

Abstract
Purpose
To report the effects of aflibercept on eyes with large retinal pigment epithelial detachment (PED) associted with polypoidal choroidal vasculopathy (PCV).
Methods
We reviewed the medical records of patients with PEDs associated with PCV that were treated with aflibercept after intravitreal ranibizumab had failed.
Results
Three eyes of patients aged 72, 79, and 80 years were studied. Reflective material was seen in the PED along the outer surface of the retinal pigment epithelium (RPE) by spectral-domain optical coherence tomography (SD-OCT). A complete resolution of the serous PEDs was found after two aflibercept injections; however, all eyes had a fibrovascular PED. In addition, one eye developed a retinal hemorrhage and a recurrent PED just after the third injection of aflibercept. The visual acuity in this eye decreased from 10/20 to 2/20.
Conclusion
The reflective material below the outer surface of the RPE in serous PED suggests the presence of neovascularization. Intravitreal aflibercept could be considered for large PEDs in eyes with PCV but should be carefully applied.
Keywords: age-related macular degeneration, retinal pigment epithelial detachment, polypoidal choroidal vasculopathy, aflibercept
Introduction
Intravitreal injections of pegaptanib or bevacizumab have been reported to be efficacious and safe treatments for retinal pigment epithelial detachments (PEDs) associated with occult choroidal neovascularization (CNV) secondary to age-related macular degeneration (AMD).1 Aflibercept, a recombinant fusion protein, has a higher binding affinity for vascular endothelial growth factor (VEGF), and it has been shown to be beneficial for patients with AMD who were refractory to multiple injections of either bevacizumab or ranibizumab.2,3 In addition, a recent study showed that intravitreal aflibercept may be an effective treatment for serous PEDs in which bevacizumab and ranibizumab were not effective.4
We report three cases of polypoidal choroidal vasculopathy (PCV) with a large PED that was refractory to ranibizumab but responded to intravitreal aflibercept. We present our spectral domain optical coherence tomographic (SD-OCT) findings, which provided some evidence on the development of the PED.
Case reports
Case 1
A 79-year-old man presented with a large serous PED. Fluorescein angiography (FA) displayed an occult CNV, and indocyanine green (IA) images showed a PCV. At the initial visit, his best-corrected visual acuity (BCVA) was 2/20 oculus sinister (OS). Three monthly injections of ranibizumab slightly flattened the PED and reduced the subretinal fluid (SRF), but a recurrence developed. Three additional monthly injections of ranibizumab (total of six injections) did not improve the PED, and there was an increase of the highly reflective material beneath the outer surface of the RPE in the SD-OCT images.
We switched to aflibercept and, after one intravitreal injection, the PED was slightly flattened; two additional injections of aflibercept were given, which flattened the PED over the hyper-reflective material observed by SD-OCT. The BCVA remained at 2/20 OS (Figure 1).
Figure 1.
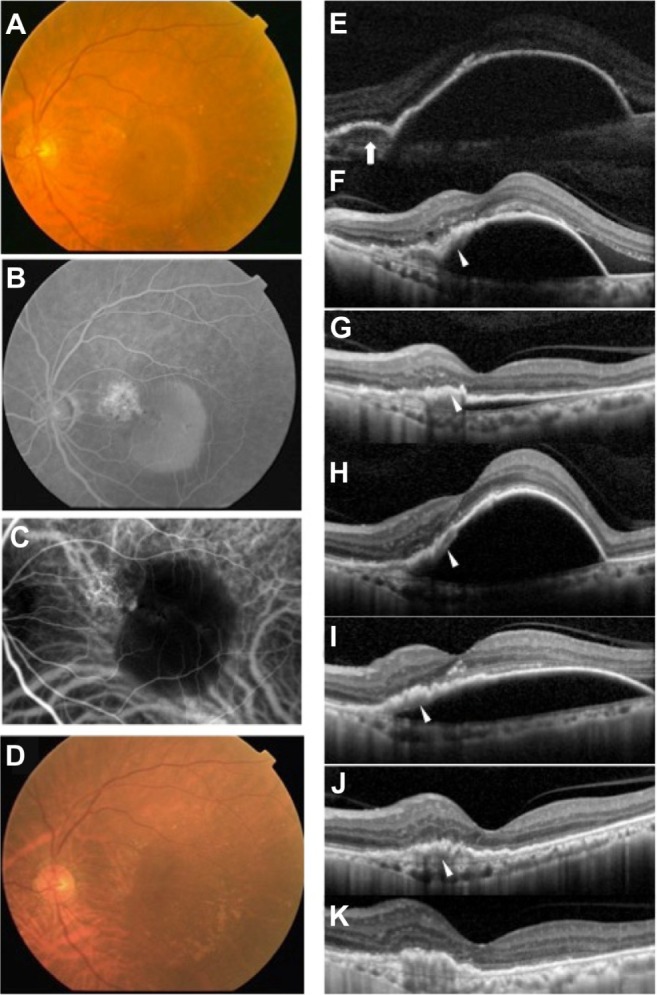
Findings from case 1, a 79-year-old Japanese man with a large PED in the left eye with PCV.
