

Abstract
Inflammatory conditions that affect the posterior pole are diverse. Specifically, birdshot chorioretinopathy and the white dot syndromes present with multiple white dots in the fundus. These diseases appear to affect similar age groups but there is question as to whether or not a difference exists between the genders. This review summarizes the current studies on birdshot chorioretinopathy and the white dot syndromes as they are related to gender, exploring the differences, if any, which may exist between prevalence, clinical presentation, and treatment response for these diseases. Though the specific etiology of these diseases remains unclear, future treatments may be guided as to how these diseases affect the sexes differently.
1. Introduction
The spectrum of posterior uveitis disorders is broad. There is a specific group, called the white dot syndromes, which presents with multiple white dots in the fundus. The characteristic inflammatory changes of the choroid and retina are typically yellow-white foci beneath or in the deep retina and include birdshot chorioretinopathy (BCR), acute posterior multifocal placoid pigment epitheliopathy (APMPPE), multiple evanescent white dot syndrome (MEWDS), multifocal choroiditis with panuveitis (MFC), punctate inner choroidopathy (PIC), and acute zonal occult outer retinopathy (AZOOR). These disorders represent a range of presentations, including that of demographics, age, genetic, and gender prevalence. The etiology of these diseases is not completely understood nor is the best approach for treatment of these diseases. The purpose of this review was to assess the current scientific evidence as it is related to the possible gender differences that may exist in birdshot chorioretinopathy and the white dot syndromes.
2. Methods and Materials
A systematic review of all the peer-reviewed, English language articles indexed in PubMed about BCR, APMPPE, MEWDS, MFC, PIC, and AZOOR was carried out. For each disease, specific terms were used and reported. Studies with ten or more patients in which patient data included gender and age were reviewed and summarized. Articles were also reviewed for any mention of presentation differences between the sexes and, for those that specified treatment, reviewed to see if differences were noted in the treatment response.
3. Results and Discussion
3.1. BCR
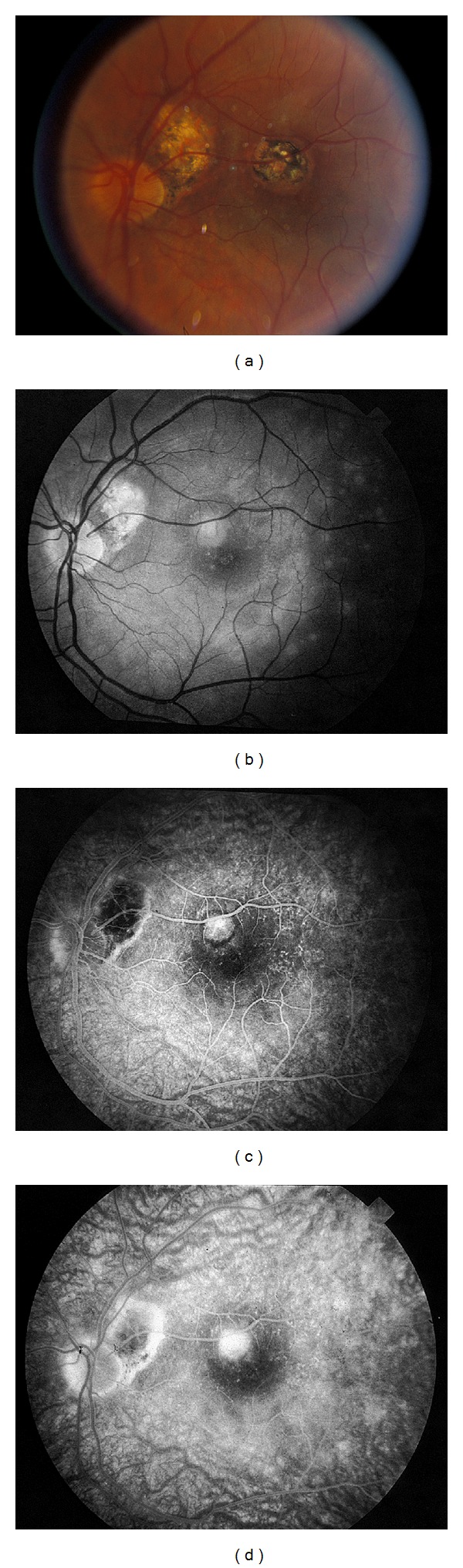
Birdshot chorioretinopathy (BCR) is a rare, chronic, bilateral, posterior inflammatory disease involving the retina and the choroid. The earliest report of this disorder was in 1949 by Franceschaetti and Babel as candle wax spot chorioretinopathy (“la choriorétinite en täche de bougie”) [1]. Ryan and Maumenee coined the term “birdshot retinochoroidopathy” to describe the distinctive lesions seen in the fundus, characterized by multiple, small, white spots that had the appearance of the scatter from a shotgun (Figure 1) [2].
Figure 1.
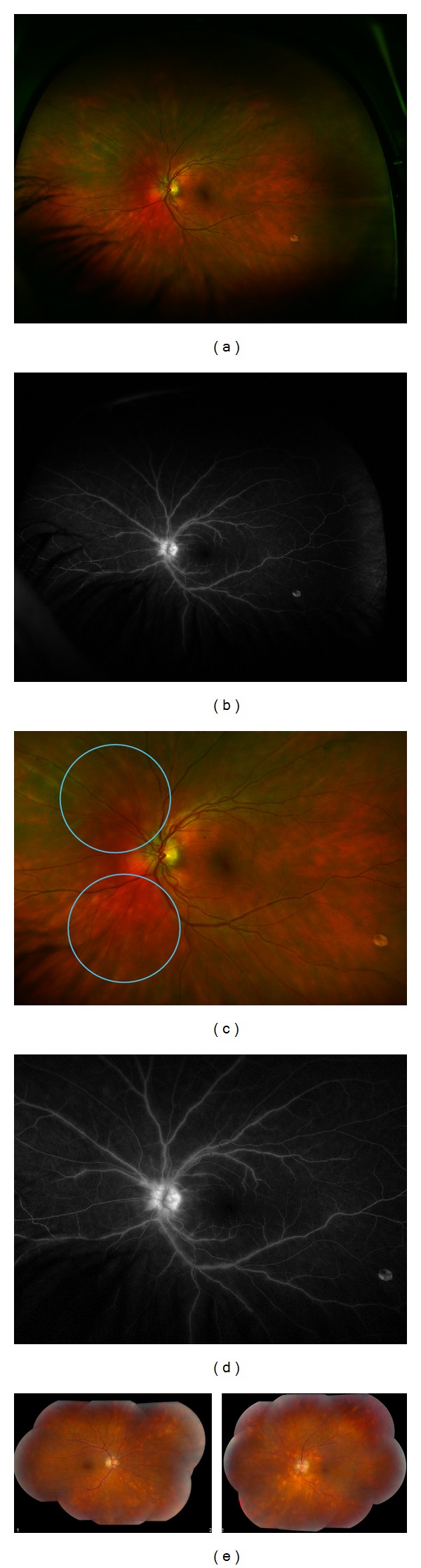
(a) Wide-field fundus photograph of a 34-year-old Caucasian male (diagnosed with BCR one year prior to presentation) with (b) corresponding fluorescein angiogram demonstrating vasculitis. (c) Magnified view of the classic lesions (blue circles) and (d) magnified view of vasculitis and late optic disc leakage. No prior treatment. (e) In contrast, bilateral fundus photography of a 55-year-old Caucasian woman diagnosed with BCR two years prior to presentation with more impressive lesions and vascular sheathing. No prior treatment.
