.
Fentanyl citrate is an opioid drug used in treating pain; it is characterized by rapid onset, short duration, and high efficiency. Its administration is intravenous, and its action is installed within 2-3 minutes, lasting about 30 minutes. It is used for sedation in combination with a benzodiazepine such as midazolam in endoscopic procedures. Midazolam is a sleep-inducing agent that can be administered intravenously, with rapid onset, short duration, and anterograde amnesia [20,21].
MATERIALS AND METHODS
The study was performed in patients from the Department of Urology, Botucatu Medical School, UNESP, after approval of the Ethics in Research Board. All participants signed an informed consent form. The inclusion criteria were as follows: abnormalities in the digital rectal examination suggesting prostate cancer, high prostate-specific antigen (PSA; >4.0 ng/mL in men over 55 years old and >2.5 ng/mL in men younger than 55 years old), PSA density greater than 0.15, and annual PSA increase greater than 0.75 ng/mL. Patients with bleeding disorders, anorectal disease (hemorrhoids, anal fissure, anal stenosis), urinary tract infection in treatment or diagnosed at the time of biopsy, spinal trauma, hypersensitivity to fentanyl citrate or midazolam, or who refused to provide written informed consent and were unable to answer the questionnaire were excluded from the study.
Some parameters were analyzed as risk factors for pain during biopsy, such as age, race, education level, serum PSA, free-PSA and the free-PSA/total PSA ratio, rebiopsy, biopsy indication, and prostate volume. Complications such as hypotension, hypoxia, hemorrhage, urinary retention, and vasovagal reaction were also recorded. The biopsy procedure was performed on an outpatient basis. A structured room with all the equipment required for urgent care and emergency care was necessary (oxygen supply, laryngoscope, endotracheal tubes, respirator, defibrillator, and drugs). All patients underwent cardiac monitoring, pulse oximetry, and blood pressure measurements [22]. Three minutes before the procedure, 50 µg of fentanyl citrate dissolved in 1 mL of distilled water and 5 mg of midazolam dissolved in a 1-mL distilled water bolus were administered in separate syringes intravenously in the upper left limb with a number 23 butterfly needle.
The procedure was performed with a 250-mL rectal enema and prophylaxis by administration of antibiotic ciprofloxacin 500 mg orally 2 hours before the procedure and after 8 hours. The procedure was performed with the use of a transrectal probe with the patient in the left lateral decubitus position with the thighs flexed. An 18-gauge, 25-cm automatic biopsy gun was used to obtain 16-core biopsies. Prostate volume was calculated by using the ellipsoid formula (height×width×length×0.52). After the procedure, the patients remained in the recovery room until they could be discharged. In the immediate biopsy recovery period, all patients were evaluated by a single investigator responsible for measuring the primary pain outcome by use of a visual analogue scale (VAS) [23]. The VAS was used to evaluate the pain generated by the transducer introduction (VAS 1) and the pain generated by biopsy (VAS 2). After 7 days, the patients were evaluated again for the presence of pain (VAS 3).
Pain was classified as follows: absence of pain, score of 0; mild pain, score of 0.1 to 3; moderate pain, score of 3.1 to 7; and severe pain, score from 7.1 to 10.
Data were collected by use of a Microsoft Excel spreadsheet (Microsoft Co., Redmond, WA, USA) and were analyzed by using SAS ver. 9.2 (SAS Institute Inc., Cary, NC, USA). Results were expressed as means and standard deviations (SDs) for age, PSA, prostate volume, and pain. Qualitative variables were described by frequency and percentage. To determine differences in pain levels among age, educational level, race, prostate volume, prebiopsy, rebiopsy, and anxiety, the Kruskal-Wallis test and Wilcoxon rank-sum test were used when comparing two or more than two samples, respectively. In all tests, the corresponding p-value of 5% was considered significant.
RESULTS
Biopsies were performed in 118 patients, and of these, 56 patients (47.9%) had undergone at least one procedure. The average age, total PSA, prostate volume, education level, and race of the patients are shown in Table 1. Of the 118 patients studied, 69 (58.4%) reported anxiety in the exam and 56 (47.4%) reported no anxiety.
