

Abstract
Background/Aims
To compare the change in the angulation of developing mandibular third molar in both first premolar extraction and non-extraction cases and to determine whether premolar extraction results in a more mesial movement of the mandibular buccal segment and causes favorable rotational changes in the mandibular third molar tilt, which can enhance later eruption of the third molars.
Materials and methods
Pretreatment (T1) and post treatment (T2) panoramic radiographs were taken of 25 subjects (age 14–19 years) who had been treated by the extraction of all the first premolars and 25 subjects who had been treated with non-extraction. The horizontal reference plane was used to measure and compare the changes in the angles of the developing mandibular third molars.
Results
The mean uprighting of the maxillary third molars seen in the extraction group was 4 ± 9° on the left side and −17 ± 13° on the right side following treatment (T2 _ T1). For the non-extraction group the mean difference was −16 ± 12° on the left side and 2 ± 13° on the right side. There was a statistically significant difference between the groups (P _ 0.021 on the right side and P _ 0.041 on the left side). Mandibular 3rd molars in extraction group showed no statistical significant change in the angulation.
Conclusion
Premolar extractions had a positive influence on the developing maxillary third molar angulations both on right and left. Mandibular 3rd molar have shown change in the angulation but not statistically significant. Non-extraction therapy did not have any adverse effect.
Keywords: Premolar extractions, Third molar angulations, OPG
Introduction
The development of third molars and their influence on the dental arches has long been of concern to the dental profession.1 Mandibular third molar impaction is a major problem in modern dentistry.2 The developmental path of third molars in human beings is very irregular and the formation, calcification timing, and the position and course of eruption of these teeth show great variability. Frequently, third molars are impacted or congenitally missing.3
In modern populations, the impaction rate is higher for third molars than for any other tooth.4–7 One explanation could be that the retromolar space frequently is inadequate. If the remodeling resorption at the anterior aspect of the mandibular ramus is limited, the eruption of the mandibular third molars might be blocked.2–11 Similarly the lack of compensatory periosteal apposition at the posterior outline of the maxillary tuberosity could prevent eruption of the maxillary third molar.4 The eruption space for the mandibular third molars is also affected by the direction of tooth eruption during the functional phase of eruption. If the posterior teeth erupt more anteriorly, the retromolar space will increase.8,9 The impact of third molar eruption on mandibular incisor crowding has been the subject of many studies.1–6
The effect of mandibular third molars on the relapse of mandibular incisor crowding following the cessation of retention in orthodontically treated patients has been a subject of much speculation. The orthodontist should be aware of the relationship of the mandibular third molars to the remaining teeth in the dental arch.
The main points to be decided are whether these teeth will erupt or become impacted, whether they will cause crowding of the mandibular anterior teeth, and whether the extraction of other teeth will prevent crowding and influence their eruption.2 Most mandibular third molar studies have concentrated on the influence that the third molars have on the rest of the dentition, rather than on the control that the rest of the dentition has on the third molars.3 The causes for third molar impaction and prediction of third molar eruption have also been studied extensively. In contrast, the effect of orthodontic treatment on the developing third molars has not been subjected too much investigation.
It is often difficult to predict the fate of the third molars, since the second molars of an average 12-year-old orthodontic patient have not yet erupted and the third molars have a limited amount of calcification at that time.
Because this is usually considered the optimum age for treatment of most malocclusions, it is important to know whether and how the third molars are developing before formulating an orthodontic treatment plan.4 Developing third molars continually change their angular positions5 and undergo important pre-eruptive rotational movements.7,11 These rotational movements take place when the third molar bud comes into close proximity to the second molar. Richardson16 found that there was an average change of 11.2° (range, 20–42.5°) of the mandibular third molar between 10 and 15 years of age with respect to the mandibular plane. This indicated a tendency for the tooth to become more upright, with the angle of the mandibular third molar to the mandibular plane tending to decrease. These rotational movements are extremely important since, if they fail to occur, impactions are inevitable.6 Therefore it would be useful to know the effect of appliance therapy on the final and crucial rotational movements of the developing third molars.
