

Abstract
Purpose
To evaluate the efficacy and safety of tadalafil 5 mg once daily use in the treatment of erectile dysfunction (ED) after robot-assisted laparoscopic radical prostatectomy (RALP).
Materials and Methods
The study retrospectively evaluated 92 patients who underwent RALP at Dong-A University Hospital. The patients were surveyed by use of the abridged five-item version of the International Index of Erectile Function (IIEF-5) questionnaire, which was self-administered before surgery and at 6 months and 1 year after surgery. The 92 patients were classified into the tadalafil group (n=47) and the non-tadalafil group (n=45). Each group was then classified depending on the nerve-sparing (NS) procedure used: bilateral NS or unilateral NS.
Results
At 6 months, the total IIEF-5 scores of the tadalafil group and the non-tadalafil group were 10.0±3.4 and 7.0±4.0, respectively. At 1 year, the total IIEF-5 score in the tadalafil group was significantly greater than that in the non-tadalafil group (13.2±5.6 vs. 7.7±4.8, p<0.0001). Statistically significant improvements (p<0.05) were observed in the tadalafil group for all 5 domains of the IIEF-5 score, whereas in the non-tadalafil group there was no significant improvement in any of the domains at 1 year. The reported side effects were flushing (8.5%, n=4), headache (4.3%, n=2), and dizziness (2.1%, n=1).
Conclusions
In ED patients after NS RALP, a once-daily dose of tadalafil 5 mg was well tolerated and significantly improved EF compared with that in the non-tadalafil group.
Keywords: Erectile dysfunction, Once daily, Prostatectomy, Robotics, Tadalafil
INTRODUCTION
Radical prostatectomy (RP) is considered to be a standard curative procedure for patients with organ-confined prostate cancer. Recently, the advent of pioneering nerve-sparing robot-assisted laparoscopic radical prostatectomy (NS RALP) has significantly increased the potency rate after RP [1-3]. However, even if NS RALP is performed, a large number of patients still experience erectile dysfunction (ED) after surgery [1]. Therefore, the need for better penile rehabilitation is anticipated. This increase in need for penile rehabilitation stems from two pillars. First, the introduction of prostate-specific antigen (PSA) testing in the 1990s made early detection of prostate cancer possible [1,4,5]. The early screening using PSA testing led to a significant drop in patient age, and younger prostate cancer patients have great interest in and need for erectile function (EF) after surgery [1,4,5]. Second, recent advances in surgical techniques have motivated more prostate cancer patients to consider penile rehabilitation. NS RALP by an experienced surgeon can minimize nerve injury, and early penile rehabilitation with oral administration of phosphodiesterase type 5 inhibitors (PDE5-Is) can maximize penile recovery in ED patients after RP [1,6].
After the advent of the orally administered PDE5-Is in 1998, there was a huge shift in the ED treatment algorithm [7]. PDE5-Is are currently considered a standard treatment for ED patients after RP. Recent literature shows that PDE5-Is are safe and effective in treating ED patients after RP. Once daily administration of PDE5-Is has been experimentally proven to have a protective role in ED, and early administration of PDE5-Is helps to prevent cavernosal hypoxia, which leads to smooth muscle apoptosis and penile fibrosis [8-11]. Although PDE5-Is are one of the standard treatments for ED after RP, consensus has not been reached on their use, such as when to start, which drug is best, which dosage to use, how long to use, and when to stop [9,10]. In the case of tadalafil, doses of 10 and 20 mg have been administered on demand to ED patients, and once-a-day dosing of 5 mg has been used since the Korea Food and Drug Administration approval in 2008. Moreover, in a study that compared the efficacy, safety, and tolerability of on-demand tadalafil and daily dosed tadalafil for the treatment of ED, 72% of the patients preferred daily dosed tadalafil [12]. However, clinical studies on the daily administration of low-dose PDE5-Is and the effect of such treatment on ED patients after RP are sorely lacking [13]. The present study was therefore conducted to evaluate the efficacy and safety of once daily use of tadalafil 5 mg in the treatment of ED patients after RALP.
MATERIALS AND METHODS
We evaluated the records of 116 patients who, between September 2007 and December 2011, had undergone RALP by an experienced surgeon for localized prostate cancer at our institution. RALP was first performed in 2004 as a joint effort between our institution and Singapore General Hospital, which was the site of the initial Korean experience [14]. Standard RALP techniques including bladder neck preservation and posterior urethral reconstruction were used because these techniques during RALP can have favorable impacts on the early postoperative recovery of continence [15]. The 116 patients who developed ED after NS RALP, who had normal preoperative EF, and whose local clinical stage was T2 or lower with a Gleason score lower than 8 and a serum PSA of less than 20 ng before surgery were included in the study. The additional exclusion of 24 patients who underwent hormonal or radiation therapy preoperatively or postoperatively, who received any kind of preoperative ED treatment, or to whom PDE5-Is could not be prescribed resulted in 92 patients. The 92 patients were retrospectively evaluated in accordance with the ethical standards of the Institutional Review Board at Dong-A University Hospital. In a study of the 92 patients, 47 patients were prescribed tadalafil at a dose of 5 mg per day. In the tadalafil group, all patients took 5 mg tadalafil per day 1 hour before bedtime. For all 47 patients, oral intake of tadalafil 5 mg was initiated early after Foley catheter removal, between 2 and 3 weeks after the surgery. The tadalafil group was then stratified depending on the NS procedure they had undergone: bilateral NS (n=30) and unilateral NS (n=17).