Notes: (A) Fundus photograph of the left eye at the initial examination showing a large serous retinal PED. His BCVA was 2/20 OS. (B) FA image of the left eye at the initial visit showing late leakage at the base of the PED suggestive of occult CNV and pooling of dye within the serous PED. (C) IA images at the initial visit showing hyperfluorescent spots in the choroidal circulation at the base of the PED suggesting the presence of polyps and hypofluorescence in the serous PED lesion. (D) Fundus photograph taken after three monthly aflibercept injections. The large serous PED is not present. (E) SD-OCT images of the left eye at the initial examination showing a large serous PED with SRF. The PED appears to be optically empty. Reflective material beneath the RPE layer (white arrow) suggestive of an occult CNV was detected that corresponded to the lesion of late leakage by FA. (F) SD-OCT image 6 months after three monthly injections of ranibizumab. Three monthly injections of ranibizumab slightly flattened the PED and reduced the SRF. However 6 months later, recurrent SRF and PED were observed. Hyper-reflective materials (white arrowhead) beneath the outer surface of the RPE can be seen. (G) SD-OCT image showing near resolution of the PED with complete resolution of the SRF after three additional monthly injections of ranibizumab (total of six injections). Sub-RPE materials (white arrowhead) can be seen even though the PED is collapsed. (H) One month after the last injection of ranibizumab, a recurrent large PED can be seen. (I) Flattened PED 2 weeks after a single aflibercept injection. Sub-RPE materials (white arrowhead) can be seen. (J) A complete resolution of the PED after the second injection of aflibercept, although reflective materials (white arrowhead), suggesting fibrovascular tissue, can be seen within the PED beneath the RPE layer. (K) SD-OCT image of (D). After three monthly injections of aflibercept, complete resolution of PED had a fibrovascular PED. BCVA remained 2/20 OS.
Abbreviations: BCVA, best-corrected visual acuity; CNV, choroidal neovascularization; FA, fluorescein angiography; IA, indocyanine green; OS, oculus sinister; PCV, polypoidal choroidal vasculopathy; PED, pigment epithelial detachment; RPE, retinal pigment epithelium; SD-OCT, spectral domain optical coherence tomographic; SRF, subretinal fluid.
Case 2
A 72-year-old man presented with a large serous PED in his right eye associated with a PCV. His BCVA was 14/20 OD. He had received six ranibizumab injections over a 10-month period, but the PED worsened and the SRF recurred. Hyper-reflective materials were seen beneath the outer surface of the RPE in the SD-OCT images. The BCVA decreased to 8/20 OD.
Two monthly injections of aflibercept resulted in a complete resolution of the serous PED; however, the flattened PED contained fibrovascular material beneath the RPE layer in the SD-OCT images.
Case 3
An 80-year-old man presented with a large serous PED. FA displayed an occult CNV, and IA images showed a PCV. His BCVA was 10/20 OS. Three monthly injections of ranibizumab slightly flattened the PED, but a recurrence was observed after 3 months. Three additional monthly injections of ranibizumab (total of six injections) failed to reduce the PED, and hyper-reflective materials were seen beneath the outer surface of the RPE in the SD-OCT images. We switched to aflibercept, and after the two additional monthly injections, an exudative CNV lesion was observed instead of the serous PED. OCT showed a loss of optical free space and highly reflective materials, suggesting the formation of fibrovascular PED. One day after the third monthly injection of aflibercept, a subretinal hemorrhage and recurrent PED were observed. BCVA was reduced to 2/20 (Figure 2).
Figure 2.
