

Abstract
Background:
Radiosurgery is a well-established treatment modality for medically refractory trigeminal neuralgia. The exact mechanism of pain relief after radiosurgery is not clearly understood. Histopathology examination of the trigeminal nerve in humans after radiosurgery is rarely performed and has produced controversial results.
Case Description:
We report on a 45-year-old female who received radiosurgery treatment for trigeminal neuralgia by Cyberknife. A 6-mm portion of the cisternal segment of trigeminal nerve received a dose of 60 Gy. The clinical benefit started 10 days after therapy and continued for 8 months prior to a recurrence of her previous symptoms associated with mild background pain. She underwent microvascular decompression and partial sensory root sectioning. Atrophied trigeminal nerve rootlets were grossly noted intraoperatively under surgical microscope associated with changes in trigeminal nerve color to gray. A biopsy from the inferolateral surface of the nerve proximal to the midcisternal segment showed histological changes in the form of fibrosis and axonal degeneration.
Conclusion:
This case study supports the evidence of histological damage of the trigeminal nerve fibers after radiosurgery therapy. Whether or not the presence and degree of nerve damage correlate with the degree of clinical benefit and side effects are not revealed by this study and need to be explored in future studies.
Keywords: Histopathology, radiosurgery, trigeminal neuralgia
INTRODUCTION
Radiosurgery has recently gained popularity as a treatment modality for pharmacoresistant trigeminal neuralgia. It is considered as the least invasive procedure as compared with other treatment methods, such as percutaneous destructive procedures and microvascular decompression (MVD).[18,25] Despite the extensive research in trigeminal neuralgia; the exact mechanism of pain remains unrevealed.[21] This has lead to poor understanding of the mechanism of pain relief from various therapeutic procedures, including radiosurgery.[14]
To date, there has only been one animal study that has examined the histological effect of radiation on the trigeminal nerve.[17] This study showed axonal degeneration of the trigeminal nerve after radiation. To our current knowledge, there have only been two case reports on the histopathological trigeminal nerve features after radiosurgery in humans.[14] In one case report, an autopsy showed a trigeminal nerve lesion induced by radiation,[29] conversely, the other report showed that no lesions were identified in a specimen that was taken from the trigeminal nerve during an MVD procedure.[10] Here, we report on a patient who underwent MVD after a short-lasting benefit from a Cyberknife radiosurgery procedure. Histological findings from the trigeminal nerve biopsy are described and discussed in the context of radiation mechanisms of pain relief and microstructural effects.
CASE REPORT
Clinical scenario
A 43-year-old female not known to have any concomitant medical problems was diagnosed to have classical trigeminal neuralgia 4 years ago when she presented with paroxysmal electric-shock-type pain involving the dermatomes of the left maxillary and mandibular trigeminal branches. Her symptoms were aggravated by eating, brushing her teeth, and drinking cold water. The maximal intensity of pain was at the left cheek and left side of the upper lip and radiating to the side of the nose. There was no history of any associated sustained background pain or sensory symptoms. Her pain responded well to carbamazepine initially; however, the dose was escalated after few months without complete control of her symptoms. Subsequently, she was treated with carbamazepine, pregabalin, and baclofen without complete resolution of her severe pain. The pain remained intractable to medical therapy with a visual analogue score (VAS) for pain of 10 points prior to medical therapy and 8 points after.
On clinical examination, there were no sensory deficits or dermatological changes at trigeminal nerve distribution and no abnormal neurological signs. Magnetic resonance imaging (MRI) of the brain did not reveal any signs of demyelinating disease, tumor, vascular malformation, or any other structural lesion. A small vessel was seen above the trigeminal nerve juxtpontine segment by MRI constructive interference in steady state (CISS) sequence [Figure 1]. Management options were offered for the patient, which included percutaneous procedures, radiosurgery, and MVD. After discussing the pros and cons of each procedure, the patient decided to go for radiosurgery.
Figure 1.
