

Abstract
Hydatid disease is a human parasitic infestation caused by the larval stage of Echinococcus Granulosus. The liver and the lungs are the most common locations. Cardiac involvement is rare and accounts for 0.5–2% of all hydatid disease. We report an unusual presentation of cardiac hydatid cyst revealed by ventricular tachycardia in a patient with a history of cerebral hydatid cyst.
Keywords: Hydatid disease, Cardiac hydatid cyst, Ventricular tachycardia
Introduction
Hydatid disease is a human parasitic infestation caused by the larval stage of Echinococcus Granulosus. The liver and the lungs are the most common locations. Cardiac involvement is rare and accounts for 0.5–2% of all hydatid disease [1]. Solitary cardiac cysts can be asymptomatic over long periods, or can be discovered after serious and even fatal complications. Rupture remains the major life threatening complication and may result in anaphylactic shock. Cardiac tamponade, systemic or pulmonary embolism [2], chest pain [3], valvular regurgitation [4], and – in exceptional cases – arrhythmias can reveal hydatid cysts.[5]
Case report
A 24-year-old man was admitted to our intensive care unit for chest pain and palpitations. He had been operated on when he was nine years old for a brain hydatid cyst of the right temporoparietal area.
On physical examination, heart rate was 200 bpm, blood pressure was 100/60 mmHg, and there were no signs of heart failure. Neurological examination was normal. Electrocardiogram (ECG) showed a ventricular tachycardia (VT) with a heart rate of 200 bpm (Fig. 1). Sinus rhythm was successfully restored after intravenous infusion of amiodarone. No cardiac or pulmonary abnormalities were found on chest X-ray. Trans-thoracic echocardiography revealed the presence of a heterogeneous intramyocardial tumor with intratumoral calcifications, covering two thirds of the apico-lateral left ventricular wall (Fig. 2). Cardiac magnetic resonance imaging (MRI) showed a heterogeneous well-defined intramyocardial tumor displaying hyperintensity on T1 and T2 weighted MRI (Fig. 3a and b). Cardiac computed tomography (CT) was performed and found a large intramyocardial cystic mass measuring 5.8 × 5 cm involving the apico-lateral left ventricular wall with well-defined partially calcified limits and no enhancement after contrast injection (Fig. 4). Enzyme linked immunosorbent assay (ELISA) test for Echinococcus was negative. Laboratory tests were normal. The diagnosis of cardiac hydatid cyst was made and a surgical removal was indicated.
Figure 1.

ECG: ventricular tachycardia with a heart rate of 200 bpm.
Figure 2.

Trans-thoracic echocardiography showing a heterogeneous intramyocardial tumor with intra tumoral calcifications, covering two thirds of the apico-lateral left ventricular wall.
Figure 3.
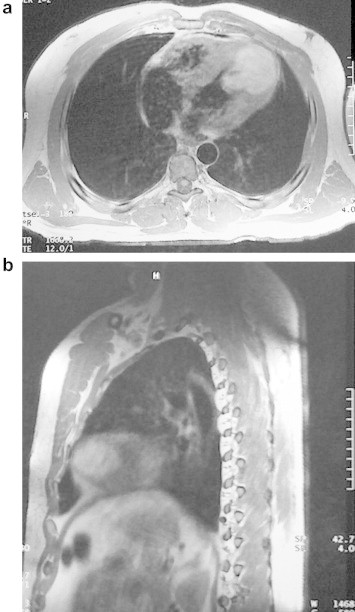
(a and b) Cardiac magnetic resonance imaging showing a heterogeneous well-defined intramyocardial tumor displaying hyper intensity on T1 and T2 weighted MRI.
Figure 4.

