

Abstract
Background and Purpose
Systemic hypertension has long been considered as a risk factor of aneurysmal rupture. However, a causal link between systemic hypertension and the development of aneurysmal rupture has not been established. In this study, using a mouse model of intracranial aneurysm rupture, we examined the roles of systemic hypertension in the development of aneurysmal rupture.
Methods
Aneurysms were induced by a combination of deoxycorticosterone acetate (DOCA)-salt induced hypertension and a single injection of elastase into the cerebrospinal fluid in mice. Anti-hypertensive treatment was started six days after aneurysm induction. Aneurysmal rupture was detected by neurological symptoms and confirmed by the presence of intracranial aneurysm with subarachnoid hemorrhage. Hydralazine (direct vasodilator) or the discontinuation of the DOCA-salt treatment was used to assess the roles of systemic hypertension. Captopril (angiotensin converting enzyme inhibitor) or losartan (angiotensin II type 1 receptor antagonist) was used to assess the roles of the local renin-angiotensin system in the vascular wall.
Results
Normalization of blood pressure by hydralazine significantly reduced the incidence of ruptured aneurysms and the rupture rate. There was a dose dependent relationship between the reduction of blood pressure and the prevention of aneurysmal rupture. Captopril and losartan were able to reduce the rupture rates without affecting systemic hypertension induced by DOCA-salt treatment.
Conclusions
Normalization of blood pressure after aneurysm formation prevented aneurysmal rupture in mice. In addition, we found that the inhibition of the local renin-angiotensin system independent from the reduction of blood pressure can prevent aneurysmal rupture.
Keywords: Intracranial aneurysm rupture, hypertension, angiotensin, animal model
Introduction
Systemic hypertension has long been considered as a risk factor of aneurysmal rupture.1, 2 However, findings from clinical studies are conflicting, presumably due to the fact that the majority of patients with a diagnosis of hypertension are treated with anti-hypertensive agents,3, 4 and as a result, these patients tend to have normal blood pressure at the time of diagnosis of intracranial aneurysm.5 While experimental studies showed a link between the formation of intracranial aneurysms and systemic hypertension,6–10 a causal link between systemic hypertension and the development of subarachnoid hemorrhage—aneurysmal rupture— has not been fully established in either experimental or clinical setting.
In patients with systemic hypertension, different types of anti-hypertensive agents with different molecular targets are chosen based on the types of end-organ damages and underlying pathophysiology.2 However, it is not clear which type of anti-hypertensive agents may be suitable for patients with unruptured aneurysms, or which type of anti-hypertensive agents can reduce aneurysmal subarachnoid hemorrhage.
Hypertension may directly or indirectly contribute to aneurysmal rupture. Hypertension may weaken the aneurysmal wall by directly increasing mechanical stresses. In addition, activation of local renin-angiotensin system by systemic hypertension can cause vascular inflammation and remodeling11 and may contribute to aneurysmal rupture. Certain polymorphisms in the genes related to renin-angiotensin system are reported to be associated with aneurysmal rupture.12–14
Recently, we have developed a mouse model of intracranial aneurysm that morphologically and histologically resemble human intracranial aneurysms.9, 15 In this model, aneurysmal rupture causes neurological symptoms that can be easily detected by a simple neurological examination.16, 17 This model provides a unique opportunity to conduct preclinical studies for identifying therapeutic targets for the prevention of aneurysmal rupture. Utilizing this mouse model of intracranial aneurysm, we examined the roles of systemic hypertension and the local renin-angiotensin system in the mechanisms for the rupture of intracranial aneurysms.
Methods
Experiments were conducted in accordance with the guidelines approved by the University of California, San Francisco, Institutional Animal Care and Use Committee. Intracranial aneurysms were induced in 8–10 week-old male mice (C57BL/6J, Jackson Laboratory) as previously described.9, 18,17 We combined induced systemic hypertension and a single injection of elastase into the cerebrospinal fluid at the right basal cistern.9, 18,17 (Detailed methods are presented in the online supplements.)
