

Abstract
The aim of this study was to evaluate the alterations in eccentric evertor/concentric invertor strength ratio and their importance in the chronically unstable ankle. Eight patients with chronic ankle instability (CAI) and nine healthy individuals participated in this study. Isokinetic concentric and eccentric invertor and evertor muscle strength measurement was carried out at an angular velocity of 120°·sec-1 by measuring maximal force moments (torque) during isokinetic ankle inversion and eversion movements. Functionally, evertor/invertor muscle strength ratios (E/I strength ratio) were calculated separately based on peak moment and angle-specific moments obtained at 0°, 5°, 10°, 15°, 20° ankle joint angles. Peak and angle-specific eccentric evertor strength values at 0°, 5°, 10°, 15°, 20° were significantly lower in the chronic ankle instability (CAI) group. In spite of this, no differences were obtained for peak and angle-specific concentric invertor torque values. Eccentric evertor/concentric invertor strength (Eecc/Icon) ratios were also significantly lower in the CAI group, but only at 15° and 20°. Eccentric evertor muscle torque and end range (15°-20°) Eecc/Icon strength ratio for the chronically unstable ankle were significantly different from those for the healthy ankle. For this reason, measurements of end range eccentric/concentric strength ratios are more valuable in monitoring chronic ankle injuries and rehabilitation should include not only concentric muscle strengthening but also eccentric muscle strengthening, particularly for the evertor muscles.
Key words: Unstable ankle, strength ratios, eccentric evertor, concentric invertor
Introduction
Sprain of the lateral ankle ligaments is one of the most common injuries sustained during sport (Garrick and Requa, 1988). Given the high prevalance of this injury, and the large proportion of sufferers who continue to experience related functional disability, it is important to identify impairments that contribute to functional ankle instability. The most common complicationsfollowing ankle sprain are mechanical and functional instability (Irrgang et al., 1994; Wester et al., 1996), and it has been suggested that weakness specifically of the ankle evertors after ankle injury may be a contributory factor in this instability (Tropp, 1986).
Isokinetic muscle strength testing is used by clinicians for the evaluation of ankle evertor or invertor muscle strength differences, for the assessment of concentric and eccentric peak torque in different sporting populations, or for detecting muscle strength loss after injury (Aydin et al., 2001a; Aydin et al., 2001b; Aydin et al., 2002). The evertor/invertor ratios for either concentric or eccentric muscle activity are also used as guidelines for managing strength training or injury rehabilitation by assessing changes in the ratios after training or injury (Wilkerson et al., 1997; Aydin et al., 2002; Munn et al., 2003). During athletic activities, agonist muscles produce concentric work to accelerate the limb, whereas antagonist muscles generate eccentric work to control this concentric work and prevent joint overloading. Because of this, it has been suggested that the concentric and eccentric agonist/antagonist strength ratio may not be functionally relevant (Aagaard et al., 1998). Aagaard et al. (1995; 1998) further suggested that functionally more important ratios are created by dividing the eccentric strength of the antagonist muscle by the corresponding concentric strength value of the agonist muscle (Antecc/Agocon strength ratio) in an isokinetic evaluation. The Antecc/Agocon ratio is velocity dependent and increases proportionately with test velocity (Perrin, 1993; Dvir, 1995).
At present there is no data Antecc/Agocon ratio in the human ankle. Earlier Aagard (1998) investigated eccentric hamstring/concentric quadriceps ratios in healthy subjects. Gibson et al. (2000) also showed that eccentric hamstring/ concentric quadriceps ratios were similar in anterior cruciate ligamant (ACL) deficient and normal limbs. Most studies about the ankle have used eccentric agonist/concentric agonist ratios (Hartsell et al., 1997; Wilkerson et al., 1997; Hartsell and Spaulding, 1999; Munn et al., 2003). Reinking (1991) reported the eccentric/concentric ratios for the dorsiflexors of the ankle to be 1,45and 1,50 for velocities of 30°·sec-1 and 90°·sec-1 respectively. Hartsell and Spaulding (1999) compared the ratios of invertor and evertor ankle muscles of healthy subjects with patients suffering from chronic unstable ankle at 4 different angular velocities (60°, 120°, 180° and 240°·sec-1). As a result, they reported no significant difference in the eccentric/concentric ratios between patients and a corresponding control group.
