

Abstract
Introduction:
Skin diseases are a common problem among young adults. There is paucity of data about it among medical students. This study aimed to find out the pattern of skin disorders and to describe their association with various socio-demographic factors among medical students.
Materials and Methods:
This cross-sectional study was conducted in June 2011 in a medical college in Mangalore, Karnataka. Two-hundred and seventy eight medical students were chosen from the 4th, 6th and 8th semester through convenient sampling method. Data on hair and skin morbidities suffered over past 1 year and its associated factors were collected using a self-administered questionnaire.
Results:
Most of the participants 171 (61.5%) were of the age group 20-21 years and majority were females 148 (53.2%). The most common hair/skin morbidities suffered in the past one year were acne 185 (66.6%), hair loss 165 (59.3%), and sun tan 147 (52.9%). Fungal infection (P = 0.051) and severe type of acne (P = 0.041) were seen significantly more among males while hair morbidities like hair loss (P = 0.003), split ends of hairs (P < 0.0001) and dandruff (P =0.006) were seen significantly more among female students. Patterned baldness (P = 0.018) and sun tan (P < 0.0001) were significantly more among non-Mangalorean students than native Mangaloreans. Presence of dandruff was significantly associated with hair loss (P = 0.039) and usage of sunscreen was found to protect from developing sun tans (P = 0.049).
Conclusion:
Skin disorders, particularly the cosmetic problems are very common among medical students. Gender and place of origin were found to significantly influence the development of certain morbidities.
Keywords: Hair morbidities, medical students, skin morbidities
INTRODUCTION
Skin diseases are a major health problem affecting a high proportion of the population in India.[1] Skin diseases can place a heavy emotional and psychological burden on patients that may be far worse than the physical impact.[2] Increased consciousness especially among the youth of their body and beauty further aggravates their anxiety.[3]
Many factors determine the pattern and prevalence of cutaneous diseases among the youth such as gender, race, personal hygiene, quality of skin care, environmental milieu and diet.[4] In some instances, patients appear to produce their skin lesions as an outlet for nervous tensions arising from interpersonal conflicts and/or unresolved emotional problems.[5]
Even though dermatology is characterized by an enormous range of disease/reaction patterns, prevalence surveys suggest that the bulk of skin diseases belong to fewer than ten categories.[6] Such observations are useful in developing educational and preventive health programs for the benefit of university students. Their proper management at earlier stages with education of students is important to prevent disfiguring complications and psychological sequelae later in life.[3]
However, very few studies have been carried out in India to find out the problem of skin diseases and that especially among the medical students. The reason for this negligence could be the low mortality rate of the majority of skin diseases in comparison with other diseases. This has also resulted in international health policy makers and local decision makers to make dermatological morbidities a low priority.[7] Another concern is that the benefits of public health interventions in reducing the prevalence, morbidity and mortality of skin diseases may be underestimated.[8] Thus there is a need for more studies with respect to dermatological morbidities in a developing country like India. With this background, this study was carried out to find out the pattern and severity of skin disorders and to describe their association with various socio-demographic factors among medical students of a private medical college in Mangalore city of south India.
MATERIALS AND METHODS
This cross-sectional study was done in June 2011. The ethical approval for conducting this study was obtained from institutional ethics clearance committee. A sample size of 278 was determined using a confidence level of 95%, with 15% degree of precision of the expected proportion and an estimated minimum prevalence of 40%. These students were chosen from the 4th, 6th and 8th semester through convenient sampling method so that the sample will have a balanced representation of 2nd, 3rd and final phase medical students of the institution.
The students were briefed about the objective of the study and written informed consent was taken for participation. A pre-tested self-administered semi-structured questionnaire was used for data collection. The face validity of this questionnaire was done by an expert in dermatology who reviewed the contents of the questionnaire. The questionnaire was subjected to a pilot trial on 10 students before it was distributed in its final form. Reliability of the questionnaire was assessed using Cronbach's Alpha the value of which was 0.82 indicating good internal consistency. Questions on the presence of any skin morbidities suffered by the student participants in the past 1 year were asked.
Additionally questions like frequency of face wash in a day, usage of facial cleansing products, frequency of head and body bath in a week, frequency of usage of hair shampoo in a week, usage of sunscreen lotions, moisturizers or cosmetics, frequency of changing into new clothes, habit of sharing linen with friends and promptness in seeking dermatologist consultation for skin ailments were asked to assess the quality of skin care.