Postoperative EF was assessed through the patients' responses to the Korean version of the five-item International Index of Erectile Function (IIEF-5) questionnaire, which is also referred to as the Sexual Health Inventory of Men. The IIEF-5 questionnaire is the abridged version of the IIEF-15 and consists of 5 questions related to ED diagnosis and EF improvement. The IIEF-5 questionnaire is a self-administered questionnaire that can sensitively detect subtle changes in EF recovery. Each of the 5 questions is scored from 0 to 5 or from 1 to 5, where 0, the absence of sexual activity; 1, very low/almost never or never/extremely difficult; 2, low/a few times/very difficult; 3, moderate/sometimes/difficult; 4, high/most times/slightly difficult; and 5, very high/almost always or always/not difficult. The total IIEF-5 score is calculated by summing each score from the five questions and varies from 1 to 25, where a score of 1 to 7, severe ED; 8 to 11, moderate ED; 12 to 16, mild-moderate ED; 17 to 21, mild ED; and 22 to 25, no ED. In the present study, the IIEF-5 questionnaire was conducted 3 times: before surgery, at 6 months after surgery, and at 1 year after surgery. All patients were also counseled on ED, tadalafil intake, and its side effects at each visit.
In the present study, positive responders were defined as those patients whose combined score for Q2, "When you had erections with sexual stimulation, how often were your erections hard enough for penetration?" and Q3, "During sexual intercourse, how often were you able to maintain your erection after you had penetrated your partner?" on the IIEF-5 questionnaire was 8 or more.
Outcomes from the tadalafil group and the non-tadalafil group were compared and analyzed according to NS status on the basis of the patients' IIEF-5 score. Data were summarized by using descriptive statistics: frequency and percentage for categorical variables and mean±standard deviation and median (range) for continuous variables. Differences in the patients' demographic and clinical characteristics were compared across subgroups with Fisher exact test for categorical variables or Mann-Whitney U-test for continuous variables. Wilcoxon's rank sum test was performed to test differences in IIEF-5 domains between time points. The cumulative incidence of recovery of erection firm enough for sexual intercourse was estimated by the Kaplan-Meier product limit method. The log-rank test was also employed to investigate the difference in recovery of erection between groups. A p-value lower than 0.05 was considered statistically significant. By its nature, this study was explorative and, therefore, no adjustment for multiple testing was applied. All statistical analyses were carried out by using IBM SPSS ver. 19.0 (IBM Co., Armonk, NY, USA) and MedCalc 11.6.1.0 (MedCalc, Ostend, Belgium).
RESULTS
Demographic and clinical variables at baseline were well balanced between the tadalafil group and the non-tadalafil group (Table 1). The 92 patients who were screened for eligibility according to the inclusion and exclusion criteria were retrospectively assessed in the present study. Of the 92 patients, 47 patients were prescribed tadalafil 5 mg per day. The patients in the tadalafil group (n=47) and those in the non-tadalafil group (n=45) were also stratified according to NS status. In the tadalafil group, 63.8% of the patients (n=30) underwent a bilateral NS procedure and 36.2% of the patients (n=17) underwent a unilateral NS procedure. In the non-tadalafil group, bilateral NS was performed for 60% of the patients (n=27) and unilateral NS was performed for 40% of the patients (n=18).
TABLE 1.