There is a strong possibility that appliance therapy that holds back the mandibular molars or actively tips them distally may have the effect of encouraging abnormal rotational movements of the third molar crown and thereby increase the possibility of impaction.6 On the other hand, extraction of premolars might cause favorable mesial movement and uprighting rotational changes in the developing third molars, thereby increasing the possibility of eruption.
Extraction of premolars to allow mesial drifting of the buccal segment has been the subject of many investigations.4,9–26 The relationship between the extraction of maxillary premolars in class II malocclusion subjects and the availability of space for the maxillary third molars has not been specifically investigated.
The intent of the present study was to determine whether extraction of the first premolars results in more mesial movement of the maxillary and mandibular buccal segment and causes favorable rotational changes in the maxillary and mandibular third molar tilt. This study evaluated the changes in the maxillary and mandibular third molar angulations relative to a reference plane and to the second molar long axis. These changes were compared in patients treated with the extraction of first premolars and in patients treated with non-extraction.
Materials and methods
A sample of 60 orthodontic patients who had undergone fixed orthodontic treatment at Department of Orthodontics and Dentofacial Orthopedics, KLE VK institute of Dental Sciences, Belgaum, Karnataka, India, were selected for the study.
Pretreatment (T1) and post treatment (T2) panoramic radiographs (pantographs) were taken of 30 subjects (16 male and 14 female) between age group of 14–19 years who had been treated with the extraction of all first premolars (group 1) and 30 subjects (15 male and 15 female) who had been treated with non-extraction therapy (group 2).
Inclusion criteria
-
•
Bilaterally unerupted mandibular third molars could be seen on a panoramic radiograph in mesioangular positions. Not more than two thirds of the root development of the third molars had taken place.
-
•
Skeletal and dental class I malocclusion was present, with high anchorage requirement (transpalatal arch and lingual arch).
-
•
Treatment of the extraction cases included full closure of the extraction spaces.
-
•
The total treatment time in both the extraction and non-extraction cases should have been no less than 24 months.
-
•
High-quality pretreatment and post treatment pantographs without any magnification and distortion errors and in which a clear, well defined lower contour of orbit and external auditory meatus.
Exclusion criteria
-
•
Standard edgewise cases requiring anchorage preparation.
-
•
The samples included for the present study had patients with class II malocclusion requiring extraction of the second premolars and mandibular molar protraction were excluded from this study.
Method
Pretreatment and post treatment panoramic radiograph tracings were done on lead acetate paper and reference plane constructed in this study was Frankfort horizontal plane and termed the horizontal reference plane (HP). The outlines of the mandibular second and third molars and their long axes were drawn on the tracing sheet. The long axis of the second molar was traced from the midocclusal point through the midpoint of the root bifurcation and the midpoint between the mesial and distal root tips. The long axes of the third molar buds were drawn by the line bisecting a line connecting the mesial and distal outlines of the cervical areas. The following measurements were made, as shown in (Fig. 1).
-
•
The outer angles formed by the third molar axes to the horizontal reference plane (HP) on both the right and left sides (8 to HP [right and left]).
-
•
The outer angles formed by the second molar axes to the horizontal reference plane (HP) on both the right and left sides (7 to HP [right and left]).
-
•
An increase in the angle of the third molar to the horizontal reference plane (HP), which would indicate an improvement in the position of the third molar.
Fig. 1.
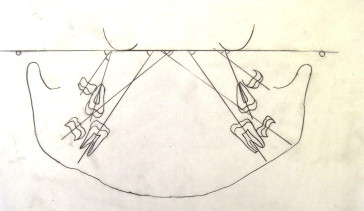
Diagram of angular measurement of 2nd and 3rd maxillary and mandibular molar wrt horizontal plane.
Statistical analysis
The data gathered was stored and analyzed using the SPSS v. 15.0 statistical analysis program. Comparison between pre and post treatment values of different variables in extraction and non-extraction group was done by students paired t test. The results were regarded as statistically significant at P < 0.05.