BCR is relatively uncommon, ranging from 1.2 to 7.9% of patients with posterior uveitis [3, 4]. It mostly affects those of Northern European ancestry and those of middle age (average age 48–53), though the range has been reported between 15 and 79 years old [5, 6]. In Shah et al. review, one of the largest reviews on birdshot chorioretinopathy, there was slight female predominance (54.1%), though there have been other studies that have shown a near equal male : female ratio and some with slight male predominance [6–10].
In evaluating the current literature for BCR, data was obtained from 16 articles (Table 1) [6, 8, 9, 11–23]. In PubMed, the term “birdshot chorioretinopathy,” using all or parts of the term, brought up 112 articles. After reviewing and eliminating reports with less than 10 patients, no specificity on patient data for gender and age, and those in which data was repeated, 16 reports remained. Eleven of the 16 reports revealed female predominance, ranging from 54.1 to 100%. When all patients from these articles were considered (n = 1157), 669 patients (58%) were female. The mean age was 53.3 years old, with a range from 46.5 to 61 years old.
Table 1.
Reports for birdshot chorioretinopathy.
| Author | Year published | No. of patients | No. of women (%) | Average age (years) |
|---|---|---|---|---|
| Keane et al. [11] | 2013 | 12 | 5 (42) | 59 |
| Yang and Foster [12] | 2013 | 17 | 8 (47) | 52 |
| Cervantes-Castaneda et al. [23] | 2013 | 49 | 28 (57) | 48.8 |
| Papadia and Herbort [13] | 2013 | 25 | 19 (76) | 49.6 |
| Artornsombudh et al. [22] | 2013 | 22 | 17 (77.3) | 53 |
| Kuiper et al. [14] | 2011 | 16 | 15 (94) | 61 |
| Rothova et al. [21] | 2011 | 76 | 49 (64) | 54 |
| Giuliari et al. [15] | 2010 | 15 | 15 (100) | 52.3 |
| Pagnoux et al. [16] | 2010 | 118 | 73 (62) | 51.5 |
| Trinh et al. [17] | 2009 | 10 | 4 (40) | 46.5 |
| Kappel et al. [18] | 2009 | 63 | 38 (60) | 60.9 |
| Thorne et al. [9] | 2008 | 55 | 25 (45) | 56 |
| Monnet et al. [19] | 2006 | 80 | 51 (64) | 55.6 |
| Shah et al. [6] | 2005 | 522 | 283 (54.1) | 53 |
| Sobrin et al. [20] | 2005 | 23 | 13 (56.5) | 49 |
| Rothova et al. [8] | 2004 | 54 | 26 (48) | 53 |
3.2. APMPPE
APMPPE was first described by Gass in 1968 as a syndrome of multiple, large, placoid lesions at the level of the retinal pigment epithelium that are associated with temporary vision loss [24]. It affects both men and women without preference, usually of good health between the ages of 20 and 50 years old [25]. Vision loss is usually bilateral but may be asymmetric. APMPPE is characterized by bilateral, multifocal yellowish-white placoid lesions usually less than 1 disc diameter in size found in the posterior pole. Classically, these lesions, on fluorescein angiogram, “block early, stain late (Figure 2).” The lesions fade over 1-2 weeks, usually without significant sequelae. Though the etiology is not well understood, it has been postulated that a possible viral agent may be the inciting factor, as patients report a preceding viral prodrome.
Figure 2.
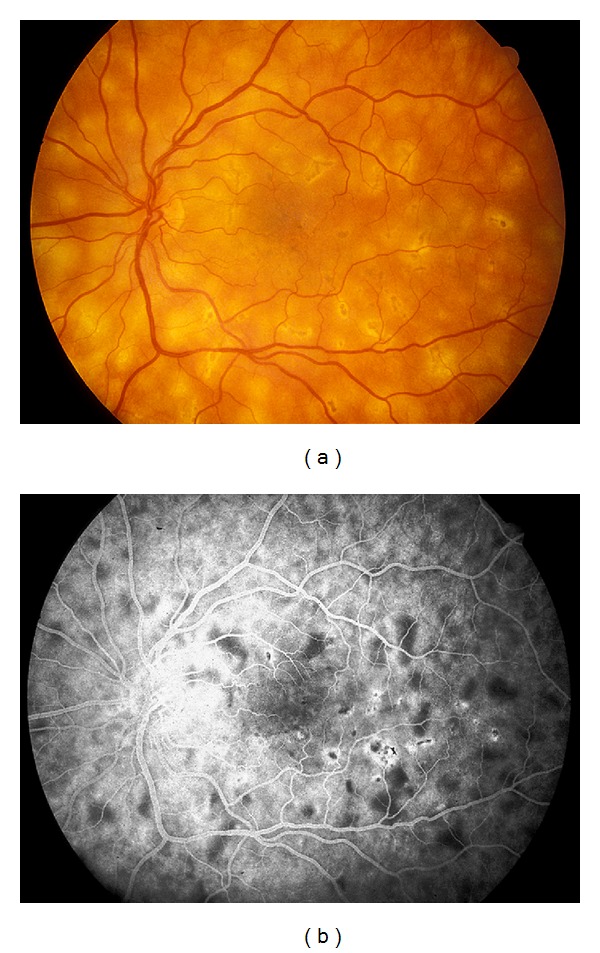
(a) Fundus photograph and corresponding (b) midphase fluorescein angiogram showing blockage of some lesions and the beginning of staining of other lesions as the later phase begins in APMPPE.
In evaluating the current literature for APMPPE, data was obtained from 3 articles (Table 2) [26–28]. In PubMed, the term “acute posterior multifocal placoid pigment epitheliopathy,” using all or parts of the term, brought up 205 articles. After reviewing and eliminating reports with less than 10 patients, no specificity on patient data for gender and age, and those in which data was repeated, 3 reports remained. None of the reports revealed female predominance, ranging from 45.5 to 50%. When all patients from these articles were considered (n = 405), 185 patients (46%) were female. The mean of the average age was 27.1 years old, with a range from 26.2 to 28.6 years old.
Table 2.