Patients' characteristics at baseline
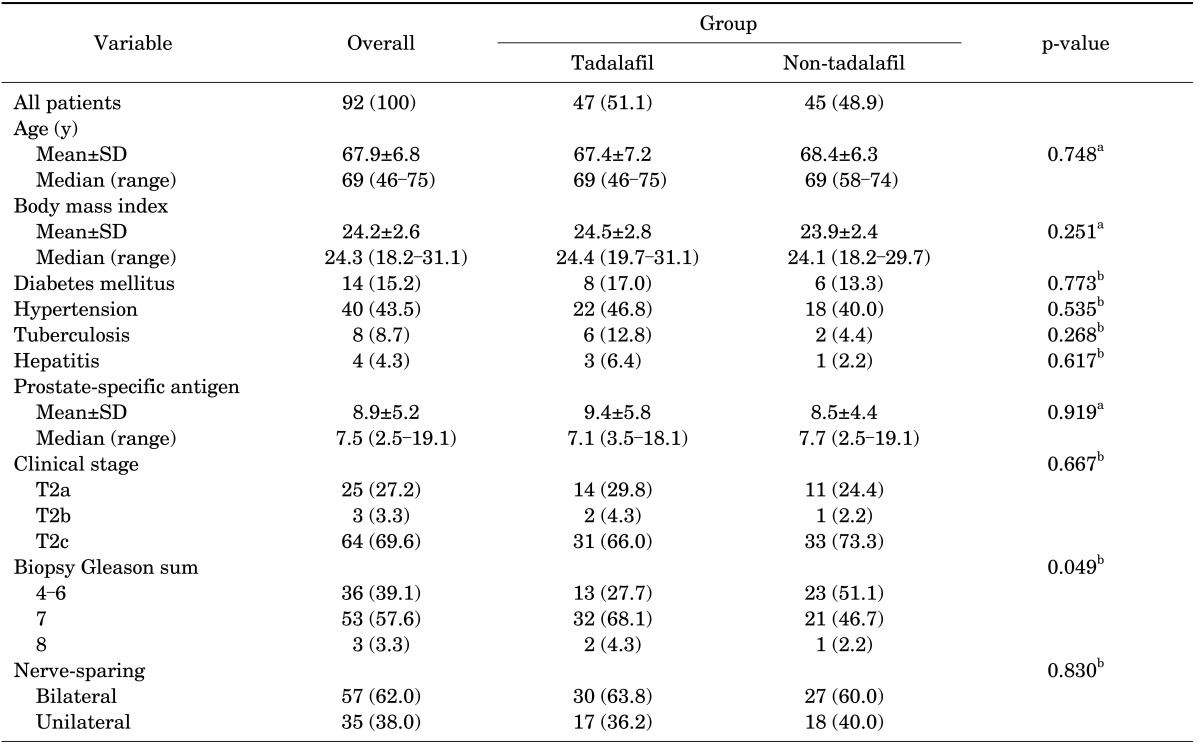
Values are presented as number (%) unless otherwise indicated.
SD, standard deviation; PSA, prostate-specific antigen.
a:Mann-Whitney U test. b:Fisher's exact test.
Compared with the non-tadalafil group, the tadalafil group regardless of NS procedure reported a statistically significant improvement in EF (p=0.0049, log-rank test). At 6 months after the surgery, 11% of the patients in the tadalafil group (n=5) responded positively to tadalafil, whereas there were no positive responders in the non-tadalafil group. At 12 months after the surgery, 32% of the patients in the tadalafil group (n=15) were able to perform intercourse, and 9% of the patients in the non-tadalafil group (n=4) had erection sufficient for sexual intercourse. Once-daily use of tadalafil 5 mg resulted in EF improvement during the course of 1 year after NS RALP (Fig. 1).
FIG. 1.

Positive responders to tadalafil following robot-assisted laparoscopic radical prostatectomy. (A) The positive responders to tadalafil with time and patients at risk determined by the Kaplan-Meier method. There was statistically significant difference between 2 subgroups (log-rank test p=0.0049). (B) The positive responders to tadalafil with time and patients at risk determined by the Kaplan-Meier method. There was statistically significant difference between 4 subgroups (log-rank test p=0.0098).
The mean IIEF-5 score at 1 year also differed between the tadalafil group and the non-tadalafil group as shown in Table 2 (p<0.05, Wilcoxon's rank sum test) and in Fig. 2. In the present study, most of the patients who had undergone NS RALP experienced ED after the surgery. At 6 months, the total IIEF-5 scores of the tadalafil group and the non-tadalafil group were 10.0±3.4 and 7.0±4.0, respectively (p<0.0001, Mann-Whitney U test). At 1 year after the surgery, the total IIEF-5 score in the tadalafil group was significantly greater than that in the non-tadalafil group (13.2±5.6 vs 7.7±4.8, p<0.0001; Mann-Whitney U test). Moreover, there was a significant increase in all 5 domains of the IIEF-5 in the tadalafil group, whereas in the non-tadalafil group no significant increases were observed in any of the domains at 1 year (Q4, p<0.0001; Q1, p<0.0001; Q3, p<0.0001; Q2, p=0.006; Q5, p<0.0001).
TABLE 2.