Lateral ankle sprains characteristically occur toward the end range (0°-30°) (Wright et al., 2000). There are numerous factors and mechanisms that are thought to prevent increased ankle sprain occurence (Lentell et al., 1995). The eccentric evertor/ concentric invertor strength ratio (Eecc/Icon) is one of those factors associated in the prevention of inversion trauma. An increase in this ratio toward end range (from 0° neutral position to 30° inversion angle) is expected for preventing ankle inversion sprain. It is thought that the ratio is decreased in an acute sprain of the ankle. However, the ratio has not been evaluated in the acute period, owing to the inability of performing isokinetic tests. In the chronic period, a decline in Eecc/Icon strength ratio toward end range may occur due to swelling, pain, injury to the muscles, ineffective exercise programmes or ligament laxity. To date there is no detailed information on this issue. The purpose of the present study was to evaluate alterations in eccentric evertor/concentric invertor strength ratio toward the end range and evaluate its importance in the chronically unstable ankle.
Methods
Subjects
Two groups of subjects were used, a control group of healthy subjects and a group with ankle instability. The chronic ankle instability group (CAI) consisted of 8 men who had sustained at least two moderate sprains to the same ankle which required medical intervention and who complained of repeated episodes of “giving way”. No subjects had suffered injury to the unstable ankle for at least six months before testing, were not undergoing rehabilitation of the ankle, nor had any complaints of pain, swelling, or functional limitations. The healthy group consisted of 9 men with no prior history of pathology to either lower extremity. Active range of motion (dorsiflexion/plantarflexion; inversion/ eversion) as measured using an electronic goniometer (Cybex, EDI 320, USA) were found to be within normal limits for both groups. No subjects were involved in physical activity that exceeded three sessions a week for more than half an hour per session. Written consent was obtained from each subject before testing, and all subjects were screened to ensure that were no lower extremity neuromuscular or musculoskeletal problems or contraindications for isokinetic testing. After being informed about the study and test procedures, and any possible risks and discomfort that might ensue, their written informed consent to participate was obtained in accordance with the Helsinki Declararion (WMADH, 2000).
Isokinetic Strength Measurement
Subjects performed a ten-minute warm-up of general range of motion and stretching exercise for joint movements of inversion/eversion and dorsiflexion/ plantarflexion. After the warm-up, they were appropriately positioned on the isokinetic dynamometer (Cybex Norm, USA), which was calibrated before testing each subject. The subtalar joint was positioned in the neutral of inversion, and eversion was identified using palpation during passive movement of the talus (Ronkonkoma, 1995; Donatelli, 1996). The talocrural joint was positioned in 10°-15° plantarflexion as a consequence of the low cut lace up shoe worn by each subject that simulated a position for inversion injury (Wong et al., 1984). Two straps, which crossed to the dorsum of the foot, were attached to the footplate. The knee of the test leg was positioned in 80°-110° flexion and the lower leg was parallel to the floor. The thigh stabiliser pad and strap secured the distal aspect of the thigh for the test leg and a seatbelt placed around the abdomen secured the torso.
Three submaximal trials were followed by five maximal concentric and eccentric invertor trials. Evertor muscle strength was obtained by measuring maximal force moments (torque) during isokinetic ankle inversion and eversion movements at 120°·sec -1 angular velocity. To ensure that a maximal effort was attained, all subjects received positive verbal encouragement during testing. The same investigator performed all the tests to ensure standardization. A two-minute rest was permitted between the test for inversion and eversion to prevent the build up of fatigue (Perrin, 1993; Dvir, 1995).
Functional Evertor/Invertor Muscle Strength Ratio
Evertor/Invertor muscle strength ratios (E/I strength ratio) were calculated separately based on peak moment and angle-specific moments obtained at 0°, 5°, 10°, 15° and 20° ankle joint angles. The functional E/I strength ratio representative for ankle inversion (Eecc/Icon) was determined as the maximal eccentric evertor moment divided by maximal concentric invertor moment and was calculated separately at each of the respective joint angles.
Data Analysis
The Cybex NORM software program provided the measures of peak torque at each ankle angle (0°-20°). The Mann Whitney U and Friedman tests were used for comparing parameters between and within groups, respectively. The level of significance for statistical analysis was set at a p value of <0.05. The data is presented as means ± SD.