TABLE 1.
Demographic characteristics of the patients
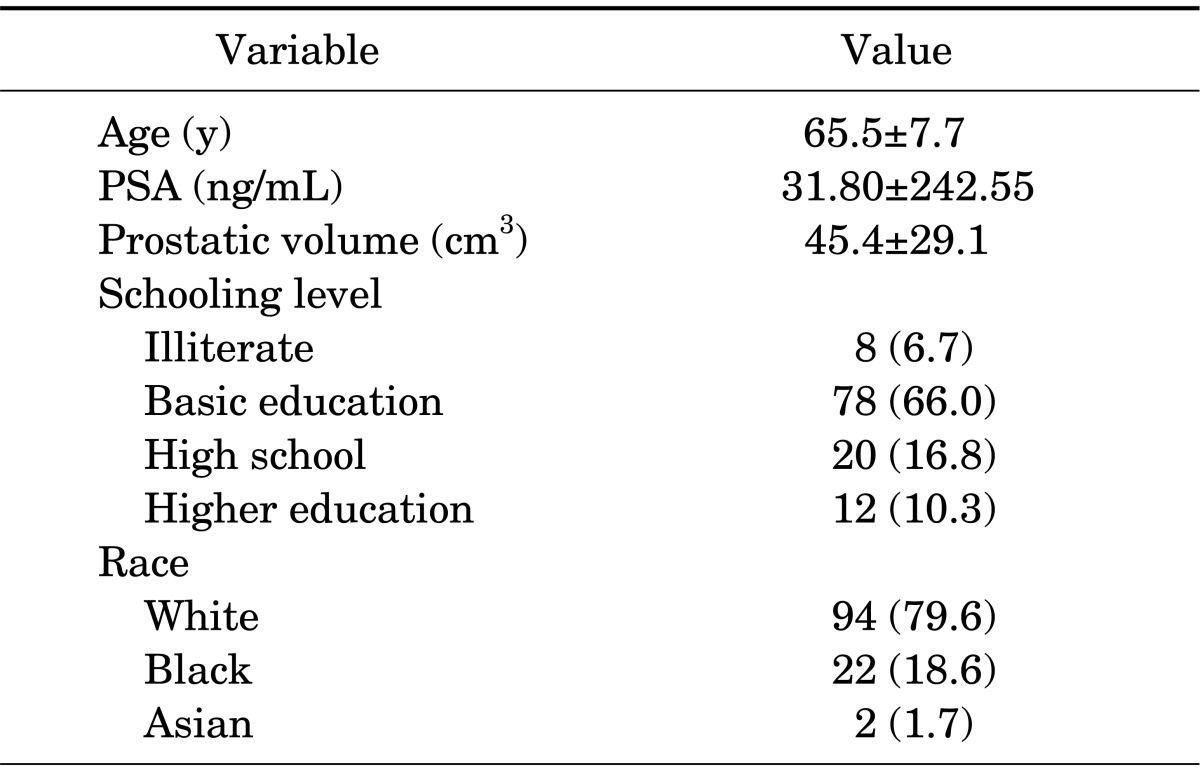
Values are presented as mean±standard deviation or number (%).
PSA, prostate-specific antigen.
The average (SD) pain VAS 1 was 1.95±1.98 mm. At this time, 75% of the patients reported pain lower than 3.1 mm, or mild pain. Pain assessment during the introduction of the probe for biopsy (VAS 2) had a mean of 2.73±2.55 mm. At the time of the VAS 2, 75% of the patients reported pain lower than 4.5 and 50% reported pain lower than 1.5, or mild pain. Just 5.4% and 11% of the patients reported severe pain at VAS 1 and VAS 2, respectively. Evaluation of pain in the weeks following the biopsy (VAS 3) had a mean of 0.3±0.9 mm, whereas 75% of patients reported no pain. There were huge differences among VAS 1, 2, and 3 with high significance (VAS 2>VAS 1>VAS 3, p=0.0013).