To induce systemic hypertension, we used deoxycorticosterone acetate-salt hypertension (DOCA-salt hypertension).19 Mice underwent nephrectomy followed by an implantation of DOCA pellet one week later; 1% sodium chloride drinking water was started on the same day as the DOCA pellet implantation.15, 19 Mice received a single injection of elastase (0.035 units) into the cerebrospinal fluid at the right basal cistern on the same day as DOCA pellet implantation. Aneurysms were defined as a localized outward bulging of the vascular wall, whose diameter was greater than the parent artery diameter.9, 18
To detect aneurysmal rupture, two blinded observers performed daily neurological examination as previously described.17 Neurological symptoms were scored as followings; 0: normal function; 1: reduced eating or drinking activity demonstrated by a weight loss greater than two grams of body weight (approximately 10% weight loss) over 24 hours; 2: flexion of the torso and forelimbs upon lifting of the whole animal by the tail; 3: circling to one side with a normal posture at rest; 4: leaning to one side at rest; 5: no spontaneous activity. We have shown that this neurological testing system is sensitive and specific for detecting aneurysmal rupture in this model.17 Mice were sacrificed when they developed neurological symptoms (score 1–5). All asymptomatic mice were sacrificed 28 days after aneurysm induction. The brain samples were perfused with phosphate-buffered saline, followed by a gelatin containing blue dye in order to visualize cerebral arteries. Two blinded observes assessed aneurysm formation and subarachnoid hemorrhage. Rupture rate was defined as the total number of mice with ruptured aneurysms divided by the number of mice with any aneurysms.17 Figure 1 shows representative mouse with normal cerebral arteries, an unruptured aneurysm from a mouse that was asymptomatic throughout the experimental period, and a ruptured aneurysm with subarachnoid hemorrhage from a mouse that became symptomatic 12 days after aneurysm induction.
Figure 1. Representative intracranial aneurysms.
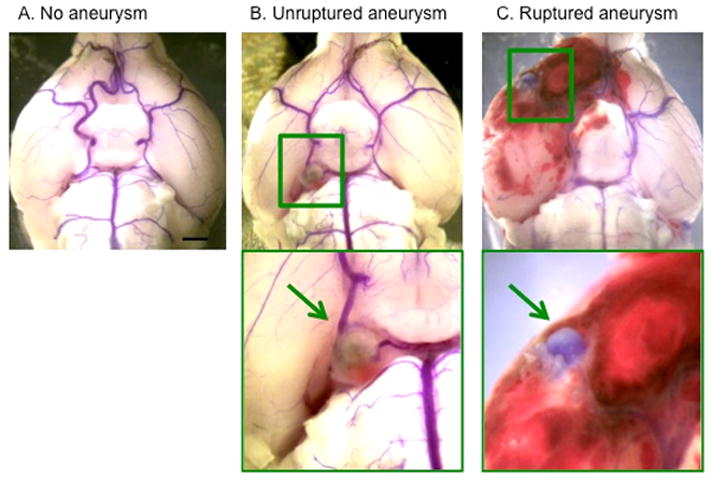
A: Normal cerebral arteries. B: Unruptured aneurysm in the posterior cerebral artery. C: Ruptured aneurysm with subarachnoid hemorrhage. Cerebral arteries were visualized by blue dyes dissolved in gelatin. Arrows indicate aneurysms.
Our previous study found that aneurysm formation happens during first 6 days after aneurysm induction and aneurysmal rupture start occurring approximately 7 days after the aneurysm induction in this model.17 We found that by treating the mice with an experimental agent stating from 6 days after aneurysm induction, we can test whether the experimental agent can reduce the rupture rate.17 Therefore, in this study, the treatments with anti-hypertensive agents were started 6 days after aneurysm induction and continued for two weeks.
Statistical Analysis
Primary outcomes were the incidence of unruptured intracranial aneurysms and the rupture rate (number of mice with ruptured aneurysm/number of mice with ruptured or unruptured aneurysms). We used Fisher’s exact test for the analysis of primary outcomes. As an exploratory analysis, the survival analysis was performed using the Log-rank test. Mice that did not develop aneurysms were excluded in the survival analysis. Blood pressure and body weight were analyzed by ANOVA, followed by the Tukey-Kramer post hoc test. All of the results were expressed as mean ± SD. Statistical significance was considered at P < 0.05.
Results
Effect of normalization of blood pressure on the development of aneurysmal rupture
As a first step to examine the contributions of systemic hypertension to aneurysmal rupture, we tested effects of normalization of systemic hypertension after aneurysmal formation on the development of aneurysmal rupture. We used hydralazine to normalize the blood pressure. Hydralazine, a direct vasodilator, can normalize systemic hypertension induced by DOCA-salt hypertension without directly affecting the renin-angiotensin system.19 The hydralazine treatment (25 or 50 mg/kg/day in drinking water)19, 20 was started 6 days after aneurysm induction and continued for two weeks (Figure 2A). The control group received drinking water without hydralazine.