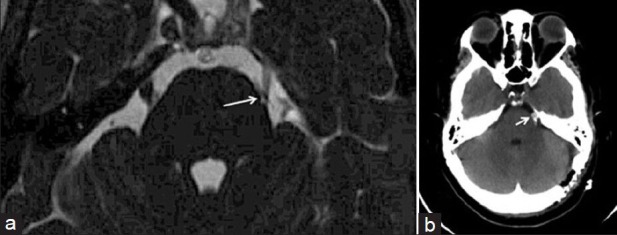
MRI brain (CISS sequence) depicting small vessel (arrow) at the trigeminal nerve juxtapontine segment (a). Post-MVD CT brain demonstrating the Teflon patch (arrow) at the juxtapontine and cisternal segments of the trigeminal nerve (b)
Subsequently, she underwent stereotactic image-guided radiosurgery using CyberKnife® (Accuray, Inc., Sunnyvale, CA, USA). A total dose of 60 Gy prescribed to 76% Isodose line covering 100% of the target, which consisted of a 6-mm length of the left trigeminal nerve cisternal segment [Figure 2]. Maximum dose to the target was 7894.74 cGy. This was delivered by a single fixed 5-mm cone with a total of 100 beams. The conformality index was 1.61, and the homogeneity index was 1.32. The stereotactic planning was carried out with fusing 1 mm cuts computed tomography (CT) scan with T1 3D MRI and 3D CISS sequence. Of note, the identified length of trigeminal nerve by MRI CISS sequence was 11.5 mm. The pain relief benefit started approximately 10 days after the procedure, and the patient continued to have 80% reduction of the lancinating trigeminal neuralgia pain (Barrow Neurological Institute (BNI) grade III).[26] However, 2 months later, she started complaining of dull background pain with an intensity of 3 VAS and intermittent mild facial numbness at V2 distribution (BNI grade II for facial numbness). There was no change in the lancinating shooting pain pattern. The medications remained unchanged. The patient had a recurrence of the pain 8 months later with more frequent attacks than before the procedure and remained intractable to medical therapy. At that time, clinical examination showed reduced sensation at V2 and V3 and relative reduction in the corneal reflex on the left eye. No corneal ulceration was noted, and the patient had with normal visual acuity. MRI of the brain did not demonstrate any enhancement or signal changes at the trigeminal nerve and brainstem.
Figure 2.
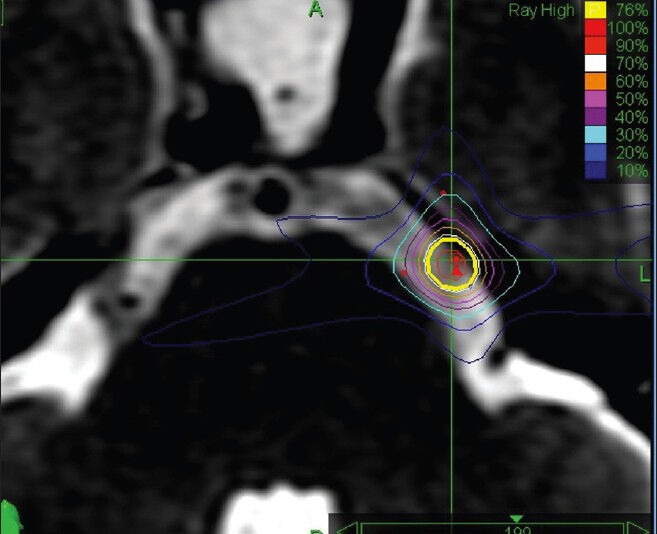
Cyberknife® radiosurgery plan on MRI depicting the dose target and isodense lines
We elected to perform MVD to explore the nerve with possible partial sensory sectioning. The procedure was done under neurophysiology monitoring of the facial, vestibulocochlear, and trigeminal nerves on the left side in addition to motor evoked potential (MEP) and somatosensory evoked potential (SSEP). Electromyography (EMG) was used for trigeminal nerve monitoring. Intraoperatively, the trigeminal nerve appeared atrophied and flattened with grayish discoloration of the nerve rootlets [Figure 3]. An arterial loop was identified at the superior surface of the juxtpontine trigeminal nerve segment; however, the artery was not causing obvious compression [Figure 3]. This vessel was separated from the nerve by a Teflon patch. Partial sensory sectioning was done and a small nerve rootlets biopsy from the midcisternal nerve segment was taken and submitted for histopathological examination [Figure 3]. The interval between histological examination and radiosurgery was 13 months.
Figure 3.