Mean IIEF-5 score at baseline, 6 months, and 1 year
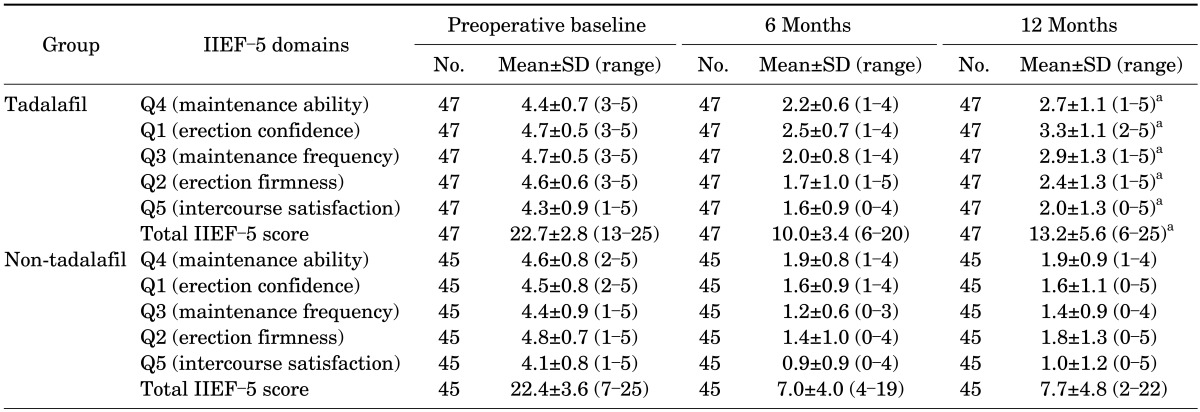
Each IIEF-5 domain was scored from 0 to 5 or 1 to 5: 0, the absence of sexual activity; 1, very low/almost never or never/extremely difficult; 2, low/a few times/very difficult; 3, moderate/sometimes/difficult; 4, high/most times/slightly difficult; and 5, very high/almost always or always/not difficult; the total IIEF-5 score was calculated by totaling and taking the mean of the responses to all 5 domains of IIEF-5.
IIEF-5, the abridged five-item version of the International Index of Erectile Function questionnaire; SD, standard deviation.
a:p<0.05, 6 months vs. 12 months (Wilcoxon's rank sum test).
FIG. 2.
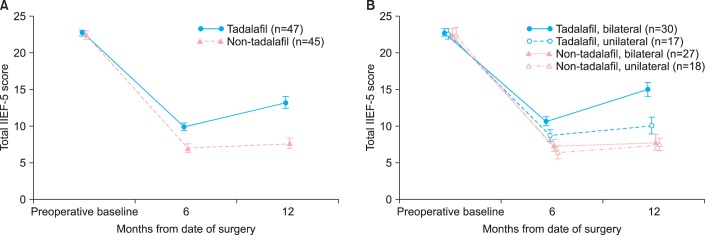
Comparision of total IIEF-5 scores between nerve-sparing groups following robot-assisted laparoscopic radical prostatectomy. (A) Mean±SEM plot of total IIEF-5 score across 2 subgroups. (B) Mean±SEM plot of total IIEF-5 score across 4 subgroups. IIEF-5, the abridged five-item version of the International Index of Erectile Function Questionnaire; SEM, standard error of measurements.
In the tadalafil group, the IIEF-5 score of the bilateral NS group was greater on all 5 domains of the IIEF-5 questionnaire than the score in the unilateral NS group at 1 year after surgery (Table 3). Moreover, as shown in Fig. 1, the patients' NS status largely influenced the response rate to tadalafil (p=0.0098, log-rank test). Among the patients who were prescribed tadalafil 5 mg per day, four patients (13%) in the bilateral NS group and one patient (6%) in the unilateral NS group positively responded to tadalafil at 6 months after the surgery. At 1 year, 12 patients (40%) in the bilateral NS group and 3 patients (18%) in the unilateral NS group responded positively to tadalafil and were able to perform intercourse. In the non-tadalafil group, only three patients (11%) for whom bilateral NS was performed and one patient (6%) for whom unilateral NS was performed had erections sufficient for vaginal intercourse. In the tadalafil group, two patients did not attempt sexual intercourse even though they had sufficient erections after the surgery. According to the results of the study, the once-daily dosage of tadalafil 5 mg was most effective when bilateral NS was performed.
TABLE 3.
Response to tadalafil at 1 year stratified by nerve-sparing status
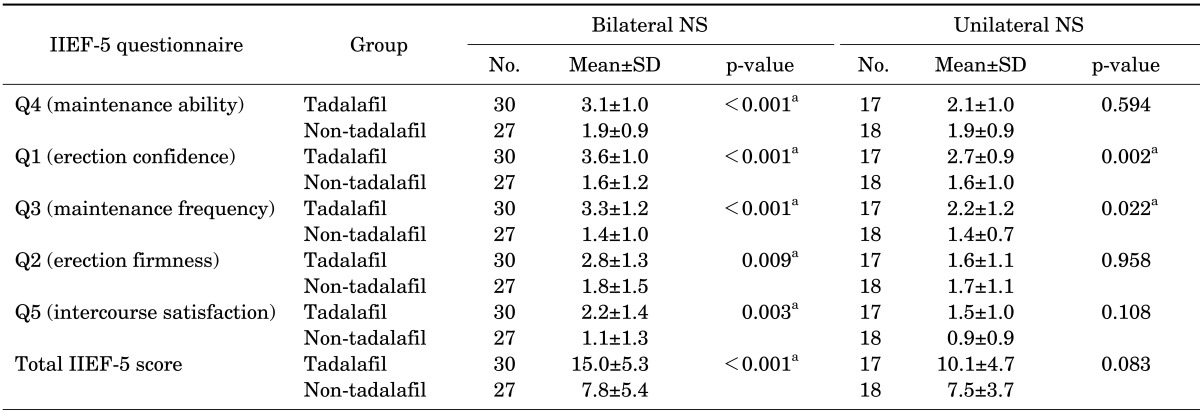
Each IIEF-5 domain was scored from 0 to 5 or 1 to 5: 0, the absence of sexual activity; 1, very low/almost never or never/extremely difficult; 2, low/a few times/very difficult; 3, moderate/sometimes/difficult; 4, high/most times/slightly difficult; and 5, very high/almost always or always/not difficult; the total IIEF-5 score was calculated by totaling and taking the mean of the responses to all 5 domains of IIEF-5. The total IIEF-5 ranged from 1 to 25: 1 to 7, severe ED; 8 to 11, moderate ED; 12 to 16, mild-moderate ED; 17 to 21, mild ED; and 22 to 25, no ED.