Results
Age, height and weight of the two groups were similar (Table 1). Eccentric evertor peak torque values were lower in the CAI group (p=0.009, Table 2). In spite of this, concentric invertor peak torque and peak eccentric evertor/concentric invertor strength ratios (p-Eecc/Icon) were similar in the two groups (Table 2). Eccentric evertor peak torque values were significantly lower in the CAI group from 0° to 20° inversion angle (Table 2).
Table 1.
Physical characteristics of the subjects. Data are mean (SD).
| Chronic Ankle Instability | Healthy | |
|---|---|---|
| Age (years) | 26 (2) | 25 (2) |
| Height (m) | 1.73 (.06) | 1.74 (.04) |
| Weight (kg) | 72.3 (4.3) | 71.9 (5.1) |
Table 2.
Peak and angle specific eccentric evertor, concentric invertor strength and Eecc/Icon ratio toward the end range in chronic ankle instability and healthy groups. Data are mean (SD).
| Chronic Ankle Instability | Healthy | |||||
|---|---|---|---|---|---|---|
| Ecc-Ev (Nm) |
Con-In (Nm) |
Ratio | Ecc-Ev (Nm) |
Con-In (Nm) |
Ratio | |
| Peak Torque | 28.9 (5.3)** | 18.6 (4.5) | 1.7 (0.6) | 37.3 (5.8) | 19.7 (3.6) | 1.9 (0.5) |
| 0° | 24.4 (5.4)* | 18.8 (4.2) | 1.3 (0.3) | 32.8 (4.9) | 20.9 (4.3) | 1.7 (0.5) |
| 5° | 24.8 (6.5)* | 15.8 (3.4) | 1.6 (0.3) | 34.7 (5.2) | 17.6 (4.5) | 2.1 (0.7) |
| 10° | 23.1 (8.4)** | 12.5 (3.7) | 1.9 (0.6) | 36.7 (5.5) | 15.3 (5.0) | 2.7 (1.1) |
| 15° | 19.1 (10.3)** | 8.6 (3.0) | 2.2 (0.6)* | 37.6 (5.7) | 11.4 (4.8) | 3.9 (1.7) |
| 20° | 15.7 (8.2)** | 6.0 (2.3) | 2.6 (0.7)* | 32.8 (6.0) | 8.3 (4.4) | 4.9 (2.5) |
Abbreviations: Ecc-Ev: Eccentric Evertor, Con-In: Concentric Invertor, Ratio: Eccentric Evertor/Concentric Invertor (Eecc/Icon).
* denote p<0.05
** denote p <0.01 – CAI group compared with healthy group.
Although concentric invertor peak torque values from 0° to 20° inversion angle were lower in the CAI group, these differences were not statistically significant compared with the control group (Table 2).
Eccentric evertor/concentric invertor strength (Eecc/Icon) ratios were significantly lower in the CAI group at 15° and 20° compared with the healthy group (p<0.05, Figure 1, Table 2).
Figure 1.
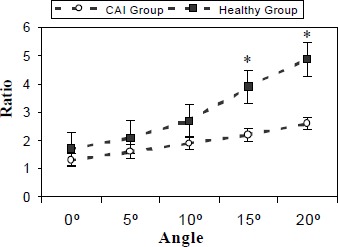
Eccentric evertor/concentric invertor (Eecc/Icon) strength ratios toward the end range at 120° sec-1 angular velocity. Error bars indicate SD. * indicates p < 0.05.
Eccentric evertor peak torque values toward the end range were significantly decreased in the chronic ankle instability group compared with the healthy group (Table 2, Figure 1). Concentric invertor peak torque values were significantly decreased toward the end range for both groups. In contrast, Eecc/Icon strength ratios toward the end range were significantly increased within both groups.
Discussion
Muscle weakness and functional instability at the ankle were found to exist at the same time. The chronically unstable ankle was significantly weaker than the healthy ankle especially for the eccentric evertors. While this observed relation between peroneal muscle weakness and functional instability supported earlier findings (Bosien et al., 1955; Tropp, 1986), a similar finding was also observed for the invertor muscle, which is a new finding (Hartsell et al., 1997; Munn et al., 2003).
The chronically unstable ankle would appear to be at risk of re-injury. Ligamentous injury typically occurs when the peroneal muscles are called upon to work eccentrically in response to high velocity movements (Lentell et al., 1990).
