

Abstract
Background
Cigarette rod length as a design feature may play a specific role in harm perception and tobacco use. Internal tobacco industry documents have shown targeting of females with long/ultra-long cigarettes. This study assessed trends and differences in smoking of long/ultra-long cigarettes among U.S. smokers aged ≥20 years during 1999 through 2012.
Methods
Data were obtained from the 1999/2000 through 2011/2012 National Health and Nutrition Examination Survey. The proportion of current smokers who reported using long/ultra-long cigarettes during each survey year was calculated and compared using χ2 statistics. Linear and quadratic trends during 1999 through 2012 were assessed using binary logistic regression (p<0.05). Multi-variable analyses were performed to assess current disparities in smoking of long/ultra-long cigarettes.
Results
Despite overall declines in current smoking of long/ultra-long cigarettes during the 1999 through 2012 period (p<0.001 for both linear and quadratic trends), the proportion of smokers of long/ultra-long brands increased in recent years, with over a third (38.7%) of current smokers reporting smoking of long/ultra-long cigarettes during 2011/2012. Current smokers of long/ultra-long cigarettes were more likely to be female compared to males (aOR=3.09; 95%C.I:2.09–4.58), of black race compared to whites (aOR=2.07; 95%C.I:1.30–3.28), or aged 45–64, or ≥65 years (aOR=2.39 and 5.27 respectively), compared to 18–24 year olds.
Conclusions
Specific gender, age and race/ethnic characteristics of smokers of long/ultra-long cigarettes were noted, hence potentially contributing to the widening of health disparities. Cigarette rod length should be considered an important aspect of cigarette engineering/design in regulatory efforts to reduce the burden of tobacco-related disease.
Keywords: Slim, long, design, cigarettes, tobacco, abuse liability, product appeal
1. INTRODUCTION
The initiation and continuation of tobacco use is driven not only by the pharmacologic addictiveness of tobacco products (i.e., abuse liability), but also by product design features which may increase their attractiveness to consumers and potential consumers (i.e., product appeal). The World Health Organization’s (WHO) Framework Convention on Tobacco Control Article 11 calls on member nations to ensure that no tobacco product is promoted by means that are misleading, or likely to create an erroneous impression about its health effects or relative harm (WHO, 2003). Consequently, the use of descriptors such as “light,” “low,” “mild,” or other similar labels on tobacco products has been banned in the U.S., the European Union, as well as several low and middle income countries, including South Africa, Seychelles, Togo, India, Nepal and Philippines (Centers for Disease Control and Prevention, (CDC), 2010; European Commission, 2013, Campaign for Tobacco-Free Kids, 2013).
As in several other countries (Euromonitor International, 2013), cigarettes available in the U.S. are categorized into four lengths: Regular (68–72mm); King (79–88mm); Long (94–101mm); and Ultra-long (110–121mm), with regular and ultra-long brands accounting for just small segments of the total U.S. domestic market share (3% and 2% respectively in 2011; Federal Trade Commission (FTC), 2013). Although King size cigarettes have dominated the U.S. cigarette market (59% of the total market shares in 2011), long brands have seen a growth in total domestic market shares in recent years (from 30% in 2008 to 37% in 2011; FTC, 2013). Similar upward trends in market shares for long brands have also been reported in several other countries during 2008 to 2012, including Georgia (2.6% to 9.5%), Egypt (8.5% to 12.5%), Russia (9.7% to 13.2%), Hungary (12.0% to 21.0%), and Croatia (13.2% to 23.8%). In addition, during 2012, long brands held a relatively large percentage of the cigarette market in the United Kingdom (22.3%), Turkey (27%), South Korea (34%), and Romania (35%) (Euromonitor International, 2013). It is interesting to note the emergence of long and slim design features in novel products such as electronic cigarettes.
These market shifts in favor of long brands in several countries around the world may provide some insight into consumer behavior at a population level, and further highlight the need for more research on risk perceptions and health communication. Previous research has shown that aesthetic features of cigarettes including stick color, length, and branding design elements such as patterns and logos may also be associated with increased appeal and altered risk perception among smokers (Borland and Savvas, 2013; Kotnowski and Hammond, 2013; Mutti et al., 2011; Ford et al., 2013a). In addition, internal tobacco industry documents have shown that long/ultra-long cigarettes were particularly attractive among certain population subgroups based on the perceptions that such longer brands were more sophisticated and modern products with a particular appeal to limited typological groups such as women, and people of a higher status, and were designed especially to be used in social situations where added length would be fully appreciated both in terms of extended enjoyment and the added status value (Carpenter et al., 2005, 2007).
A closer examination of cigarette design characteristics and their effect on product appeal and smoking susceptibility is important, given the enormous health and economic burden of smoking in the U.S. (CDC, 2008). Targeted product marketing may also result in disparities in tobacco use and its aftermaths. Hence, an assessment of demographic differences in receptivity to tobacco marketing may help in formulating tailored policies to reduce such disparities. In addition, more information on cigarette design features in the U.S. is warranted and timely given that product standardization is starting to appear on the international tobacco control agenda, e.g., in Australia, as part of the plain packaging legislation, and in the European Union, as envisaged in the European Commission’s draft Tobacco Products Directive (Australian Government, 2013; European Commission, 2013).
While several studies have assessed design features such as packaging, “light cigarettes,” flavors and other smoke-masking design features (Ford et al., 2013a; Behm et al., 2013; Caruso and O'Connor, 2012; Carpenter et al., 2005b; Kennedy et al., 2013), little population-based information exists on cigarette rod length as a design characteristic. To fill this gap in knowledge, this study assessed trends and correlates in current smoking of regular, king size, and long/ultra-long cigarettes among U.S. adults aged ≥20 years during 1999 through 2012 using nationally representative data from the National Health and Nutrition Examination Survey (NHANES).
2. METHODS
2.1 Sources of data
NHANES is a household interview and examination survey that uses a complex multi-stage probability sampling design to select participants from the non-institutionalized U.S. population (CDC, 1999). We analyzed seven consecutive waves of the NHANES, with overall response rates (%) and sample sizes (n) for the interviewed sample by survey year as follows: 1999/2000 (82.0%; n = 4,880), 2001/2002 (84.0%; n = 5,411); 2003/2004 (79.0%; n = 5,041); 2005/2006 (80.5%; n = 4,979); 2007/2008 (78.4%; n = 11,870); 2009/2010 (79.4%; n = 6,218) and 2011/2012 (72.6%; n = 9,756).