Life style habits were assessed based on amount of water consumed in a day, frequency of eating fatty or oily food stuffs in a week, frequency of consumption of fruits and vegetables in a week, smoking habits and recreation habits like swimming.
Each response for the question meant to assess quality of skin care and life style habits were given scores from 0 to 2. Scores from 0 to 11 for questions deciding quality of skin care meant poor, 12-22 meant good level of skin care. Similarly scores from 0 to 5 for questions deciding life style meant poor and 6-10 meant good level of lifestyle habits.
The data entry and analysis were done using Statistical Package for Social Sciences software package (SPSS Inc., Chicago, IL) version 16. Chi-square test was used to find out the association of socio-demographic variables with the presence of skin morbidities, quality of skin care and life style habits P < 0.05 was taken as statistically significant association.
RESULTS
Mean age of participants was 20.35 ± 1.23 years [Table 1].
Table 1.
Age, gender and place distribution of students
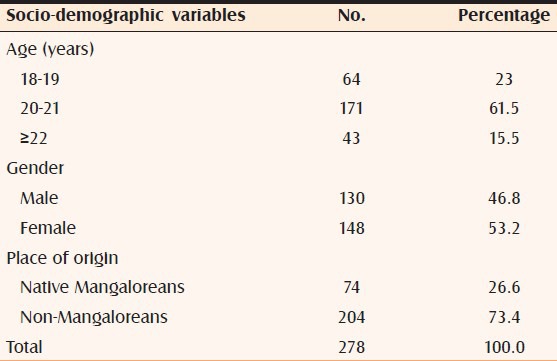
Of the 278 students, 69 (24.8%) had fair skin, 120 (43.2%) had wheatish skin, 74 (26.6%) had brown skin and 15 (5.4%) had dark skin. The one- year-period prevalence of various skin morbidities showed acne to be the commonest skin morbidity in 185 (66.5%) cases followed by sun tan in 147 (52.9%) cases. Among the hair morbidities commonest was hair loss seen in 165 (59.3%) cases followed by dandruff seen in 129 (46.4%) cases [Table 2].
Table 2.
Association between various hair/skin morbidities among students with gender
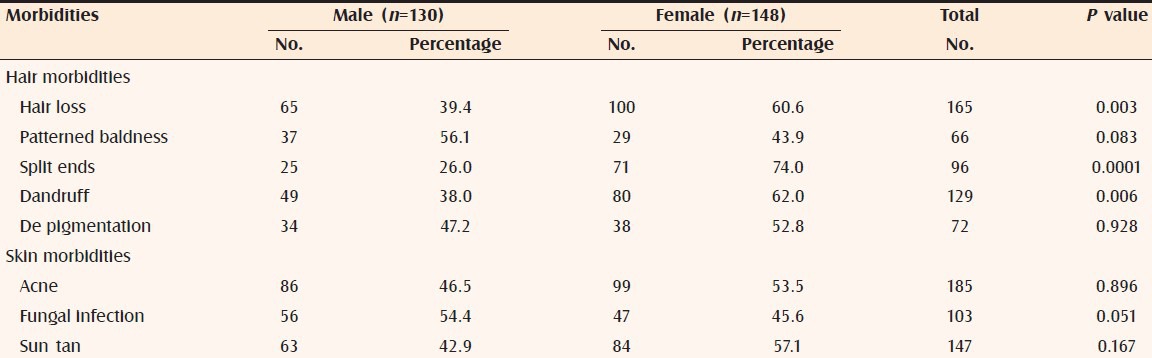
Fungal infection was seen significantly among a greater proportion of males while among females the significant morbidities were hair loss, split end of hairs and dandruff [Table 2].