IIEF-5, the abridged five-item version of the International Index of Erectile Function questionnaire; NS, nerve-sparing; SD, standard deviation; ED, erectile dysfunction.
a:p<0.05, tadalafil vs. non-tadalafil (Mann-Whitney U test).
Daily use of tadalafil was well tolerated in the present study. At 6 months, flushing and dizziness were the most commonly reported adverse events. In the tadalafil group, four patients (8.5%) experienced flushing and one patient (2.1%) experienced dizziness at 6 months. At 1 year, two patients (4.3%) had headache, one patient (2.1%) experienced dizziness, and three patients (6.4%) were reported to experience flushing after taking the drug. All adverse events were mild or moderate in severity and transient in nature. In our retrospective review, we learned that the dropout rate was 8% (4 of 51) over a period of 1 year; two of the four patients had discontinued treatment owing to the high cost of the medication and the other two patients owing to a lack of efficacy.
DISCUSSION
The results of the current study of daily administration of tadalafil 5 mg for 1 year demonstrate the efficacy and safety of once-a-day dosing of tadalafil 5 mg in ED patients after RALP. After the surgery, patients in the tadalafil group showed greater improvement in EF than did those in the non-tadalafil group. The potency rate in the tadalafil groups who underwent either unilateral or bilateral NS continued to increase after the surgery, whereas the magnitude of improvement in the bilateral NS group was far greater than in the unilateral NS group. According to the IIEF-5 scores at 6 months and 1 year in the tadalafil group, the scores of the bilateral NS group (10.7±3.3 and 15.0±5.3, respectively) were significantly higher than the scores in the unilateral NS group (8.7±3.2 and 10.1±4.7, respectively). Erection sufficient enough for sexual intercourse with the administration of tadalafil was observed in 40% of the patients in the bilateral NS group and 18% of the patients in the unilateral NS group. The efficacy of daily administration of tadalafil was highly dependent on the degree of neurovascular bundle preservation.
Clinical results on the response rate to PDE5-Is are not homogeneous and vary widely. Zippe et al. [16] reported that the efficacy of sildenafil citrate for ED patients who underwent bilateral, unilateral, and non-NS retropubic RP was 71.7%, 50%, and 15.4%, respectively. In another study that evaluated 91 ED patients after RP, 52% of the patients (n=48) responded positively to sildenafil citrate and were able to have successful vaginal intercourse 1 year after the surgery [2]. In a randomized, double-blind, placebo-controlled, parallel study, Montorsi et al. [17] reported that tadalafil once-a-day significantly improved EF compared with the placebo group. After 12 weeks of drug administration, IIEF-EF domain scores ≥26 were obtained for 67 patients (45.9%) in the tadalafil group and 21 patients (31.3%) in the placebo group. However, in a randomized, double-blind, placebo-controlled study on the effects of nightly sildenafil citrate for the prevention of ED after bilateral NS RP, erection good enough for satisfactory sexual activity occurred only in 27% of the sildenafil group (n=14 of 51) and in 4% of the placebo group (n=1 of 25) [18]. Moreover, Montorsi et al. [19] conducted a prospective, randomized, double-blind, double-dummy, multinational, multicenter, parallel group study and evaluated 628 patients after bilateral NS RP. They compared the efficacy of on-demand versus nightly dosages of vardenafil and reported that IIEF scores ≥22 were obtained in 24.8%, 32.0%, and 48.2% of the placebo, vardenafil nightly, and vardenafil on-demand groups, respectively. Response rates to sildenafil after NS RP varied from 10% to 76%, whereas the response rates for the non-NS group varied from 0% to 15% [2,9,16].
The potency rate of 32% in the tadalafil group in the current study is slightly lower than the rates in previously published studies. The slightly lower response rate (32%) in the tadalafil group may stem from the rather stringent criteria applied in this study. For instance, several other studies did not provide a clear definition or criteria for a positive response, and in those studies a positive response did not necessarily mean the ability to achieve sexual intercourse [18]. In the current study, a summed score of 8 or more on Q2 ("When you had erections with sexual stimulation, how often were your erections hard enough for penetration?") and Q3 ("During sexual intercourse, how often were you able to maintain your erection after you had penetrated your partner?") of the IIEF-5 questionnaire was required for patients to be classified as positive responders.