Results
Table 1 showed comparison of age and sex between extraction and non-extraction group had no significant difference. Tables 2 and 3 showed pretreatment and post treatment change in the angulation of maxillary and mandibular 3rd and 2nd molar right and left side in extraction group. Table 4 showed a comparison between pretreatment and post treatment extraction and non-extraction group. In extraction group, Mean change in the maxillary 3rd molar was 17 ± 13 (degree) on right side and 4 ± 9 (degree) left side. No significant change in the angulation of mandibular 3rd molar was found.
Table 1.
Distribution of study subjects by gender and groups.
| Gender | Extraction | % | Non-extraction | % | Total |
|---|---|---|---|---|---|
| Male | 16 | 53.33 | 15 | 50.00 | 31 |
| Female | 14 | 46.67 | 15 | 50.00 | 29 |
| Total | 30 | 100.00 | 30 | 100.00 | 60 |
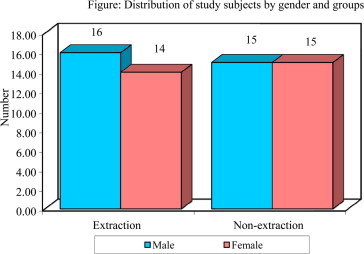
Table 2.
Comparison of pre and post treatment values of different variables in extracted group by paired t-test.
| Variable | Treatment | Mean | Std. Dv. | Mean diff | SD diff | Paired t | P-value |
|---|---|---|---|---|---|---|---|
| HP to 3rd mandi molar (rt) | Pre | 42.8333 | 9.8789 | −0.8333 | 10.9924 | −0.4152 | 0.6810 |
| Post | 43.6667 | 6.3427 | |||||
| HP to 2nd mandi molar (rt) | Pre | 58.5667 | 5.1708 | −3.6000 | 6.6881 | −2.9482 | 0.0063* |
| Post | 62.1667 | 6.0349 | |||||
| HP to 3rd mandi molar (lft) | Pre | 48.9333 | 11.2370 | 3.4000 | 12.5247 | 1.4869 | 0.1478 |
| Post | 45.5333 | 8.7916 | |||||
| HP to 2nd mandi molar (lft) | Pre | 59.9000 | 8.2977 | 0.2667 | 5.8069 | 0.2515 | 0.8032 |
| Post | 59.6333 | 9.1707 | |||||
| HP to 3rd maxi molar (rt) | Pre | 54.8333 | 14.4367 | −17.100 | 13.4993 | −6.9382 | 0.0000* |
| Post | 71.9333 | 8.3828 | |||||
| HP to 2nd maxi molar (rt) | Pre | 71.0667 | 6.5281 | 17.6333 | 12.7509 | 7.5745 | 0.0000* |
| Post | 53.4333 | 13.6273 | |||||
| HP to 3rd maxi molar (lft) | Pre | 60.9333 | 17.4276 | −4.7667 | 9.6443 | −2.7071 | 0.0113* |
| Post | 65.7000 | 14.8467 | |||||
| HP to 2nd maxi molar (lft) | Pre | 69.9667 | 12.4637 | 2.3000 | 10.5835 | 1.1903 | 0.2436 |
| Post | 67.6667 | 8.1085 |
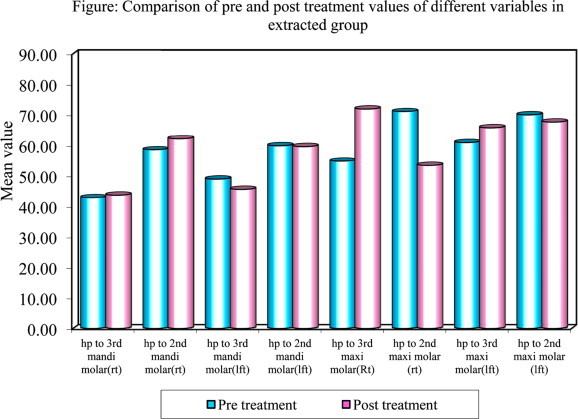
Table 3.