2.2 Measures
2.2.1 Current Cigarette Smoking
Current cigarette smokers were respondents who had smoked ≥100 cigarettes during their lifetimes and, at the time of interview, reported smoking every day or on some days.
2.2.2 Cigarette Rod length
Cigarette brand in NHANES was assessed among respondents aged ≥20 years, and was documented after having being seen by the interviewer, or if not, selected from the brand list by the respondent. Universal Product Code was used for identifying cigarettes with a single brand name and possible multiple rod sizes. Cigarette rod length was measured in the following four categories: “Regular (68–72 mm)”; “King (79–88 mm)”; “Long (94–101 mm)”; or “Ultra long (110–121 mm)”. Because of the small sample sizes for ultra-long cigarettes during each survey year, long and ultra-long rod lengths were collapsed together as a category for all analyses.
2.2.3 Demographic characteristics
Because the tobacco industry has been known to target certain population niches by sex, age, race, and several other socio-demographic characteristics (Cook et al., 2003; Carpenter, et al. 2005a, 2007), we measured trends across several populations sub-groups, by sex (male or female), age (≤24; 25– 44; 45–64; or ≥65 years), race/ethnicity (Hispanics; or non-Hispanic: whites, blacks, or other race), marital status (married or living with partner; widowed, divorced or separated; or never married), educational level (<9 grade; 9–11 grade; high school graduate/General Educational Development Certificate; or > high school), and body mass index (underweight: <18.5; normal weight: 18.5–24.9; overweight: 25–29.9; obese: ≥30). Body mass index was included to assess the relationship between respondents’ weight and smoking of long/ultra-long cigarettes in particular.
2.3 Data Analysis
The primary outcome of interest was cigarette rod length smoked. The denominator for all analyses across all survey years was current cigarette smokers aged ≥20 years. Prevalence estimates by cigarette rod length across survey years were calculated overall as well as by sex, race/ethnicity, age, educational level, marital status, and body mass index. Prevalence estimates with relative standard errors ≥30% were considered statistically unreliable and not presented. Chi-squared tests were used to assess for within-group differences.
Results were assessed for the presence of linear trends (p<0.05). A linear trend indicates an overall change from the beginning to the end of the study period but does not necessarily indicate a constant rate of change. If a linear trend was detected, data were also assessed for the presence of a quadratic trend. Quadratic trends indicate a significant but nonlinear trend in the data over time. When a significant quadratic trend accompanied a significant linear trend, the data demonstrated some nonlinear variation (e.g., leveling off or change in direction) in addition to a linear trend. Linear and quadratic trends during 1999–2012 were assessed by means of binary logistic regression, controlling for sex, race/ethnicity, age, educational level, marital status, and body mass index to adjust for any changes in the population composition during the study period. In addition, the annual percentage change (APC) in proportion of smokers for each cigarette rod length category during 1999–2012 was calculated using Join Point regression.
To further assess the correlates of smoking king size and long/ultra-long cigarettes among current smokers, multi-variable logistic regression models were fitted, assessing for sex, marital status, age, race/ethnicity, school level, and body mass index (p<0.05). All data were weighted to account for the complex survey design. Statistical analyses were performed with Joinpoint Software version 4.0.1 (National Cancer Institute) and Stata version 11 (StataCorp, 2009).
3. RESULTS
3.1 Long/Ultra-long cigarettes
A significant decline in the overall prevalence of long/ultra-long cigarette use among all current smokers was observed between 1999 through 2012 (from 43.1% to 38.7%; p<0.001 for both linear and quadratic trends; Table 1, Figure 1). Despite this overall decline, during more recent years, the proportion of current smokers who reported smoking long/ultra-long cigarettes has begun to increase (from 29.7% in 2007/2008, to 38.7% in 2011/2012, p=0.015; Figure 1).
Table1.
Trends in current smoking of long/ultra-long cigarettes among U.S. adult Smokers a, National Health and Nutrition Examination Survey, 1999/2000 to 2011/2012
| Characteristic | 1999/2000; n=999 % (95% CI) |
2001/2002; n=1171 % (95% CI) |
2003/2004 n=1,131 % (95% CI) |