Figure 2. Normalization of blood pressure by hydralazine reduced the incidence of ruptured aneurysms and the rupture rates.
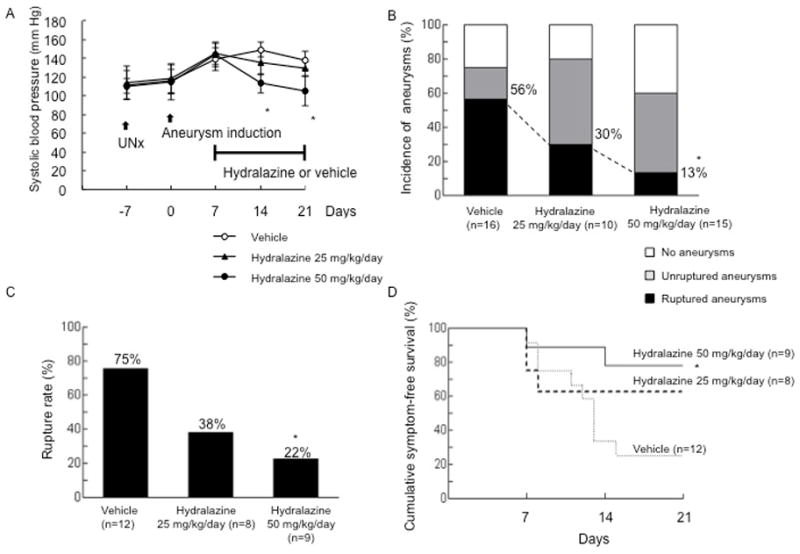
A: Blood pressure. B: Incidence of ruptured and unruptured aneurysms. C: Rupture rate. D. Survival curve. Survival curves were constructed after excluding those mice that did not have aneurysms so that the curves mimic clinical settings.
As shown in Figure 2A, systemic hypertension was successfully induced in the mice receiving the DOCA-salt treatment. The hydralazine at 50 mg/kg/day that was started 6 days after aneurysm induction effectively normalized blood pressure. The lower dose of hydralazine (25 mg/kg/day) partially normalized blood pressure. Normalization of blood pressure by hydralazine did not significantly affect the formation of aneurysms, as demonstrated by no difference in the total incidence of aneurysms (i.e., the incidence of both ruptured and unruptured aneurysms) between two groups (75 vs. 60%, P = 0.46) (Figure 2B). However, normalization of blood pressure by hydralazine (50 mg/kg/day) significantly reduced the incidence of ruptured aneurysms and the rupture rate (incidence of ruptured aneurysms: 56 vs. 13%, P < 0.05; rupture rate: 75 vs. 22%, P < 0.05) (Figures 2B and 2C). There was a trend for partial normalization of blood pressure by the lower dose of hydralazine (25 mg/kg/day) to reduce the rupture rate (incidence of ruptured aneurysms: 56 vs. 30 %, P = 0.25; rupture rate: 75 vs. 38 %, P = 0.17). Taken together, there was a dose dependent effect of the blood pressure reduction on the development of aneurysmal rupture. For the purpose of exploratory analysis, a symptom-free curve (Kaplan-Meier analysis curve) was plotted after excluding mice that did not have aneurysms (Figure 2D). A log-rank test revealed a significant reduction of aneurysmal rupture with the normalization of blood pressure by hydralazine (P < 0.05).
As a next step to further confirm the critical role of hypertension in the development of aneurysmal rupture, we tested whether a reduction of blood pressure by the discontinuation of DOCA-salt treatment reduces aneurysmal rupture. For the discontinuation of DOCA-salt treatment, we removed the DOCA pellet and switched the drinking water with water without salt at 6 days after aneurysm induction (Figure 3A). The control group received the standard DOCA-salt treatment throughout the experimental period.
Figure 3. Effects of the discontinuation of DOCA-salt treatment one week after aneurysm induction.