Comparison of pre and post treatment values of different variables in non-extracted group by paired t-test.
| Variable | Treatment | Mean | Std. Dv. | Mean diff | SD diff | Paired t | P-value |
|---|---|---|---|---|---|---|---|
| HP to 3rd mandi molar (rt) | Pre | 43.4333 | 8.9969 | 0.3000 | 8.2049 | 0.2003 | 0.8427 |
| Post | 43.1333 | 9.9680 | |||||
| HP to 2nd mandi molar (rt) | Pre | 61.8667 | 7.3613 | −0.6333 | 5.9624 | −0.5818 | 0.5652 |
| Post | 62.5000 | 6.4581 | |||||
| HP to 3rd mandi molar (lft) | Pre | 49.8333 | 14.9714 | 1.2667 | 9.6773 | 0.7169 | 0.4792 |
| Post | 48.5667 | 12.9046 | |||||
| HP to 2nd mandi molar (lft) | Pre | 63.4667 | 6.3666 | 1.7333 | 8.4687 | 1.1210 | 0.2715 |
| Post | 61.7333 | 9.0817 | |||||
| HP to 3rd maxi molar (rt) | Pre | 59.9333 | 13.8214 | −16.900 | 12.1694 | −7.6064 | 0.0000* |
| Post | 76.8333 | 7.6252 | |||||
| HP to 2nd maxi molar (rt) | Pre | 75.2667 | 12.1767 | 10.8333 | 15.1477 | 3.9172 | 0.0005* |
| Post | 64.4333 | 12.8457 | |||||
| HP to 3rd maxi molar (lft) | Pre | 69.7667 | 15.3638 | 2.0333 | 13.2626 | 0.8397 | 0.4079 |
| Post | 67.7333 | 12.8061 | |||||
| HP to 2nd maxi molar (lft) | Pre | 74.2667 | 13.1803 | −2.9000 | 11.0652 | −1.4355 | 0.1618 |
| Post | 77.1667 | 8.6626 |
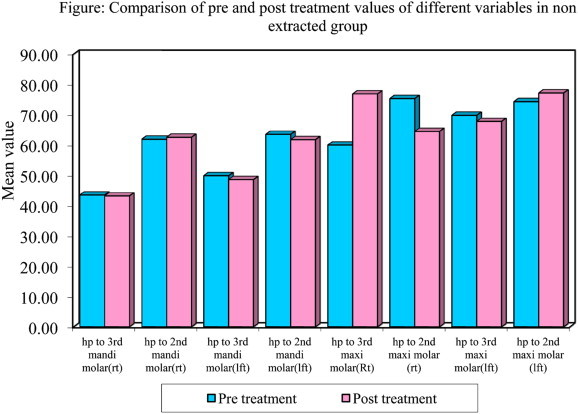
Table 4.
Comparison of extraction and non-extraction cares by t-test.
