

Abstract
PURPOSE
The purpose of this study was to evaluate whether surface treatments affect the translucency of laminate veneers with different shades and thicknesses.
MATERIALS AND METHODS
A total of 224 disc-shaped ceramic veneers were prepared from A1, A3, HT (High Translucent) and HO (High Opaque) shades of IPS e.max Press (Ivoclar Vivadent) with 0.5 mm and 1.0 mm thicknesses. The ceramics were divided into four groups for surface treatments. Group C: no surface treatments; Group HF: etched with hydrofluoric acid; Group SB: sandblasted with 50-µm Al2O3; and Group L; irradiated with an Er;YAG laser. A translucent shade of resin cement (Rely X Veneer, 3M ESPE) was chosen for cementation. The color values of the veneers were measured with a colorimeter and translucency parameter (TP) values were calculated. A three-way ANOVA with interactions for TP values was performed and Bonferroni tests were used when appropriate (α=0.05).
RESULTS
There were significant interactions between the surface treatments, ceramic shades and thicknesses (P=.001). For the 0.5-mm-thick specimens there were significant differences after the SB and L treatments. There was no significant difference between the HF and C treatments for any shades or thicknesses (P>.05). For the 1-mm-thick ceramics, there was only a significant difference between the L and C treatments for the HT shade ceramics (P=.01). There were also significant differences between the SB and C treatments except not for the HO shades (P=.768).
CONCLUSION
The SB and L treatments caused laminate veneers to become more opaque; however, HF treatment did not affect the TP values. When the laminate veneers were thinner, both the shade of the ceramic and the SB and laser treatments had a greater effect on the TP values.
Keywords: Translucency, Laminate veneer, Surface treatment
INTRODUCTION
Porcelain laminate veneers (PLVs) are one of the conservative restoration types and provide superior translucency.1,2 The challenge with PLVs is the achievement of ideal aesthetics and a desirable bond between the ceramic and the tooth with limited preparation.3 The internal surface of the PLVs can optimize the micromechanical retention of the cement into the microroughness of the ceramic.4 Surface treatment methods, such as acid etching with hydrofluoric acid (HF), sandblasting with Al2O3 particles (SB), laser treatment, or a combination of these methods, have been proposed to provide roughness and micromechanical retention.5 These treatments increase the roughness and create microporosities on the surface of ceramic materials. Surface texture of an object can significantly affect the optical properties and change the perceived translucency.6
Translucency means that a substance permits the passage of light, but it may also scatter the light so that objects cannot be seen clearly through the material; therefore, it could be explained as a state between complete opacity and transparency.7 Reproducing not only the color but also the translucency of the natural tooth is essential for optimal esthetics; as it provides a natural appearance to the restorations.3,4 Based on the CIE L*a*b* system, the translucency of a material is usually determined using the translucency parameter (TP).7,8 The TP value is zero when the material is completely opaque. The greater the TP value shows that the actual translucency of a material is higher.9
The shade of all ceramic restorations can be affected by the small changes in the thickness and shade of the opaque and translucent porcelain layers.10 Small changes may significantly change the color value of the restoration, thereby changing the perception of the color under it.11 The degree of translucency of a material is an inherent property.2 Translucency is mentioned to be directly related to the diffusion of light, and both concepts depend on the refraction index of the material.12 If a surface reflects more light, then less selective absorption is observed. If surface conditions increase light reflection, than transmission is equivalently reduced.6 When light reflection is increased, the color of the object tends to be more luminous and of a higher value.13 Translucency of a sandblasted glass may be greatly reduced14 due to a reflection on its irreugular surface. The glass therefore becomes more opaque on the surface because of the reflection limits the light transmission. These changes on the surface modify not only the color but also the perception of translucency and opacity.6
Lithium disilicate ceramics are currently recommended for PLVs, and can be produced thinner in their crystalline form which makes these ceramics more translucent and aesthetic.14 Previous studies,11,15,16 showed that the color of the underlying tooth and the luting cements can have great influence on the final appearance of laminate restorations. However, there is no existing knowledge about the surface treatments' effect on the translucency values of these esthetic restorations.