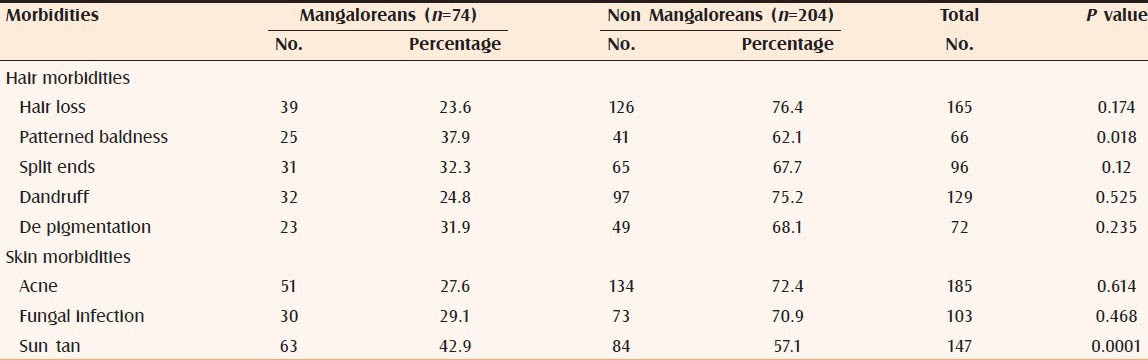
Patterned baldness and sun tan were seen significantly more among greater proportion of non-Mangaloreans than native Mangaloreans [Table 3].
Table 3.
Association between various hair/skin morbidities among students with place of origin (n=278)
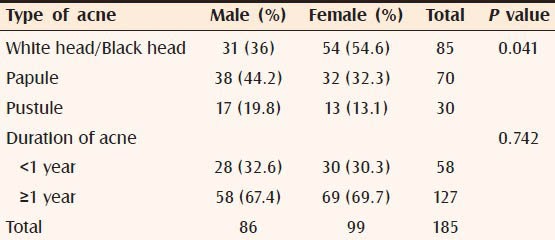
White/black heads were seen significantly more among females while papular and pustular types of acne were seen significantly more among a greater proportion of males. The proportion of cases with pustular type of acne was 30 (10.8%) [Table 4].
Table 4.
Association between gender with type and duration of acne
Of the 278 students with morbidities, 236 (84.9%) had good quality skin care and the rest had poor quality skin care. 108 (83.1%) males and 128 (86.5%) females reported good quality skin care (P = 0.428). Among the participants with good quality skin care, 161 (68.2%) reported presence of morbidities whereas among participants with poor quality skin care, 24 (57.1%) reported presence of morbidities (P = 0.161).
Of the 278 students with morbidities, 236 (84.9%) had good life style habits and the rest had poor life style habits. One hundred and seven (82.3%) males and 129 (87.2%) females reported good life style habits (P = 0.259). Among the participants with good life-style habits, 162 (68.6%) reported presence of morbidities, whereas among participants with poor life-style habits, 23 (54.8%) reported presence of morbidities (P = 0.079). Out of 129 cases with history of dandruff, hair loss was present in 85 (65.9%) cases (P = 0.039).
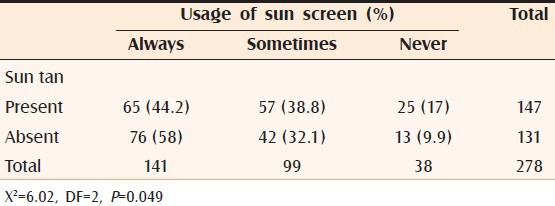
Usage of sunscreen in hot sun was associated with significant reduction in proportion of cases with sun tan among the participants [Table 5].
Table 5.
Association between presence of sun tan with usage of sun screen among students
DISCUSSION
It has been found that one- fourth of us (or more) suffer from at least one skin disease, a situation that constitutes a significant global burden of disease.[9] Economic burden of skin diseases is enormous and added to this easy visibility of dermatological illness has led to deterioration in the quality of life resulting in social handicap.[10,11]
In certain parts of the world, it was observed that the mortality rate and disability-adjusted life years due to skin diseases were at par with certain communicable and non-communicable diseases.[7] In a regression model, skin diseases as well as rheumatism was more strongly associated with feeling depressed than asthma, diabetes and angina pectoris.[12] Considering their significant impact on the individual, the family, the social life of patients and their heavy economical burden, the public health importance of these diseases is underappreciated.[8] This study too has shown that various types of skin morbidities are common among medical students. It has been reported that younger adults suffer more social problems as a result of skin problems than older adults.[12] Thus control of skin morbidities will definitely lead to improvement in the quality of life of young adults. In this study the most common morbidity reported was acne followed by hair loss which was also supported by other studies.[3,13]
Acne has been incriminated with sweating and hot weather, which is very compatible with the hot and humid climatic conditions prevailing in Mangalore.[14] The proportion of severe acne cases in this study was 10.8% which was more than the observation of 5.4% made in the Sindh based study.[3] Studies carried out in other countries have found that acne is a disfiguring disease and it should not be looked at as trivial,[15] as it may seriously affect the patient's life.[16] Screening adolescents for conditions like acne may be of great importance because it affects their image in the society and because of the wide armamentarium of therapy which is available.[17]
Hair loss was the next most common problem, which is very much global in nature. The true magnitude of problem is difficult to establish from this study as the data on the hair density and thickness in our subjects was lacking. There was significant association of dandruff as a risk factor for hair loss in this study which was similar to the findings of other studies.[3,18] However, in the absence of any apparent systemic or local cause for generalized hair loss, it can be assumed that constitutional factors or micro-deficiency of iron, vitamins and proteins may be the cause of hair loss in these subjects.[19,20]
Hair loss culminating in baldness is another sensitive issue among adolescents as they are invariably sensitive regarding their external features and thus may be easily withdrawn psychologically and avoid social activities due to androgenetic alopecia and this tends to affect girls more than boys.[21] In this study almost a quarter of students had baldness with greater proportion observed among males.