2005/2006 n=1089 % (95% CI) |
2007/2008 n=1,319 % (95% CI) |
2009/2010 n=1,346 % (95% CI) |
2011/2012 n=1,108 % (95% CI) |
Unadjusted Annual Percentage Change (95% CI) |
Test for Linear trend b p-value |
Test for Quadratic trend b p-value |
|---|---|---|---|---|---|---|---|---|---|---|
| Overall | 43.1 (37.0–49.1) | 40.5 (36.0–45.0) | 39.3 (35.0–43.6) | 37.0 (31.4–42.7) | 29.7 (24.8–34.5) | 32.4 (27.1–37.7) | 38.7 (33.0–44.3) | −1.8 (−4.2 to 0.7) | <0.001 | <0.001 |
| Sex | ||||||||||
| Male | 34.7 (27.9–41.5) | 30.2 (25.9–34.6) | 29.8 (25.5–34.1) | 26.9 (20.7–33.0) | 20.2 (16.5–24.0) | 24.9 (17.9–31.8) | 28.0 (23.0–32.9) | −2.4 (−5.7 to 1.1) | <0.001 | <0.001 |
| Female | 52.9 (46.3–59.4) | 52.1 (46.4–57.8) | 50.5 (44.8–56.3) | 49.6 (42.1–57.1) | 41.4 (33.5–49.4) | 40.7 (34.6–46.8) | 52.7 (43.8–61.5) | −1.4 (−3.6 to 0.8) | 0.005 | 0.005 |
| Marital Status | ||||||||||
| Married/Living with partner | 43.0 (34.0–51.9) | 43.9 (37.7–50.2) | 39.0 (34.0–43.9) | 36.4 (29.9–43.0) | 27.1 (19.2–35.0) | 33.4 (25.0–41.7) | 36.4 (30.6–42.1) | −2.1 (−4.4 to 0.3) | <0.001 | <0.001 |
| Widowed/divorced/separated | 45.8 (37.3–54.3) | 50.9 (41.9–59.9) | 49.4 (41.8–57.0) | 46.3 (38.4–54.2) | 42.5 (37.5–47.5) | 35.2 (27.0–43.3) | 49.9 (40.6–59.1) | −1.0 (−3.9 to 1.9 | 0.023 | 0.022 |
| Never married | 37.9 (28.9–46.9) | 24.5 (20.0–29.0) | 30.2 (22.5–37.9) | 28.9 (20.6–37.3) | 22.2 (15.7–28.8) | 27.7 (22.5–33.0) | 33.8 (23.7–43.8) | −0.6 (−5.0 to 4.0) | 0.125 | - c |
| Age, years | ||||||||||
| 18–24 | 29.2 (16.4–41.9) | 22.6 (16.7–28.6) | 25.3 (16.7–33.9) | 21.8 (13.2–30.4) | 12.4 (3.5–21.3) | 20.2 (12.6–27.7) | 25.9 (13.1–38.8) | −1.7 (−6.2 to 3.0) | 0.259 | - c |
| 25–44 | 39.5 (31.8–47.3) | 36.4 (31.4–41.3) | 31.5 (26.2–36.7) | 28.8 (20.8–36.9) | 22.6 (17.1–28.0) | 25.0 (19.2–30.8) | 31.4 (23.2–39.6) | −0.4 (−2.5 to 1.8) | 0.001 | 0.001 |
| 45–64 | 50.7 (42.4–59.0) | 51.3 (44.4–58.1) | 51.6 (43.7–59.4) | 47.8 (37.8–57.8) | 39.6 (30.6–48.6) | 42.7 (33.1–52.2) | 45.1 (36.8–53.4) | −1.7 (−3.2 to −0.1) | 0.025 | 0.022 |
| ≥65 | 71.0 (61.0–80.9) | 67.0 (57.6–76.3) | 61.2 (48.3–74.2) | 63.6 (51.5–75.7) | 55.8 (47.4–64.3) | 54.1 (41.4–66.8) | 62.5 (46.0–79.0) | −2.1 (−3.5 to −0.6) | 0.465 | - c |
| Race/ethnicity | ||||||||||
| White, non-Hispanic | 44.9 (37.3–52.4) | 42.3 (37.1–47.5) | 39.7 (34.5–44.9) | 38.2 (32.4–44.0) | 28.6 (21.3–35.9) | 31.5 (24.4–38.7) | 37.8 (31.0–44.6) | −2.3 (−4.6 to 0.1) | <0.001 | <0.001 |
| Black, non-Hispanic | 39.3 (28.2–50.3) | 38.8 (31.5–46.0) | 49.3 (43.4–55.2) | 38.7 (29.6–47.9) | 42.5 (38.1–47.0) | 42.0 (33.5–50.4) | 54.5 (47.7–61.2) | 1.7 (−1.7 to 5.3) | 0.220 | - c |
| Hispanic | 35.3 (26.9–43.8) | 32.6 (24.1–41.0) | 26.7 (18.1–35.3) | 23.9 (14.2–33.7) | 18.7 (14.2–23.2) | 24.1 (16.0–32.2) | 28.8 (20.3–37.3) | 1.1 (−1.9 to 4.2) | 0.221 | - c |
| Other race, non-Hispanic | 47.2 (28.2–66.1) | 43.3 (22.9–63.8) | 37.6 (21.5–53.6) | 37.2 (17.4–57.1) | 36.3 (19.7–53.0) | 34.2 (21.0–47.5) | 34.2 (11.3–57.2) | −1.5 (−3.5 to 0.5) | 0.142 | - c |
| School Level | ||||||||||
| <9th grade | 38.3 (20.1–56.6) | 30.5 (18.1–43.0) | 39.4 (30.1–48.6) | 23.6 (10.1–37.2) | 26.9 (13.4–40.3) | 41.6 (23.8–59.4) | 30.9 (16.5–45.4) | −0.9 (−6.2 to 4.8) | 0.660 | - c |
| 9–11 grade | 40.9 (33.7–48.1) | 42.1 (33.7–50.5) | 44.1 (38.1–50.2) | 41.5 (30.8–52.1) | 30.2 (24.4–35.9) | 35.4 (28.1–42.7) | 42.6 (35.2–50.0) | −1.0 (−4.2 to 2.4) | 0.023 | 0.023 |
| High School graduate/GED | 41.3 (33.4–49.2) | 42.7 (33.3–52.0) | 37.8 (33.6–42.1) | 34.5 (25.7–43.4) | 32.5 (24.2–40.8) | 28.9 (21.4–36.4) | 38.4 (26.9–49.8) | −2.4 (−4.7 to 0.0) | 0.044 | 0.042 |
| > High school | 47.3 (38.0–56.6) | 39.4 (32.4–46.4) | 38.4 (31.6–45.2) | 39.0 (33.3–44.6) | 27.5 (22.5–32.6) | 31.8 (26.2–37.5) | 38.0 (30.3–45.7) | −2.6 (−6.1 to 0.9) | <0.001 | <0.001 |
| Body Mass Index | ||||||||||
| Underweight | 50.0 (9.7–90.4) | 30.4 (10.1–50.7) | 38.7 (15.2–62.3) | 49.9 (27.2–72.5) | 36.8 (20.2–53.3) | 44.3 (22.4–66.2) | 33.1 (1.9–64.4) | −0.1 (−5.8 to 6.1) | 0.902 | - c |
| Normal | 40.5 (30.9–50.1) | 39.1 (33.0–45.1) | 39.2 (33.0–45.5) | 30.9 (24.5–37.4) | 29.8 (21.1–38.4) | 30.6 (22.0–39.2) | 37.6 (29.5–45.6) | −1.6 (−4.4 to 1.3) | 0.003 | 0.003 |
| Overweight | 44.7 (38.1–51.3) | 34.7 (27.6–41.7) | 35.8 (29.3–42.3) | 33.4 (25.1–41.6) | 29.7 (23.7–35.8) | 28.0 (20.3–35.7) | 39.8 (32.3–47.4) | −1.8 (−5.2 to 1.8) | 0.010 | 0.010 |
| Obese | 45.5 (36.9–54.2) | 50.2 (42.2–58.1) | 42.3 (35.3–49.4) | 46.7 (37.5–56.0) | 29.5 (23.6–35.4) | 38.5 (30.9–46.0) | 39.2 (30.7–47.7) | −2.6 (−6.1 to 1.1) | 0.020 | 0.020 |
Note: n=unweighted number, CI=Confidence Interval, GED= General Education Development certificate.
