

Introduction
Locating, handling, and reading a primary source typically yields a surprise or two. Like searching for an old snapshot in a musty attic, it may transport you to a different time, but also permit reflection on how things have changed. In the event you only found the negative for that precious photo, you would still have the task of creating a decipherable print in a digital world. Obtaining and translating “Radiography of the Trapeziometacarpal Joint — Degenerative Changes of This Joint” [6], the 1936 communication of Monsieur Paul Robert, was a lot like that heirloom treasure hunt.
Our Stanford Lane Medical Library stacks are currently housed 45 miles east of the main campus in a warehouse. Once located, retrieved, and handled (with special permission), I discovered the well-preserved volume of the Bulletins and Records of the Société de Radiologie Médicale de France, which was bound and acquired around the time Sterling Bunnell practiced at the medical school, which then was located 45 miles north in San Francisco.
Dr. Seth Leopold, Editor-In-Chief of Clinical Orthopaedics and Related Reserach®, addressed the next critical step; he and a French orthopaedic colleague, Dr. Rémy Nizard, provided a superb translation of the original publication. The following translation maintains both the medical cadence of the epoch, and its timelessness.
Robert was a radiologist who practiced at the Etablissement Thermal d’Aix-les-Bains in the foothills of the French Alps, a resort town known for its sulfur springs and catering to the affluent bourgeoisie of the 19th century. Like Saratoga Springs, Vichy, or Spa, Belgium, the water and medical offerings still suggest healing powers — whether magical or clinical.
Although no radiograph appears in the three-page communication, Robert explains the anatomy of the trapezium in a nutshell: the distal articulating surface is concave in the “transverse” (ulnar-radial) plane and convex in the “anteroposterior” (volar-dorsal) plane, and that the matching metacarpal surface is relatively reciprocal. The offset of the trapezium and the thumb in general “are not exactly in the frontal plane,” creating a challenge to obtain a radiograph of the thumb in profile [6]. Robert suggests positioning the dorsal side of the hand flat on the plate, providing a more reproducible image, since the bulk of the palm precludes the joint lying flat. Forced pronation, he posits, is “easier to achieve and more comfortable for the patient … [and] is more likely to position the joint exactly in the plane of the radiographic plate” centering the beam on the joint [6]. Two photographs represent the figures illustrating the forearm in what is described as forced supination and forced pronation on a plate (intriguingly, the palm is facing upward). One can only assume this is intended to illustrate and resolve the bulk-versus-profile problem.
Although radiographs of his technique would have been helpful, Robert nonetheless provides an apt description of how this view assists in diagnosing trapeziometacarpal arthritis progression. He comments on a continuum from subchondral sclerosis, osteophyte formation, and joint degradation: “This joint plays such a large functional role in thumb opposition, the arthritis progresses, and the base of the first metacarpal erodes the trapezium” [6]. Advanced disease affects the trapezium primarily becoming “progressively more hollowed, and in the several cases, it may take on a scaphoid shape,” [6] suggesting a reversal of the convex volar-dorsal plane. He also comments that erosive changes, such as seen with inflammatory arthritis, are rarely seen in arthritis in this joint as compared to other carpal bones, with the exception in late, advanced disease.
Returning to the present day: the “Robert’s view” is one of several radiographic views reported in the literature that image the trapeziometacarpal joint in some form of profile. The Gedda view (variably termed the Bett’s view) [2, 3] is a posterioranterior view first described for examining the oblique Bennett’s fragment, perhaps popular because it has the advantage of being originally published in English, with specific positioning instructions and radiographs. The trapeziometacarpal joint may be difficult to image reliably with this technique, however, given the thenar bulk that Robert indicated, my colleagues and I have found excellent reproducibility with the Lewis technique modifying the pronated Robert’s view, angled 15° proximally (Fig. 1) [1, 5]. This view opens up and corrects the slight offset of the trapeziometacarpal joint from the horizontal (Fig. 2). As Robert pointed out, the trapezium itself is oblique to the remainder of the palm; the volar tangential groove that seats the longitudinal flexor carpi radialis tendon illustrates this position (Fig. 3).
Fig. 1.
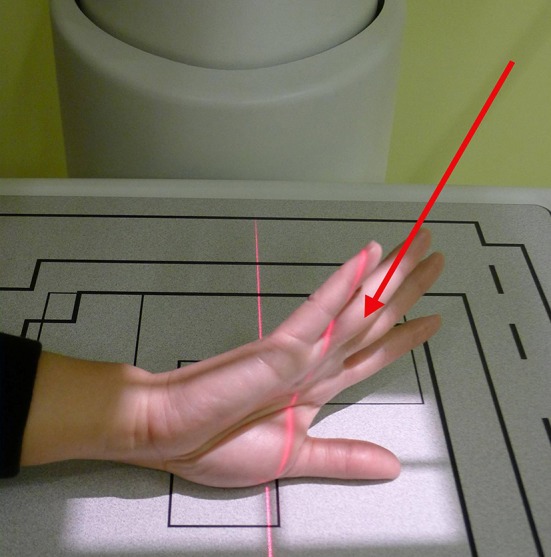
The figure shows the radiograph beam aimed 15° proximal. Published with permission of © Amy L. Ladd 2013. All Rights Reserved.