Therefore, the aims of this study were to assess whether HF, SB or laser surface treatments affect the translucency of laminates and to evaluate whether different shades of laminates with different thicknesses are affected differently after surface treatments.
The hypotheses of the study were that (i) there would be differences in the TP values of laminates after surface treatments, (ii) surface treatments would differently affect the TP values of the laminates prepared with various shades and (iii) surface treatments would differently affect the TP values of the laminates of various thicknesses.
MATERIALS AND METHODS
A1, A3, HT and HO shades of lithium disilicate all-ceramic (IPS e.max #Press; Ivoclar Vivadent AG, Schaan, Liechtenstein) was used as a PLV material for this study. A total of 224 disc-shaped specimens were prepared according to the manufacturer's directions by burning out 0.5-mm and 1-mm thicknesses of wax with a diameter of 10 mm. The specimens were heat-pressed (IPS Empress EP 600 press furnace) at 920℃ and finished flat on a grinder/polisher with wet #400 to #1200 grit silicone carbide paper; then, they were ultrasonically cleaned in distilled water for 10 minutes. Specimens were then coated on one side with a layer of neutral-shade glaze and fired at 765℃. The thickness of the polished and glazed specimens was measured with a digital caliper (Electronic Digital Caliper; Shan, China), and the specimens were within the range of 0.5 ± 0.05 and 1 ± 0.05 mm. Specimens were ultrasonically cleaned for 10 minutes before cementation. The specimens were divided into four groups for surface treatment (n=7).
Group (C), control
In group (C), no surface treatments were applied on the ceramic surfaces.
Group (HF), acid-etching
The bonding surfaces of ceramic discs were etched with 5% hydrofluoric acid (IPS Ceramic Etching Gel; Ivoclar Vivadent, Schaan, Liechtenstein) for 60 seconds. The gel was rinsed with water for 20 seconds, and then dried with oil-free compressed air.
Group (SB), sandblasting
Ceramic surfaces were abraded for 20 seconds with 50-µm Al2O3 particles (Cojet; 3M ESPE) with a pressure of 2.8 bar and, a distance of 10 mm, perpendicular to the treated surface, by the same operator.
Group (L) laser
An Er:YAG laser (Fotona, Fidelis, Ljublrina, Slovenia) was used for laser irradiation. The laser optical fiber (1.3 mm in diameter) was aligned perpendicular to the ceramic surface at a distance of 1 mm, and then the whole ceramic area was scanned. The parameters of the laser used were 500 mJ (pulse energy), 20 Hz (pulse per second), 10 W (power setting), 37.86 J/cm2 (energy density) and 150 µs (pulse length). Laser irradiation was performed by the same operator.
After the surface treatment of all of the ceramic groups, the specimens were ultrasonically cleaned in distilled water for 5 minutes. A silane coupling agent was applied to the ceramic surfaces using a clean brush, and the specimens were air dried. Rely X Ceramic Primer was applied for 5 seconds and air dried. For all groups a translucent shade of resin cement (Rely X Veneer; 3M ESPE, St. Paul, MN, USA) was chosen for cementation. Resin cements were applied directly from a syringe to the unglazed surface of the ceramic surfaces; then a clean glass slide was placed onto the resin mixture, and a 1-kg weight was placed on top for 20 seconds, forming a 0.1-mm-thick cement layer. Next, to simulate clinical conditions, a curing light was applied to the ceramic surfaces (Elipar Freelight 2; 3M ESPE, St. Paul, MN, USA) for 40 seconds. After cementation, irregularities from excessive resin cement were adjusted with 600-grit wet silicone-carbide paper, and the specimen thickness was calibrated again and standardized at 0.6 and 1.1 mm for all specimens.