Reports for acute posterior multifocal placoid pigment epitheliopathy.
3.3. MEWDS
MEWDS, first described by Jampol et al., presents with numerous small, discrete white lesions in the deep retina or level of the RPE and appears in the posterior pole and extends to the midperiphery [29]. Classically, the fluorescein demonstrates wreath-like lesions and granular appearance to the fovea (Figure 3). Though usually unilateral in young, myopic women ages 20 to 45 years old, there have been bilateral cases described [30]. A preceding viral illness has been reported in approximately 1/3 of cases, and though the cause is unknown, a viral etiology has been suggested. This disease usually resolves spontaneously.
Figure 3.
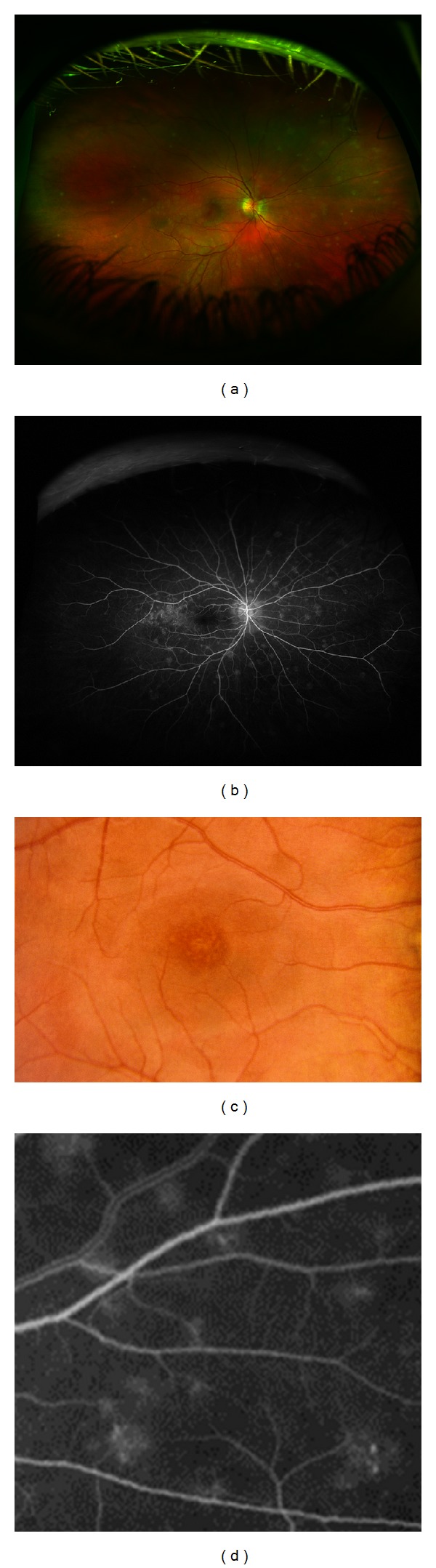
(a) Fundus photograph and corresponding (b) fluorescein angiogram (FA) demonstrating classic wreath-like patterns in MEWDS. (c) Fundus photograph of the macula of different patient demonstration foveal granularity and (d) magnified view of the wreath-like patterns seen on FA in MEWDS.
In evaluating the current literature for MEWDS, data was obtained from 3 articles (Table 3) [13, 31, 32]. In PubMed, the term “multifocal evanescent white dot syndrome,” using all or parts of the term, brought up 151 articles. After reviewing and eliminating reports with less than 10 patients, no specificity on patient data for gender and age, and those in which data was repeated, 3 reports remained. Two of the three reports revealed female predominance, ranging from 50 to 91%. When all patients from these articles were considered (n = 77), 57 patients (74%) were female. The mean of the average age was 28.7 years old, with a range from 28–29.9 years old.
Table 3.
Reports for multiple evanescent white dot syndrome.
3.4. MFC
MFC, unlike classic APMPPE and MEWDS, is more likely to have irreversible visual damage and impairment (Figure 4). This syndrome simulates presumed ocular histoplasmosis (POHS) except that patients present with vitreous cells and inflammation. The punched-out chorioretinal scars with pigmented borders found in the posterior pole and periphery are similar to those in POHS. There is frequent development of choroidal neovascular membranes, which can cause severe vision loss [33]. This disease is usually bilateral with a predilection for patients in their third decade. Though the cause is unknown, it has been hypothesized that an exogenous pathogen may sensitize the individual, with subsequent episodes not requiring the inciting antigen. MFC tends to be a chronic disorder with, generally, a poorer visual prognosis. Some patients require systemic immunosuppression, while other treatments, such as photodynamic therapy and antivascular endothelial growth factor, are used to treat the resultant CNVM [34–36].
Figure 4.
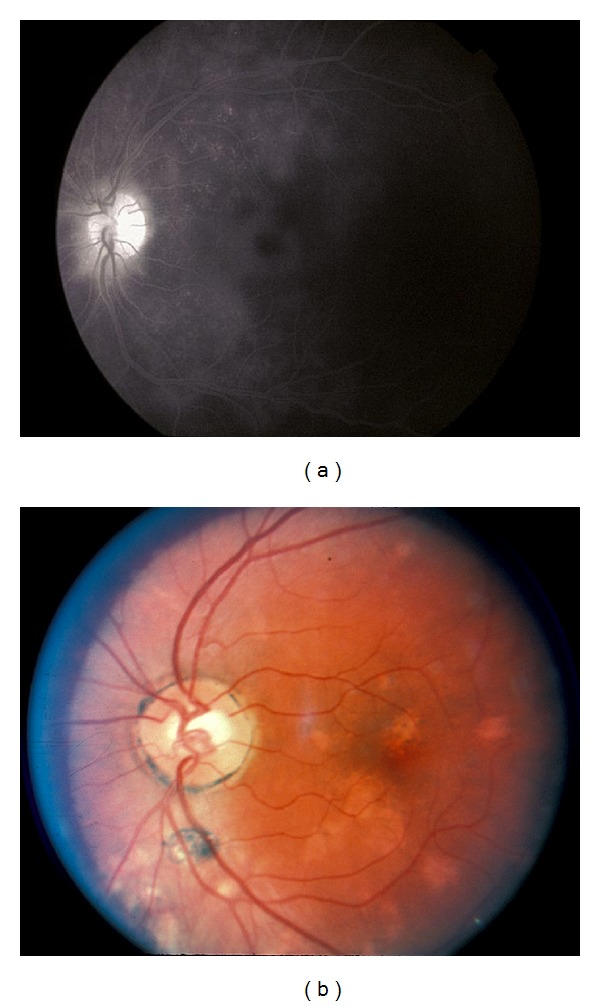
(a) Fluorescein angiogram of a patient with MFC demonstrating concurrent macular edema. (b) Fundus photograph of a patient with MFC requiring systemic immunosuppression.