Increased tanning of skin was the third most common morbidity. This was understandable as 68% of the participants had fair or wheatish skin. This skin type is prone to tanning on sun exposure. Being less aware of the tanning effect of sun light and not using personal protective measures while outdoors must have promoted tanning and darkening in these subjects.[22]
Fungal infections were reported by more than a third of our participants in the past 1 year. Previous studies have reported that periods of high humidity (50-80%) and elevated temperatures reaching up to 35°C are ideal for fungal infections.[17] This probably could explain the reason behind a number of cases with fungal infections among students in Mangalore.
In a study carried out among university students in Sindh, Pakistan acne was seen in 59.5%, hair loss in 59%, pigmentary disorders in 36.3%, dandruff in 26.1% and fungal infection in 4.9% of the cases. All these observations made were lower than our findings. The study also found pruritis among 2.3% of the cases and eczema among 2.1% of the cases.[3] In another study carried out among 1279 university medical students by Roodsari et al., 91.7% students had skin morbidities. Here acne was seen in 56%, hair loss (evaluated only in females) in 14%, dandruff in 11%, hand eczema in 10%, seborrheic dermatitis in 9% and pityriasis versicolor in 8% cases.[13] But for acne which is easily identifiable, the other skin morbidities were higher in this study than ours probably because disease identification in the former study was done by dermatologists unlike our study where it was self-reported by students. An Icelandic study found that the prevalence of urticaria was significantly higher among the medical students and was seen in 41% of students.[23] These variations in morbidities among students of same age group in different parts of the world could be due to racial, genetic and environmental variations.
In this study acne was found to be slightly more and hair problems was seen significantly more among females, which was similar to the findings of a study done among university students in Lebanon where both acne and hair problems were significantly more among females.[17]
Although there was no significant difference between the proportion of males and females with acne in the present study, the type of acne differed significantly between the two groups. White/black heads were seen significantly more among females while papule and pustule were seen significantly more males. This was similar to the observation made in another study carried out in New Zealand where severe type of acne was seen more among males.[24] Severity of this condition among males could be because of hormonal factors.[25]
Fungal infection seen significantly more among males in this study could be due to their lesser quality of skin care and life style habits in comparison to females. Other cutaneous disorders like pyoderma, folliculitis, scabies and pediculosis were not seen in this study. The reason for absence of these bacterial and parasitic infections could probably be that very few participants in this study had poor quality of skin care or hygiene. No cases of eczema, hyper pigmentary lesions like melasma, hypopigmentary lesions like vitiligo, nail disorders or skin cancers were reported by any of the participants.
Sun tans were seen significantly more among a greater proportion of non-Mangaloreans than native Mangaloreans. This could probably be explained by the non-adjustment to the hot and humid conditions of Mangalore among the outstation students. It was also observed that the users of sunscreen had significantly less cases of sun tans compared to non-users, signifying the importance of spreading awareness about the usage of such protective methods.
Limitations
The present study may not be generalized to other population groups because of different factors associated with different skin morbidities. It may not reveal the true burden of skin disorders among young adults as much as a population-based study. Also as these morbidities were self-reported there may be a possibility of recall bias. In this study, quality of skin care was assessed based on frequency of activities like face wash or body bath or based on the frequency of usage of hair shampoo or sunscreen lotions or moisturizers or cosmetics. Since the quality of these activities or products as well as its proper application on the body was not enquired, it could be a limitation in estimating the true quality of skin care.