| Variables | Treatment | Extraction |
Non-extraction |
t-value | P-value | ||
|---|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | ||||
| HP to 3rd mandi molar (rt) | Pre | 43.4333 | 8.9969 | 42.8333 | 9.8789 | 0.2460 | 0.8066 |
| Post | 43.1333 | 9.9680 | 43.6667 | 6.3427 | −0.2472 | 0.8056 | |
| HP to 2nd mandi molar (rt) | Pre | 61.8667 | 7.3613 | 58.5667 | 5.1708 | 2.0092 | 0.0492* |
| Post | 62.5000 | 6.4581 | 62.1667 | 6.0349 | 0.2066 | 0.8371 | |
| HP to 3rd mandi molar (lft) | Pre | 49.8333 | 14.9714 | 48.9333 | 11.2370 | 0.2633 | 0.7932 |
| Post | 48.5667 | 12.9046 | 45.5333 | 8.7916 | 1.0640 | 0.2917 | |
| HP to 2nd mandi molar (lft) | Pre | 63.4667 | 6.3666 | 59.9000 | 8.2977 | 1.8679 | 0.0668 |
| Post | 61.7333 | 9.0817 | 59.6333 | 9.1707 | 0.8912 | 0.3765 | |
| HP to 3rd maxi molar (rt) | Pre | 59.9333 | 13.8214 | 54.8333 | 14.4367 | 1.3977 | 0.1675 |
| Post | 76.8333 | 7.6252 | 71.9333 | 8.3828 | 2.3684 | 0.0212* | |
| HP to 2nd maxi molar (rt) | Pre | 75.2667 | 12.1767 | 71.0667 | 6.5281 | 1.6650 | 0.1013 |
| Post | 64.4333 | 12.8457 | 53.4333 | 13.6273 | 3.2172 | 0.0021* | |
| HP to 3rd maxi molar (lft) | Pre | 69.7667 | 15.3638 | 60.9333 | 17.4276 | 2.0825 | 0.0417* |
| Post | 67.7333 | 12.8061 | 65.7000 | 14.8467 | 0.5680 | 0.5722 | |
| HP to 2nd maxi molar (lft) | Pre | 74.2667 | 13.1803 | 69.9667 | 12.4637 | 1.2983 | 0.1993 |
| Post | 77.1667 | 8.6626 | 67.6667 | 8.1085 | 4.3853 | 0.0000* | |
*P < 0.05.
In non-extraction group no significant change in the angulation of maxillary and mandibular 3rd molar was seen.
Discussion
The study of the mandibular third molar has always aroused great interest in clinical practice. Normally, studies on the third molar has centered on investigating the effects of its eruption on dental arches, but not on observing the changes that orthodontic treatments, with or without extractions, cause in the position and angulation of that molar.
Studies that do appear in the literature on these changes are difficult to compare, as the material and methods used vary.
Third molar eruption can be predicted at an early age during the course of orthodontic treatment, and then later occurrences of difficult impactions can be avoided. The subjects of this study ranged in age from 12 to 17 years, with a mean age of about 13 years; during this time, the third molar bud is developing and is undergoing important rotational pre-eruptive movements.11,12 Therefore, patients in this age group were selected to determine whether the treatment technique (extraction or non-extraction) had any favorable effect on the rotational, uprighting, and pre-eruptive movements taking place at that time.
Measurements of third molar angulation on lateral cephalograms, as seen in previous studies4,17,18,21,22 may be biased because of differences in angulation between the superimposed images. Similar problems are present in any cephalometric study of changes in posterior tooth positions and can only be overcome if measurements are made on 60-degree head films of the left and right sides, as shown by Richardson. However, studies23,24 have shown that panoramic radiographs are a reliable indicator in evaluating third molar positions, and so they were used in the present study. Previous studies have used the occlusal plane,19,20,24,25 mandibular plane,24,25 and palatal plane29 as the horizontal plane of reference to measure treatment changes. However, the changes in the occlusal plane, with treatment, remodeling of the lower border of the mandible during growth and palatal plane may cause misinterpretation of third molar angle calculations. It may be postulated that calculation of third molar angulation relative to Frankfort horizontal plane at each time period may not be misinterpreted in the event of remodeling changes over time. So Frankfort horizontal plane was considered as reference plane in this study.
A significant improvement in maxillary third molar angulation following extraction treatment was seen on both the right (−17 ± 13°) and left (−4 ± 6°) sides. But no change in the angulation of mandibular 3rd molar was seen in extraction group. The present findings associated with mandibular 3rd molars are similar to some previous studies by Graber and Kaineg14 and McCoy,13 which showed that premolar extraction probably does not enhance normal eruption of third molars and contradict previous studies reporting that uprighting or improvements in third molar angulations. With extraction of premolars on mandibular third molar by4,17–22 and Elsey and Rock,19 using the MRP on panoramic radiographs, showed an improvement in third molar angulation by a mean of 7°. However, these authors did not compare the changes on the right and left sides in high anchorage cases and no comparisons were made with a representative group of non-extraction patients.