The color of each specimen was measured according to the Commission Internationale de l'Eclairage (CIE) system, which evaluates the degree of perceptible color change based on three coordinates; L* (lightness, in which 100 represents white and 0 represents black), a* (red-green chromatic coordinate) and b* (blue-yellow chromatic coordinate).11,17 The color of the glazed surfaces of the specimen was measured over a white (CIE L* = 96.68, a* =-0.18 and b* =-0.22) and a black (CIE L* = 1.15, a* =-0.11 and b* =-0.50) background with a colorimeter (ShadeEye Ex; Shofu, Japan) in a viewing booth under D65 standard illumination. Before the experimental measurements, the colorimeter was calibrated according to the manufacturer's instructions, and the colorimeter was positioned in the middle of each sample. The L*a*b* color notation of each specimen was measured consecutively three times, and the average of the three readings was calculated to give the initial color of the specimen. The TP was obtained by calculating the color difference between the specimen over the white background and that over the black background as follows;
TP = [(Lw* - Lb*)2 + (aw* - ab*)2 + (bw* - bb*)2]1/2(The subscript 'w' refers to the color coordinates over the white background, and the 'b' refers to those over the black).6,10,18 The color differences were analyzed by a three-way analysis of variance (ANOVA) with factors for surface treatments, ceramic shades, and thickness to determine their interactions with TP values. For multiple comparisons, a Bonferroni test was used (α=0.05).
RESULTS
The three-way ANOVA (Table 1) indicated that there were significant interactions between the surface treatment, the ceramic type and the thickness (P=.001). The mean TP values and standard deviations of the ceramics are provided in Table 2 and Table 3.
Table 1.
Three-way ANOVA results
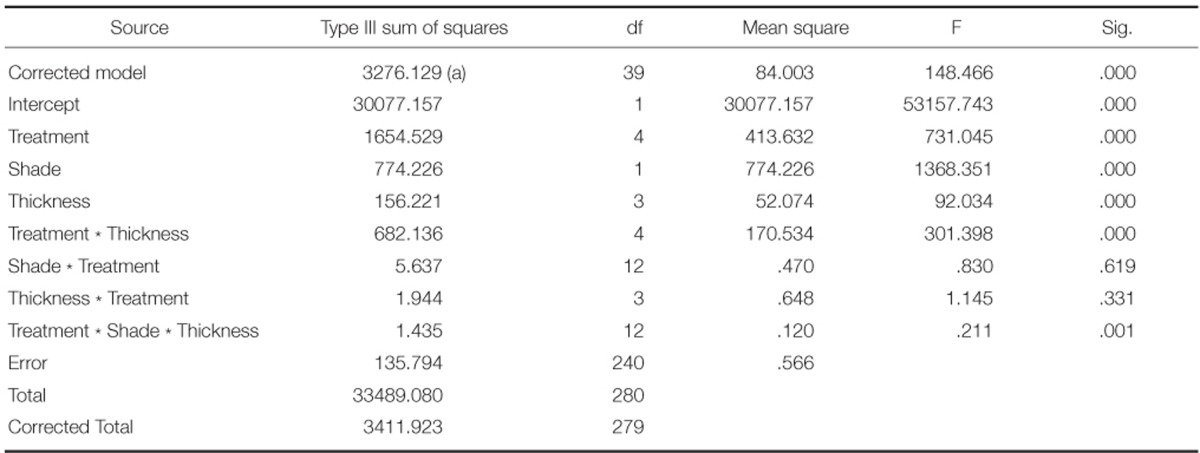
Table 2.
TP values of 0.5-mm-thick laminate veneers after surface treatments

The same superscript upper case letters in same row indicate no significant differences (P>.05) whereas different superscript uppercase letters indicate significant differences (P<.05). The same superscript lower case letters in same column indicate no significant differences (P>.05) whereas different superscript uppercase letters indicate significant differences (P<.05).