Moreover it was difficult to differentiate between the physiological and pathological conditions in hair loss. The most important drawback of this study was that few skin morbidities might have been diagnosed by medical students themselves without actually consulting a dermatologist leading to inaccurate self-reported diagnosis. Hence more of such studies from a broader socioeconomic spectrum are required, which need to be suitably supported with dermatological examination of study subjects.
CONCLUSION
From the findings of one- year- period prevalence of various skin disorders we conclude that skin morbidities are very common among medical students, particularly cosmetic problems like acne, hair loss and skin tan. Severe types of acne and fungal infections were significantly more among males whereas hair morbidities were significantly more among females. Patterned baldness and sun tans were seen significantly more among non-Mangalorean students than native Mangaloreans. This emphasizes the need to popularize the importance of personal protective measures like usage of sun screens among students. Establishment of registries for specific skin diseases, particularly for those with a high disease burden will also help in good case accountability stressing importance to dermatological public health.
ACKNOWLEDGMENTS
The authors of this study would like to thank M.B.B.S students, Ms. Monica N, Mr. Ishan Parashar, Ms. Hemashri, Ms. Supraja Subramanian, Ms. Liya Susan Peter, Ms. Anupriya Dalmiya and Ms. Akanksha Bansal of K.M.C Mangalore for their help in data collection. We also thank Dr. Mohan Kudur, Associate Professor, Department of Dermatology, Venereology and Leprology, Srinivas Institute of Medical sciences and Research Centre, Mangalore for his help and support.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Abolfotouh MA, Bahamdan K. Skin disorders among blind and deaf male students in Southwestern Saudi Arabia. Ann Saudi Med. 2000;20:161–4. doi: 10.5144/0256-4947.2000.161. [DOI] [PubMed] [Google Scholar]
- 2.Ayer J, Burrows N. Acne: More than skin deep. Postgrad Med J. 2006;82:500–6. doi: 10.1136/pgmj.2006.045377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bajaj DR, Devrajani BR, Ghouri RA, Matlani BL. Pattern of skin disorders among adolescent female students at Hyderabad, Sindh. J Pak Assoc Derma. 2009;19:79–85. [Google Scholar]
- 4.Dunwell P, Rose A. Study of the skin disease spectrum occurring in an Afro-Caribbean population. Int J Dermatol. 2003;42:287–9. doi: 10.1046/j.1365-4362.2003.01358.x. [DOI] [PubMed] [Google Scholar]
- 5.Obasi OE, Naguib M. Dermatitis artefacta: A review of 14 cases. Ann Saudi Med. 1999;19:223–7. doi: 10.5144/0256-4947.1999.223. [DOI] [PubMed] [Google Scholar]
- 6.Dogra S, Kumar B. Epidemiology of skin diseases in school children: A study from northern India. Pediatr Dermatol. 2003;20:470–3. doi: 10.1111/j.1525-1470.2003.20602.x. [DOI] [PubMed] [Google Scholar]
- 7.Hay R, Bendeck SE, Chen S, Estrada R, Haddix A, McLeod T, et al. Skin diseases. In: Jamison DT, Breman JG, Measham AR, editors. Disease Control Priorities in Developing Countries. 2nd ed. New York: Oxford University Press; 2006. pp. 707–22. [Google Scholar]
- 8.Khatami A, San Sebastian M. Skin disease: A neglected public health problem. Dermatol Clin. 2009;27:99–101. doi: 10.1016/j.det.2008.11.011. [DOI] [PubMed] [Google Scholar]
- 9.Burns DA, Cox NH. Introduction and historical bibliography. In: Breathnach S, Burns T, Griffiths C, editors. Rook's Textbook of Dermatology. 7th ed. Oxford: Blackwell Science; 2004. p. 1. [Google Scholar]