Pain intensity at different times (VAS 1, VAS 2, and VAS 3) was compared with stratification by age, race, educational level, and other possible influencing factors such as prostate volume, rebiopsy, prebiopsy anxiety, and prostate cancer diagnosis. None of these factors had a significant influence on the pain level with this kind of sedoanalgesia. These results are shown in Table 2. The main complications were rectal bleeding (21 patients, 17.7%), vasovagal reaction (5 patients, 4.2%), urinary retention (8 patients, 6.7%), urethral bleeding and fever (1 patient, 0.8%), pain (14 patients, 11.8%), hematuria (75 patients, 63.4%), and hemospermia (51 patients, 43.2%).
TABLE 2.
Pain intensity at different times according to age, race, schooling level, prostate volume, rebiopsy, anxiety, and prostate cancer
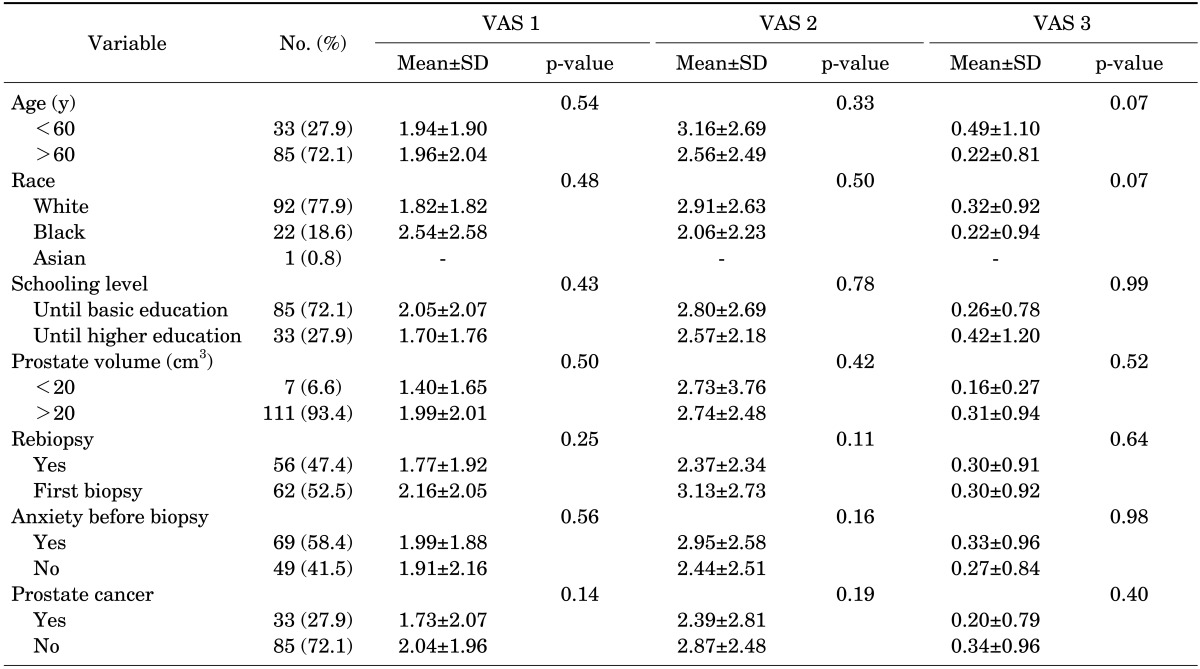
VAS, visual analogue scale; SD, standard deviation.
Of 14 patients who reported moderate to severe pain during the procedure, it was necessary to use a double dose to perform the procedure in 11 (78%). There were no respiratory or cardiac complications, even in elderly patients who required an additional dose of medication (10 mg midazolam and 100 µg fentanyl citrate).
DISCUSSION
With the introduction of serum PSA in prostate cancer screening, there has been a significant increase in the number of biopsies, which has consequently led to a better diagnosis [2]. A considerable number of patients consider the biopsy procedure uncomfortable and painful, however. About 65% to 90% of patients report pain of moderate to severe intensity, and 20% do not repeat the examination [3,12].