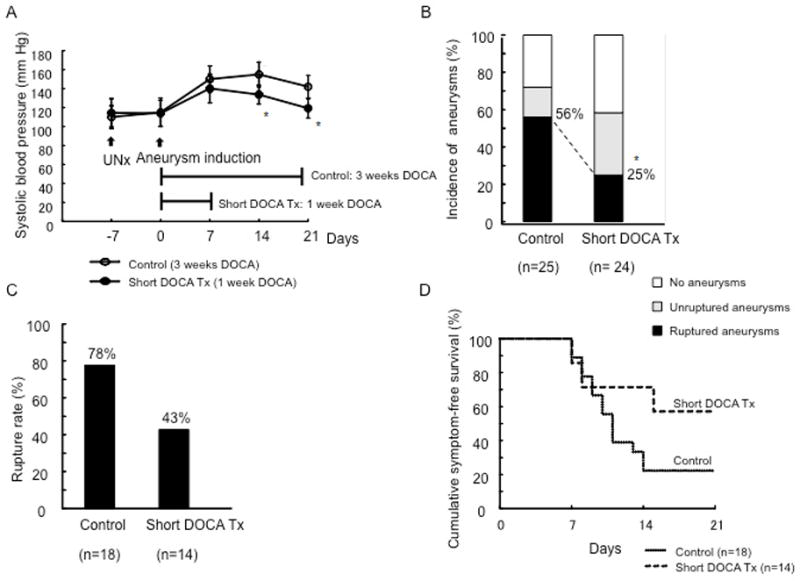
A: Blood pressure. B: Incidence of ruptured and unruptured aneurysms. C: Rupture rate. D. Survival curve.
As shown in Figure 3A, in the mice whose DOCA-salt treatment was discontinued 6 days after aneurysm induction, there was a gradual reduction of blood pressure. However, the discontinuation of DOCA-salt treatment did not completely normalize the blood pressure over the course of 2 weeks, possibility reflecting the residual effects of the DOCA-pellet or salt treatment. There was no difference in the total incidence of aneurysms (72 vs. 58%, P = 0.38) (Figure 3B). The discontinuation of the DOCA-salt treatment significantly reduced the incidence of ruptured aneurysms (P < 0.05) (Figure 3B). However, there was only a trend for the discontinuation of the DOCA-salt treatment to reduce the rupture rate (P = 0.07) (Figure 3C), probably reflecting the failure of normalization of blood pressure in this group. The improvement of survival by the discontinuation of the DOCA-salt treatment was not statistically significant (Figure 3D).
Local renin-angiotensin II system was up-regulated in aneurysmal walls
Since systemic hypertension can affect the local-renin angiotensin system in the vascular wall,19 we examined the expression of angiotensin II and angiotensin type 1 receptor (AT1 receptor) in the normal cerebral artery and intracranial aneurysms in mice. Three representative samples were used. While there was weak expression of angiotensin II and AT1 receptor in the normal cerebral artery, both angiotensin II and AT1 receptor were abundant in the mouse model of intracranial aneurysm (Figure 4).
Figure 4.
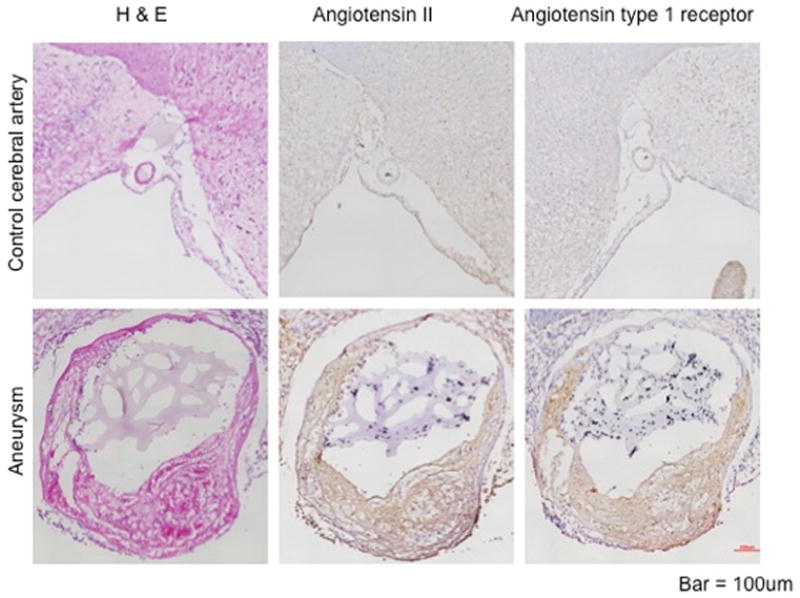
Expression of angiotensin II and angiotensin II type 1 receptor.