Few studies have investigated eccentric evertor and invertor ankle strength in functional ankle instability. To date, three studies have compared the injured with the non-injured limb in subjects with functional ankle instability. None of the studies showed a deficit in eccentric evertor muscle strength (Bernier et al., 1997; Heitmann et al., 1997; Kaminski et al., 1999; Munn et al., 2003). Hartsell et al. (1997) established eccentric evertor muscle weakness comparing patients with normal subjects. In our study, eccentric evertor peak torque strength of the evertor muscles was 28.9±5.3 Nm in CAI and 37.3±5.8 Nm in the control group (p < 0.01).
Eccentric evertor strength weakness might be explained as follows. Biomechanical changes around the ankle joint caused by chronically unstable ankle deficiency might affect eccentric activity to a greater degree than healthy ankle joints. In addition, evertor muscle atrophy might affect eccentric activity at the cellular level. It is not possible to assess from our study which of these factors is the cause of the deficits in evertor eccentric peak torque relative to the healthy ankle. The finding that the concentric invertor peak torque was not significantly different between the CAI and healthy groups indicates that strength losses were not a result of altered joint motion dynamics, but rather from a deficiency in the muscles themselves or their neural control mechanism.
It was previously reported that concentric invertor muscle strength deficit was observed in the chronic unstable ankle (Wilkerson et al., 1997). In a recent study, concentric invertor muscle weakness was not observed when comparing the normal and disabled limbs (Munn et al., 2003). They supported the idea that eccentric strength deficits of the invertor muscle may contribute to symptoms of ankle instability through a reduced capacity to control lateral postural sway in weight bearing. In our study, we did not find a concentric invertor muscle strength deficit (CAI Group:18.6±4.5 Nm; Control Group:19.7±3.6 Nm). This data shows that concentric invertor muscle strength may not contribute to chronic ankle instability.
Eccentric evertor/concentric evertor and eccentric invertor/concentric invertor strength ratios have been described in individuals with chronically unstable ankle (Hartsell and Spaulding, 1999). However, no previous studies have described the functional Eecc/Icon strength ratio changes associated with CAI and healthy groups. Hartsell and Spaulding (1999) reported that eccentric/concentric strength ratio for the eversion and inversion motions were found to be similar in both groups (injured and healthy groups) and to increase proportionally with increasing velocities, which supports previous research on healthy subjects tested at the elbow and knee. They found that with 120°·sec-1 angular velocity eccentric evertor/concentric evertor strength ratio was 1.72 in the healthy group and 1.83 in patients with chronic ankle instability. The eccentric evertor/concentric evertor strength ratio found in their study contradicts Aagaard’s recent findings (Aagaard et al., 1998). Gibson et al. (2000) showed that the eccentric hamstring/concentric quadriceps strength ratios were similar in ACL deficient and normal limbs .
In our study peak Eecc/Icon strength ratio was 1.7 in the CAI and 1.9 in the healthy group. This difference was not significant. It has been suggested that the eccentric/concentric ratio describes functional capacity more accurately than the agonist concentric/antagonist concentric or agonist eccentric/antagonist eccentric muscle strength ratios. This is because normal gait and movement patterns involve interaction between eccentric and concentric antagonist activity, rather than concentric-concentric muscle activity as described by the concentric agonist/antagonist strength ratio (Aagaard et al., 1998). Thus, the finding that the Eecc/Icon strength ratio is similar in CAI and healthy groups may have functional significance. First of all, we can speculate about the neural activity pattern regulating and reducing the loss of strength in evertor and invertor muscles for the continuity of the normal function of the ankle joint in the CAI group. Indeed, Synder-Mackler et al. (1997) suggested that the ability to alter neuromuscular control patterns might be a determining factor in successful compensation after ACL injury. In our study we can not establish either the alterations originating from peripheral proprioceptive receptor or their effects after acute ankle injury. Nevertheless, the theory suggesting a neural pathway was changed that may explain the similarity of Eecc/Icon strength ratios in the CAI and healthy group. In addition to this, evertor eccentric muscle strength and Eecc/Icon strength ratio serve as a preventive force in chronic ankle injury. Therefore, despite the similar Eecc/Icon strength ratios between CAI and the healthy group, during functional activity the protective eccentric evertor response may not operate with enough vigour to reduce functional instability in the CAI. Relating to this result, we suggest that in addition to increased laxity, the loss of eccentric strength in evertor muscles may also account for recurrent ankle traumain the CAI group.