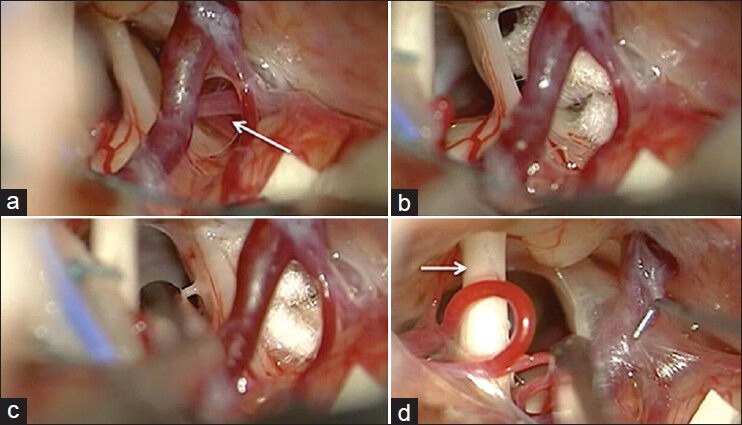
Intraoperative photos demonstrating the left trigeminal nerve and artery loop at the upper surface of the juxtapontine nerve segment (arrow) (a). The artery loop was isolated from the nerve using Teflon patch (b). Note the trigeminal nerve atrophy, flattening and changes in color as compared with the faciocochlear complex (arrow) (a, b and d). The site of trigeminal nerve biopsy at the midcisternal segment is demonstrated (c)
Histopathology features
The submitted specimen was too small to be utilized for full staining methods. Therefore, the biopsy was completely processed for electron microscopy (EM). The toluidine blue-stained, epoxy-embedded section revealed fibrous tissue (fibrosis) and a few haphazardly arranged and distorted myelinated nerve fibers [Figure 4]. Some were thinly myelinated and many had empty or dense axoplasm. A regenerative axonal cluster was noted as well. Transmission EM revealed variably sized myelinated axons in a marked collagenous background [Figure 5]. Most axons had empty axoplasm with markedly degraded myelin sheaths. Few had filamentous axoplasmic inclusions. There were many degenerated myelin/myelinoid profiles in the background. No active cellular component was noted. The changes were suggestive of advanced traumatic/destructive process.
Figure 4.
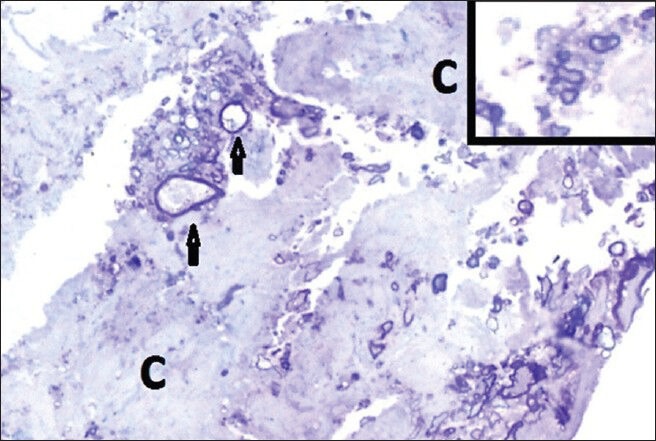
Histopathology thick section of the specimen showing abundant collagen fibers (C) where nerve sprouts are embedded. In the center two large and thinly myelinated axons (arrows) have empty axoplasm. Inset: A regenerating axonal cluster. (Toluidine blue. Original magnifications × 400)
Figure 5.