Roles of the local renin-angiotensin system in the development of aneurysmal rupture
To test roles of local renin-angiotensin system in the formation of aneurysms, we utilized captopril (angiotensin converting enzyme inhibitor) and losartan (AT1 antagonist) in mice with DOCA-salt hypertension. We took advantage of the ability of these agents to block the local renin-angiotensin system without affecting systemic hypertension induced by DOCA-salt hypertension.15, 19 These agents were previously used to assess the roles of the activation of the local renin-angiotensin system in the vasculature in animals that were rendered hypertensive by the DOCA-salt treatment.15, 19 The captopril and losartan doses were chosen based on the previous studies.15, 19, 21–23
The treatment with captopril (6mg/kg/day in PBS, AK Scientific) or vehicle through an implanted osmotic pump was started 6 days after aneurysm induction and continued for two weeks (Figure 5A). As expected, captopril did not affect the systemic hypertension induced by DOCA-salt treatment. While the captopril treatment started 6 days after aneurysm induction did not affect the overall incidence of aneurysms, it significantly reduced the incidence of ruptured aneurysms and the rupture rate (incidence of ruptured aneurysms: 63 vs. 24%, P < 0.05; rupture rate: 91 vs. 36%, P < 0.05) (Figure 5B and Figure 5C). The survival analysis using those mice that had aneurysms revealed a significant improvement of the survival by captopril treatment (P < 0.05) (Figure 5D).
Figure 5. Inhibition of the local renin-angiotensin system by captopril prevented aneurysmal rupture without affecting systemic hypertension.

A: Blood pressure. B: Incidence of ruptured and unruptured aneurysms. C: Rupture rate. D. Survival curve.
As a next step, we tested the effect of losartan that blocks AT1 that is the downstream from captopril’s target. The treatment with losartan (30mg/kg/day, AK Scientific) or vehicle was started 6 days after aneurysm induction. Losartan did not affect the systemic hypertension induced by the DOCA-salt treatment (Figure 6A). Similarly to the captopril treatment, the losartan treatment significantly reduced the incidence of ruptured aneurysms and the rupture rate (incidence of ruptured aneurysms: 54 vs. 24%, P < 0.05; rupture rate: 71 vs. 33%, P < 0.05) without affecting the total incidence of aneurysms (Figure 6B and 6C). The survival analysis using those mice that had aneurysms revealed a significant improvement of the survival by losartan treatment (P < 0.05) (Figure 6D).
Figure 6. Inhibition of the local renin-angiotensin system by losartan prevented aneurysmal rupture without affecting systemic hypertension.

A: Blood pressure. B: Incidence of ruptured and unruptured aneurysms. C: Rupture rate. D. Survival curve.
The inhibition of the local renin-angiotensin system by captopril or losartan without affecting systemic hypertension reduced aneurysmal rupture, suggesting a potential contribution of the activation of the local renin-angiotensin system to the development of aneurysmal rupture.
Discussion
In this study, we found that the normalization of blood pressure after aneurysm formation prevents aneurysmal rupture in mice and that there is a dose-dependent relationship between blood pressure and aneurysmal rupture, establishing the causal relationship between the normalization of blood pressure and the prevention of aneurysmal rupture for the first time. In addition, we found that the inhibition of the local renin-angiotensin system independent from the reduction of blood pressure can prevent aneurysmal rupture. These observations suggest that the activation of the local renin-angiotensin system in the aneurysmal wall presumably by systemic hypertension can induce aneurysmal rupture, at least, in a mouse model of intracranial aneurysm.
Recently, an increasing number of unruptured intracranial aneurysms have been diagnosed, primarily due to the increased use of non-invasive brain imaging techniques.24–26 Unruptured aneurysms are asymptomatic until they rupture. The 30-day mortality rate after aneurysmal subarachnoid hemorrhage is as high as 45%.27 Surgical clipping or endovascular coiling can be offered to patients with unruptured aneurysms for the prevention of aneurysmal rupture. Significant technical advancements and refinements have been made in these invasive treatments. However, the mortality and morbidity resulting from the clipping and coiling of unruptured aneurysms are not negligible.3 The one-year adverse outcome rate, including mortality and significant morbidity, can be as high as 20%.28, 29 In addition, these invasive therapies are technically intensive and costly. Therefore, the pharmacological prevention of aneurysmal rupture is an attractive alternative approach in patients with unruptured aneurysms.
Previous studies performed by our group and others have focused on the mechanisms involved in the formation of aneurysms. These efforts were based on the assumption that the processes of aneurysmal formation, growth, and rupture share similar mechanisms.8, 30 however, the mechanisms of aneurysmal rupture may be fundamentally different from those of formation and growth. In the mouse model that was used in this study, spontaneous aneurysmal rupture occurs with a predictable time course, and the aneurysmal rupture can be easily detected by assessing neurological symptoms, as presented in our recently published paper.17 This model provides us with a unique opportunity to study the mechanisms of aneurysmal rupture as well as pharmacological prevention.