In evaluating the current literature for this review for MFC, data was obtained from 22 articles (Table 4) [33–35, 37–56]. In PubMed, the term “multifocal choroiditis and panuveitis,” using all or part of the term, brought up 184 articles. After reviewing and eliminating reports with less than 10 patients, no specificity on patient data for gender and age, and those reports in which data was repeated, 22 articles remained. All reports revealed female predominance, ranging from 55 to 100%. When all patients from these articles were considered (n = 538), 406 patients (75%) were female. The mean of the average age was 39.2 years old, with a range from 30.2 to 57 years old.
Table 4.
Reports for multifocal choroiditis and panuveitis.
| Author | Year | No. of patients | No. of women (%) | average Age (years) |
|---|---|---|---|---|
| Fung et al. [37] | 2013 | 41 | 29 (70.7) | 38.4 |
| Spaide et al. [38] | 2013 | 17 | 13 (78.3) | 33 |
| Parodi et al. [39] | 2013 | 14 | 9 (64) | 48 |
| Mansour et al. [40] | 2012 | 12 | 9 (75) | 37.8 |
| Atan et al. [41] | 2011 | 30 | 20 (67) | 57 |
| Parodi et al. [42] | 2010 | 27 | 18 (67) | 39 |
| Kotsolis et al. [43] | 2010 | 17 | 14 (82) | 42.7 |
| Haen and Spaide [44] | 2008 | 18 | 15 (83) | 43.2 |
| Kedhar et al. [45] | 2007 | 66 | 50 (75.8) | 49 |
| Thorne et al. [46] | 2006 | 66 | 50 (76) | 45 |
| MacLaren and Lightman [47] | 2006 | 20 | 11 (55) | 37.1 |
| Vianna et al. [48] | 2006 | 19 | 13 (68) | 46.2 |
| Parodi et al. [49] | 2004 | 13 | 11 (85) | 47 |
| Michel et al. [34] | 2002 | 19 | 15 (79) | 34.8 |
| Spaide et al. [35] | 2002 | 17 | 15 (88) | 34.2 |
| Parnell et al. [50] | 2001 | 25 | 23 (92) | 31.1 |
| Vadalà et al. [51] | 2001 | 13 | 13 (100) | 33 |
| Slakter et al. [52] | 1997 | 14 | 8 (57) | 31 |
| Brown Jr. et al. [33] | 1996 | 41 | 32 (78) | 36 |
| Tiedeman [53] | 1987 | 10 | 6 (60) | 36.6 |
| Morgan and Schatz [54] | 1986 | 11 | 11 (100) | 30.2 |
| Dreyer and Gass [55] | 1984 | 28 | 21 (75) | 33 |
| *Watzke and Claussen [56] | 1981 | 40 | N/A | N/A |
*Not included in data analysis.
3.5. PIC
PIC, a possible variant of MFC, was first described by Watzke et al [57]. This disease was originally described in young, myopic women with punched-out lesions of the posterior pole without ocular inflammation. Like MFC, CNVM may develop and contribute to vision loss (Figure 5).
Figure 5.
(a) Fundus photography and corresponding fluorescein angiogram ((b)–(d)) of a young woman with PIC demonstrating leakage consistent with a choroidal neovascular membrane.
In evaluating the current literature for PIC, data was obtained from 13 articles (Table 5) [33, 57–64]. In PubMed, the term “punctate inner choroidopathy,” using all or parts of the term, brought up 76 articles. After reviewing and eliminating reports with less than 10 patients, no specificity on patient data for gender and age, and those in which data was repeated, 13 articles remained. All 13 articles revealed female predominance, ranging from 64 to 100%. When all patients from these articles were considered (n = 471), 400 patients (85%) were female. The mean of the average age was 33.1 years old, with a range from 26 to 41.5 years old.
Table 5.
Reports for punctate inner choroidopathy.
| Author | Year published | No. of patients | No. of women (%) | average Age (years) |
|---|---|---|---|---|
| Zhang et al. [58] | 2013 | 42 | 27 (64) | 26 |
| Spaide et al. [38] | 2013 | 13 | 12 (92) | 38 |
| Mansour et al. [40] | 2012 | 24 | 19 (79) | 41.5 |
| Zhang et al. [60] | 2012 | 12 | 11 (92) | 32.9 |
| Zhang et al. [59] | 2011 | 75 | 54 (72) | 32 |
| Patel et al. [61] | 2011 | 12 | 11 (92) | 32 |
| Atan et al. [41] | 2011 | 31 | 26 (84) | 40 |
| Essex et al. [62] | 2010 | 136 | 126 (93) | 32 |
| Menezo et al. [63] | 2010 | 10 | 8 (80) | 40.7 |
| Kedhar et al. [45] | 2007 | 13 | 12 (92) | 29 |
| Gerstenblith et al. [64] | 2007 | 77 | 69 (90) | 30 |
| Brown Jr. et al. [33] | 1996 | 16 | 15 (94) | 30 |
| Watzke et al. [57] | 1984 | 10 | 10 (100) | 26.8 |
3.6. AZOOR
AZOOR, thought of predominantly in young women, includes a rapid loss of one or more large zones of outer retinal function and photopsias with minimal fundus changes. Though the cause is unknown, 28% of patients had associated autoimmune diseases, such as Hasimoto's thyroiditis and relapsing transverse myelopathy [65]. No treatment has found to be effective. In Gass' series, 78% of patients with AZOOR had stabilization of the visual field loss and 20% had improvement [65].
In evaluating the current literature for AZOOR, data was obtained from 5 articles (Table 6) [66–70]. In PubMed, the term “acute zonal occult outer retinopathy,” using all or part of the term, brought up 82 articles. After reviewing and eliminating reports with less than 10 patients, no specificity on patient data for gender and age, and those with repeated data, 5 articles remained. All articles revealed female predominance, ranging from 75 to 93%. When all patients from these articles were considered (n = 190), 150 patients (79%) were female. The mean of the average age was 38 years old, with a range from 33 to 49.1 years old.
Table 6.
Reports for acute zonal occult outer retinopathy.
3.7. Summary of Gender Differences in Prevalence
A summary of the gathered data from this paper is provided in Table 7. A review of the presented data appears to demonstrate female predominance, in order from most to least, in the following diseases: PIC > AZOOR > MFC > MEWDS. There appeared to be very slight female predominance in BCR in this review. Very slight male predominance was seen in APMPPE in this review. As for age at onset, from youngest to oldest, this review revealed APMPPE > MEWDS > PIC > AZOOR > MFC > BCR. The BCR patients, on average, were twice as old as the patients of the other WDS for age of onset.
Table 7.