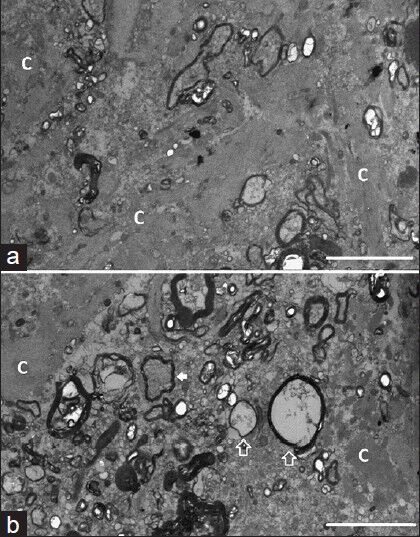
Histopathology slide showing distorted nerve fibers (myelinated axons) surrounded by abundant collagen fibers (letter C). Transmission electron microscopy, original magnification × 1000; bar = 5 μm (a). Some axons have clear axoplasm (open arrows) and others have dense filamentous axoplasm (white arrow). Transmission electron microscopy, original magnification × 1000; bar = 5 μm (b)
DISCUSSION
The effects of radiation on peripheral nerves have been investigated in several early experimental animal works.[3,12,13,14] These studies demonstrated conduction blockage at high doses (1500-1300 cGy) in cold-blooded animals.[13] A lower threshold of radiation for a complete conduction block was observed in warm-blooded animals.[12] These studies showed that the resistance of peripheral nerves to radiation is significant, and gamma fibers were found to be more sensitive to radiation than were alpha or beta fibers.[12,14] The radiation dose used in the aforementioned experiments was much higher than the current clinically applied dose. In contrast, there is conflicting data regarding the physiological effects of low-dose radiation. In some early studies, conduction excitability was observed at 100 G.[4,14] However, more recent studies showed that the “excitability effect” a is related to artifacts in injured nerve conduction.[11,27] At present, the most acceptable hypothesis for the physiological effects of radiation on a peripheral nerve is that the nerve conduction block is induced by impaired sodium ion channels function.[14,27] In our case, neurophysiological monitoring showed only nerve irritation on EMG during surgical manipulation, and the nerve was not stimulated intraoperatively. Intraoperative nerve stimulation and neurophysiological conduction studies can be performed in similar cases in the future to explore the neurophysiological effects of radiation on the human trigeminal nerve.
Radiation-induced structural abnormalities visualized in MRI postradiosurgery procedure have been described.[2,9,15] Certain MRI changes, such as trigeminal nerve focal enhancement, might occur in some cases after radiosurgery treatment. This might give an evidence of radiation-induced structural changes within the nerve fibers. In a report of 15 cases, Alberico et al. found that trigeminal nerve enhancement did not correlate with clinical response.[2] More recently, Gorgulho et al. found that pons enhancement in an MRI appears to correlate with pain relief without higher incidence of complications.[15] This finding is supported by other studies, which suggests that proximal nerve targeting at the root entry zone (REZ) to the brainstem can be more effective in pain control.[5,26,28] Conversely, this was not evident in other studies.[23,24] In this presented case, the radiosurgical target was 4 mm from the brainstem at the midcisternal segment. No enhancement or signal changes were identified in the follow-up MRI. Recently, Hodaie et al. reported on trigeminal nerve microstructural changes in tractography after gamma knife radiosurgery.[16] In this report, five patients underwent 3 Tesla MRIs and diffusion tensor imaging (DTI). Fractional anisotropy diffusivity was affected in a focal manner within the nerve, and this modality was more sensitive to demonstrating focal structural abnormality than enhancement to gadolinium. Moreover, this study suggested that radiosurgery predominantly affects myelin. Overall, these radiological abnormalities support the evidence of radiation-induced structural changes within nerve fibers. The reason behind the variability in the trigeminal nerve clinical and radiological responses to radiation is still unresolved.
Histopathology examinations of the effect of radiation on peripheral nerves have been limited for both animal and human studies. Central demyelination of the trigeminal nerve was histologically identified in three patients with vascular compression after performing partial sensory sectioning.[22] Although this study explored the ultrastructural changes in trigeminal sensory rootlets associated with the presence of vascular compression, those patients did not receive radiosurgery. Devore et al. demonstrated similar finding in 12 patients who underwent MVD for trigeminal neuralgia.[8] The main finding is dysmyelination without necrosis. In a single case report, histological examination of the facial nerve after radiosurgery for vestibular schwannoma demonstrated loss of axons and microvascilitis.[30] In another study done on animal spinal nerves that received 90 Gy of radiation, researchers have demonstrated focal islands of denudation in the axons.[7] To date, there are two animal studies that examined the histological effect of radiosurgery on the trigeminal nerve.[17,31] In 2000, Kondziolka et al. examined the histological effects of radiosurgery on the trigeminal nerves of two baboons.[17] A gamma knife single 4-mm isocentric radiation was applied to deliver 80 or 100 Gy, targeting the proximal trigeminal nerve anterior to the brainstem. The nonradiated brains and nerves were used as controls. An MRI was done 6 months after radiosurgery, which showed gadolinium enhancement of all radiated trigeminal nerves. Histological examination performed 6 months after radiosurgery demonstrated focal axonal degeneration, demyelination, and edema after 80 Gy of radiation. Necrosis was observed in the nerves that received 100 Gy, and in one specimen, the entire nerve was necrotic. This animal study demonstrated evidence of structural damage of the trigeminal nerve by radiation, and the degree of damage could be dose-dependent. Although this experiment added significant information and paved the way for further investigation, it was done on normal trigeminal nerves. Zhao et al. reported on the effect of different doses of radiation on trigeminal nerve of rhesus monkeys.[31] This study showed that 60-70 Gy have very minimal effect, 80 Gy induced partial axonal degeneration, and 100 Gy caused some necrosis.