Table 3.
TP values of 1.0-mm-thick laminate veneers after surface treatments

The same superscript upper case letters in same row indicate no significant differences (P>.05) whereas different superscript uppercase letters indicate significant differences (P<.05). The same superscript lower case letters in same column indicate no significant differences (P>.05) whereas different superscript uppercase letters indicate significant differences (P<.05).
For 0.5-mm-thick ceramics, there were no significant differences between the control and HF groups for all shades (P>.05). There were significant differences between the laser and the control groups apart from the HO shade ceramics. (P=.726). There were significant differences for all shades of ceramics between the SB and the control groups (P<.05).
Although there were significant differences between the SB and laser groups for the A3 and HT shades (P<.05), there were no significant differences for the A1 or HO shades (P>.05).
For all 1.0-mm-thick ceramics, there were no significant differences between the control and HF groups. There were no significant differences for any shades except the HT shade between the control and laser groups (P=.01). There was no significant difference between the SB and control groups for the HO shades.
The highest TP value occurred after HF treatment of a 0.5-mm-thick HT shade ceramic (22.59) and the lowest TP value occurred after SB treatment of a 1.0-mm-thick HO shade ceramics (4.97).
DISCUSSION
The first hypothesis of the present study, (i), was partially accepted; there were significant differences between the TP values of ceramic veneers after SB or laser treatment, although HF etching did not affect the TP values of the ceramic veneers. The second hypothesis, (ii), was accepted; the surface treatments affected the TP values of the ceramic veneers prepared with different shades. The third hypothesis, (iii), was also accepted; surface treatments differently affected the TP values of ceramic veneers of various thicknesses.
Many studies on the esthetics of laminates have only investigated the color of these restorations. However, many factors, such as the color, opacity and thickness of the porcelain, along with the color of the underlying tooth and the color and thickness of the luting cement could affect the final appearance.11,17,19,20 In previous studies,2,21 ceramic materials have demonstrated varying translucency values, and some ceramics tend to be more opaque and can mask discoloration of the underlying tooth structure. Imitating the translucency of the natural tooth with the color is an important optical factor for ideal esthetics, because the translucency will strongly influence the appearance of the laminates.22
The properties of surface treatments for ceramic surfaces before cementation play a major role in the clinical success of laminates. Changes at the surface texture could also affect the optical properties of the ceramics, and it has been described that the surface waviness has high correlation coefficients with optical parameters.23
After HF etching procedures, the glassy matrix of the ceramic is selectively removed, crystalline structures are exposed, and ceramic surfaces show an amorphous microstructure with numerous porosities.24,25 In the present study, HF etching increased the TP values of the ceramics. However, these changes were not found to be statistically significant. HF etching was performed according to the manufacturers recommendations, and after etching, the ceramic surfaces were rinsed with water. Additionally, before the color measurements were performed, the specimens were ultrasonically cleaned. Ultrasonic cleaning of the etched ceramic in alcohol or distilled water is suggested to remove all residual acid and dissolved debris from the surface. Inadequate rinsing after etching the ceramic surface may leave remineralized salts24 and the ceramics may become more opaque. The etching procedure likely did not affect the ceramics in the present study because the remineralized salts were removed with ultrasonic cleaning.
In the present study, SB was the most effective treatment that changed the TP values of the ceramics. Only the TP values of 1.0-mm-thick HO shade ceramics were not affected after SB; the other ceramics became more opaque. Changes in surface topography have been shown to occur after SB procedures.26 The impact of the blasted particles on the substrate surface results in the transfer of kinetic energy and causes microscopic melting of the surface, causing the surface temperature to rise to 1200℃.27 The silicacoated alumina particles penetrate and are embedded into the surface of the ceramic, leaving the surface partially coated with silica.28 These embedded alumina particles on the ceramic surfaces may also have caused the decrease in TP values after SB in the present study. The decrease of TP values in HT shade ceramics was found to be higher than that in the other shades, and 0.5-mm-thick ceramics were affected more than the 1.0-mm-thick ceramics. It is well-known that ceramics with a greater thickness exhibit lower translucency.29 The thinner and less opaque ceramics may have become more opaque after SB treatment due to the more translucent structure of these restorations, whose surface differences can be observed more clearly.