Summary of gathered data.
| Disease | Average age (years) | Gender analysis (% women) |
|---|---|---|
| BCR | 53.5 | F > M (58%) |
| APMPPE | 27.1 | M > F (46%) |
| MEWDS | 28.7 | F > M (74%) |
| MFC | 39.2 | F > M (75%) |
| PIC | 33.1 | F > M (85%) |
| AZOOR | 38 | F > M (79%) |
BCR: birdshot chorioretinopathy, APMPPE: acute posterior multifocal placoid pigment epitheliopathy, MEWDS: multiple evanescent white dot syndrome, MFC: multifocal choroiditis and panuveitis, PIC: punctate inner choroidopathy, AZOOR: acute zonal occult outer retinopathy.
3.8. Gender Differences in Clinical Presentations
Though some of the above white dot syndromes have differences in the ratios of involvement of men to women, no clinical differences have been described between the sexes [1–3, 5, 8–15, 17–20, 24, 26–29, 31–33, 37, 38, 44–47, 50–52, 54–59, 61, 62, 65, 68–71]. In review of the reports, no distinctions were made between the genders in age of onset, initial clinical findings, or severity of disease.
3.9. Gender Differences in Treatment and Prognosis
Though this review revealed female predominance in PIC, AZOOR, MFC, and MEWDS, treatment differences have not been documented between these and the other white dot syndromes [34, 35, 48, 61]. This should be considered in future studies as differences in response to steroids in SLE, another female predominant autoimmune disease (9 : 1), have been noted [72]. Estrogens have been implicated as enhancers of the immune system (with androgens and progesterone being considered immunosuppressors), and such possible explanations have been given for the differences in steroid response in SLE [72]. The other WDS diseases, without preference or with male predominance, also have not had treatment differences noted in the literature [5, 7, 21–23, 71, 73, 74]. BCR, MFC, and PIC in general have poorer VA prognoses than APMPPE and MEWDS, though systemic immunomodulatory therapy may help to decrease the amount of vision loss in BCR, MFC, and PIC. MFC and MEWDS appear to be female dominant and on the different ends of the spectrum for disease prognosis, suggesting that gender, for these diseases, may have little to no effect on visual prognosis. The most abundant amount of data in the literature on treatment of the white dot syndrome diseases concerns BCR. Articles on the use of intravitreal triamcinolone, intravenous immunoglobulin, cyclosporine alone, cyclosporine plus mycophenolate mofetil, methotrexate, infliximab, and daclizumab can be found in the literature on the treatment of BCR with varying success and no mention of response differences between the genders [5, 7, 21–23, 71, 73, 74].
3.10. A Hormonal Difference?
Sex hormones influence the immune system, resulting in females having higher immunoglobulin levels and mounting stronger immune responses following immunizations or infections than males [75]. However, this also increases woman's susceptibility to autoimmune diseases [75]. Abnormal hormone levels may trigger disease [75]. BCR tends to involve older patients, including women who may be menopausal. This is less likely to occur in the other WDS diseases, as they tend to be younger. This may be a possible reason why the ratio is much closer in female : male involvement in BCR than such diseases as PIC, AZOOR, MFC, and MEWDS. Unfortunately, this does not explain the near equal development of APMPPE in males and females, as the patients tend to be younger and this disease usually follows a viral prodrome. Clearly, there is something more. Other factors, such as the involvement of HLA A29 factor in BCR, may influence the occurrence of disease [71].
4. Conclusion
In conclusion, though in this review PIC, AZOOR, MFC, and MEWD were found to have female predominance, there does not appear to be a significant difference in clinical presentation nor in the treatment of these diseases between the genders. BCR and APMPPE appear to affect both men and women equally and again, both in presentation and treatment, there does not appear to be a significant difference between the genders. Though estrogens have been implicated in the manipulations of the immune system, further work is needed to truly elicit how estrogen levels may affect prevalence, presentation, and treatment in these ocular diseases.
Conflict of Interests
The author declares that there is no conflict of interests regarding the publication of this paper.
References
- 1.Franceschaetti A, Babel J. La choriorétinite en täche de bougie, manifestation de la maladie de Besnier-Boeck. Ophthalmologica. 1949;118:701–710. doi: 10.1159/000300769. [DOI] [PubMed] [Google Scholar]
- 2.Ryan SJ, Maumenee AE. Birdshot retinochoroidopathy. American Journal of Ophthalmology. 1980;89(1):31–45. doi: 10.1016/0002-9394(80)90226-3. [DOI] [PubMed] [Google Scholar]
- 3.Henderly DE, Genstler AJ, Smith RE, Rao NA. Changing patterns of uveitis. American Journal of Ophthalmology. 1987;103(2):131–136. doi: 10.1016/s0002-9394(14)74217-5. [DOI] [PubMed] [Google Scholar]
- 4.Rodriguez A, Calonge M, Pedroza-Seres M, et al. Referral patterns of uveitis in a tertiary eye care center. Archives of Ophthalmology. 1996;114(5):593–599. doi: 10.1001/archopht.1996.01100130585016. [DOI] [PubMed] [Google Scholar]
- 5.Gasch AT, Smith JA, Whitcup SM. Birdshot retinochoroidopathy. British Journal of Ophthalmology. 1999;83(2):241–249. doi: 10.1136/bjo.83.2.241. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Shah KH, Levinson RD, Yu F, et al. Birdshot chorioretinopathy. Survey of Ophthalmology. 2005;50(6):519–541. doi: 10.1016/j.survophthal.2005.08.004. [DOI] [PubMed] [Google Scholar]