The denominator for all analyses was current cigarette smokers aged ≥20 years (i.e. respondents who reported that they had smoked at least 100 cigarettes during their lifetime, and smoked daily or on some days at the time of the survey).
Assessed in a binary logistic regression model that adjusted for all factors listed in table.
Quadratic trend not assessed because of a non-significant linear trend.
Figure 1.
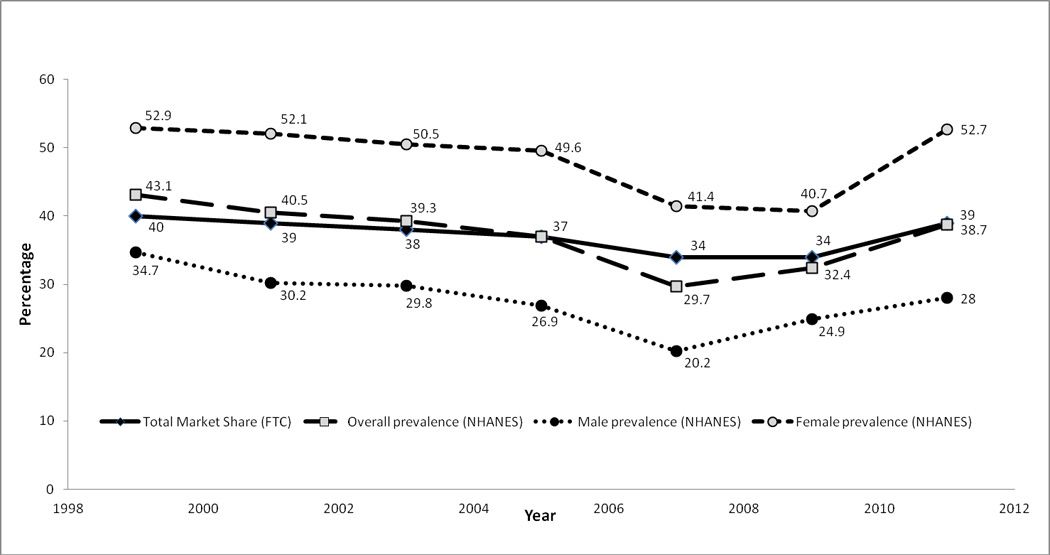
Overall and Sex-specific trends* in current smoking of Long/Ultra-long cigarettes among U.S. adult Smokers a, National Health and Nutrition Examination Survey, 1999/2000 to 2011/2012
Note: FTC=Federal Trade Commission; NHANES=National Health and Nutrition Examination Survey
a The denominator for all analyses was current cigarette smokers aged ≥20 years (i.e. respondents who reported that they had smoked at least 100 cigarettes during their lifetime, and smoked daily or on some days at the time of the survey).
Significant declines during the 1999 through 2012 period were noted among both sexes. However, prevalence of smoking long/ultra-long cigarettes was significantly higher among female smokers (52.7% during 2011/2012) compared to males (28.0% during 2011/2012) at all points during the study period. By marital status, significant declines in smoking of long/ultra-long cigarettes were observed among smokers who were married or living with a partner, whereas no significant change was observed among smokers who had never been married. By age, significant declines in the proportion of respondents who smoked long/ultra-long cigarettes was observed among smokers aged 25–44, or 45–64 years, whereas no significant change was observed among smokers at the extremes of age (i.e., ≤24 years, or ≥65 years). In addition, during each survey year, the proportion of current smokers who reported smoking long/ultra-long cigarettes was lowest among the youngest category and highest among the oldest (in 2011/2012: 25.9% among 18–24 year old smokers, vs. 62.5% among ≥65 year old smokers).
By race/ethnicity, white smokers were the only group to see significant declines in smoking of long/ultra-long cigarettes (44.9% during 1999/2000, to 37.8% during 2011/2012, p<0.001), whereas no significant trends were observed among all other race/ethnic groups. However, within-group analyses during 2011/2012 showed that smoking of long/ultra-long brands was significantly higher among non-Hispanic black smokers (54.5%) compared to either non-Hispanic white (37.8%) or Hispanic smokers (28.8%). By educational level, no significant change in smoking of long/ultra-long cigarettes was observed among smokers that had completed < 9th grade, whereas significant changes were observed during 1999 through 2012 among: those that had completed 9–11 grade (40.9% to 42.6%, p=0.023 for linear trend), high school graduates or those with a General Education Development certificate (41.3% to 38.4%; p=0.044 for linear trend), as well as among smokers with > high school education (47.3% to 38.0%; p<0.001 for linear trend). Finally, by body mass index, no significant change during 1999/2000 to 2011/2012 was observed in the proportion of underweight smokers that reported smoking of long/ultra-long cigarettes. However, significant declines were observed among smokers with normal, overweight, or obese body mass indices (Table 1).
3.2 King Size cigarettes
There was no significant change in the overall prevalence of king size cigarette use among all current smokers during 1999 through 2012 (55.0% to 56.2%; p=0.792 for linear trend). Similarly, no significant changes were observed among population subgroups on stratifying by sex, marital status, age, and body mass index (Table 2). Significant changes was observed during 1999 through 2012 among Hispanics (from 64.5% to 61.8%; p<0.001), and smokers with <9th grade education (from 56.8% to 64.5%; p=0.008)
Table 2.