Sextant biopsy was considered the method of choice for many years, but nowadays it is recommended to obtain at least 12 fragments to increase the tumor diagnoses [24,25]. The high number of punctures increases the prostate cancer diagnosis, but pain, anxiety, and discomfort are proportional to the number of punctures. The main factors responsible for pain during the biopsy are anal discomfort generated by transducer insertion and as a result of the needle penetration in the rectal wall, prostatic capsule, and periprostatic tissue [11,16,17]. Other factors such as age, transducer size, and procedure time can affect pain intensity [26,27].
Some studies have shown that younger patients or patients with smaller prostates have more discomfort during the biopsy [26,27]. Additionally, prebiopsy anxiety or rebiopsy as a result of a prior biopsy procedure are mentioned as factors predisposing to a higher pain intensity [13,16]. We did not observe that these factors affected the pain scores, which may have been the result of the excellent analgesia and sedation obtained by the drugs used. In our research, there was no control group, because it is not ethical to perform this design without analgesia. Even if there were risk factors involved in providing pain relief, this method of sedoanalgesia alleviated pain regardless of the presence or absence of these factors. Thus, these factors were not important when using this type of procedure.
Although the best means of analgesia for prostate biopsy has not yet been defined, several techniques have been described in the literature. PPNB is the most widely used procedure [11-16]. Several studies have shown that one of the benefits of PPNB is to reduce pain safely in prostate biopsy. PPMB can be performed by the urologist on an outpatient basis. Because of these indicators, PPNB is considered the standard analgesia procedure for prostate biopsy [11].
However, patients still suffer significant emotional and physical discomfort before the procedure, which can increase the pain stimulus. Moreover, PPNB does not act in the pain mechanism generated by the anal stretching that occurs when the rectal probe is introduced. Thus, it cannot alleviate all pain during the procedure.
Therefore, we believe that the use of intravenous sedation and analgesia is the most effective method for controlling pain during prostate biopsy. This method of analgesia can optimize the benefits of the PPNB and may directly interfere in the anxiety and pain sensation caused by anal stretching from the transducer. These beneficial effects of intravenous sedation and analgesia are important considering that the number of prostate biopsies has been growing steadily, especially in economically active young patients, and also that biopsy may be repeated several times in the same patient including a larger number of fragments (16, 20, or 24 fragments).
The drug used should preferably be rapidly metabolized with few side effects and, if necessary, be easily reversed. We do not doubt that sedoanalgesia with the attendance of an anesthesiologist will have a higher cost than the cost of a urologist or radiologist performing the procedure alone. However, this kind of sedoanalgesia can be performed by the urologist in a structured room with a defibrillator, material for resuscitation, and airway intubation. Despite the small number of patients, there were no problems with the use of these drugs at this dose. In fact, the costs of sedoanalgesia and prostatic nerve block are similar. In our service, we do not work with anesthesiologists to perform sedation and analgesia. In the United Kingdom, it is common to use nitrous oxide [28]. However, the procedure requires the compulsory attendance of the anesthesiologist, which can be considered a drawback, because it increases the cost of the procedure. Moreover, owing to nausea and vomiting as side effects, the patients must stay in the recovery room for up to 4 hours after the procedure. With the use of midazolam and fentanyl citrate, the patients could leave the recovery room on average 30 minutes after the procedure, which facilitated its logistics.
Some studies have evaluated the use of midazolam and meperidine for sedation and analgesia for prostatic biopsy. Tobias-Machado et al. [18] conducted a randomized controlled trial comparing three different types of anesthesia (administration of 2% intrarectal lidocaine gel, PPNB, and sedation with a combination of midazolam and meperidine) to evaluate efficacy in reducing pain during prostate biopsy. In the PPNB group, 78.33% of the patients reported pain, with 86.7% reporting weak pain and only 3.33% reporting severe pain. No patient had unbearable pain, and compared with the control group, there was significant reduction in pain (p<0.001). In the group receiving sedation with midazolam and meperidine, 76% of patients reported some pain, and of these 81.6% had little or no pain; only 4.99% reported severe or unbearable pain. Compared with the control group, the pain reduction in the group receiving sedation with midazolam and meperidine was significant (p<0.001). The use of midazolam and meperidine significantly reduced pain without cardiac or respiratory complications [18].