- 7.Kiss S, Ahmed M, Letko E, Foster CS. Long-term follow-up of patients with birdshot retinochoroidopathy treated with corticosteroid-sparing systemic immunomodulatory therapy. Ophthalmology. 2005;112(6):1066–1071. doi: 10.1016/j.ophtha.2004.12.036. [DOI] [PubMed] [Google Scholar]
- 8.Rothova A, Berendschot TTJM, Probst K, Van Kooij B, Baarsma GS. Birdshot chorioretinopathy: long-term manifestations and visual prognosis. Ophthalmology. 2004;111(5):954–959. doi: 10.1016/j.ophtha.2003.09.031. [DOI] [PubMed] [Google Scholar]
- 9.Thorne JE, Jabs DA, Kedhar SR, Peters GB, Dunn JP. Loss of visual field among patients with birdshot chorioretinopathy. American Journal of Ophthalmology. 2008;145(1):23–28. doi: 10.1016/j.ajo.2007.08.039. [DOI] [PubMed] [Google Scholar]
- 10.Thorne JE, Jabs DA, Peters GB, Hair D, Dunn JP, Kempen JH. Birdshot retinochoroidopathy: ocular complications and visual impairment. American Journal of Ophthalmology. 2005;140(1):45.e1–45.e7. doi: 10.1016/j.ajo.2005.01.035. [DOI] [PubMed] [Google Scholar]
- 11.Keane PA, Allie M, Turner SJ, et al. Characterization of birdshot chorioretinopathy using extramacular enhanced depth optical coherence tomography. JAMA Ophthalmology. 2013;131(3):341–350. doi: 10.1001/jamaophthalmol.2013.1724. [DOI] [PubMed] [Google Scholar]
- 12.Yang P, Foster CS. Interleukin 21, interleukin 23, and transforming growth factor β1 in HLA-A29-associated birdshot retinochoroidopathy. American Journal of Ophthalmology. 2013;156(2):400–406. doi: 10.1016/j.ajo.2013.03.004. [DOI] [PubMed] [Google Scholar]
- 13.Papadia M, Herbort CP. Reappraisal of birdshot retinochoroiditis (BRC): a global approach. Graefe's Archive for Clinical and Experimental Ophthalmology. 2013;251(3):861–869. doi: 10.1007/s00417-012-2201-7. [DOI] [PubMed] [Google Scholar]
- 14.Kuiper JJW, Mutis T, De Jager W, De Groot-Mijnes JDF, Rothova A. Intraocular interleukin-17 and proinflammatory cytokines in HLA-A-29-associated birdshot chorioretinopathy. American Journal of Ophthalmology. 2011;152(2):177–182. doi: 10.1016/j.ajo.2011.01.031. [DOI] [PubMed] [Google Scholar]
- 15.Giuliari GP, Pujari S, Shaikh M, Marvell D, Foster CS. Microperimetry findings in patients with birdshot chorioretinopathy. Canadian Journal of Ophthalmology. 2010;45(4):399–403. doi: 10.3129/i09-278. [DOI] [PubMed] [Google Scholar]
- 16.Pagnoux C, Mahr A, Aouba A, et al. Extraocular manifestations of birdshot chorioretinopathy in 118 French patients. Presse Medicale. 2010;39(5):e97–e102. doi: 10.1016/j.lpm.2009.12.005. [DOI] [PubMed] [Google Scholar]
- 17.Trinh L, Bodaghi B, Fardeau C, et al. Clinical features, treatment methods, and evolution of birdshot chorioretinopathy in 5 different families. American Journal of Ophthalmology. 2009;147(6):1042–1047. doi: 10.1016/j.ajo.2008.12.035. [DOI] [PubMed] [Google Scholar]
- 18.Kappel PJ, Monnet D, Yu F, Brezin AP, Levinson RD, Holland GN. Contrast sensitivity among patients with birdshot chorioretinopathy. American Journal of Ophthalmology. 2009;147(2):351–356. doi: 10.1016/j.ajo.2008.08.021. [DOI] [PubMed] [Google Scholar]
- 19.Monnet D, Brézin AP, Holland GN, et al. Longitudinal cohort study of patients with birdshot chorioretinopathy. I. Baseline clinical characteristics. American Journal of Ophthalmology. 2006;141(1):135–142. doi: 10.1016/j.ajo.2005.08.067. [DOI] [PubMed] [Google Scholar]
- 20.Sobrin L, Lam BL, Liu M, Feuer WJ, Davis JL. Electroretinographic monitoring in birdshot chorioretinopathy. American Journal of Ophthalmology. 2005;140(1):52–64. doi: 10.1016/j.ajo.2005.01.053. [DOI] [PubMed] [Google Scholar]
- 21.Rothova A, Ossewaarde-Van Norel A, Los LI, Berendschot TTJM. Efficacy of low-dose methotrexate treatment in birdshot chorioretinopathy. Retina. 2011;31(6):1150–1155. doi: 10.1097/IAE.0b013e3181ff0d8f. [DOI] [PubMed] [Google Scholar]
- 22.Artornsombudh P, Gevorgyan O, Payal A, Siddique S, Foster CS. Infliximab treatment of patients with birdshot retinochoroidopathy. Ophthalmology. 2013;120:588–592. doi: 10.1016/j.ophtha.2012.05.048. [DOI] [PubMed] [Google Scholar]
- 23.Cervantes-Castaneda RA, Gonzalez-Gonzalez LA, Cordero-Coma M. Combined therapy of cyclosporine A and mycophenolate mofetil for the treatment of birdshot retinochoroidopathy: a 12-month follow-up. British Journal of Ophthalmology. 2013;97:637–643. doi: 10.1136/bjophthalmol-2012-302123. [DOI] [PubMed] [Google Scholar]
- 24.Gass JD. Acute posterior multifocal placoid pigment epitheliopathy. Archives of Ophthalmology. 1968;80(2):177–185. doi: 10.1001/archopht.1968.00980050179005. [DOI] [PubMed] [Google Scholar]
- 25.Quillen DA, Davis JB, Gottlieb JL, et al. The white dot syndromes. American Journal of Ophthalmology. 2004;137(3):538–550. doi: 10.1016/j.ajo.2004.01.053. [DOI] [PubMed] [Google Scholar]
- 26.Thomas BC, Jacobi C, Korporal M, Becker MD, Wildemann B, Mackensen F. Ocular outcome and frequency of neurological manifestations in patients with acute posterior multifocal placoid pigment epitheliopathy (APMPPE) Journal of Ophthalmic Inflammation and Infection. 2012;2(3):125–131. doi: 10.1007/s12348-012-0077-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Fiore T, Iaccheri B, Androudi S, et al. Acute posterior multifocal placoid pigment epitheliopathy: outcome and visual prognosis. Retina. 2009;29(7):994–1001. doi: 10.1097/IAE.0b013e3181a0bd15. [DOI] [PubMed] [Google Scholar]
- 28.Jones NP. Acute posterior multifocal placoid pigment epitheliopathy. British Journal of Ophthalmology. 1995;79(4):384–389. doi: 10.1136/bjo.79.4.384. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Jampol LM, Sieving PA, Pugh D. Multiple evanescent white dot syndrome. I. Clinical findings. Archives of Ophthalmology. 1984;102(5):671–674. doi: 10.1001/archopht.1984.01040030527008. [DOI] [PubMed] [Google Scholar]