The effect of PDE5-Is can be influenced by patient age [20]. The relatively older age of the patients in the present study (67.9±6.8 years) might have had a negative impact on the potency rate. Furthermore, 2 patients in the tadalafil group did not attempt sexual intercourse even though they had sufficient erections after the surgery. Lastly, the biopsy Gleason score, which is known to be related to PSA failure, was slightly higher in the tadalafil group than in the non-tadalafil group even though a high Gleason score of 8 or more was observed in only three of the patients (one in the non-tadalafil group and two in the tadalafil group). Diverse factors including preoperative EF, frequency of sexual intercourse before surgery, type of NS procedure, degree of postoperative potency, and the interval between surgery and the administration of PDE5-Is might have affected the potency results [17]. The discrepancy among published results suggests that further confirmatory studies are needed on the effects of PDE5-Is and the optimal regimen.
The mechanism of action of PDE5-Is is related to the etiology of ED after RP. Even though the NS technique with the advent of RALP significantly improved the potency rate, neurapraxia and nerve injury still persist even 1 year after surgery [1]. The current study demonstrates the profound loss of spontaneous erection after NS RALP. The patients' IIEF-5 score at 1 year was significantly lower than the patients' IIEF-5 score at preoperative baseline, and most patients (n=116) experienced ED after the surgery even though NS RALP was performed. When neurologic injury occurs, penile hypoxia and fibrosis lead to the absence of spontaneous nocturnal erections, which decreases the release of nitric oxide [1,6]. This decrease in nitric oxide production leads to a drop in the amount of available cyclic guanosine monophosphate (cGMP) [2,18]. PDE5-Is inhibit PDE5, which metabolizes cGMP, and this results in an increase in cGMP levels [2]. This increase in the amount of cGMP coupled with nitric oxide induces corporal smooth muscle relaxation, and this leads to subsequent erection by allowing blood flow to the penis [21-24]. The whole process requires nerve preservation, because if there is no cGMP, there is no substrate for PDE5 to metabolize [2]. This mechanism of action explains why the effect of tadalafil was much greater in the bilateral NS group than in the unilateral NS group in the current study.
Persistent use of PDE5-Is inhibits hypoxia-associated fibrosis by amplifying the depressed nitric oxide signaling pathway, and this leads to erectile recovery after RP [9]. In a recent study that compared the effects of different PDE5-Is, tadalafil was the most effective agent, followed by vardenafil, although there was no significant difference in the safety profile of the drugs [25]. In long-term studies, once daily administration of tadalafil 5 mg was effective and safe and thus became a viable alternative to the widely used on-demand administration of tadalafil for ED patients [26]. Moreover, the mean half-life of tadalafil (17.5 hours) is longer than that of sildenafil and vardenafil (about 4 hours) [27]. The longer duration of the drug may allow patients with ED to enjoy sexual activity free from the burden of planning drug intake before intercourse, which can improve the patients' sexual quality of life [27-29].
Previously published studies maintain that PDE5-Is can be administered as early as at the time of removal of the Foley catheter or within 1 month after RP [3,9]. Early administration of PDE5-Is helps to prevent cavernosal hypoxia, which leads to smooth muscle apoptosis and penile fibrosis [9]. In our study, all patients in the tadalafil group initiated oral intake of tadalafil 5 mg right after Foley catheter removal, between 2 to 3 weeks after the surgery, and tadalafil was administered for a period of 1 year. The potency rate of the bilateral NS group who took tadalafil (40%) was significantly higher than that of the non-tadalafil group (11%) at 1 year after the surgery. The results of our study suggest that ED after RALP can be well treated with once daily dosage of tadalafil 5 mg if NS RALP is performed. Therefore, tadalafil should be considered as a first-line treatment for a well-selected subgroup of ED patients after RP.
There were several limitations to the current study. The first and most notable limitation pertains to the retrospective study design. The current study was neither randomized nor placebo-controlled because it was carried out in a retrospective manner. Although the results of the study should be applied with caution, the findings suggest that once daily dosage of tadalafil 5 mg was effective and well-tolerated by ED patients after RALP at 1 year after the surgery. A second limitation of the current study is related to the relatively small number of patients. However, the current study can be a pilot for further studies that have larger randomized samples of patients. Despite these limitations, this study is the first long-term study that evaluated the efficacy and safety of tadalafil 5 mg once daily use in ED patients after NS RALP. More confirmatory studies that are prospective, crossover, randomized, placebo-controlled, and double-blind are clearly required to determine the effects and the optimal regimen of tadalafil in ED patients after RALP.
CONCLUSIONS
This study is the first long-term study that evaluated the efficacy and safety of tadalafil 5 mg once daily use in ED patients after NS RALP. The results of the study indicate that once-a-day dosing of tadalafil 5 mg is effective and safe in properly selected ED patients after NS RALP. At 1 year after the surgery, a recovery rate of 40% was attained in the bilateral NS group who took tadalafil 5 mg once per day before bedtime. Once daily administration of tadalafil 5 mg was effective and safe for ED patients who had undergone NS RALP, and the patients showed gradual improvement in their EF over a period of 1 year.