Currently, laser irradiation is a popular approach for the surface treatment of ceramic materials and many advances have been directed at the use of lasers in clinical applications. This technique has been proposed for surface modification, such as forming a glazed surface on ceramics, etching the ceramic inner surface, or removing ceramic veneers.30-34 However, there is a little information available about the effects of laser lights on restorative materials. In one study;33 the surface of IPS Empress 2 ceramics was analyzed by atomic force microscopy after SB, HF and laser treatments, revealing that SB had the most distinct sharp peaks among the Groups. In another study,34 the roughness of a lithium disilicate-based ceramic was examined and it was reported that Er;YAG laser-irradiated surfaces showed less roughness than air-abraded surfaces while there were no significant differences between acid etching and laser irradiation. Moreover, air abrasion increased the surface roughness of lithium disilicate-based ceramics more effectively than the other treatments. It was apparent that as the ceramic surface became rougher, the light that passed through the ceramic would no longer pass through the matter with the same incidence and direction. Similarly, in the present study, although laser treatment had a significant effect on the TP values, SB was the most effective procedure. Laser treatments caused the ceramics especially 0.5-mm-thick samples to become more opaque. Only the TP value of the 1-mm thick HT shade ceramics was affected by the laser treatment. Surface treatment procedures may cause the ceramics to become more opaque. Considering their effect on the translucency of PLVs, clinicians should use SB or laser treatments carefully, especially when the restoration is thin or prepared with a translucent shade.
CONCLUSION
Within the limitations of the study, the following conclusions were drawn;
- SB treatments caused PLVs to become more opaque.
- Laser treatments caused the PLVs to become more opaque, with the exception of the HO shade ceramics.
- HF etching did not affect the TP values of the PLVs.
- The shades of the PLVs affected the TP values after SB and laser treatments.
- When the PLVs were thinner, the SB and laser treatments had a greater effect on the TP values.
References
- 1.Freire A, Archegas LR. Porcelain laminate veneer on a highly discoloured tooth: a case report. J Can Dent Assoc. 2010;76:a126. [PubMed] [Google Scholar]
- 2.Heffernan MJ, Aquilino SA, Diaz-Arnold AM, Haselton DR, Stanford CM, Vargas MA. Relative translucency of six all-ceramic systems. Part II: core and veneer materials. J Prosthet Dent. 2002;88:10–15. [PubMed] [Google Scholar]
- 3.Addison O, Marquis PM, Fleming GJ. The impact of hydrofluoric acid surface treatments on the performance of a porcelain laminate restorative material. Dent Mater. 2007;23:461–468. doi: 10.1016/j.dental.2006.03.002. [DOI] [PubMed] [Google Scholar]
- 4.Addison O, Marquis PM, Fleming GJ. Adhesive luting of allceramic restorations--the impact of cementation variables and short-term water storage on the strength of a feldspathic dental ceramic. J Adhes Dent. 2008;10:285–293. [PubMed] [Google Scholar]