Trends in current smoking of King-sized cigarettes among U.S. adults Smokers a, National Health and Nutrition Examination Survey, 1999/2000 to 2011/2012
| Characteristic | 1999/2000 n=999 % (95% CI) |
2001/2002 n=1171 % (95% CI) |
2003/2004 n=1,131 % (95% CI) |
2005/2006 n=1089 % (95% CI) |
2007/2008 n=1,319 % (95% CI) |
2009/2010 n=1,346 % (95% CI) |
2011/2012 n=1,108 % (95% CI) |
Unadjusted Annual Percentage Change (95% CI) |
Test for Linear trend b p-value |
Test for Quadratic trend b p-value |
|---|---|---|---|---|---|---|---|---|---|---|
| Overall | 55.0 (49.2–60.9) | 58.5 (53.9–63.0) | 57.7 (54.0–61.4) | 54.3 (49.1–59.6) | 55.2 (49.4–61.1) | 51.4 (46.3–56.4) | 56.2 (50.7–61.8) | −0.6 (−1.6 to 0.5) | 0.792 | - c |
| Sex | ||||||||||
| Male | 62.0 (55.3–68.7) | 68.1 (63.5–72.6) | 66.1 (61.8–70.4) | 62.4 (56.5–68.3) | 60.1 (55.5–64.7) | 55.7 (49.4–62.0) | 66.0 (60.7–71.3) | −0.6 (−2.2 to 1.0) | 0.528 | - c |
| Female | 46.9 (40.2–53.5) | 47.7 (42.1–53.3) | 47.7 (41.7–53.8) | 44.4 (37.4–51.3) | 49.2 (39.5–58.8) | 46.6 (40.0–53.2) | 43.4 (33.9–53.0) | −0.4 (−1.3 to 0.6) | 0.820 | - c |
| Marital Status | ||||||||||
| Married/Living with partner | 55.2 (46.5–64.0) | 55.2 (49.1–61.4) | 59.5 (54.6–64.4) | 55.7 (49.3–62.1) | 55.7 (46.2–65.2) | 47.8 (40.2–55.5) | 56.9 (51.0–62.8) | −0.3 (−1.9 to 1.3) | 0.907 | - c |
| Widowed/divorced/separated | 52.9 (44.2–61.6) | 47.6 (38.1–57.2) | 46.1 (38.1–54.1) | 43.8 (34.9–52.8) | 47.2 (39.4–55.0) | 52.5 (44.3–60.6) | 48.4 (39.6–57.2) | −0.1 (−1.9 to 1.7) | 0.480 | - c |
| Never married | 59.5 (50.7–68.2) | 74.7 (70.2–79.2) | 64.6 (56.7–72.5) | 61.6 (53.7–69.5) | 62.8 (53.9–71.7) | 58.5 (53.2–63.7) | 62.0 (52.0–72.0) | −1.9 (−4.2 to 0.3) | 0.472 | - c |
| Age, years | ||||||||||
| 18–24 | 67.9 (55.6–80.2) | 75.7 (70.1–81.2) | 71.8 (63.9–79.7) | 67.7 (58.8–76.5) | 64.5 (52.6–76.4) | 62.0 (52.4–71.6) | 69.9 (57.7–82.2) | −1.4 (−2.9 to 0.2) | 0.224 | - c |
| 25–44 | 59.7 (52.0–67.4) | 63.6 (58.7–68.6) | 65.3 (60.7–69.9) | 61.1 (53.5–68.8) | 57.9 (49.2–66.6) | 56.6 (49.9–63.4) | 61.2 (52.1–70.3) | −0.8 (−2.1 to 0.6) | 0.590 | - c |
| 45–64 | 45.6 (37.3–54.0) | 46.8 (39.6–54.1) | 46.1 (39.0–53.2) | 44.9 (36.5–53.3) | 51.5 (43.3–59.7) | 43.6 (36.4–50.7) | 51.3 (42.8–59.7) | 0.6 (−1.0 to 2.2) | 0.339 | - c |
| ≥65 | 28.0 (18.2–37.8) | 31.0 (21.8–40.1) | 33.1 (20.8–45.5) | 33.3 (21.4–45.3) | 39.9 (32.1–47.6) | 35.0 (21.4–48.7) | 35.8 (18.7–52.8) | 2.9 (0.5–5.3) | 0.793 | - c |
| Race/ethnicity | ||||||||||
| White, non-Hispanic | 53.1 (45.8–60.4) | 56.8 (51.4–62.1) | 57.4 (53.0–61.9) | 54.8 (49.1–60.4) | 55.8 (47.6–64.0) | 54.0 (47.0–61.0) | 57.8 (51.1–64.6) | 0.1 (−0.8 to 1.0) | 0.205 | - c |
| Black, non-Hispanic | 59.8 (48.6–71.1) | 59.1 (51.4–66.7) | 48.4 (42.5–54.3) | 57.7 (49.2–66.3) | 54.5 (49.3–59.8) | 54.4 (46.0–62.8) | 43.3 (36.6–50.0) | −1.5 (−4.1 to 1.1) | 0.141 | - c |
| Hispanic | 64.5 (56.1–73.0) | 67.0 (58.1–75.8) | 68.9 (60.4–77.5) | 45.4 (38.1–52.6) | 57.9 (49.3–66.5) | 36.3 (27.4–45.2) | 61.8 (54.4–69.3) | −1.5 (−5.6 to 2.7) | <0.001 | <0.001 |
| Other race, non-Hispanic | 46.2 (27.0–65.4) | 56.7 (36.2–77.1) | 58.5 (41.9–75.1) | 54.5 (31.4–77.7) | 42.0 (28.6–55.5) | 47.1 (33.7–60.5) | 55.2 (32.1–78.4) | −1.0 (−4.5 to 2.6) | 0.875 | - c |
| School Level | ||||||||||
| <9th grade | 56.8 (40.1–73.5) | 67.8 (55.9–79.7) | 56.4 (46.8–65.9) | 60.0 (46.2–73.9) | 52.5 (38.5–66.4) | 25.0 (15.3–34.6) | 64.5 (51.8–77.3) | −1.2 (−6.9 to 4.8) | 0.008 | 0.006 |
| 9–11 grade | 58.9 (51.7–66.2) | 57.4 (49.1–65.7) | 53.3 (47.7–58.9) | 51.1 (40.9–61.4) | 57.7 (50.4–64.9) | 49.7 (40.6–58.8) | 53.3 (45.3–61.3) | −0.8 (−2.1 to 0.6) | 0.442 | - c |
| High School graduate/GED | 56.6 (49.2–63.9) | 56.7 (47.5–66.0) | 58.9 (54.8–63.0) | 58.7 (49.9–67.4) | 52.0 (43.2–60.8) | 56.0 (49.5–62.5) | 58.3 (46.4–70.2) | −0.3 (−1.4 to 0.8) | 0.896 | - c |
| > High school | 50.3 (41.7–58.8) | 59.2 (51.9–66.4) | 58.8 (52.6–64.9) | 51.7 (46.1–57.4) | 57.0 (48.8–65.1) | 53.5 (46.1–60.8) | 55.5 (47.9–63.2) | −0.2 (−2.0 to 1.6) | 0.325 | - c |
| Body Mass Index | ||||||||||
| Underweight | 50.0 (9.6–90.3) | 62.9 (44.0–81.8) | 55.6 (27.5–83.7) | 43.4 (21.4–65.4) | 55.3 (32.3–78.2) | 44.5 (22.6–66.5) | 64.3 (31.9–96.6) | −1.0 (−5.2 to 3.3) | 0.865 | - c |
| Normal | 55.7 (47.4–64.0) | 60.5 (54.3–66.7) | 57.2 (51.9–62.5) | 60.7 (53.5–67.9) | 58.0 (49.8–66.2) | 55.1 (46.3–63.9) | 57.6 (49.6–65.6) | −0.2 (−1.2 to 0.9) | 0.410 | - c |
| Overweight | 54.9 (48.5–61.2) | 63.6 (56.6–70.5) | 61.9 (55.5–68.4) | 53.7 (44.7–62.7) | 50.4 (42.1–58.7) | 56.8 (46.1–67.5) | 56.7 (48.9–64.6) | −0.6 (−2.6 to 1.5) | 0.481 | - c |
| Obese | 52.7 (43.5–61.9) | 49.6 (41.3–57.9) | 56.0 (48.8–63.3) | 48.2 (37.5–59.0) | 59.3 (53.1–65.6) | 42.1 (35.6–48.6) | 53.5 (44.7–62.3) | −0.3 (−3.6 to 3.2) | 0.464 | - c |
Note: n=unweighted number, CI=Confidence Interval, GED= General Education Development certificate.