Lateral ankle sprain are seen in situations which ligamentory support is decreased and the mechanical axis is compromised (at the end range). Eccentric evertor muscle strength and Eecc/Icon strength ratios toward the end range are the preventive factors in this kind of trauma. The increase in Eecc/Icon strength ratios in both groups can be determined as a mechanism which prevents ankle injury. However, the question remains; why do the recurrent injuries occur in the CAI group? Although the decreases in concentric invertor muscle strength in both groups were similar; the decrease in eccentric evertor muscle strength was significantly greater in the CAI than in the healthy group at 0°, 5°, 10°, 15° and 20°. Eecc/Icon strength ratios were significantly lower in the CAI than the control group, especially at 15° and 20° (Table 2, Figure 1). The loss of eccentric strength in evertor muscle and the the low Eecc/Icon strength ratios toward the end range clarify the recurrent ankle sprain in CAI group.
Conclusion
The current study supports that end range (15°-20°) Eecc/Icon strength ratios and eccentric evertor muscle torque for the chronically unstable ankle are significantly different from those for the healthy ankle. On the contrary, there was no significant difference between the two groups for peak Eecc/Icon strength ratio. For this reason, measurements of end range Ecc/Con strength ratios rather than ratios evaluated at smaller ranges are most valuable in chronic ankle injuries. Eccentric evertor strength weakness may predispose recurrent ankle injuries in cases of biomechanical insufficiency of the ankle joint. It may be concluded that rehabilitation should include not only concentric muscle strengthening but also eccentric muscle strengthening, particularly for the evertor muscles.
Biographies

Yavuz YILDIZ
Employment:
Ass. Prof. Depart. of Sports Medicine, Gulhane Military Med. Academy, Ankara, Turkey
Degree:
MD
Research interest:
Sports injuries, isokinetic exercise, proprioception, metabolism and gas exchange kinetics.
E-mail: yasabis@yahoo.com
Taner AYDIN
Employment:
Assoc. Prof. Depart. of Sports Med., Gulhane Military Medical Academy, Ankara, TUR
Degrees:
MD
Research interest:
ACL rehabilitation, proprioception, metabolism and gas exchange kinetics.
E-mail: taydin@gata.edu.tr

Ufuk SEKIR
Employment:
Consultant, Depart. of Sports Med., Uludag Univ., Bursa, TUR
Degrees:
MD
Research interest:
Proprioception, ACL rehabilitation, ostearthritis and exercise.
E-mail: ufuksek@hotmail.com
Bulent HAZNECI
Employment:
Ass. Prof., Depart. of Physical Med. and Rehab., Gulhane Military Medical Academy, Ankara, TUR
Degree:
MD
Research interest:
Sports injuries, ostearthritis and exercise, paediatric rehabilitation
E-mail: bhazneci@gata.edu.tr
Mahmut KOMURCU
Employment:
Assis.t Prof., Depart. of Orthopaedic Surgery and Traumatology, Gulhane Military Medical Academy, Ankara, TUR
Degrees:
MD
Research interest:
Hand and ankle surgery
E-mail: mkomurcu@gata.edu.tr
Tunc Alp KALYON
Employment:
Chair Prof., Depart. of Sports Med., Gulhane Military Medical Academy, Ankara, TUR
Degrees:
MD
Research interest:
Sports injuries, ostearthritis and exercise, metabolism and gas exchange kinetics
E-mail: tkalyon@gata.edu.tr
References
- Aagaard P., Simonsen E. B., Magnusson S.P., Larsson B., Dyhre-Poulsen P. (1998) A new concept for isokinetic hamstring: quadriceps muscle strength ratio. American Journal of Sports Medicine 26, 231-237 [DOI] [PubMed] [Google Scholar]
- Aagaard P., Simonsen E.B., Trolle M., Bangsbo J., Klausen K. (1995) Isokinetic hamstring/ quadriceps strength ratio: influence from joint angular velocity, gravity correction and contraction mode. Acta Physiologica Scandinavica 154, 421-427 [DOI] [PubMed] [Google Scholar]
- Aydin T., Yildiz Y., Yanmis I., Yildiz C., Kalyon T.A. (2001a) Shoulder proprioception: a comparison between the shoulder joint in healthy and surgically repaired shoulders. Archives of Orthopaedic and Trauma Surgery 121, 422-425 [DOI] [PubMed] [Google Scholar]