- 30.Aaberg TM, Campo RV, Joffe L. Recurrences and bilaterality in the multiple evanescent white-dot syndrome. American Journal of Ophthalmology. 1985;100(1):29–37. doi: 10.1016/s0002-9394(14)74979-7. [DOI] [PubMed] [Google Scholar]
- 31.Asano T, Kondo M, Kondo N, Ueno S, Terasaki H, Miyake Y. High prevalence of myopia in Japanese patients with multiple evanescent white dot syndrome. Japanese Journal of Ophthalmology. 2004;48(5):486–489. doi: 10.1007/s10384-004-0107-6. [DOI] [PubMed] [Google Scholar]
- 32.Reddy CV, Brown J, Jr., Folk JC, et al. Enlarged blind spots in chorioretinal inflammatory disorders. Ophthalmology. 1996;103(4):606–617. doi: 10.1016/s0161-6420(96)30645-3. [DOI] [PubMed] [Google Scholar]
- 33.Brown Jr. J, Folk JC, Reddy CV, Kimura AE. Visual prognosis of multifocal choroiditis, punctate inner choroidopathy, and the diffuse subretinal fibrosis syndrome. Ophthalmology. 1996;103(7):1100–1105. doi: 10.1016/s0161-6420(96)30561-7. [DOI] [PubMed] [Google Scholar]
- 34.Michel SS, Ekong A, Baltatzis S, Foster CS. Multifocal choroiditis and panuveitis: Immunomodulatory therapy. Ophthalmology. 2002;109(2):378–383. doi: 10.1016/s0161-6420(01)00901-0. [DOI] [PubMed] [Google Scholar]
- 35.Spaide RF, Freund KB, Slakter J, Sorenson J, Yannuzzi LA, Fisher Y. Treatment of subfoveal choroidal neovascularization associated with multifocal choroiditis and panuveitis with photodynamic therapy. Retina. 2002;22(5):545–549. doi: 10.1097/00006982-200210000-00003. [DOI] [PubMed] [Google Scholar]
- 36.Cionni DA, Lewis SA, Petersen MR, et al. Analysis of outcomes for intravitreal bevacizumab in the treatment of choroidal neovascularization secondary to ocular histoplasmosis. Ophthalmology. 2012;119(2):327–332. doi: 10.1016/j.ophtha.2011.08.032. [DOI] [PubMed] [Google Scholar]
- 37.Fung AT, Pal S, Yannuzzi NA, et al. MULTIFOCAL CHOROIDITIS WITHOUT PANUVEITIS: clinical characteristics and progression. Retina. 2014;34(1):98–107. doi: 10.1097/IAE.0b013e31829234cb. [DOI] [PubMed] [Google Scholar]
- 38.Spaide RF, Goldberg N, Freund KB. Redefining multifocal choroiditis and panuveitis and punctate inner choroidopathy through multimodal imaging. Retina. 2013;33(7):1315–1324. doi: 10.1097/IAE.0b013e318286cc77. [DOI] [PubMed] [Google Scholar]
- 39.Parodi MB, Iacono P, Mansour A, et al. Intravitreal bevacizumab for juxtafoveal choroidal neovascularization secondary to multifocal choroiditis. Retina. 2013;33(5):953–956. doi: 10.1097/IAE.0b013e318275397c. [DOI] [PubMed] [Google Scholar]
- 40.Mansour AM, Arevalo JF, Fardeau C, et al. Three-year visual and anatomic results of administrating intravitreal bevacizumab in inflammatory ocular neovascularization. Canadian Journal of Ophthalmology. 2012;47(3):269–274. doi: 10.1016/j.jcjo.2012.03.042. [DOI] [PubMed] [Google Scholar]
- 41.Atan D, Fraser-Bell S, Plskova J, et al. Punctate inner choroidopathy and multifocal choroiditis with panuveitis share haplotypic associations with IL10 and TNF loci. Investigative Ophthalmology & Visual Science. 2011;52(6):3573–3581. doi: 10.1167/iovs.10-6743. [DOI] [PubMed] [Google Scholar]
- 42.Parodi MB, Iacono P, Kontadakis DS, Zucchiatti I, Cascavilla ML, Bandello F. Bevacizumab vs photodynamic therapy for choroidal neovascularization in multifocal choroiditis. Archives of Ophthalmology. 2010;128(9):1100–1103. doi: 10.1001/archophthalmol.2010.205. [DOI] [PubMed] [Google Scholar]
- 43.Kotsolis AI, Killian FA, Ladas ID, Yannuzzi LA. Fluorescein angiography and optical coherence tomography concordance for choroidal neovascularisation in multifocal choroidtis. British Journal of Ophthalmology. 2010;94(11):1506–1508. doi: 10.1136/bjo.2009.159913. [DOI] [PubMed] [Google Scholar]
- 44.Haen SP, Spaide RF. Fundus autofluorescence in multifocal choroiditis and panuveitis. American Journal of Ophthalmology. 2008;145(5):847–853. doi: 10.1016/j.ajo.2008.01.008. [DOI] [PubMed] [Google Scholar]
- 45.Kedhar SR, Thorne JE, Wittenberg S, Dunn JP, Jabs DA. Multifocal choroiditis with panuveitis and punctate inner choroidopathy: comparison of clinical characteristics at presentation. Retina. 2007;27(9):1174–1179. doi: 10.1097/IAE.0b013e318068de72. [DOI] [PubMed] [Google Scholar]
- 46.Thorne JE, Wittenberg S, Jabs DA, et al. Multifocal choroiditis with panuveitis. Incidence of ocular complications and of loss of visual acuity. Ophthalmology. 2006;113(12):2310–2316. doi: 10.1016/j.ophtha.2006.05.067. [DOI] [PubMed] [Google Scholar]
- 47.MacLaren RE, Lightman SL. Variable phenotypes in patients diagnosed with idiopathic multifocal choroiditis. Clinical and Experimental Ophthalmology. 2006;34(3):233–238. doi: 10.1111/j.1442-9071.2006.01191.x. [DOI] [PubMed] [Google Scholar]
- 48.Vianna RNG, Özdal PC, Deschênes J, Burnier MN., Jr. Combination of azathioprine and corticosteroids in the treatment of serpiginous choroiditis. Canadian Journal of Ophthalmology. 2006;41(2):183–189. doi: 10.1139/I06-006. [DOI] [PubMed] [Google Scholar]
- 49.Parodi MB, Di Crecchio L, Lanzetta P, Polito A, Bandello F, Ravalico G. Photodynamic therapy with verteporfin for subfoveal choroidal neovascularization associated with multifocal choroiditis. American Journal of Ophthalmology. 2004;138(2):263–269. doi: 10.1016/j.ajo.2004.03.029. [DOI] [PubMed] [Google Scholar]
- 50.Parnell JR, Jampol LM, Yannuzzi LA, Gass JDM, Tittl MK. Differentiation between presumed ocular histoplasmosis syndrome and multifocal choroiditis with panuveitis based on morphology of photographed fundus lesions and fluorescein angiography. Archives of Ophthalmology. 2001;119(2):208–212. [PubMed] [Google Scholar]