In non-extraction group, maxillary third molar angulation increased minimally (2.3°) on the right side, and on the left side the mean increase was only (2°) and mandibular third molar angulation increased to 0.3 ± 8 on right side and 1.2 ± 9 on left which were not statistically significant. Hence, the third molar angulations were more or less maintained in all cases and showed very minimal improvement when treatment was done with the non-extraction technique. The present findings corroborate those of previous studies,15,16 in which improvements in some of the third molar angulations occurred, but they were significantly less than those seen in extraction cases. The present results are similar to the findings of Yigit et al,20 who showed a worsening of mandibular third molar angulations with non-extraction treatment. Silling13 stated that non-extraction therapy, by holding back or distally tipping the mandibular first and second molars increased the chances of third molar impaction. The slight changes taking place in the absence of extractions could be attributed to the growth taking place in the retromolar area.
A comparison between extraction and non-extraction group results shown in this study are in contrast with those of previous studies,19–25,29 in which definite improvements were seen with extraction treatment vs non-extraction therapy. The results favor with those of Staggers et al,1 who showed that orthodontic treatment involving premolar extractions did not improve mandibular third molar angulation any more than non-extraction treatment. Staggers et al found that mandibular third molar angulations improved regardless of the method of orthodontic treatment. The uprighting of the maxillary third molars in this study can be attributed to changes occurring at maxillary tuberosity region. Also results of this study suggest that factors other than extractions could influence the inclination and subsequent eruption of maxillary third molars. Bjork et al26 and Svendsen27 suggested that low mandibular growth rate, early physical maturity and late third molar mineralization may be etiological factors of mandibular third molar impactions. Richardson27 stated that the original space conditions in extraction cases, may have more influence on the eruption of third molars than do the premolar extractions. Forsberg3 proposed that extraction cases have a larger tooth size/arch length discrepancy ay still make the third molar impactions more likely in extraction cases than in non-extraction cases.
The initial angulation of third molars may also influence their subsequent eruption. Richardson28 found that third molars with a small degree of angulation erupted earlier than steeper angulations, she believed that mandibular growth is a contributing factor in mandibular third molar eruption, but its exact role is uncertain.
All the patients in this study were dentally and skeletally class I, therefore, there was no need to protract mandibular molars in order to obtain a class I molar relationship. If the subjects had been class II dentally and mandibular molar protraction had been used to correct the molar relation, an even more favorable change in mandibular third molar angulation may have occur. Perhaps the type of mechanics used and anchorage considerations have more of an effect on third molar angulation than actual premolar extraction.
Clinical implications
The greater maxillary and mandibular third molar impaction probability in non-extraction treatment of these cases should also be considered. Preserving the maxillary premolars may result in later extraction of the third molars. Premolar extraction surgery is usually easier and less expensive than third molar extraction (Kim et al, 2003).
Premolar extractions in preadolescent orthodontic patients have a positive influence on third molar angulations by promoting mesial migration and improving the possibility that the third molars will erupt in acceptable positions in maxillary region. Hence, this aspect of dental practice needs to be more widely appreciated in the planning of treatment for children. Although it is not possible to predict from the results how many third molars would erupt fully later on, it is clear that the improved positions would facilitate surgery for many of those teeth that did ultimately require removal. The authors recommend that third molar angulations be included in the treatment planning of borderline extraction cases. When third molar angulations are seen to be less favorable for eruption, although their chances for eruption (as dictated by other factors) can be predicted as high, extracting premolars in such cases will improve their angulations, making them favorable for eruption. The orthodontist must be cautious in evaluating the positions of the third molars when planning treatment, since their final characteristics are late to develop. In patients in whom orthodontic treatment is concluded before complete third molar development, regardless of whether premolar extractions have been done or not, the patient should be recalled when he or she is older for radiographic examination to assess the development of the third molars. If the third molars are becoming impacted, referral to an oral surgeon for surgical removal should be made.
Conclusions
-
•
Premolar extractions had a positive influence on the developing maxillary third molar angulations, and these improved angulations might favor third molar eruptions later in life but no significant change in the angulation of mandibular third molar was seen.
-
•
Non-extraction therapy did not have any adverse effects. Third molar angulations were minimally improved or maintained.