The denominator for all analyses was current cigarette smokers aged ≥20 years (i.e. respondents who reported that they had smoked at least 100 cigarettes during their lifetime, and smoked daily or on some days at the time of the survey).
Assessed in a binary logistic regression model that adjusted for all factors listed in table.
Quadratic trend not assessed because of a non-significant linear trend.
During 2011/2012, prevalence of smoking king size cigarettes was significantly (p<0.05) higher among males smokers (66%) compared to females (43.4%), as well as among Hispanics (61.8) and non-Hispanic whites (57.8%), compared to non-Hispanic blacks (43.3%). In addition, prevalence generally decreased with increasing age of smokers during each survey year (Table 2).
3.3 Regular Cigarettes
The proportion of current smokers who smoked regular cigarettes increased during 1999 through 2012 (1.9% to 5.1%; p<0.001). Results by population subgroups are not presented due to inflated relative standard errors (≥30%) in the majority of groups.
3.4 Correlates of long/ultra-long and King size cigarette smoking during 2011/2012
Results from logistic regression analyses performed to assess the characteristics of those who smoked long/ultra-long and king size cigarettes during 2011/2012 showed that gender, age, and race/ethnicity were significantly associated with rod length of cigarette smoked. Female smokers were three times more likely to smoke long/ultra-long cigarettes than males (aOR=3.09; 95%C.I:2.09–4.58), while significantly less likely to smoke king size cigarettes (aOR=0.38; 95%C.I:0.25–0.58). Moreover, in comparison to those aged 18–24 years, smokers aged 45–64 and ≥65 years of age were more likely to be smokers of long/ultra-long cigarettes (aOR=2.39 and aOR=5.27 respectively). Finally, in comparison to non-Hispanic whites, non-Hispanic blacks were twice more likely to be smokers of long/ultra-long cigarettes (aOR=2.07; 95%C.I: 1.30–3.28; Table 3).
Table 3.
Adjusted a logistic regression analyses assessing correlates of current smoking of Long/Ultra-long and King-sized cigarettes among U.S. adults Smokers b, National Health and Nutrition Examination Survey, 2011/2012 (n=1,108)
| Characteristic | Categories | Long/Ultra-long cigarettes aOR (95% CI) |
King-sized cigarettes aOR (95% CI) |
|---|---|---|---|
| Sex | |||
| Male (Referent) | |||
| Female | 3.09 (2.09–4.58)* | 0.38 (0.25–0.58)* | |
| Marital Status | |||
| Married/Living with partner | |||
| Widowed/divorced/separated | 1.26 (0.81–1.96) | 0.93 (0.60–1.43) | |
| Never married | 1.28 (0.77–2.11) | 0.97 (0.58–1.63) | |
| Age, years | |||
| 18–24 (Referent) | |||
| 25–44 | 1.29 (0.59–2.83) | 0.73 (0.33–1.60) | |
| 45–64 | 2.39 (1.08–5.30)* | 0.47 (0.21–1.05) | |
| ≥65 | 5.27 (1.4–19.78)* | 0.23 (0.06–0.84) | |
| Race/ethnicity | |||
| White, non-Hispanic (Referent) | |||
| Black, non-Hispanic | 2.07 (1.30–3.28)* | 0.52 (0.34–0.79) | |
| Hispanic | 0.94 (0.59–1.48) | 0.82 (0.48–1.41) | |
| Other race, non-Hispanic | 1.09 (0.33–3.59) | 0.71 (0.23–2.14) | |
| School level | |||
| <9th grade (Referent) | |||
| 9–11 grade | 1.87 (0.95–3.67) | 0.56 (0.29–1.09) | |
| High School graduate/GED | 1.39 (0.76–2.54) | 0.74 (0.38–1.42) | |
| > High school | 1.45 (0.74–2.82) | 0.64 (0.34–1.19) | |
| Body Mass Index | |||
| Underweight (Referent) | |||
| Normal | 1.64 (0.35–7.67) | 0.58 (0.13–2.72) | |
| Overweight | 1.82 (0.35–9.56) | 0.58 (0.11–3.07) | |
| Obese | 1.70 (0.39–7.45) | 0.51 (0.12–2.26) |
Note: n=unweighted number, CI=Confidence Interval, GED= General Education Development certificate.
Adjusted for all factors listed in Table.
The denominator for all analyses was current cigarette smokers aged ≥20 years (i.e. respondents who reported that they had smoked at least 100 cigarettes during their lifetime, and smoked daily or on some days at the time of the survey).
Statistically significant at p<0.05
4. DISCUSSION
Our findings indicated that despite the overall declines in current smoking of long/ultra-long cigarettes during 1999 through 2012, the proportion of smokers of long/ultra-long brands increased in recent years. The overall trend line thus showed series of continuing declines between 1999 through 2008 (from 43.1% to 29.7%), whereas an upward trend was observed in more recent years (32.4% during 2009/2010, and 38.7% during 2011/2012). As shown in Figure 1, this trend shows a striking resemblance to trends in total market shares for long/ultra-long cigarettes during 1999 through 2011 based on recent data from the U.S. FTC (2013). The FTC data showed that the combined domestic market shares of long/ultra-long cigarettes declined continuously between 1999 (40%) and 2008 (34%), but subsequently increased to 39% by 2011. The increasing smoking of long/ultra-long cigarettes may possibly be related to increasing influence of social or societal factors and other steady marketing forces, especially with the increasing expenditures on internet advertising of cigarette products in recent years (FTC, 2013). This could also be related to the increasing "portion size" phenomenon that is being observed with food, drink, and other products subject to over-consumption (Nielsen and Popkin, 2003; Piernas and Popkin, 2011), or the perception of “more value for money,” especially in an increasingly austere economic climate.