Recently, Izol et al. [29] published a study that evaluated three different analgesia techniques on prostate biopsy. Pain intensity was assessed by VAS graded in three stages: during biopsy (VAS 1), immediately after the procedure (VAS 2), and 1 hour later (VAS 3). A total of 100 patients were randomized into 4 groups: group 1 (control), group 2 (periprostatic block with 2% lidocaine), group 3 (intrarectal lidocaine gel), and group 4 (sedation and analgesia with 2 mg midazolam and 2 µg/kg fentanyl intravenously). In the group receiving sedation and analgesia with midazolam and fentanyl, a decrease in pain intensity in these three conditions (VAS 1, VAS 2, and VAS 3) was observed. Groups 2 and 4 were statistically significant compared with the group that received intrarectal lidocaine gel and the gel control group (p=0.0001). There were no significant cardiorespiratory complications in any group. Of 100 patients undergoing the procedure, only 1 patient (belonging to the group that underwent periprostatic block) presented with hypotension, which was quickly treated. The study concluded that the association of midazolam with fentanyl and PPNB are effective and superior to the other techniques to relieve pain. The authors recommended sedoanalgesia only in patients who do not tolerate pain, in saturation biopsies, and in patients who are allergic to lidocaine.
In our study, the combination of midazolam and fentanyl citrate proved to be easy to apply, safe, and effective in reducing pain and discomfort both during and after the procedure. In our samples, cardiorespiratory complications were not observed. The association of these two drugs proved to be an excellent method of analgesia and sedation. Midazolam acts by promoting sedation, retrograde amnesia, and relaxation of the anal muscle tone, which is one of the mechanisms responsible for pain during the procedure. Fentanyl, in turn, is a potent opioid analgesic drug during and after the procedure. We noticed that after the procedure, when the patients were discharged, some of them did not remember having undergone it, which must be due to retrograde amnesia promoted by midazolam. It is important to emphasize that midazolam promotes only retrograde amnesia without compromising cognition, which did not interfere in the evaluation of pain after the procedure.
The evaluation of the patient before the procedure can be carried out in the questionnaire that is routinely given before the biopsy indication. In our previous experience, there is a contraindication to perform it in patients with low cardiac and respiratory reserve. The average time for patient recovery is either about 30 minutes or is not different from the care given to patients with the use of PPNB. Complications due to the use of these drugs are very rare with similar rates [16-19]. When complications do occur, they can be circumvented because the procedure is performed in an appropriate and structured place by providers professionally trained and qualified to treat them.
CONCLUSIONS
Intravenous sedation and analgesia with midazolam and fentanyl citrate is a good method to reduce the discomfort and pain caused by prostate biopsy, even during probe insertion.
Footnotes
The authors have nothing to disclose.
References
- 1.Siegel R, DeSantis C, Virgo K, Stein K, Mariotto A, Smith T, et al. Cancer treatment and survivorship statistics, 2012. CA Cancer J Clin. 2012;62:220–241. doi: 10.3322/caac.21149. [DOI] [PubMed] [Google Scholar]
- 2.Clements R, Aideyan OU, Griffiths GJ, Peeling WB. Side effects and patient acceptability of transrectal biopsy of the prostate. Clin Radiol. 1993;47:125–126. doi: 10.1016/s0009-9260(05)81188-2. [DOI] [PubMed] [Google Scholar]