- 10.Bickers DR, Lim HW, Margolis D, Weinstock MA, Goodman C, Faulkner E, et al. The burden of skin diseases: 2004 a joint project of the American Academy of Dermatology Association and the Society for Investigative Dermatology. J Am Acad Dermatol. 2006;55:490–500. doi: 10.1016/j.jaad.2006.05.048. [DOI] [PubMed] [Google Scholar]
- 11.Johnson ML. Defining the burden of skin disease in the United States–A historical perspective. J Investig Dermatol Symp Proc. 2004;9:108–10. doi: 10.1046/j.1087-0024.2003.09117.x. [DOI] [PubMed] [Google Scholar]
- 12.Dalgard F, Svensson A, Holm JØ, Sundby J. Self-reported skin morbidity among adults: Associations with quality of life and general health in a Norwegian survey. J Investig Dermatol Symp Proc. 2004;9:120–5. doi: 10.1046/j.1087-0024.2003.09111.x. [DOI] [PubMed] [Google Scholar]
- 13.Roodsari RM, Malekzad F, Amini R, Shiri M. Frequency of skin disorders among university students in Shahid Beheshti University of Medical Sciences. Pajouhesh Dar Pezeshkir. 2006;30:183–6. [Google Scholar]
- 14.Yang YC, Cheng YW, Lai CS, Chen W. Prevalence of childhood acne, ephelides, warts, atopic dermatitis, psoriasis, alopecia areata and keloid in Kaohsiung County, Taiwan: A community-based clinical survey. J Eur Acad Dermatol Venereol. 2007;21:643–9. doi: 10.1111/j.1468-3083.2006.02036.x. [DOI] [PubMed] [Google Scholar]
- 15.Mallon E, Newton JN, Klassen A, Stewart-Brown SL, Ryan TJ, Finlay AY. The quality of life in acne: A comparison with general medical conditions using generic questionnaires. Br J Dermatol. 1999;140:672–6. doi: 10.1046/j.1365-2133.1999.02768.x. [DOI] [PubMed] [Google Scholar]
- 16.Barankin B, DeKoven J. Psychosocial effect of common skin diseases. Can Fam Physician. 2002;48:712–6. [PMC free article] [PubMed] [Google Scholar]
- 17.Khattar JA, Hamadeh GN, Rahi AC, Musharrafieh UM. Common dermatologic diseases among students at a tertiary care center in Lebanon. J Med Liban. 2010;58:195–8. [PubMed] [Google Scholar]
- 18.Nematian J, Ravaghi M, Gholamrezanezhad A, Nematian E. Increased hair shedding may be associated with the presence of Pityrosporum ovale. Am J Clin Dermatol. 2006;7:263–6. doi: 10.2165/00128071-200607040-00008. [DOI] [PubMed] [Google Scholar]
- 19.Rushton DH, Norris MJ, Dover R, Busuttil N. Causes of hair loss and the developments in hair rejuvenation. Int J Cosmet Sci. 2002;24:17–23. doi: 10.1046/j.0412-5463.2001.00110.x. [DOI] [PubMed] [Google Scholar]
- 20.Kantor J, Jay K, Brooks D, Cotsarelis G. Decreased serum ferritin is associated with alopecia in women: A case controlled study. J Invest Dermatol. 2001;117:435–41. doi: 10.1046/j.1523-1747.2003.12540.x. [DOI] [PubMed] [Google Scholar]
- 21.Cash TF, Price VH, Savin RC. Psychological effects of androgenetic alopecia on women: Comparisons with balding men and with female control subjects. J Am Acad Dermatol. 1993;29:568–75. doi: 10.1016/0190-9622(93)70223-g. [DOI] [PubMed] [Google Scholar]
- 22.Cestari TF, Benvenuto-Andrade C. Hyperpigmentation and melasma: A physiopathologic review for the clinical dermatologist. Cosmetic Dermatol. 2005;18:703–6. [Google Scholar]
- 23.Bjarnadóttir E, Gíslason D, Gíslason T. Atopy and allergic disorders among Icelandic medical students. Laeknabladid. 2001;87:621–4. [PubMed] [Google Scholar]
- 24.Lello J, Pearl A, Arroll B, Yallop J, Birchall NM. Prevalence of acne vulgaris in Auckland senior high school students. N Z Med J. 1995;108:287–9. [PubMed] [Google Scholar]
- 25.Paik JH, Yoon JB, Sim WY, Kim BS, Kim NI. The prevalence and types of androgenetic alopecia in Korean men and women. Br J Dermatol. 2001;145:95–9. doi: 10.1046/j.1365-2133.2001.04289.x. [DOI] [PubMed] [Google Scholar]