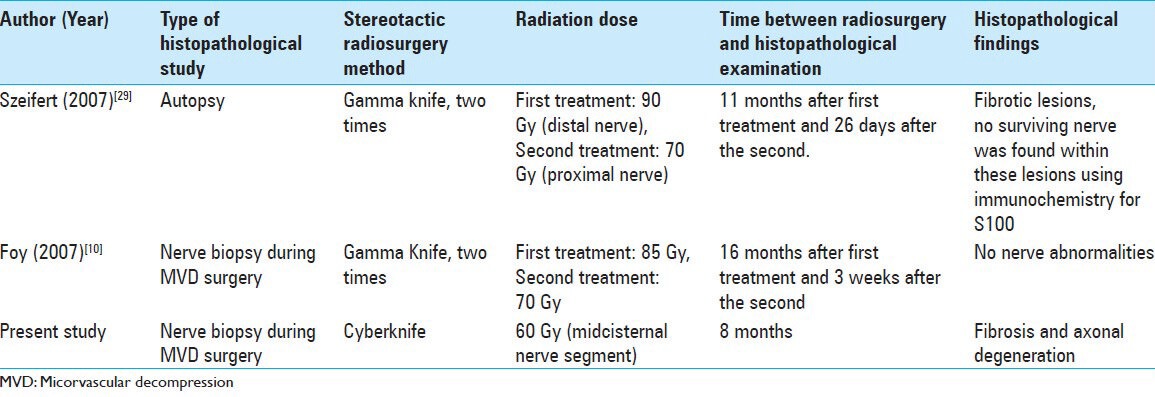
Histological features on an irradiated trigeminal nerve by radiosurgery for trigeminal neuralgia was reported by Szeifert et al.[29] The investigator reported on a patient with left trigeminal neuralgia who was treated twice with gamma knife radiosurgery. The first treatment targeted the distal cisternal trigeminal nerve segment with 90 Gy; in the second, 70 Gy was delivered to target the proximal nerve closer to the REZ. The patient died 26 days after the second treatment from a stroke not related to radiosurgery. Autopsy and histological examination were carried out for the treated trigeminal nerve, and the contralateral one was used as a control. The timing of the autopsy was 11 months and 26 days after the first and second radiosurgery procedures, respectively. Histological examination showed acute and chronic changes. At the site of the first radiosurgery, fibrotic lesions were identified, and no surviving nerve was found within these lesions using immunochemistry for S100. These abnormalities were considered to be chronic radiation effects. At the second radiosurgery site, a well-demarcated necrotic lesion was found that was considered to be acute radiation effect. The authors suggested that 90 Gy of radiation can induce more effective pathological lesions within the nerve. This is supported by the aforementioned animal study with the hypothesis that histopathological changes are dependent on radiation dose. The authors considered the acute histological changes to be related to the radiation dose of 70 Gy. However, the time frame between the second radiosurgery and histological examination was too short to prove such conclusion. In this report, the size of the nerve specimen was sufficient for a detailed histological and immunohistochemical studies. In contrast, in our case, the submitted biopsy specimen was not sufficient for detailed immunohistochemical investigation.