In patients with hypertension, the normalization of blood pressure has been clinically proved to be effective in preventing ischemic stroke, intracerebral hemorrhage, and cardiac events. While the anti-hypertensive treatment is generally recommended for hypertensive patients with unruptured intracranial aneurysm, whether the normalization of blood pressure confers the protection against the development of aneurysmal rupture is not known. It would be practically impossible to test such question in clinical setting, as not treating hypertension is not an ethical option. However, it may be possible to test which class of anti-hypertensive agent is suitable for those hypertensive patients with unruptured aneurysms.
Systemic hypertension can affect the tissue remodeling and inflammation of the aneurysmal wall. In addition to exerting abnormal hemodynamic stresses, hypertension can activate local renin-angiotensin system that exists in the vascular wall.19 Local renin-angiotensin system can control vascular remodeling by affecting smooth muscle migration and proliferation,31 the processes that can potentially lead to the destabilization of the aneurysmal wall. In addition, it can mediate vascular inflammation through the activation of NF-kappa B which can further promote the inflammation inside the aneurysmal wall.30 Gene polymorphisms in angiotensin converting enzymes are associated with the rupture of intracranial aneurysms,12–14 suggesting a link between renin-angiotensin system and aneurysmal rupture. Taken together with our findings, the local renin-angiotensin system can be a therapeutic target for the prevention of aneurysmal rupture. There are many clinically available anti-hypertensive agents that can inhibit different steps of the local renin-angiotensin system. Anti-hypertensive agents that possess the inhibitory effects on the local renin-angiotensin system may contribute to the prevention of aneurysmal rupture not only through the normalization of blood pressure by also through the inhibition of the local renin-angiotensin system.
There are a number of limitations of this study. First, the study design of our study depended on the pharmacological approach. While the utilization of clinically available anti-hypertensive agents makes our findings readily translatable, the anti-hypertensive agents chosen for our study may not be specific to their designed targets (i.e., vascular calcium channel, angiotensin II type 1 receptor, angiotensin converting enzyme and others). These anti-hypertensive agents possess non-hemodynamic effects that can potentially affect the processes that lead to aneurysmal rupture. Another major limitation of this study is that we did not directly assess the activity of the local renin-angiotensin system. Although our immunohistochemistry data suggested the activation of the renin-angiotensin system, we were not able to measure its activity. As it was previously recognized by others, currently there is no reliable way to directly quantify the activation of the local renin angiotensin system.19
Summary
Using the mouse model of intracranial aneurysms, we revealed critical roles of systemic hypertension and the local renin-angiotensin system in the development of aneurysmal rupture. Our study may be a basis for the clinical study to find the optimal choice of anti-hypertensive agents for patients with unruptured intracranial aneurysms.
Supplementary Material
Acknowledgments
Sources of Funding
The project described was supported by Grant Number R01NS055876 (TH), R01NS082280 (TH), and P01NS044155-5202 (TH) from the National Institute of Neurological Disorders and Stroke (NIH/NINDS), American Heart Association Grant-in-aid 11GRNT6380003 (TH), and the Brain Aneurysm Foundation Shirley Dudek Demmer Chair of Research (KS). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institute Of Neurological Disorders And Stroke, the National Institutes of Health, the American Heart Association, or the Brain Aneurysm Foundation.