- 3.Collins GN, Lloyd SN, Hehir M, McKelvie GB. Multiple transrectal ultrasound-guided prostatic biopsies: true morbidity and patient acceptance. Br J Urol. 1993;71:460–463. doi: 10.1111/j.1464-410x.1993.tb15993.x. [DOI] [PubMed] [Google Scholar]
- 4.Desgrandchamps F, Meria P, Irani J, Desgrippes A, Teillac P, Le Duc A. The rectal administration of lidocaine gel and tolerance of transrectal ultrasonography-guided biopsy of the prostate: a prospective randomized placebo-controlled study. BJU Int. 1999;83:1007–1009. doi: 10.1046/j.1464-410x.1999.00080.x. [DOI] [PubMed] [Google Scholar]
- 5.Issa MM, Bux S, Chun T, Petros JA, Labadia AJ, Anastasia K, et al. A randomized prospective trial of intrarectal lidocaine for pain control during transrectal prostate biopsy: the Emory University experience. J Urol. 2000;164:397–399. [PubMed] [Google Scholar]
- 6.Saad F, Sabbagh R, McCormack M, Peloquin F. A prospective randomized trial comparing lidocaine and lubricating gel on pain level in patients undergoing transrectal ultrasound prostate biopsy. Can J Urol. 2002;9:1592–1594. [PubMed] [Google Scholar]
- 7.Irer B, Gulcu A, Aslan G, Goktay Y, Celebi I. Diclofenac suppository administration in conjunction with lidocaine gel during transrectal ultrasound-guided prostate biopsy: prospective, randomized, placebo-controlled study. Urology. 2005;66:799–802. doi: 10.1016/j.urology.2005.04.053. [DOI] [PubMed] [Google Scholar]
- 8.Olmez G, Kaya S, Aflay U, Sahin H. Comparison of lornoxicam versus tramadol analgesia for transrectal prostate biopsy: a randomized prospective study. Int Urol Nephrol. 2008;40:341–344. doi: 10.1007/s11255-007-9297-4. [DOI] [PubMed] [Google Scholar]
- 9.Valero G, Gonzalez EU. Periprostatic anaesthesic infiltration for prostatic biopsy: a prospective, randomized, double blind and placebo-controlled study. Actas Urol Esp. 2005;29:550–552. doi: 10.1016/s0210-4806(05)73295-2. [DOI] [PubMed] [Google Scholar]
- 10.Nash PA, Bruce JE, Indudhara R, Shinohara K. Transrectal ultrasound guided prostatic nerve blockade eases systematic needle biopsy of the prostate. J Urol. 1996;155:607–609. [PubMed] [Google Scholar]
- 11.Autorino R, De Sio M, Di Lorenzo G, Damiano R, Perdona S, Cindolo L, et al. How to decrease pain during transrectal ultrasound guided prostate biopsy: a look at the literature. J Urol. 2005;174:2091–2097. doi: 10.1097/01.ju.0000181212.51025.06. [DOI] [PubMed] [Google Scholar]
- 12.Soloway MS, Obek C. Periprostatic local anesthesia before ultrasound guided prostate biopsy. J Urol. 2000;163:172–173. [PubMed] [Google Scholar]
- 13.Adamakis I, Mitropoulos D, Haritopoulos K, Alamanis C, Stravodimos K, Giannopoulos A. Pain during transrectal ultrasonography guided prostate biopsy: a randomized prospective trial comparing periprostatic infiltration with lidocaine with the intrarectal instillation of lidocaine-prilocain cream. World J Urol. 2004;22:281–284. doi: 10.1007/s00345-003-0386-4. [DOI] [PubMed] [Google Scholar]
- 14.Arguelles Salido E, Congregado Ruiz CB, Conde Sanchez JM, Ruiz Zafra V, Medina Lopez RA, Campoy Martinez P. Ultrasound guided transrectal prostatic biopsy and pain. Prospective randomized study comparing lubricant gel, lidocaine gel, and anesthetic blockage of the neurovascular bundles with 1% lidocaine. Arch Esp Urol. 2008;61:579–590. doi: 10.4321/s0004-06142008000500003. [DOI] [PubMed] [Google Scholar]
- 15.Pareek G, Armenakas NA, Fracchia JA. Periprostatic nerve blockade for transrectal ultrasound guided biopsy of the prostate: a randomized, double-blind, placebo controlled study. J Urol. 2001;166:894–897. [PubMed] [Google Scholar]