Footnotes
The authors have nothing to disclose.
References
- 1.Zippe CD, Pahlajani G. Penile rehabilitation following radical prostatectomy: role of early intervention and chronic therapy. Urol Clin North Am. 2007;34:601–618. doi: 10.1016/j.ucl.2007.08.012. [DOI] [PubMed] [Google Scholar]
- 2.Raina R, Lakin MM, Agarwal A, Sharma R, Goyal KK, Montague DK, et al. Long-term effect of sildenafil citrate on erectile dysfunction after radical prostatectomy: 3-year follow-up. Urology. 2003;62:110–115. doi: 10.1016/s0090-4295(03)00157-2. [DOI] [PubMed] [Google Scholar]
- 3.Salonia A, Burnett AL, Graefen M, Hatzimouratidis K, Montorsi F, Mulhall JP, et al. Prevention and management of postprostatectomy sexual dysfunctions part 2: recovery and preservation of erectile function, sexual desire, and orgasmic function. Eur Urol. 2012;62:273–286. doi: 10.1016/j.eururo.2012.04.047. [DOI] [PubMed] [Google Scholar]
- 4.Stephenson RA. Prostate cancer trends in the era of prostate-specific antigen. An update of incidence, mortality, and clinical factors from the SEER database. Urol Clin North Am. 2002;29:173–181. doi: 10.1016/s0094-0143(02)00002-2. [DOI] [PubMed] [Google Scholar]
- 5.Greene KL, Cowan JE, Cooperberg MR, Meng MV, DuChane J, Carroll PR, et al. Who is the average patient presenting with prostate cancer? Urology. 2005;66(5 Suppl):76–82. doi: 10.1016/j.urology.2005.06.082. [DOI] [PubMed] [Google Scholar]
- 6.Defade BP, Carson CC, 3rd, Kennelly MJ. Postprostatectomy erectile dysfunction: the role of penile rehabilitation. Rev Urol. 2011;13:6–13. [PMC free article] [PubMed] [Google Scholar]
- 7.Moreland RB, Goldstein I, Traish A. Sildenafil, a novel inhibitor of phosphodiesterase type 5 in human corpus cavernosum smooth muscle cells. Life Sci. 1998;62:PL 309–PL 318. doi: 10.1016/s0024-3205(98)00158-1. [DOI] [PubMed] [Google Scholar]
- 8.Megas G, Papadopoulos G, Stathouros G, Moschonas D, Gkialas I, Ntoumas K. Comparison of efficacy and satisfaction profile, between penile prosthesis implantation and oral PDE5 inhibitor tadalafil therapy, in men with nerve-sparing radical prostatectomy erectile dysfunction. BJU Int. 2013;112:E169–E176. doi: 10.1111/j.1464-410X.2012.11561.x. [DOI] [PubMed] [Google Scholar]
- 9.Hatzimouratidis K, Burnett AL, Hatzichristou D, McCullough AR, Montorsi F, Mulhall JP. Phosphodiesterase type 5 inhibitors in postprostatectomy erectile dysfunction: a critical analysis of the basic science rationale and clinical application. Eur Urol. 2009;55:334–347. doi: 10.1016/j.eururo.2008.10.028. [DOI] [PubMed] [Google Scholar]
- 10.Lee J. Penile rehabilitation should not be the norm for patients post-radical prostatectomy. Can Urol Assoc J. 2009;3:54–56. doi: 10.5489/cuaj.1018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Montorsi F, Guazzoni G, Strambi LF, Da Pozzo LF, Nava L, Barbieri L, et al. Recovery of spontaneous erectile function after nerve-sparing radical retropubic prostatectomy with and without early intracavernous injections of alprostadil: results of a prospective, randomized trial. J Urol. 1997;158:1408–1410. [PubMed] [Google Scholar]
- 12.McMahon C. Comparison of efficacy, safety, and tolerability of on-demand tadalafil and daily dosed tadalafil for the treatment of erectile dysfunction. J Sex Med. 2005;2:415–425. doi: 10.1111/j.1743-6109.2005.20360.x. [DOI] [PubMed] [Google Scholar]
- 13.Mulhall JP, Morgentaler A. Penile rehabilitation should become the norm for radical prostatectomy patients. J Sex Med. 2007;4:538–543. doi: 10.1111/j.1743-6109.2007.00486.x. [DOI] [PubMed] [Google Scholar]
- 14.Kong GS, Seong YK, Sung GT. Robotic-assisted radical prostatectomy using da VinciTM surgical robotic system: initial Korean experience. Korean J Urol. 2005;46:353–359. [Google Scholar]
- 15.You YC, Kim TH, Sung GT. Effect of bladder neck preservation and posterior urethral reconstruction during robot-assisted laparoscopic radical prostatectomy for urinary continence. Korean J Urol. 2012;53:29–33. doi: 10.4111/kju.2012.53.1.29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Zippe CD, Jhaveri FM, Klein EA, Kedia S, Pasqualotto FF, Kedia A, et al. Role of Viagra after radical prostatectomy. Urology. 2000;55:241–245. doi: 10.1016/s0090-4295(99)00441-0. [DOI] [PubMed] [Google Scholar]