Footnotes
Disclosures
None
References
- 1.Schievink WI. Intracranial aneurysms. N Engl J Med. 1997;336:28–40. doi: 10.1056/NEJM199701023360106. [DOI] [PubMed] [Google Scholar]
- 2.Connolly ES, Jr, Rabinstein AA, Carhuapoma JR, Derdeyn CP, Dion J, Higashida RT, et al. Guidelines for the management of aneurysmal subarachnoid hemorrhage: A guideline for healthcare professionals from the american heart association/american stroke association. Stroke. 2012;43:1711–1737. doi: 10.1161/STR.0b013e3182587839. [DOI] [PubMed] [Google Scholar]
- 3.Wiebers DO, Whisnant JP, Huston J, 3rd, Meissner I, Brown RD, Jr, Piepgras DG, et al. Unruptured intracranial aneurysms: Natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003;362:103–110. doi: 10.1016/s0140-6736(03)13860-3. [DOI] [PubMed] [Google Scholar]
- 4.Investigators TISoUIA. Unruptured intracranial aneurysms--risk of rupture and risks of surgical intervention. International study of unruptured intracranial aneurysms investigators. N Engl J Med. 1998;339:1725–1733. doi: 10.1056/NEJM199812103392401. [DOI] [PubMed] [Google Scholar]
- 5.Juvela S. Recommendations for the management of patients with unruptured intracranial aneurysms. Stroke. 2001;32:815–816. doi: 10.1161/01.str.32.3.815. [DOI] [PubMed] [Google Scholar]
- 6.Hashimoto N, Handa H, Hazama F. Experimentally induced cerebral aneurysms in rats. Surgical neurology. 1978;10:3–8. [PubMed] [Google Scholar]
- 7.Hashimoto N, Handa H, Hazama F. Experimentally induced cerebral aneurysms in rats: Part ii. Surgical neurology. 1979;11:243–246. [PubMed] [Google Scholar]
- 8.Hashimoto T, Meng H, Young WL. Intracranial aneurysms: Links between inflammation, hemodynamics and vascular remodeling. Neurol Res. 2006;28:372–380. doi: 10.1179/016164106X14973. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Nuki Y, Tsou TL, Kurihara C, Kanematsu M, Kanematsu Y, Hashimoto T. Elastase-induced intracranial aneurysms in hypertensive mice. Hypertension. 2009;54:1337–1344. doi: 10.1161/HYPERTENSIONAHA.109.138297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Morimoto M, Miyamoto S, Mizoguchi A, Kume N, Kita T, Hashimoto N. Mouse model of cerebral aneurysm: Experimental induction by renal hypertension and local hemodynamic changes. Stroke. 2002;33:1911–1915. doi: 10.1161/01.str.0000021000.19637.3d. [DOI] [PubMed] [Google Scholar]
- 11.Muller M, van den Beld AW, Bots ML, Grobbee DE, Lamberts SW, van der Schouw YT. Endogenous sex hormones and progression of carotid atherosclerosis in elderly men. Circulation. 2004;109:2074–2079. doi: 10.1161/01.CIR.0000125854.51637.06. [DOI] [PubMed] [Google Scholar]
- 12.Keramatipour M, McConnell RS, Kirkpatrick P, Tebbs S, Furlong RA, Rubinsztein DC. The ace i allele is associated with increased risk for ruptured intracranial aneurysms. J Med Genet. 2000;37:498–500. doi: 10.1136/jmg.37.7.498. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Takenaka K, Yamakawa H, Sakai H, Yoshimura S, Murase S, Okumura A, et al. Angiotensin i-converting enzyme gene polymorphism in intracranial saccular aneurysm individuals. Neurological research. 1998;20:607–611. doi: 10.1080/01616412.1998.11740571. [DOI] [PubMed] [Google Scholar]
- 14.Slowik A, Borratynska A, Pera J, Betlej M, Dziedzic T, Krzyszkowski T, et al. Ii genotype of the angiotensin-converting enzyme gene increases the risk for subarachnoid hemorrhage from ruptured aneurysm. Stroke; a journal of cerebral circulation. 2004;35:1594–1597. doi: 10.1161/01.STR.0000131655.45227.f7. [DOI] [PubMed] [Google Scholar]