Foy et al. reported on a 74-year-old female who received two gamma knife radiosurgery procedures for V2 and V3 classical trigeminal neuralgia Table 1.[10] The patient underwent prior percutaneous glycerol rhizotomy and MVD. The proximal nerve segment received a radiation dose of 85 and 70 Gy in the first and second radiosurgical procedures, respectively. An MRI did not show any nerve enhancement. Similar to our case, the patient underwent MVD and partial sensory sectioning, and a small biopsy was submitted for pathology. The time frame between the biopsy and the two radiosurgical procedures was 16 months and 3 weeks, respectively. Intraoperatively, the nerve looked grossly normal. A histological examination did not reveal any abnormality. This normal histological finding despite prior destructive procedures and two radiosurgery treatments cannot be fully explained. This small nerve biopsy might have been taken from an area that was not affected by prior therapeutic procedures.
Table 1.
Summary of human trigeminal nerve histopathological studies poststereotactic radiosurgery for trigeminal neuralgia
In this case report, the patient developed short-lasting pain relief, facial numbness, and mild sustained background pain. All of these clinical features represent trigeminal nerve response to radiation. An MRI did not show any enhancement or signal changes; however, it is not necessary to be present after radiosurgery and does not necessery correlate with the clinical benefit.[2] The patient received radiosurgery after medical therapy with no destructive procedures prior to that. This has rolled out the confounding effect of other procedure. Of note, the safety and benefit of the applied Cyberknife radiosurgery in the treatment of trigeminal neuralgia have been found to be comparable to gamma knife results in several reports during the past decade.[1,6,19,20] During the MVD surgery, the nerve grossly appeared somewhat atrophied and flattened under a surgical microscope Figure 3. In addition, grayish discoloration was noted as compared with the usual normal trigeminal nerve appearance and also as compared with the visualized faciocochlear complex. We think this particular gross intraoperative finding is worthy of reporting for the benefit of future studies. The biopsy was taken from the targeted nerve portion by radiosurgery. Although the histological examination demonstrated a clear fibrotic lesion and axonal degeneration, the small specimen was not enough for further immunohistochemical investigations. This is a clear limitation of this report, and a larger biopsy might reveal more histological details.
CONCLUSION
Histological studies of the human trigeminal nerve after radiosurgery are very rare. This case report supports previous reports on animal and human studies, and demonstrates radiation-induced microstructural trigeminal nerve damage. More detailed histological investigations of trigeminal nerve specimens will be of value in the future. Moreover, intraoperative neurophysiological investigations of irradiated trigeminal nerves might add new information about physiological effects of radiation on peripheral nerves.
Footnotes
Available FREE in open access from: http://www.surgicalneurologyint.com/text.asp?2013/4/7/462/125463
Contributor Information
Faisal Al-Otaibi, Email: faisalruwais@gmail.com.
Hindi Alhindi, Email: hal-hindi@kfshrc.edu.sa.
Adnan Alhebshi, Email: adnanhebshi@gmail.com.
Monirah Albloushi, Email: monirah_albloushi@yahoo.com.
Saleh Baeesa, Email: salehbaeesa@gmail.com.
Mojgan Hodaie, Email: Mojgan.Hodaie@uhn.ca.
REFERENCES
- 1.Adler JR, Jr, Bower R, Gupta G, Lim M, Efron A, Gibbs IC, et al. Nonisocentric radiosurgical rhizotomy for trigeminal neuralgia. Neurosurgery. 2009;64(2 Suppl):A84–90. doi: 10.1227/01.NEU.0000341631.49154.62. [DOI] [PubMed] [Google Scholar]