Current smoking of long/ultra-long cigarettes was defined by specific racial/ethnic, gender and age correlates with current users more likely to be female compared to male, of black race compared to white, and aged over 45 compared to less than 24 years of age, hence describing specific subpopulations. The lower likelihood of smoking long/ultra-long cigarette smoking among younger smokers observed in our study may be a price response, as long/ultra-long cigarettes are usually more expensive than king size brands, and hence may be less favored by youths who are generally price-sensitive (U.S. DHHS, 2012). Our finding of higher likelihood of smoking of long/ultra-long cigarettes among female smokers is consistent with research findings from review of internal tobacco industry documents showing female-tailored marketing of long/ultra-long brands (Carpenter et al., 2005). Long/ultra-long cigarettes were targeted at women right from their inception, by highlighting themes designed to appeal to females such as independence, liberation, slimness, ambition, success, attractiveness, glamour, style, and taste (Cook et al., 2003; Carpenter et al., 2005a). In our study, virtually 100% of ultra-long brands smoked were slim cigarettes (i.e., 17∙1–23∙4 mm circumference; data not shown). It is not surprising that such cigarettes would appeal to females, since slim stick design and marketing have been tailored to strengthen the perceived association with a slender appearance (US DHHS, 2012).
With respect to perception of relative harm from long/ultra-long brands, research has demonstrated that stick design characteristics may be associated with altered perception of harm among smokers (Kotnowski and Hammond, 2013; Mutti et al., 2011; Ford et al., 2013a, 2013b: O'Connor et al., 2013). Recent evidence however indicates that long/ultra-long cigarettes are associated with significantly higher levels of tobacco carcinogen markers (serum cotinine and urinary total 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanonol or NNAL) compared to king or regular size cigarettes (Agaku et al., 2013). Taken together, these findings underscore the need to take to take into account female-targeted product differences when implementing smoking cessation and prevention programs tailored to women (Carpenter et al., 2005a). Such tailored smoking prevention/cessation counseling may include the information that all cigarettes are harmful, regardless of length or circumference.
These findings also underscore the need to regulate design features that may increase consumer product appeal. However, such regulatory measures would need to focus on a holistic examination of cigarette rod and packaging design features rather than on just a single design feature such as cigarette rod length. For example, it is not unusual for feminine-oriented long cigarettes to also be slimmer, usually with white tips, as well as colored markings and bands/patterns (Carpenter et al., 2005a). In addition, restrictions on marketing strategies by the tobacco industry that target youths and females as part of a comprehensive tobacco control program may help reduce disparities in smoking and smoking-attributable morbidity and mortality. While the overall prevalence of current smoking among U.S. adults aged ≥18 years declined significantly during the time period covered by this study (23.5% in 1999 to 18.0% in 2012), the 2012 national adult smoking prevalence is still currently higher than the Healthy People 2020 target of ≤12% for all U.S adults (CDC 2001, 2013; U.S. DHHS 2010). This underscores the need for enhanced and sustained efforts to further reduce smoking among all subpopulation groups.
4.1 Strengths and Limitations
This study is the first study to assess trends in cigarette rod length among smokers. Strengths of the study included the use of a nationally representative sample of the NHANES data and the ability to assess trends across several years. However, some limitations exist. First, due to the small sample size of regular cigarette smokers, sub-group analyses could not be presented due to the inflated relative standard errors of stratified estimates. In addition, rod length could have been misclassified during collection of the data as about a quarter of the respondents’ brands were self-reported and not actually seen by the interviewer.
4.2 Conclusions
This study demonstrated that despite the overall declines in current smoking of long/ultra-long cigarettes during 1999/2012, the proportion of smokers of long/ultra-long brands has increased in recent years, with over a third of current smokers reporting smoking of long/ultra-long cigarettes during 2011/2012. Notably as smokers of long/ultra-long cigarettes were of specific racial, gender and age characteristics. Cigarette rod length should be considered an important aspect of cigarette engineering/design- in regulatory efforts to reduce health disparities and the burden of tobacco related disease.
Acknowledgement
Dr. Israel Agaku initiated the reported research while affiliated with the Center for Global Tobacco Control at Harvard University. He is currently affiliated with the Centers for Disease Control and Prevention’s Office on Smoking and Health. The research in this report was completed and submitted outside of the official duties of his current position and does not reflect the official policies or positions of the Centers for Disease Control and Prevention.
Role of Funding Source
Funding for this study was provided by the National Cancer Institute (grant numbers NCI 3R01 CA125224-03s1rev++, NCI 2R01 CA087477-09A2); the National Cancer Institute had no further role in study design; in the collection, analysis and interpretation of data; in the writing of the report; or in the decision to submit the paper for publication.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Contributors
AIT designed the study, analyzed the data, and wrote the first draft of the manuscript. CIV, OAA-Y, HA, and GNC contributed to data interpretation and were involved with extensive writing and editing of the paper. All authors contributed to and have approved the final manuscript.
Conflict of Interest
The authors have no conflicts of interest relevant to this article to disclose
REFERENCES
- Agaku IT, Vardavas CI, Connolly GN. Cigarette rod length and its impact on serum cotinine and urinary total NNAL levels, NHANES 2007–2010. Nicotine Tob. Res. 2013 doi: 10.1093/ntr/ntt140. epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Australian Government. Tobacco Plain Packaging Act. [Accessed October 12, 2013];2011 Available at http://www.comlaw.gov.au/Details/C2011A00148.
- Behm I, Sokol NA, Kennedy RD, Rees VW, Connolly GN. Population, use, sales, and design: a multidimensional assessment of "light" cigarettes in the United States, 2009. AmJ. Public Health. 2013;103:e93–e99. doi: 10.2105/AJPH.2012.300950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borland R, Savvas S. Effects of stick design features on perceptions of characteristics of cigarettes. Tob. Control. 2013;22:331–337. doi: 10.1136/tobaccocontrol-2011-050199. [DOI] [PubMed] [Google Scholar]
- Campaign for Tobacco-Free Kids. Tobacco Control Laws. [Accessed October, 15, 2013]; Available at http://www.tobaccocontrollaws.org/legislation/country/south-africa/summary.