-
•
Borderline cases with favorable third molar angulations can benefit by premolar extractions.
-
•
If the third molars do become impacted after treatment, the improved angulations can help facilitate their surgical removal.
-
•
Study data also apply that orthodontic treatment involving premolar extraction does not improve mandibular 3rd molar angulation any differently than non-extraction treatment. Third molar angulation improved regardless of the method of orthodontic treatment. However, an improvement in angulation does not necessarily mean that 3rd molars will erupt in good position. One can conclude that factors other than first premolar extraction influence 3rd molar angulation and eruption. Therefore it may be prudent for orthodontists to inform their patients that premolar extractions may not prevent the need for third molar extractions in future.
Conflicts of interest
All authors have none to declare.
Contributor Information
Avinash Gohilot, Email: gehlot_avinash@yahoo.co.in.
Kanhoba Mahabaleshwar Keluskar, Email: keluskar@yahoo.com.
References
- 1.Staggers J.A., Germane N., Fortson W.M. A comparison of the effects of first premolar extractions on third molar angulation. Angle Orthod. 1992;2:135–138. doi: 10.1043/0003-3219(1992)062<0135:ACOTEO>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 2.Richardson M.E. The etiology and prediction of mandibular third molar impaction. Angle Orthod. 1977;47:165–172. doi: 10.1043/0003-3219(1977)047<0165:TEAPOM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 3.Forsberg C.M. Tooth size, spacing, and crowding in relation to eruption or impaction of third molars. Am J Orthod Dentofacial Orthop. 1988;94:57–62. doi: 10.1016/0889-5406(88)90451-9. [DOI] [PubMed] [Google Scholar]
- 4.Kim T.-W., Ǻrtun J., Behbehani F., Artese F. Prevalence of third molar impaction in orthodontic patients treated nonextraction and with extraction of 4 premolars. Am J Orthod Dentofacial Orthop. 2003 Feb;123(2):138–145. doi: 10.1067/mod.2003.13. [DOI] [PubMed] [Google Scholar]
- 5.Dachi S.F., Howell F.V. A survey of 3874 routine full-mouth radiographs II. A study of impacted teeth. Oral Surg Oral Med Oral Pathol. 1961;14:1165–1169. doi: 10.1016/0030-4220(61)90204-3. [DOI] [PubMed] [Google Scholar]
- 6.Bishara S.E., Andreasen G. Third molars: a review. Am J Orthod Dentofacial Orthop. 1983;83:131–137. doi: 10.1016/s0002-9416(83)90298-1. [DOI] [PubMed] [Google Scholar]
- 7.Grover P.S., Lorton L. The incidence of unerupted permanent teeth and related clinical cases. Oral Surg Oral Med Oral Pathol. 1985;59:420–425. doi: 10.1016/0030-4220(85)90070-2. [DOI] [PubMed] [Google Scholar]
- 8.Bjork A., Jensen E., Palling M. Mandibular growth and third molar impaction. Acta Odontol Scand. 1956;14:231–271. [Google Scholar]
- 9.Bjork A. Variations in the growth pattern of the human mandible: longitudinal radiographic study by the implant method. J Dent Res. 1963;42:400–411. doi: 10.1177/00220345630420014701. [DOI] [PubMed] [Google Scholar]
- 10.Alling C.C., Alling R.D. WB Saunders Co; Philadelphia, PA: 1993. Indications for Management of Impacted Teeth. Impacted Teeth. 6–49. [Google Scholar]
- 11.Silling G. Development and eruption of the mandibular third molar and its response to orthodontic therapy. Angle Orthod. 1973;43:271–278. doi: 10.1043/0003-3219(1973)043<0271:DAEOTM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 12.Richardson M.E. Pre-eruptive movements of the mandibular third molar. Angle Orthod. 1978;48:187–193. doi: 10.1043/0003-3219(1978)048<0187:PMOTMT>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 13.McCoy J.R. A study of growth potential; from observations made in over 50 years of orthodontic practice. Am J Orthod Dentofacial Orthop. 1965;51:79–97. doi: 10.1016/0002-9416(65)90163-6. [DOI] [PubMed] [Google Scholar]