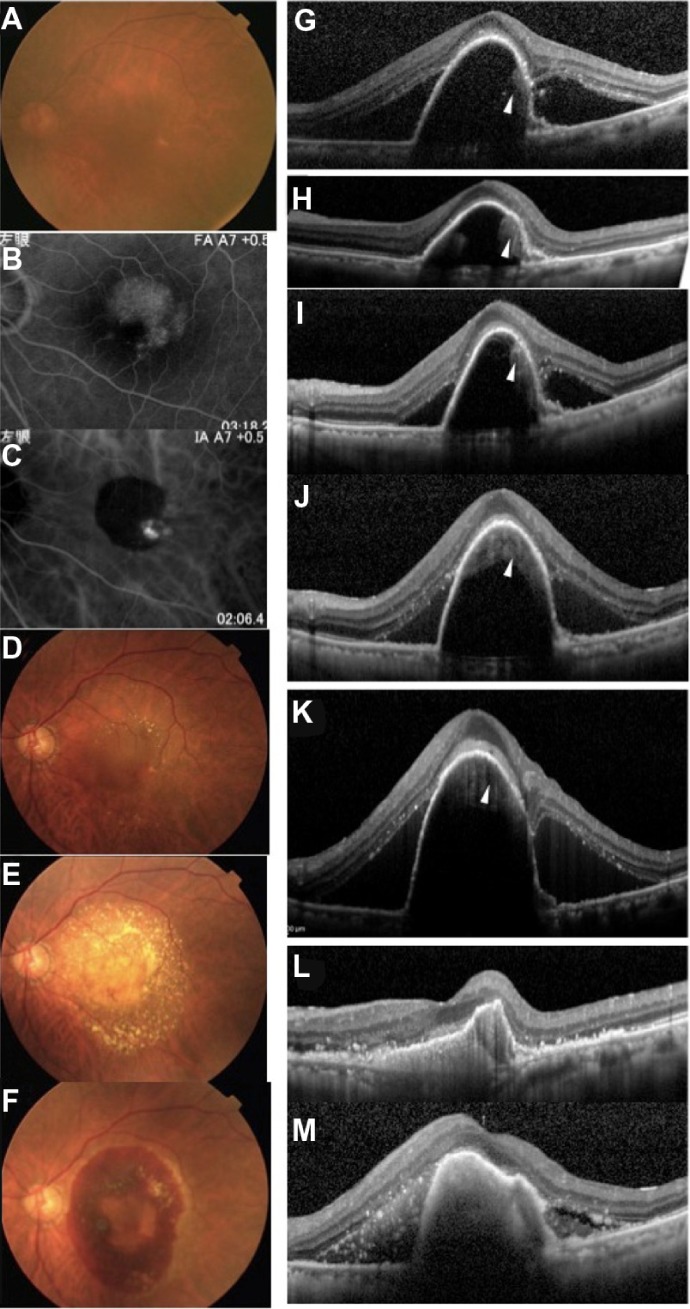
Images from case 3, an 80-year-old Japanese man with a large PED associated with a PCV in the left eye.
Notes: (A–C and G). Images at the initial visit. (A) Fundus photograph of the left eye at the initial visit shows a large serous PED. His BCVA was 10/20 OS. (B) FA images of the left eye at the initial visit showing late leakage at the base of the PED suggestive of an occult CNV and pooling of dye within the serous PED. (C) IA image showing hyperfluorescent spots from the choroidal circulation at the base of the PED suggestive of polyps and hypofluorescence in the PED lesion. (D) Fundus photograph after a single injection of aflibercept. The large serous PED is still present. (E) After two monthly injections of aflibercept, an exudative lesion with small hemorrhages can be seen instead of the serous PED. Yellowish precipitates are faintly seen in the subretinal space. (F) One day after the third monthly injection of aflibercept. The patient reported a central dark spot, a scotoma, in his left eye. Fundus photograph shows the presence of a subretinal hemorrhage and a recurrent PED. The PED was hemorrhagic. The BCVA was reduced to 2/20. (G–M) SD-OCT images of the left eye. (G) SD-OCT shows a large serous PED with SRF at the initial examination. The PED is optically empty but hyper-reflective materials (white arrowheads) can be seen beneath the outer surface of the RPE. Hyper-reflective materials located at the base of the temporal side of the PED, corresponding to the late leakage by FA, suggesting an occult CNV lesion, can be seen beneath the RPE layer. (H) SD-OCT image showing that three monthly injections of ranibizumab slightly flattened the PED and reduced the SRF. (I) Three months after the last injection of ranibizumab, a recurrence of the SRF and PED are observed. Hyper-reflective materials (white arrowhead) can be seen along the outer surface of the RPE. (J) SD-OCT shows that the PED with SRF enlarged despite three additional monthly ranibizumab injections (total of six injections). Hyper-reflective materials (white arrowhead) from the back surface of the RPE layer were increased. (K) SD-OCT image of (D). A single aflibercept injection did not resolve the PED and SRF but worsened. (L) SD-OCT image of (E). After two monthly injections of aflibercept, a near resolution of PED with complete resolution of SRF can be seen. However, hyper-reflective materials, suggesting the existence of fibrovascular PED, are present beneath the RPE layer. (M) SD-OCT image of (F). After three monthly injections of aflibercept, a recurrent large PED with SRF can be seen. Hyper-reflective materials reflecting hemorrhages in the subretinal space and PED space were detected. BCVA was reduced to 2/20.
Abbreviations: BCVA, best-corrected visual acuity; CNV, choroidal neovascularization; FA, fluorescein angiography; IA, indocyanine green; OS, oculus sinister; PCV, polypoidal choroidal vasculopathy; PED, pigment epithelial detachment; RPE, retinal pigment epithelium; SD-OCT, spectral domain optical coherence tomographic; SRF, subretinal fluid.