- 17.Montorsi F, Aversa A, Moncada I, Perimenis P, Porst H, Barker C, et al. A randomized, double-blind, placebo-controlled, parallel study to assess the efficacy and safety of once-a-day tadalafil in men with erectile dysfunction who are naïve to PDE5 inhibitors. J Sex Med. 2011;8:2617–2624. doi: 10.1111/j.1743-6109.2011.02353.x. [DOI] [PubMed] [Google Scholar]
- 18.Padma-Nathan H, McCullough AR, Levine LA, Lipshultz LI, Siegel R, Montorsi F, et al. Randomized, double-blind, placebo-controlled study of postoperative nightly sildenafil citrate for the prevention of erectile dysfunction after bilateral nerve-sparing radical prostatectomy. Int J Impot Res. 2008;20:479–486. doi: 10.1038/ijir.2008.33. [DOI] [PubMed] [Google Scholar]
- 19.Montorsi F, Brock G, Lee J, Shapiro J, Van Poppel H, Graefen M, et al. Effect of nightly versus on-demand vardenafil on recovery of erectile function in men following bilateral nerve-sparing radical prostatectomy. Eur Urol. 2008;54:924–931. doi: 10.1016/j.eururo.2008.06.083. [DOI] [PubMed] [Google Scholar]
- 20.Zagaja GP, Mhoon DA, Aikens JE, Brendler CB. Sildenafil in the treatment of erectile dysfunction after radical prostatectomy. Urology. 2000;56:631–634. doi: 10.1016/s0090-4295(00)00659-2. [DOI] [PubMed] [Google Scholar]
- 21.Lue TF. Erectile dysfunction. N Engl J Med. 2000;342:1802–1813. doi: 10.1056/NEJM200006153422407. [DOI] [PubMed] [Google Scholar]
- 22.Mydlo JH, Viterbo R, Crispen P. Use of combined intracorporal injection and a phosphodiesterase-5 inhibitor therapy for men with a suboptimal response to sildenafil and/or vardenafil monotherapy after radical retropubic prostatectomy. BJU Int. 2005;95:843–846. doi: 10.1111/j.1464-410X.2005.05413.x. [DOI] [PubMed] [Google Scholar]
- 23.Lagoda G, Jin L, Lehrfeld TJ, Liu T, Burnett AL. FK506 and sildenafil promote erectile function recovery after cavernous nerve injury through antioxidative mechanisms. J Sex Med. 2007;4(4 Pt 1):908–916. doi: 10.1111/j.1743-6109.2007.00519.x. [DOI] [PubMed] [Google Scholar]
- 24.Lagoda G, Sezen SF, Liu T, Hoke A, Burnett AL. FK506-binding protein localizations in human penile innervation. BJU Int. 2008;101:604–609. doi: 10.1111/j.1464-410X.2007.07290.x. [DOI] [PubMed] [Google Scholar]
- 25.Yuan J, Zhang R, Yang Z, Lee J, Liu Y, Tian J, et al. Comparative effectiveness and safety of oral phosphodiesterase type 5 inhibitors for erectile dysfunction: a systematic review and network meta-analysis. Eur Urol. 2013;63:902–912. doi: 10.1016/j.eururo.2013.01.012. [DOI] [PubMed] [Google Scholar]
- 26.Porst H, Rajfer J, Casabe A, Feldman R, Ralph D, Vieiralves LF, et al. Long-term safety and efficacy of tadalafil 5 mg dosed once daily in men with erectile dysfunction. J Sex Med. 2008;5:2160–2169. doi: 10.1111/j.1743-6109.2008.00935.x. [DOI] [PubMed] [Google Scholar]
- 27.Porst H, Giuliano F, Glina S, Ralph D, Casabe AR, Elion-Mboussa A, et al. Evaluation of the efficacy and safety of once-a-day dosing of tadalafil 5mg and 10mg in the treatment of erectile dysfunction: results of a multicenter, randomized, double-blind, placebo-controlled trial. Eur Urol. 2006;50:351–359. doi: 10.1016/j.eururo.2006.02.052. [DOI] [PubMed] [Google Scholar]
- 28.Hanson-Divers C, Jackson SE, Lue TF, Crawford SY, Rosen RC. Health outcomes variables important to patients in the treatment of erectile dysfunction. J Urol. 1998;159:1541–1547. doi: 10.1097/00005392-199805000-00037. [DOI] [PubMed] [Google Scholar]
- 29.Kang DH, Lee JY, Park SY, Moon HS, Jeong TY, Yoo TK, et al. Efficacy and safety of tadalafil 5 mg administered once daily in Korean men with erectile dysfunction: a prospective, multicenter study. Korean J Urol. 2010;51:647–652. doi: 10.4111/kju.2010.51.9.647. [DOI] [PMC free article] [PubMed] [Google Scholar]