- 14.Graber T.M., Kaineg T.F. The mandibular third molar: its predictive status and role in lower incisor crowding. Proc Finn Dent Soc. 1981;77:37–44. [PubMed] [Google Scholar]
- 15.Forsberg C.M., Vingren B., Wesslen U. Mandibular third molar eruption in relation to available space as assessed on lateral cephalograms. Swed Dent J. 1989;13:23–31. [PubMed] [Google Scholar]
- 16.Richardson M.E. The effect of mandibular first premolar extraction on third molar space. Angle Orthod. 1989;59:291–294. doi: 10.1043/0003-3219(1989)059<0291:TEOMFP>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 17.Capelli J., Jr. Mandibular growth and third molar impaction in extraction cases. Angle Orthod. 1991;61(3):223–229. doi: 10.1043/0003-3219(1991)061<0223:MGATMI>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 18.Erdem D., Ozdiler E., Toygar Memikoglu U., Baspinar E. Third molar impaction in extraction cases treated with the Begg technique. Eur J Orthod. 1998;20:263–270. doi: 10.1093/ejo/20.3.263. [DOI] [PubMed] [Google Scholar]
- 19.Elsey M.J., Rock W.P. Influence of orthodontic treatment on development of third molars. Br J Oral Maxillofac Surg. 2000;38:350–353. doi: 10.1054/bjom.2000.0307. [DOI] [PubMed] [Google Scholar]
- 20.Yigit M., Gokce D., Kocadereli I., Tasar F. The effects of first premolar extractions on third molar angulations. Angle Orthod. 2005;75:719–722. doi: 10.1043/0003-3219(2005)75[719:TEOFPE]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 21.Artun J., Thalib L., Little R.M. Third molar angulations during and after treatment of adolescent orthodontic patients. Eur J Orthod. 2005;27:590–596. doi: 10.1093/ejo/cji049. [DOI] [PubMed] [Google Scholar]
- 22.Behbehani F., Artun J., Thalib L. Prediction of mandibular third molar impaction in adolescent orthodontic patients. Am J Orthod Dentofacial Orthop. 2006;130:47–55. doi: 10.1016/j.ajodo.2006.03.002. [DOI] [PubMed] [Google Scholar]
- 23.Olive R.J., Basford K.E. Transverse dentoskeletal relationships and third molar impaction. Angle Orthod. 1981;51:41–47. doi: 10.1043/0003-3219(1981)051<0041:TDRATM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 24.Larheim T.A., Svanaes D.B. Reproducibility of rotational panoramic radiography: mandibular linear dimensions and angles. Am J Orthod Dentofacial Orthop. 1986;90:45. doi: 10.1016/0889-5406(86)90026-0. [DOI] [PubMed] [Google Scholar]
- 25.Nanda R.S. Reappraising ‘‘Wits.’’ Readers' forum. Am J Orthod Dentofacial Orthop. 2004;125:18A. doi: 10.1016/j.ajodo.2003.12.012. [DOI] [PubMed] [Google Scholar]
- 26.Bjork A., Jensen, Palling Mandibular growth and third molars. J Am Dent Assoc. 1969;76:316–320. [Google Scholar]
- 27.Svenden H., Bjork A. Third molar impaction – a consequence of late M3 mineralization and early physical maturity. Eur J Orthod. 1988;10:1–12. doi: 10.1093/ejo/10.1.1. [DOI] [PubMed] [Google Scholar]
- 28.Richardson M.E. Some aspects of lower third molar eruption. Angle Orthod. 1947;44:141–145. doi: 10.1043/0003-3219(1974)044<0141:SAOLTM>2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- 29.Jain Suruchi, Valithan Ashima. Influence of first premolar extraction on mandibular third molar angulation. Angle Orthod. 2009;79:1143–1148. doi: 10.2319/100708-525R.1. [DOI] [PubMed] [Google Scholar]