Cardiac computed tomography showing a large intra myocardial cystic mass (5.8 × 5 cm) involving the apico-lateral left ventricular wall with well-defined partially calcified edges.
On intervention, an abnormal convexity of the anterolateral and apical wall of the left ventricle was found. The cyst was punctured and rinsed with hypertonic saline solution to destroy daughter cysts, after which total cystectomy was performed except for the pericyst tissue that adhered to the left ventricular wall. Histologic examination confirmed the diagnosis of a hydatid cyst. The postoperative period was uneventful, and the patient was discharged home on the tenth day under amiodarone. There was no recurrence of ventricular tachycardia and amiodarone was stopped three months later. Control trans-thoracic echocardiography showed a residual cavity of 4 cm2. Five years later, the patient is still doing well with no symptoms.
Comment
Since the first report of cardiac hydatidosis by Williams in 1836, cases of cardiac hydatid disease have increasingly been reported [6]. Hydatid disease is endemic in tropical and subtropical regions, particularly in the Mediterranean basin, South America, Africa and Australia [1]. Cardiac involvement is rare [1] and often asymptomatic. Only 10% of patients, especially those with large hydatid cysts have clinical manifestations.
In most cases, a vague chest pain or typical angina had been reported and may be secondary to coronary arteries compression. Myocardial infarction is exceptional [5]. Pericardial type pain is encountered when the pericardium is involved. The cysts are commonly located over the interventricular septum and can be responsible for varying degrees of atrioventricular and intraventricular blocks [8]. The cyst location may induce obstruction of right [9] or left ventricular outflow tracts [10]. When the cyst is located near the valvular apparatus, it may simulate valvular stenosis or cause valvular regurgitation [4,11]. Rupture remains the major life threatening complication and may result in anaphylactic shock, cardiac tamponade and systemic or pulmonary embolism [2]. Cardiac arrhythmias are exceptional and to the best of our knowledge, ventricular tachycardia was reported in less than 20 cases [5]. The mechanism of the VT is uncertain. VT reproductivity by ventricular programmed stimulation in other cases reported in literature [12], suggests a re-entry mechanism. The absence of recurrence of the VT after surgical removal of the cyst implies alteration of automatic substrate for VT by the resection, even if a postoperative residual cavity was noticed. It suggests that the cyst surrounding cardiac fibers may represent the anatomic substratum for the VT.
There are no specific abnormalities for cardiac hydatid cyst on physical examination and ECG. Hypereosinophilia is not specific either and is rarely encountered. The presence of high titers of anti-Ecchinococcus antibodies is helpful but a negative serology, as in our patient, cannot rule out the diagnosis [13]. Two-dimensional echocardiography is the best tool for the detection and localization of cardiac involvement. A trans-thoracic echocardiography should therefore be performed when a non- cardiac hydatid disease is diagnosed. The cardiac hydatid cyst is often single with well-defined edges and sometimes with internal trabeculae corresponding to daughter vesicles [1–7]. CT scan and MRI are helpful when the hydatid cyst presents as solid mass due to degenerative process. They also allow the diagnosis of other thoracic cysts that need to be treated at the same time [14]. Coronary angiography is indicated in case of angina, in elderly patients and when the cyst is adjacent to coronary arteries [6]. As the outcome is unpredictable, surgical removal remains the best treatment, even in asymptomatic patients, because of the risk of rupture [2]. Data on the medical treatment of cardiac hydatid disease are limited. Albendazole was reported to be successful in some sporadic cases [15]. Some authors have reported on the association of cerebral and cardiac hydatid cysts which are generally discovered at the same time [15]. The brain cyst may be due to the rupture of the cardiac cyst with multiple cerebral hydatid embolization [15].
Liver and lungs are still the most common locations. The originality of our case is the long period separating the discovery of these two locations with absence of liver or lung involvement. Two hypotheses are possible: the presence of a very small cardiac cyst which was not detectable by echocardiography at the time of cerebral cyst discovery and re-infestation with Echinococcus Granulosus. The final question remains: are these two cysts due to the same infestation?
Conclusion
Cardiac hydatid cyst is rare but may be life threatening. It is often asymptomatic but can be revealed by arrhythmias. Cardiac involvement can be isolated or associated with other locations. Therefore, an echocardiography should be always performed in patients presenting with non-cardiac hydatid disease.
Footnotes
Peer review under responsibility of King Saud University.