- 5.Saraçoğlu A, Cura C, Cötert HS. Effect of various surface treatment methods on the bond strength of the heat-pressed ceramic samples. J Oral Rehabil. 2004;31:790–797. doi: 10.1111/j.1365-2842.2004.01305.x. [DOI] [PubMed] [Google Scholar]
- 6.Villarroel M, Fahl N, De Sousa AM, De Oliveira OB., Jr Direct esthetic restorations based on translucency and opacity of composite resins. J Esthet Restor Dent. 2011;23:73–87. doi: 10.1111/j.1708-8240.2010.00392.x. [DOI] [PubMed] [Google Scholar]
- 7.Powers JM. Restorative dental materials. 12th ed. St. Louis: Mosby; 2006. pp. 35–42. [Google Scholar]
- 8.Paravina RD, Ontiveros JC, Powers JM. Curing-dependent changes in color and translucency parameter of composite bleach shades. J Esthet Restor Dent. 2002;14:158–166. doi: 10.1111/j.1708-8240.2002.tb00516.x. [DOI] [PubMed] [Google Scholar]
- 9.Craig RG, Powers JM. Optical, thermal, and electrical properties. In: Craig RG, Powers JM, editors. Restorative dental materials. 11th ed. St Louis: (MO)Mosby; 2002. pp. 38–44. [Google Scholar]
- 10.Ryan EA, Tam LE, McComb D. Comparative translucency of esthetic composite resin restorative materials. J Can Dent Assoc. 2010;76:a84. [PubMed] [Google Scholar]
- 11.Turgut S, Bagis B. Colour stability of laminate veneers: an in vitro study. J Dent. 2011;39:e57–e64. doi: 10.1016/j.jdent.2011.11.006. [DOI] [PubMed] [Google Scholar]
- 12.Fujita K, Nishiyama N, Nemoto K, Okada T, Ikemi T. Effect of base monomer's refractive index on curing depth and polymerization conversion of photo-cured resin composites. Dent Mater J. 2005;24:403–408. doi: 10.4012/dmj.24.403. [DOI] [PubMed] [Google Scholar]
- 13.Duarte S, Jr, Perdigão J, Lopes M. Composite resin restorations--natural aesthetic and dynamics of light. Pract Proced Aesthet Dent. 2003;15:657–664. quiz 666. [PubMed] [Google Scholar]
- 14.Chu FC, Chow TW, Chai J. Contrast ratios and masking ability of three types of ceramic veneers. J Prosthet Dent. 2007;98:359–364. doi: 10.1016/S0022-3913(07)60120-6. [DOI] [PubMed] [Google Scholar]
- 15.Stevenson B, Ibbetson R. The effect of the substructure on the colour of samples/restorations veneered with ceramic: a literature review. J Dent. 2010;38:361–368. doi: 10.1016/j.jdent.2010.01.009. [DOI] [PubMed] [Google Scholar]
- 16.Chaiyabutr Y, Kois JC, Lebeau D, Nunokawa G. Effect of abutment tooth color, cement color, and ceramic thickness on the resulting optical color of a CAD/CAM glass-ceramic lithium disilicate-reinforced crown. J Prosthet Dent. 2011;105:83–90. doi: 10.1016/S0022-3913(11)60004-8. [DOI] [PubMed] [Google Scholar]
- 17.Kilinc E, Antonson SA, Hardigan PC, Kesercioglu A. Resin cement color stability and its influence on the final shade of all-ceramics. J Dent. 2011;39:e30–e36. doi: 10.1016/j.jdent.2011.01.005. [DOI] [PubMed] [Google Scholar]
- 18.Yu B, Lee YK. Influence of color parameters of resin composites on their translucency. Dent Mater. 2008;24:1236–1242. doi: 10.1016/j.dental.2008.01.016. [DOI] [PubMed] [Google Scholar]
- 19.Imirzalioglu P, Karacaer O, Yilmaz B, Ozmen Msc I. Color stability of denture acrylic resins and a soft lining material against tea, coffee, and nicotine. J Prosthodont. 2010;19:118–124. doi: 10.1111/j.1532-849X.2009.00535.x. [DOI] [PubMed] [Google Scholar]