- 2.Alberico RA, Fenstermaker RA, Lobel J. Focal enhancement of cranial nerve V after radiosurgery with the Leksell gamma knife: Experience in 15 patients with medically refractory trigeminal neuralgia. AJNR Am J Neuroradiol. 2001;22:1944–8. [PMC free article] [PubMed] [Google Scholar]
- 3.Bachofer CS, Kaak SM. Response of the nervous system to ionized radiation. UK: Little, Brown and Company Inc; 1964. Relative sensitivity of isolated nerves to CO60 gamma rays; pp. 221–42. [Google Scholar]
- 4.Bergstrom RM. The effect of 5.3 MeV polonium 210 alpha-particles on the electrical activity of alpha- and beta-fibres of the frog sciatic nerve. Ann Med Exp Biol Fenn. 1961;39:211–5. [PubMed] [Google Scholar]
- 5.Brisman R, Mooij R. Gamma knife radiosurgery for trigeminal neuralgia: Dose-volume histograms of the brainstem and trigeminal nerve. J Neurosurg. 2000;93(Suppl 3):155–8. doi: 10.3171/jns.2000.93.supplement. [DOI] [PubMed] [Google Scholar]
- 6.Chang SD, Main W, Martin DP, Gibbs IC, Heilbrun MP. An analysis of the accuracy of the CyberKnife: A robotic frameless stereotactic radiosurgical system. Neurosurgery. 2003;52:140–6. doi: 10.1097/00006123-200301000-00018. [DOI] [PubMed] [Google Scholar]
- 7.De Salles A, Medin P. New York: Thieme Medical Publisher; 2009. Functional Spine Radiosurgery. In. Spine Radiosurgery; p. 176. [Google Scholar]
- 8.Devor M, Govrin-Lippmann R, Rappaport ZH. Mechanism of trigeminal neuralgia: An ultrastructural analysis of trigeminal root specimens obtained during microvascular decompression surgery. J Neurosurg. 2002;96:532–43. doi: 10.3171/jns.2002.96.3.0532. [DOI] [PubMed] [Google Scholar]
- 9.Flickinger JC, Pollock BE, Kondziolka D, Phuong LK, Foote RL, Stafford SL, et al. Does increased nerve length within the treatment volume improve trigeminal neuralgia radiosurgery? A prospective double-blind, randomized study. Int J Radiat Oncol Biol Phys. 2001;51:449–54. doi: 10.1016/s0360-3016(01)01606-6. [DOI] [PubMed] [Google Scholar]
- 10.Foy AB, Parisi JE, Pollock BE. Histologic analysis of a human trigeminal nerve after failed stereotactic radiosurgery: Case report. Surg Neurol. 2007;68:655–8. doi: 10.1016/j.surneu.2006.11.055. [DOI] [PubMed] [Google Scholar]
- 11.Gaffey CT. The response of maximal and submaximal action potentials from frog sciatic nerve to 200-kV x-rays. Radiat Res. 1971;45:311–25. [PubMed] [Google Scholar]
- 12.Gerstner HB. Effect of high-intensity X-radiation on the A group fibers of the frog's sciatic nerve. Am J Physiol. 1956;184:333–7. doi: 10.1152/ajplegacy.1956.184.2.333. [DOI] [PubMed] [Google Scholar]
- 13.Gerstner HB, Orth JS, Richey EO. Effect of high-intensity x-radiation on velocity of nerve conduction. Am J Physiol. 1955;180:232–6. doi: 10.1152/ajplegacy.1954.180.1.232. [DOI] [PubMed] [Google Scholar]
- 14.Gorgulho A. Radiation mechanisms of pain control in classical trigeminal neuralgia. Surg Neurol Int. 2012;3(Suppl 1):S17–25. doi: 10.4103/2152-7806.91606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Gorgulho A, De Salles AA, McArthur D, Agazaryan N, Medin P, Solberg T, et al. Brainstem and trigeminal nerve changes after radiosurgery for trigeminal pain. Surg Neurol. 2006;66:127–35. doi: 10.1016/j.surneu.2006.05.016. [DOI] [PubMed] [Google Scholar]
- 16.Hodaie M, Chen DQ, Quan J, Laperriere N. Tractography delineates microstructural changes in the trigeminal nerve after focal radiosurgery for trigeminal neuralgia. PloS One. 2012;7:e32745. doi: 10.1371/journal.pone.0032745. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Kondziolka D, Lacomis D, Niranjan A, Mori Y, Maesawa S, Fellows W, et al. Histological effects of trigeminal nerve radiosurgery in a primate model: Implications for trigeminal neuralgia radiosurgery. Neurosurgery. 2000;46:971–6. doi: 10.1097/00006123-200004000-00038. [DOI] [PubMed] [Google Scholar]