- 16.Barbosa RA, da Silva CD, Torniziello MY, Cerri LM, Carmona MJ, Malbouisson LM. A comparative study among three techniques of general anesthesia for ultrasound-guided transrectal prostate biopsy. Rev Bras Anestesiol. 2010;60:457–465. doi: 10.1016/S0034-7094(10)70057-X. [DOI] [PubMed] [Google Scholar]
- 17.Peters JL, Thompson AC, McNicholas TA, Hines JE, Hanbury DC, Boustead GB. Increased patient satisfaction from transrectal ultrasonography and biopsy under sedation. BJU Int. 2001;87:827–830. doi: 10.1046/j.1464-410x.2001.02221.x. [DOI] [PubMed] [Google Scholar]
- 18.Tobias-Machado M, Verotti MJ, Aragao AJ, Rodrigues AO, Borrelli M, Wroclawski ER. Prospective randomized controlled trial comparing three different ways of anesthesia in transrectal ultrasound-guided prostate biopsy. Int Braz J Urol. 2006;32:172–179. doi: 10.1590/s1677-55382006000200007. [DOI] [PubMed] [Google Scholar]
- 19.Song JH, Doo SW, Yang WJ, Song YS, Kim GW, Ku JH, et al. Value and safety of midazolam anesthesia during transrectal ultrasound-guided prostate biopsy. Korean J Urol. 2011;52:216–220. doi: 10.4111/kju.2011.52.3.216. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Kanto JH. Midazolam: the first water-soluble benzodiazepine. Pharmacology, pharmacokinetics and efficacy in insomnia and anesthesia. Pharmacotherapy. 1985;5:138–155. doi: 10.1002/j.1875-9114.1985.tb03411.x. [DOI] [PubMed] [Google Scholar]
- 21.Jin SJ, Jung JY, Noh MH, Lee SH, Lee EK, Choi BM, et al. The population pharmacokinetics of fentanyl in patients undergoing living-donor liver transplantation. Clin Pharmacol Ther. 2011;90:423–431. doi: 10.1038/clpt.2011.133. [DOI] [PubMed] [Google Scholar]
- 22.American Society of Anesthesiologists Task Force on Sedation and Analgesia by Non-Anesthesiologists. Practice guidelines for sedation and analgesia by non-anesthesiologists. Anesthesiology. 2002;96:1004–1017. doi: 10.1097/00000542-200204000-00031. [DOI] [PubMed] [Google Scholar]
- 23.Campbell WI, Lewis S. Visual analogue measurement of pain. Ulster Med J. 1990;59:149–154. [PMC free article] [PubMed] [Google Scholar]
- 24.Lopez-Corona E, Ohori M, Scardino PT, Reuter VE, Gonen M, Kattan MW. A nomogram for predicting a positive repeat prostate biopsy in patients with a previous negative biopsy session. J Urol. 2003;170(4 Pt 1):1184–1188. doi: 10.1097/01.ju.0000087451.64657.fa. [DOI] [PubMed] [Google Scholar]
- 25.de Jesus CM, Correa LA, Padovani CR. Complications and risk factors in transrectal ultrasound-guided prostate biopsies. Sao Paulo Med J. 2006;124:198–202. doi: 10.1590/S1516-31802006000400005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Westenberg AM, Cossar EH, Lorimer LB, Costello JP. The acceptability of transrectal ultrasound guided prostatic biopsy without anaesthesia. N Z Med J. 1999;112:231–232. [PubMed] [Google Scholar]
- 27.Han KS, Lee KH Korean Urologic Oncology Society Prostate Cancer Study Group. Factors influencing pain during transrectal ultrasonography-guided prostate biopsy. Prostate Cancer Prostatic Dis. 2008;11:139–142. doi: 10.1038/sj.pcan.4501004. [DOI] [PubMed] [Google Scholar]
- 28.McIntyre IG, Dixon A, Pantelides ML. Entonox analgesia for prostatic biopsy. Prostate Cancer Prostatic Dis. 2003;6:235–238. doi: 10.1038/sj.pcan.4500670. [DOI] [PubMed] [Google Scholar]
- 29.Izol V, Soyupak B, Seydaoglu G, Aridogan IA, Tansug Z. Three different techniques for administering analgesia during transrectal ultrasound-guided prostate biopsy: a comparative study. Int Braz J Urol. 2012;38:122–128. doi: 10.1590/s1677-55382012000100017. [DOI] [PubMed] [Google Scholar]