- 15.Kanematsu Y, Kanematsu M, Kurihara C, Tsou TL, Nuki Y, Liang EI, et al. Pharmacologically induced thoracic and abdominal aortic aneurysms in mice. Hypertension. 2010;55:1267–1274. doi: 10.1161/HYPERTENSIONAHA.109.140558. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Tada Y, Kanematsu Y, Kanematsu M, Nuki Y, Liang EI, Wada K, et al. A mouse model of intracranial aneurysm: Technical considerations. Acta Neurochir Suppl. 2011;111:31–35. doi: 10.1007/978-3-7091-0693-8_6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Makino H, Tada Y, Wada K, Liang EI, Chang M, Mobashery S, et al. Pharmacological stabilization of intracranial aneurysms in mice: A feasibility study. Stroke. 2012;43:2450–2456. doi: 10.1161/STROKEAHA.112.659821. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Kanematsu Y, Kanematsu M, Kurihara C, Tada Y, Tsou TL, van Rooijen N, et al. Critical roles of macrophages in the formation of intracranial aneurysm. Stroke. 2011;42:173–178. doi: 10.1161/STROKEAHA.110.590976. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Weiss D, Taylor WR. Deoxycorticosterone acetate salt hypertension in apolipoprotein e-/- mice results in accelerated atherosclerosis: The role of angiotensin ii. Hypertension. 2008;51:218–224. doi: 10.1161/HYPERTENSIONAHA.107.095885. [DOI] [PubMed] [Google Scholar]
- 20.Wilson RM, De Silva DS, Sato K, Izumiya Y, Sam F. Effects of fixed-dose isosorbide dinitrate/hydralazine on diastolic function and exercise capacity in hypertension-induced diastolic heart failure. Hypertension. 2009;54:583–590. doi: 10.1161/HYPERTENSIONAHA.109.134932. [DOI] [PubMed] [Google Scholar]
- 21.Mercure C, Prescott G, Lacombe MJ, Silversides DW, Reudelhuber TL. Chronic increases in circulating prorenin are not associated with renal or cardiac pathologies. Hypertension. 2009;53:1062–1069. doi: 10.1161/HYPERTENSIONAHA.108.115444. [DOI] [PubMed] [Google Scholar]
- 22.Dilauro M, Zimpelmann J, Robertson SJ, Genest D, Burns KD. Effect of ace2 and angiotensin-(1–7) in a mouse model of early chronic kidney disease. Am J Physiol Renal Physiol. 2010;298:F1523–1532. doi: 10.1152/ajprenal.00426.2009. [DOI] [PubMed] [Google Scholar]
- 23.Katz SA, Opsahl JA, Wernsing SE, Forbis LM, Smith J, Heller LJ. Myocardial renin is neither necessary nor sufficient to initiate or maintain ventricular hypertrophy. American journal of physiology. Regulatory, integrative and comparative physiology. 2000;278:R578–586. doi: 10.1152/ajpregu.2000.278.3.R578. [DOI] [PubMed] [Google Scholar]
- 24.Gabriel RA, Kim H, Sidney S, McCulloch CE, Singh V, Johnston SC, et al. Ten-year detection rate of brain arteriovenous malformations in a large, multiethnic, defined population. Stroke. 2010;41:21–26. doi: 10.1161/STROKEAHA.109.566018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Loumiotis I, Wagenbach A, Brown RD, Jr, Lanzino G. Small (< 10-mm) incidentally found intracranial aneurysms, part 1: Reasons for detection, demographics, location, and risk factors in 212 consecutive patients. Neurosurg Focus. 2011;31:E3. doi: 10.3171/2011.9.FOCUS11234. [DOI] [PubMed] [Google Scholar]
- 26.Brisman JL, Song JK, Newell DW. Cerebral aneurysms. The New England journal of medicine. 2006;355:928–939. doi: 10.1056/NEJMra052760. [DOI] [PubMed] [Google Scholar]
- 27.Bederson JB, Awad IA, Wiebers DO, Piepgras D, Haley EC, Jr, Brott T, et al. Recommendations for the management of patients with unruptured intracranial aneurysms: A statement for healthcare professionals from the stroke council of the american heart association. Stroke. 2000;31:2742–2750. doi: 10.1161/01.str.31.11.2742. [DOI] [PubMed] [Google Scholar]
- 28.Berman MF, Solomon RA, Mayer SA, Johnston SC, Yung PP. Impact of hospital-related factors on outcome after treatment of cerebral aneurysms. Stroke. 2003;34:2200–2207. doi: 10.1161/01.STR.0000086528.32334.06. [DOI] [PubMed] [Google Scholar]
- 29.Zacharia BE, Ducruet AF, Hickman ZL, Grobelny BT, Badjatia N, Mayer SA, et al. Technological advances in the management of unruptured intracranial aneurysms fail to improve outcome in new york state. Stroke. 2011;42:2844–2849. doi: 10.1161/STROKEAHA.111.619767. [DOI] [PubMed] [Google Scholar]
- 30.Aoki T, Nishimura M, Kataoka H, Ishibashi R, Nozaki K, Hashimoto N. Reactive oxygen species modulate growth of cerebral aneurysms: A study using the free radical scavenger edaravone and p47phox(−/−) mice. Lab Invest. 2009;89:730–741. doi: 10.1038/labinvest.2009.36. [DOI] [PubMed] [Google Scholar]
- 31.Ohkuma H, Suzuki S, Fujita S, Nakamura W. Role of a decreased expression of the local renin-angiotensin system in the etiology of cerebral aneurysms. Circulation. 2003;108:785–787. doi: 10.1161/01.CIR.0000087339.31094.3C. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.