- Carpenter CM, Wayne GF, Connolly GN. Designing cigarettes for women: new findings from the tobacco industry documents. Addiction. 2005a;100:837–851. doi: 10.1111/j.1360-0443.2005.01072.x. [DOI] [PubMed] [Google Scholar]
- Carpenter CM, Wayne GF, Pauly JL, Koh HK, Connolly GN. New cigarette brands with flavors that appeal to youth: tobacco marketing strategies. Health Aff. 2005b;24:1601–1610. doi: 10.1377/hlthaff.24.6.1601. [DOI] [PubMed] [Google Scholar]
- Carpenter CM, Wayne GF, Connolly GN. The role of sensory perception in the development and targeting of tobacco products. Addiction. 2007;102:136–147. doi: 10.1111/j.1360-0443.2006.01649.x. [DOI] [PubMed] [Google Scholar]
- Caruso RV, O'Connor RJ. Cigarette design features in low-, middle-, and high-income countries. J. Environ. 2012 doi: 10.1155/2012/269576. Public Health epub ahead of print. [DOI] [PMC free article] [PubMed] [Google Scholar]
- CDC. Cigarette smoking among adults--United States, 1999. MMWR. 2001;50:869–873. [PubMed] [Google Scholar]
- CDC. Smoking-attributable mortality, years of potential life lost, and productivity losses—United States, 2000–2004. MMWR. 2008;57:1226–1228. [PubMed] [Google Scholar]
- CDC. National Center for Health Statistics.,2013. [Accessed November, 19, 2013];Current Smoking. 2013 Available at http://www.cdc.gov/nchs/data/nhis/earlyrelease/earlyrelease201306_08.pdf.
- CDC. Current cigarette smoking among adults - United States, 2011. MMWR. 2012;61:889–894. [PubMed] [Google Scholar]
- CDC, National Center for Health Statistics (NCHS), 1999. National Health and Nutrition Examination Survey Data. Hyattsville, MD: U. S. Department of Health and Human Services, Centers for Disease Control and Prevention, 1999; 1999. http://www.cdc.gov/nchs/nhanes/nhanes1999-2000/nhanes99_00.htm. [Google Scholar]
- CDC. Smoking and Tobacco Use- Regulation. [Accessed March 1, 2013];2010 http://www.cdc.gov/tobacco/data_statistics/by_topic/policy/regulation/index.htm.
- Cook BL, Wayne GF, Keithly L, Connolly G. One size does not fit all: how the tobacco industry has altered cigarette design to target consumer groups with specific psychological and psychosocial needs. Addiction. 2003;98:1547–1561. doi: 10.1046/j.1360-0443.2003.00563.x. [DOI] [PubMed] [Google Scholar]
- Euromonitor International. Retrieved from: Euromonitor Passport GMID database. [Accessed October 12, 2013];2013 [Google Scholar]
- European Commission. Revision of the Tobacco Products Directive. [Accessed October 12, 2013]; Available at http://www.ftc.gov/os/2013/05/130521cigarettereport.pdf.
- FTC. Federal Trade Commission Cigarette Report for 2011. [Accessed February 21, 2013];2013 Available at http://www.ftc.gov/os/2012/09/120921cigarettereport.pdf.
- Ford A, Mackintosh AM, Moodie C, Richardson S, Hastings G. Cigarette pack design and adolescent smoking susceptibility: a cross-sectional survey. BMJ Open. 2013a;3 doi: 10.1136/bmjopen-2013-003282. e003282-2013-003282. doi:10.1136/bmjopen-2013-003282; 10.1136/bmjopen-2013-003282. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ford A, Moodie C, Mackintosh AM, Hastings G. Adolescent perceptions of cigarette appearance. Eur. J. Public Health. 2013b doi: 10.1093/eurpub/ckt161. [DOI] [PubMed] [Google Scholar]
- Kennedy RD, Millstein RA, Rees VW, Connolly GN. Tobacco industry strategies to minimize or mask cigarette smoke: Opportunities for tobacco product regulation. Nicotine Tob Res. 2013;15(2):596–602. doi: 10.1093/ntr/nts169. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kotnowski K, Hammond D. The impact of cigarette pack shape, size and opening: evidence from tobacco company documents. Addiction. 2013;108:1658–1668. doi: 10.1111/add.12183. [DOI] [PubMed] [Google Scholar]
- Mutti S, Hammond D, Borland R, Cummings MK, O'Connor RJ, Fong GT. Beyond light and mild: cigarette brand descriptors and perceptions of risk in the international tobacco control (ITC) four country survey. Addiction. 2011;106:1166–1175. doi: 10.1111/j.1360-0443.2011.03402.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nielsen SJ, Popkin BM. Patterns and trends in food portion sizes, 1977–1998. JAMA. 2003;289:450–453. doi: 10.1001/jama.289.4.450. [DOI] [PubMed] [Google Scholar]
- O'Connor RJ, Caruso RV, Borland R, Cummings KM, Bansal-Travers M, Fix BV, King B, Hammond D, Fong GT. Relationship of cigarette-related perceptions to cigarette design features: findings from the 2009 ITC U. S. survey. Nicotine Tob. Res. 2013;15:1943–1947. doi: 10.1093/ntr/ntt075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Piernas C, Popkin BM. Food portion patterns and trends among U. S. children and the relationship to total eating occasion size, 1977–2006. J. Nutr. 2011;141:1159–1164. doi: 10.3945/jn.111.138727. [DOI] [PMC free article] [PubMed] [Google Scholar]
- US Department of Health and Human Services. Healthy people 2020. [Accessed November, 19, 2013];Tobacco use. 2010 Available at http://healthypeople.gov/2020/topicsobjectives2020.
- U. S. Department of Health and Human Services. Atlanta, GA: U.S Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2012. Preventing Tobacco Use among Youth and Young Adults: A Report of the Surgeon General. [Google Scholar]
- World Health Organization. WHO Framework Convention on Tobacco Control. [Accessed September 23, 2012];2012 Available at http://whqlibdoc.who.int/publications/2003/9241591013.pdf.