Fig. 2.

The figure shows a modified Robert’s [4] view of an asymptomatic thumb demonstrating the horizontal profile of both the trapeziometacarpal and scaphotrapezial joints. Published with permission of © Amy L. Ladd 2013. All Rights Reserved.
Fig. 3.
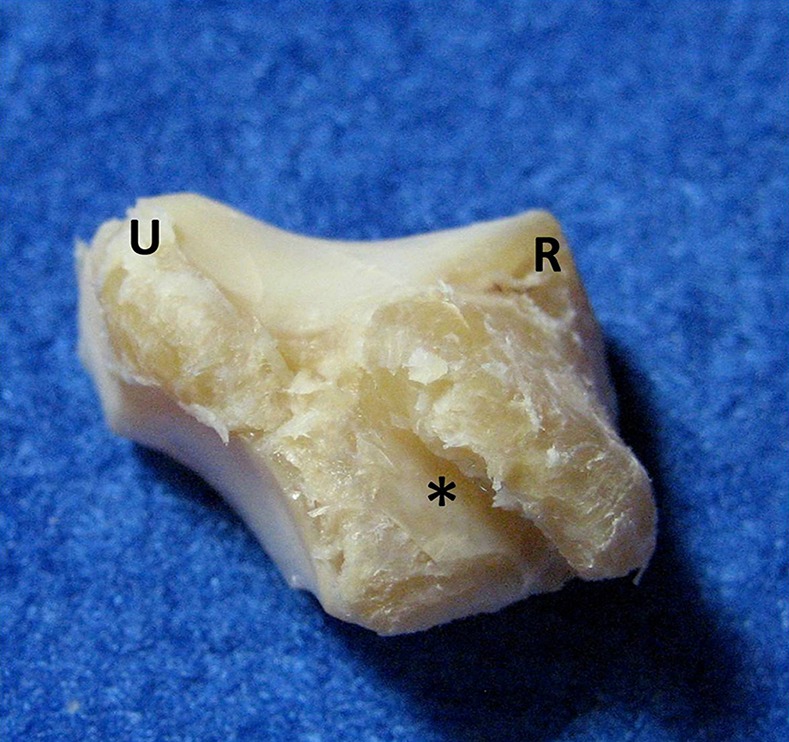
The normal right trapezium is shown from the palmar (volar) side in the same horizontal plane as the radiograph in Fig. 2. The trapezium assumes a convex shape in the ulnar (U) to radial (R) direction, and a convex shape in the volar to dorsal direction. The oblique position of the flexor carpi radialis groove (*), a relatively longitudinal structure in the palm, illustrates the tangential position of the trapezium and base of thumb relative to the rest of the hand. Published with permission of © Amy L. Ladd 2013. All Rights Reserved.
This view also demonstrates advanced disease, as seen in Figs. 4 and 5. The hollowed out distal trapezium with exuberant osteophyte formation, yet relative sparing of the metacarpal reflects Robert’s observations. With some imagination and adopting a 1930s lens, this dysmorphology might suggest a “scaphoid shape.”
Fig. 4.

The modified Robert’s view of a patient with advanced disease is shown. The figure shows the radiograph of a patient with significant radial and ulnar osteophytes of the distal articulating trapezial surface, and loss of trapezial height and joint space degradation. Published with permission of © Amy L. Ladd 2013. All Rights Reserved.
Fig. 5.