Discussion
We found from three cases that intravitreal injections of aflibercept reduced or flattened large serous PEDs associated with PCV that were refractory to ranibizumab. Bird and Marshall5 and Casswell et al6 proposed that an interaction between the RPE and the Bruch membrane was central to the development of a PED, and they were not mutually exclusive.7 Alternatively, Gass8 proposed that PEDs in eyes with AMD occurred by neovascular ingrowth with subsequent exudation from the new vessels.
It is well known that PCVs frequently accompany PEDs.9 We found highly reflective materials within the serous PED beneath the outer surface of the RPE in all three cases. After aflibercept treatment, all of our cases had an apparent contracture of the accumulated material. This suggested the presence of fibrovascular tissues within the flattened PED. This is supported by the findings of Spaide,10 who examined the internal structure of PEDs in eyes with AMD and found that PEDs frequently have reflective materials on the back surface of the RPE, suggestive of CNV. These findings can be explained by the hypothesis presented by Gass8 on PED formation.
We found a sudden subretinal hemorrhage and recurrent PED in case 3. Following anti-VEGF therapy, a contracture of fibrovascular tissue has been reported in eyes with proliferative diabetic retinopathy.11 We suggest that aflibercept therapy may have enhanced fibrosis of neovascular tissues and caused a traction of the vessels, which then resulted in a sudden subretinal hemorrhage and a recurrence of the PED.
In conclusion, the reflective material below the outer surface of the RPE in serous PEDs suggests the presence of neovascularization. Intravitreal aflibercept could be considered for large PEDs in eyes with PCV but should be carefully applied.
Footnotes
Disclosure
The authors have no conflict of interest to declare in this work.
References
- 1.Arias L. Treatment of retinal pigment epithelial detachment with antiangiogenic therapy. Clin Ophthalmol. 2010;4:369–374. doi: 10.2147/opth.s9307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Bakall B, Folk JC, Boldt HC, et al. Aflibercept therapy for exudative age-related macular degeneration resistant to bevacizumab and ranibizumab. Am J Ophthalmol. 2013;156(1):15–22. doi: 10.1016/j.ajo.2013.02.017. [DOI] [PubMed] [Google Scholar]
- 3.Cho H, Shah CP, Weber M, Heier JS. Aflibercept for exudative AMD with persistent fluid on ranibizumab and/or bevacizumab. Br J Ophthalmol. 2013;97(8):1032–1035. doi: 10.1136/bjophthalmol-2013-303344. [DOI] [PubMed] [Google Scholar]
- 4.Patel KH, Chow CC, Rathod R, et al. Rapid response of retinal pigment epithelial detachments to intravitreal aflibercept in neovascular age-related macular degeneration refractory to bevacizumab and ranibizumab. Eye (Lond) 2013;27(5):663–667. doi: 10.1038/eye.2013.31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bird AC, Marshall J. Retinal pigment epithelial detachments in the elderly. Trans Ophthalmol Soc U K. 1986;105(Pt 6):674–682. [PubMed] [Google Scholar]
- 6.Casswell AG, Kohen D, Bird AC. Retinal pigment epithelial detachments in the elderly: classification and outcome. Br J Ophthalmol. 1985;69(6):397–403. doi: 10.1136/bjo.69.6.397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Singerman LJ, Stockfish JH. Natural history of subfoveal pigment epithelial detachments associated with subfoveal or unidentifiable choroidal neovascularization complicating age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 1989;227(6):501–507. doi: 10.1007/BF02169440. [DOI] [PubMed] [Google Scholar]
- 8.Gass JD. Drusen and disciform macular detachment and degeneration. Trans Am Ophthalmol Soc. 1972;70:409–436. [PMC free article] [PubMed] [Google Scholar]
- 9.Saito M, Iida T, Nagayama D. Cross-sectional and en face optical coherence tomographic features of polypoidal choroidal vasculopathy. Retina. 2008;28(3):459–464. doi: 10.1097/IAE.0b013e318156db60. [DOI] [PubMed] [Google Scholar]
- 10.Spaide RF. Enhanced depth imaging optical coherence tomography of retinal pigment epithelial detachment in age-related macular degeneration. Am J Ophthalmol. 2009;147(4):644–652. doi: 10.1016/j.ajo.2008.10.005. [DOI] [PubMed] [Google Scholar]
- 11.Arevalo JF, Maia M, Flynn HW, Jr, et al. Tractional retinal detachment following intravitreal bevacizumab (Avastin) in patients with severe proliferative diabetic retinopathy. Br J Ophthalmol. 2008;92(2):213–216. doi: 10.1136/bjo.2007.127142. [DOI] [PubMed] [Google Scholar]