- 18.Kondziolka D, Lunsford LD, Flickinger JC, Young RF, Vermeulen S, Duma CM, et al. Stereotactic radiosurgery for trigeminal neuralgia: A multiinstitutional study using the gamma unit. J Neurosurg. 1996;84:940–5. doi: 10.3171/jns.1996.84.6.0940. [DOI] [PubMed] [Google Scholar]
- 19.Lazzara BM, Ortiz O, Bordia R, Witten MR, Haas JA, Katz AJ, et al. Cyberknife radiosurgery in treating trigeminal neuralgia. J Neurointerv Surg. 2013;5:81–5. doi: 10.1136/neurintsurg-2011-010125. [DOI] [PubMed] [Google Scholar]
- 20.Lim M, Villavicencio AT, Burneikiene S, Chang SD, Romanelli P, McNeely L, et al. CyberKnife radiosurgery for idiopathic trigeminal neuralgia. Neurosurg Focus. 2005;18:E9. doi: 10.3171/foc.2005.18.5.10. [DOI] [PubMed] [Google Scholar]
- 21.Love S, Coakham HB. Trigeminal neuralgia: Pathology and pathogenesis. Brain. 2001;124:2347–60. doi: 10.1093/brain/124.12.2347. [DOI] [PubMed] [Google Scholar]
- 22.Love S, Hilton DA, Coakham HB. Central demyelination of the Vth nerve root in trigeminal neuralgia associated with vascular compression. Brain Pathol. 1998;8:1–11. doi: 10.1111/j.1750-3639.1998.tb00126.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Massager N, Lorenzoni J, Devriendt D, Desmedt F, Brotchi J, Levivier M. Gamma knife surgery for idiopathic trigeminal neuralgia performed using a far-anterior cisternal target and a high dose of radiation. J Neurosurg. 2004;100:597–605. doi: 10.3171/jns.2004.100.4.0597. [DOI] [PubMed] [Google Scholar]
- 24.Regis J, Arkha Y, Yomo S, Murata N, Roussel P, Donnet A, et al. Radiosurgery in trigeminal neuralgia: Long-term results and influence of operative nuances. Neurochirurgie. 2009;55:213–22. doi: 10.1016/j.neuchi.2009.01.020. [DOI] [PubMed] [Google Scholar]
- 25.Regis J, Bartolomei F, Metellus P, Rey M, Genton P, Dravet C, et al. Radiosurgery for trigeminal neuralgia and epilepsy. Neurosurg Clin N Am. 1999;10:359–77. [PubMed] [Google Scholar]
- 26.Rogers CL, Shetter AG, Fiedler JA, Smith KA, Han PP, Speiser BL. Gamma knife radiosurgery for trigeminal neuralgia: The initial experience of The Barrow Neurological Institute. Int J Radiat Oncol Biol Phys. 2000;47:1013–9. doi: 10.1016/s0360-3016(00)00513-7. [DOI] [PubMed] [Google Scholar]
- 27.Schwarz W, Fox JM. Effects of monochromatic X-radiation on the membrane of nodes of Ranvier under voltage and current clamp conditions. Experientia. 1979;35:1200–1. doi: 10.1007/BF01963288. [DOI] [PubMed] [Google Scholar]
- 28.Smith ZA, Gorgulho AA, Bezrukiy N, McArthur D, Agazaryan N, Selch MT, et al. Dedicated linear accelerator radiosurgery for trigeminal neuralgia: A single-center experience in 179 patients with varied dose prescriptions and treatment plans. Int J Radiat Oncol Biol Phys. 2011;81:225–31. doi: 10.1016/j.ijrobp.2010.05.058. [DOI] [PubMed] [Google Scholar]
- 29.Szeifert GT, Salmon I, Lorenzoni J, Massager N, Levivier M. Pathological findings following trigeminal neuralgia radiosurgery. Prog Neurol Surg. 2007;20:244–8. doi: 10.1159/000100167. [DOI] [PubMed] [Google Scholar]
- 30.Watanabe T, Saito N, Hirato J, Shimaguchi H, Fujimaki H, Sasaki T. Facial neuropathy due to axonal degeneration and microvasculitis following gamma knife surgery for vestibular schwannoma: A histological analysis. Case report. J Neurosurg. 2003;99:916–20. doi: 10.3171/jns.2003.99.5.0916. [DOI] [PubMed] [Google Scholar]
- 31.Zhao ZF, Yang LZ, Jiang CL, Zheng YR, Zhang JW. Gamma Knife irradiation-induced histopathological changes in the trigeminal nerves of rhesus monkeys. J Neurosurg. 2010;113:39–44. doi: 10.3171/2010.1.jns091116. [DOI] [PubMed] [Google Scholar]