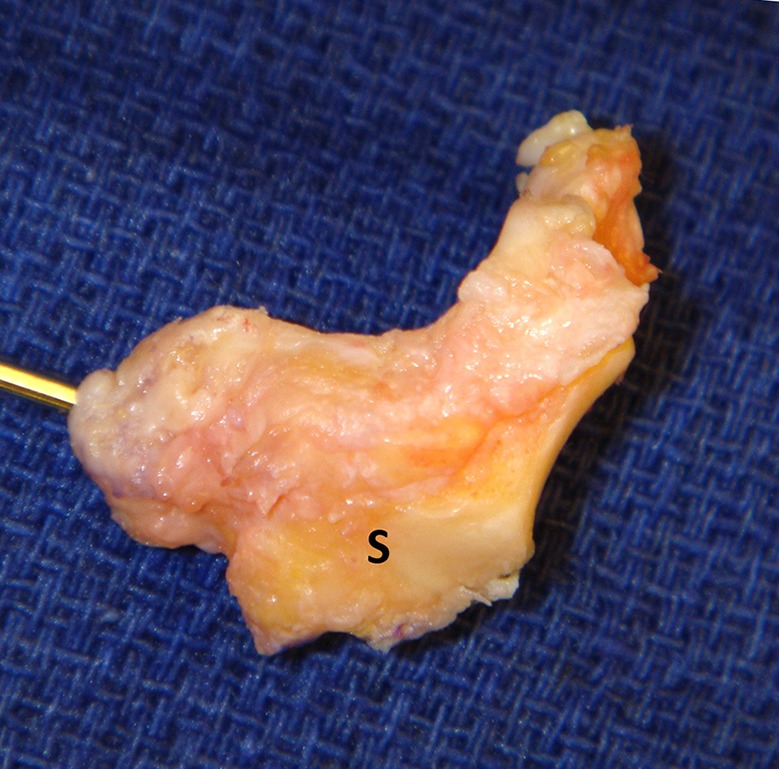
The surgically excised right trapezium of the patient shown in Fig. 4, as viewed from the dorsal side. The extensive osteophyte formation on the distal surface is seen both on the radial side (with positioning wire) and the ulnar side. Although the scaphoid articular surface (S) has a normal appearing facet with no articular wear, an adjacent nonarticular osteophyte is present. Published with permission of © Amy L. Ladd 2013. All Rights Reserved.
Robert’s final comments echo some of our current philosophy regarding thumb trapeziometacarpal arthritis. He indicates that it is “regrettable” that earlier diagnosis of this condition is not often made, “because therapeutic interventions here — like in all arthritic joints — are more likely to succeed earlier in the natural history of the condition” [6]. His article well preceded the landmark 1949 Gervis article [4] recommending simple trapeziectomy — now once again in vogue — so it is hard to know what Robert’s definitive treatment for end-stage arthritis might have been. He did, however, offer nonoperative measures, reporting that he and his colleagues achieved “very good results with a combination of local heat treatments employing thermal baths using the Berthollet [vapor] method, along with cautious radiotherapy of the joint” [6]. Similar measures remain in our spectrum of regimens: applying unguents, performing massage, and administering paraffin baths are but a few examples that linger from the early spa treatments like those of Aix-les-Bains. Radiotherapy, thankfully, is not one of them. But in 1936, radiotherapy was a relatively new technology looking for an indication, now firmly established for treating life-threatening radiosensitive tumors, and life-challenging lesions like heterotopic ossification. The collective work of this Thumb Carpometacarpal CORR® symposium presents novel ideas and approaches to trapeziometacarpal arthritis in much the way Robert’s contribution has provided a better way to image this joint and describe its progression. May we continue to decipher and possess the equipment in our metaphorical black bag to prevent arthritis with methods that are clinically relevant and, well, magically therapeutic.
Footnotes
The author certifies that she, or any members of her immediate family, have no funding or commercial associations (eg, consultancies, stock ownership, equity interest, patent/licensing arrangements, etc) that might pose a conflict of interest in connection with the submitted article.
All ICMJE Conflict of Interest Forms for authors and Clinical Orthopaedics and Related Research ® editors and board members are on file with the publication and can be viewed on request.
The opinions expressed are those of the writers, and do not reflect the opinion or policy of Clinical Orthopaedics and Related Research ® or the Association of Bone and Joint Surgeons®.
References
- 1.Ballinger P, Frank E, Merrill V. Merrill’s Atlas of Radiographic Positions & Radiologic Procedures. 10th ed. St. Louis, MO. Elsevier;2003:108–109.
- 2.Billing L, Gedda KO. Roentgen examination of Bennett’s fracture. Acta Radiol. 1952;38:471–476. doi: 10.3109/00016925209177031. [DOI] [PubMed] [Google Scholar]
- 3.Dela Rosa TL Vance MC, Stern PJ. Radiographic optimization of the Eaton classification. J. Hand Surg. 2004;29B:173–177. doi: 10.1016/j.jhsb.2003.09.003. [DOI] [PubMed] [Google Scholar]
- 4.Gervis WH. Excision of the trapezium for osteoarthritis 329 of the trapezio-metacarpal joint. J Bone Joint Surg Br. 1949;31B:537–539. [PubMed] [Google Scholar]
- 5.Lewis S. New angles on the radiographic examination of the hand—III. Radiogr Today. 1988;54:47–48. [PubMed] [Google Scholar]
- 6.Robert P. Bulletins et memoires de la Société de Radiologie Médicale de France. 1936;24:687–690. [Google Scholar]