- 51.Vadalà M, Lodato G, Cillino S. Multifocal choroiditis: indocyanine green angiographic features. Ophthalmologica. 2001;215(1):16–21. doi: 10.1159/000050820. [DOI] [PubMed] [Google Scholar]
- 52.Slakter JS, Giovannini A, Yannuzzi LA, et al. Indocyanine green angiography of multifocal choroiditis. Ophthalmology. 1997;104(11):1813–1819. doi: 10.1016/s0161-6420(97)30022-0. [DOI] [PubMed] [Google Scholar]
- 53.Tiedeman JS. Epstein-Barr viral antibodies in multifocal choroiditis and panuveitis. American Journal of Ophthalmology. 1987;103(5):659–663. doi: 10.1016/s0002-9394(14)74325-9. [DOI] [PubMed] [Google Scholar]
- 54.Morgan CM, Schatz H. Recurrent multifocal choroiditis. Ophthalmology. 1986;93(9):1138–1147. doi: 10.1016/s0161-6420(86)33611-x. [DOI] [PubMed] [Google Scholar]
- 55.Dreyer RF, Gass JDM. Multifocal choroiditis and panuveitis: a syndrome that mimics ocular histoplasmosis. Archives of Ophthalmology. 1984;102(12):1776–1784. doi: 10.1001/archopht.1984.01040031440019. [DOI] [PubMed] [Google Scholar]
- 56.Watzke RC, Claussen RW. The long-term course of multifocal choroiditis (presumed ocular histoplasmosis) American Journal of Ophthalmology. 1981;91(6):750–760. doi: 10.1016/0002-9394(81)90008-8. [DOI] [PubMed] [Google Scholar]
- 57.Watzke RC, Packer AJ, Folk JC. Punctate inner choroidopathy. American Journal of Ophthalmology. 1984;98(5):572–584. doi: 10.1016/0002-9394(84)90243-5. [DOI] [PubMed] [Google Scholar]
- 58.Zhang X, Zuo C, Li M, Chen H, Huang S, Wen F. Spectral-domain optical coherence tomographic findings at each stage of punctate inner choroidopathy. Ophthalmology. 2013;120(12):2678–2683. doi: 10.1016/j.ophtha.2013.05.012. [DOI] [PubMed] [Google Scholar]
- 59.Zhang X, Wen F, Zuo C, et al. Clinical features of punctate inner choroidopathy in Chinese patients. Retina. 2011;31(8):1680–1691. doi: 10.1097/IAE.0b013e31820a67ad. [DOI] [PubMed] [Google Scholar]
- 60.Zhang H, Liu Z-L, Sun P, Gu F. Intravitreal bevacizumab as primary treatment of choroidal neovascularization secondary to punctate inner choroidopathy: results of a 1-year prospective trial. Retina. 2012;32(6):1106–1113. doi: 10.1097/IAE.0b013e318242b9da. [DOI] [PubMed] [Google Scholar]
- 61.Patel KH, Birnbaum AD, Tessler HH, Goldstein DA. Presentation and outcome of patients with punctate inner choroidopathy at a tertiary referral center. Retina. 2011;31(7):1387–1391. doi: 10.1097/IAE.0b013e3182069a8f. [DOI] [PubMed] [Google Scholar]
- 62.Essex RW, Wong J, Fraser-Bell S, et al. Punctate inner choroidopathy: clinical features and outcomes. Archives of Ophthalmology. 2010;128(8):982–987. doi: 10.1001/archophthalmol.2010.157. [DOI] [PubMed] [Google Scholar]
- 63.Menezo V, Cuthbertson F, Downes SM. Positive response to intravitreal ranibizumab in the treatment of choroidal neovascularization secondary to punctate inner choroidopathy. Retina. 2010;30(9):1400–1404. doi: 10.1097/IAE.0b013e3181d374dc. [DOI] [PubMed] [Google Scholar]
- 64.Gerstenblith AT, Thorne JE, Sobrin L, et al. Punctate inner choroidopathy: a survey analysis of 77 persons. Ophthalmology. 2007;114(6):1201–1204. doi: 10.1016/j.ophtha.2006.10.047. [DOI] [PubMed] [Google Scholar]
- 65.Gass JD, Agarwal A, Scott IU. Acute zonal occult outer retinopathy: a long-term follow-up study. American Journal of Ophthalmology. 2002;134(3):329–339. doi: 10.1016/s0002-9394(02)01640-9. [DOI] [PubMed] [Google Scholar]
- 66.Jiang LB, Shen CY, Chen F, Yan WY, Lai TY, Wang NL. Clinical features of retinal diseases masquerading as retrobulbar optic neuritis. Chinese Medical Journal. 2013;126(17):3301–3306. [PubMed] [Google Scholar]
- 67.Saito M, Saito W, Hashimoto Y, et al. Correlation between decreased choroidal blood flow velocity and the pathogenesis of acute zonal occult outer retinopathy. Clinical & Experimental Ophthalmology. 2013 doi: 10.1111/ceo.12143. [DOI] [PubMed] [Google Scholar]
- 68.Monson DM, Smith JR. Acute zonal occult outer retinopathy. Survey of Ophthalmology. 2011;56(1):23–35. doi: 10.1016/j.survophthal.2010.07.004. [DOI] [PubMed] [Google Scholar]
- 69.Fujiwara T, Imamura Y, Giovinazzo VJ, Spaide RF. Fundus autofluorescence and optical coherence tomographic findings in acute zonal occult outer retinopathy. Retina. 2010;30(8):1206–1216. doi: 10.1097/IAE.0b013e3181e097f0. [DOI] [PubMed] [Google Scholar]
- 70.Jacobson SG, Morales DS, Sun XK, et al. Pattern of retinal dysfunction in acute zonal occult outer retinopathy. Ophthalmology. 1995;102(8):1187–1198. doi: 10.1016/s0161-6420(95)30891-3. [DOI] [PubMed] [Google Scholar]
- 71.Levinson RD, Gonzales CR. Birdshot retinochoroidopathy: immunopathogenesis, evaluation, and treatment. Ophthalmology Clinics of North America. 2002;15(3):343–350. doi: 10.1016/s0896-1549(02)00031-7. [DOI] [PubMed] [Google Scholar]
- 72.Rider V, Abdou NI. Gender differences in autoimmunity: molecular basis for estrogen effects in systemic lupus erythematosus. International Immunopharmacology. 2001;1(6):1009–1024. doi: 10.1016/s1567-5769(01)00046-7. [DOI] [PubMed] [Google Scholar]
- 73.Shah A, Branley M. Use of intravitreal triamcinolone in the management of birdshot retinochoroidopathy associated with cystoid macular oedema: a case study over a three-year period. Clinical and Experimental Ophthalmology. 2005;33(4):442–444. doi: 10.1111/j.1442-9071.2005.01048.x. [DOI] [PubMed] [Google Scholar]
- 74.LeHoang P, Cassoux N, George F, Kullmann N, Kazatchkine MD. Intravenous immunoglobulin (IVIg) for the treatment of birdshot retinochoroidopathy. Ocular Immunology and Inflammation. 2000;8(1):49–57. [PubMed] [Google Scholar]
- 75.Verthelyi D. Sex hormones as immunomodulators in health and disease. International Immunopharmacology. 2001;1(6):983–993. doi: 10.1016/s1567-5769(01)00044-3. [DOI] [PubMed] [Google Scholar]