- 20.Lu H, Powers JM. Color stability of resin cements after accelerated aging. Am J Dent. 2004;17:354–358. [PubMed] [Google Scholar]
- 21.Luo XP, Zhang L. Effect of veneering techniques on color and translucency of Y-TZP. J Prosthodont. 2010;19:465–470. doi: 10.1111/j.1532-849X.2010.00610.x. [DOI] [PubMed] [Google Scholar]
- 22.Chu SJ. Precision shade technology: contemporary strategies in shade selection. Pract Proced Aesthet Dent. 2002;14:79–83. [PubMed] [Google Scholar]
- 23.Wang H, Xiong F, Zhenhua L. Influence of varied surface texture of dentin porcelain on optical properties of porcelain specimens. J Prosthet Dent. 2011;105:242–248. doi: 10.1016/S0022-3913(11)60039-5. [DOI] [PubMed] [Google Scholar]
- 24.Lu R, Harcourt JK, Tyas MJ, Alexander B. An investigation of the composite resin/porcelain interface. Aust Dent J. 1992;37:12–19. doi: 10.1111/j.1834-7819.1992.tb00827.x. [DOI] [PubMed] [Google Scholar]
- 25.Peumans M, Van Meerbeek B, Lambrechts P, Vanherle G. Porcelain veneers: a review of the literature. J Dent. 2000;28:163–177. doi: 10.1016/s0300-5712(99)00066-4. [DOI] [PubMed] [Google Scholar]
- 26.Roulet JF, Söderholm KJ, Longmate J. Effects of treatment and storage conditions on ceramic/composite bond strength. J Dent Res. 1995;74:381–387. doi: 10.1177/00220345950740011501. [DOI] [PubMed] [Google Scholar]
- 27.Gbureck U, Masten A, Probst J, Thull R. Tribochemical structuring and coating of implant metal surfaces with titanium oxide and hydroxyapatite layers. Mater Sci Eng C. 2003;23:461–465. [Google Scholar]
- 28.Lung CY, Matinlinna JP. Aspects of silane coupling agents and surface conditioning in dentistry: an overview. Dent Mater. 2012;28:467–477. doi: 10.1016/j.dental.2012.02.009. [DOI] [PubMed] [Google Scholar]
- 29.Antonson SA, Anusavice KJ. Contrast ratio of veneering and core ceramics as a function of thickness. Int J Prosthodont. 2001;14:316–320. [PubMed] [Google Scholar]
- 30.Kamada K, Yoshida K, Atsuta M. Effect of ceramic surface treatments on the bond of four resin luting agents to a ceramic material. J Prosthet Dent. 1998;79:508–513. doi: 10.1016/s0022-3913(98)70170-2. [DOI] [PubMed] [Google Scholar]
- 31.da Silva Ferreira S, Hanashiro FS, de Souza-Zaroni WC, Turbino ML, Youssef MN. Influence of aluminum oxide sandblasting associated with Nd:YAG or Er:YAG lasers on shear bond strength of a feldspathic ceramic to resin cements. Photomed Laser Surg. 2010;28:471–475. doi: 10.1089/pho.2009.2528. [DOI] [PubMed] [Google Scholar]
- 32.Shiu P, De Souza-Zaroni WC, Eduardo Cde P, Youssef MN. Effect of feldspathic ceramic surface treatments on bond strength to resin cement. Photomed Laser Surg. 2007;25:291–296. doi: 10.1089/pho.2007.2018. [DOI] [PubMed] [Google Scholar]
- 33.Yavuz T, Dilber E, Kara HB, Tuncdemir AR, Ozturk AN. Effects of different surface treatments on shear bond strength in two different ceramic systems. Lasers Med Sci. 2013;28:1233–1239. doi: 10.1007/s10103-012-1201-5. [DOI] [PubMed] [Google Scholar]
- 34.Kara HB, Dilber E, Koc O, Ozturk AN, Bulbul M. Effect of different surface treatments on roughness of IPS Empress 2 ceramic. Lasers Med Sci. 2012;27:267–272. doi: 10.1007/s10103-010-0860-3. [DOI] [PubMed] [Google Scholar]