Contributor Information
Zied Ibn Elhadj, Email: zied.bh@laposte.net.
Salem Kachboura, Email: salem.kachboura@rns.tn.
References
- 1.Ameli M., Mobarhan H.A., Nouraii S.S. Surgical treatment of hydatid cyst of the heart: report of six cases. J Thorac Cardiovasc Surg. 1989;98(5 Pt 2):892–901. [PubMed] [Google Scholar]
- 2.Perez-Gomez F., Duran H., Tamames S., Perrote J.L., Blanes A. Cardiac echinococcosis: clinical picture and complications. Br Heart J. 1973;35(12):1326–1331. doi: 10.1136/hrt.35.12.1326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Kosar F., Aksoy Y., Sahin I., Erdil N. Pericardial hydatid cyst mimicking acute coronary syndrome. Tex Heart Inst J. 2005;32(4):570–572. [PMC free article] [PubMed] [Google Scholar]
- 4.Apaydin A.Z., Oguz E., Ayik F., Nalbantgil S., Ceylan N. Hydatid cyst confined to the papillary muscle: a very rare cause of mitral regurgitation. Tex Heart Inst J. 2009;36(6):598–600. [PMC free article] [PubMed] [Google Scholar]
- 5.Sirinelli A., Le Guludec D., Laine J.F., Sebag C., Bourguignon M., Slama M. Ventricular tachycardia revealing a hydatid cyst. Am Heart J. 1987;114(3):656–659. doi: 10.1016/0002-8703(87)90769-1. [DOI] [PubMed] [Google Scholar]
- 6.Yekeler I., Koçak H., Aydin N.E., Başoğlu A., Okur A., Senocak H. A case of cardiac hydatid cyst localized in the lungs bilaterally and on anterior wall of right ventricle. Thorac Cardiovasc Surg. 1993;41(4):261–263. doi: 10.1055/s-2007-1013868. [DOI] [PubMed] [Google Scholar]
- 7.Elangovan S., Harshavardan K., Meenakshi K., Swaminathan T.S., Murthy P. Left ventricular hydatid cyst with myocardial infarction in a patient with severe rheumatic mitral stenosis. Indian Heart J. 2004;56(6):664–667. [PubMed] [Google Scholar]
- 8.De Los Arcos E., Madurga M.P., Perez Leon J., Martinez J.L., Urquia M. Hydatid cyst of the interventricular septum causing left anterior hemiblock. Br Heart J. 1971;33(4):623–625. doi: 10.1136/hrt.33.4.623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Oliver J.M., Sotillo J.F., Domínguez F.J., López de Sá E., Calvo L., Salvador A. Two-dimensional echocardiographic features of echinococcosis of the heart and great blood vessels. Clinical and surgical implications. Circulation. 1988;78(2):327–337. doi: 10.1161/01.cir.78.2.327. [DOI] [PubMed] [Google Scholar]
- 10.Lanzoni A.M., Barrios V., Moya J.L., Epeldegui A., Celemin D., Lafuente C. Dynamic left ventricular outflow obstruction caused by cardiac echinococcosis. Am Heart J. 1992;124(4):1083–1085. doi: 10.1016/0002-8703(92)90999-c. [DOI] [PubMed] [Google Scholar]
- 11.Gomez F.P., Duran H., Tamames S., Perrote J.L., Blames A. Cardiac echinococcosis: clinical picture and complications. Br Heart J. 1973;35:1326–1331. doi: 10.1136/hrt.35.12.1326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Akar R., Eryilmaz S., Yazicioğlu L., Eren N.T., Durdu S., Uysalel A. Surgery of cardiac hydatid disease: an Anatolian experience. Anadolu Kardiyol Derg. 2003;3(3):238–244. [PubMed] [Google Scholar]
- 13.Ben-Hamda K., Maatouk F., Ben-Farhat M., Betbout F., Gamra H., Addad F. Eighteen-year experience with echinococcosis of the heart: clinical and echocardiographic features in 14 patients. Int J Cardiol. 2003;91(2–3):145–151. doi: 10.1016/s0167-5273(03)00032-9. [DOI] [PubMed] [Google Scholar]
- 14.Koubâa M., Lahiani D., Abid L., Mâaloul I., Kahla S.B., Bradii M. Can albendazole be the only treatment for cardiac echinococcosis with multiple organ involvement? Int J Cardiol. 2012;161(3):58–60. doi: 10.1016/j.ijcard.2012.04.082. [DOI] [PubMed] [Google Scholar]
- 15.Bükte Y., Kemaloglu S., Nazaroglu H., Ozkan U., Ceviz A., Simsek M. Cerebral hydatid disease: CT and MR imaging findings. Swiss Med Wkly. 2004;134(31–32):459–467. doi: 10.57187/smw.2004.10711. [DOI] [PubMed] [Google Scholar]