- Aydin T., Yildiz Y., Yildiz C., Atesalp S., Kalyon T.A. (2002) Proprioception of the ankle: a comparison between female teenaged gymnasts and controls. Foot & Ankle International 23, 123-29 [DOI] [PubMed] [Google Scholar]
- Aydin T., Yildiz Y., Yildiz C., Kalyon T.A. (2001b) The stretch-shortening cycle of the internal rotators muscle group measured by isokinetic dynamometry. Journal of Sports Medicine and Physical Fitness 41, 371-379 [PubMed] [Google Scholar]
- Bernier J., Perrin D., Rijke A. (1997) Effect of unilateral functional instability of the ankle on postural sway and inversion and eversion strength. Journal of Athletic Training 32, 226-232 [PMC free article] [PubMed] [Google Scholar]
- Bosien W.R., Staples O.S., Russel S.W. (1955) Residual disability following acute ankle sprain. Journal of Bone and Joint Surgery-American Volume 37, 1237-1243 [PubMed] [Google Scholar]
- Donatelli R. (1996) The biomechanics of the foot and ankle. 2nd edition FA Davis Co, Philadelphia [Google Scholar]
- Dvir Z. (1995) Isokinetic: muscle testing, interpretation and clinical application. Churchill Livingstone, New York [Google Scholar]
- Garrick J., Requa R. (1988) The epidemiology of foot and ankle injuries in sport. Clinics in Sports Medicine 7, 29-36 [PubMed] [Google Scholar]
- Gibson A., Lambert M.I., Durandt J.J., Scales N., Noakes T.D. (2000) Quadriceps and hamstrings peak torque ratio changes in persons with chronic anterior cruciate ligament deficiency. Journal of Orthopaedic & Sports Physical Therapy 30, 418-427 [DOI] [PubMed] [Google Scholar]
- Hartsell H.D., Spaulding S.J. (1999) Eccentric/concentric ratios at selected velocities for the invertor and evertor muscles of the chronically unstable ankle. British Journal of Sports Medicine 33, 255-258 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hartsell H.D., Wilkerson G.B., Pinerola J.J., Caturano R.W. (1997) Invertor vs. evertor peak torque and power deficiencies associated with lateral ankle ligament injury. Journal of Orthopaedic & Sports Physical Therapy 26, 78-86 [DOI] [PubMed] [Google Scholar]
- Heitmann R., Kovaleski J., Gurchiek L. (1997) Isokinetic eccentric strength of the ankle evertors after injury. Perceptual and Motor Skills 84, 258. [DOI] [PubMed] [Google Scholar]
- Irrgang J.J., Whitney S.L., Cox E.D. (1994) Balance and proprioceptive training for rehabilitation of the lower extremity. Journal of Sports Rehabilitation 3, 68-83 [Google Scholar]
- Kaminski T., Perrin D., Gansneder B. (1999) Eversion strength analysis of uninjured and functionally unstable ankles. Journal of Athletic Training 34, 239-245 [PMC free article] [PubMed] [Google Scholar]
- Lentell G., Baas B., Lopez D., McGuire L., Sarrels M., Synder P. (1995) The contributions of proprioceptive deficits, muscle function and anatomic laxity to functional instability of the ankle. Journal of Orthopaedic & Sports Physical Therapy 21, 206-215 [DOI] [PubMed] [Google Scholar]
- Lentell G., Katzman L., Walters M. (1990) The relationship between muscle function and ankle instability. Journal of Orthopaedic & Sports Physical Therapy 11, 605-611 [DOI] [PubMed] [Google Scholar]
- Munn J., Beard D.J., Refshauge K.M., Lee R.Y. (2003) Eccentric muscle strength in functional ankle instability. Medicine and Science in Sports and Exercise 35, 245-250 [DOI] [PubMed] [Google Scholar]
- Perrin D.H. (1993) Isokinetic exercise and assessment. Champaign, IL: Human Kinetics Publishers [Google Scholar]
- Reinking M.F. (1991) The effect of concentric and eccentric training on the strengthening of tibialis anterior. Isokinetics and Exercise Science 1, 193-210 [Google Scholar]
- Ronkonkoma N.Y. (1995) Cybex Norm Int.Inc: Tesing and Rehabilitation System: Pattern Selection and set up: Automated Protocols; User’s Guide, Blue Sky Software Corporation [Google Scholar]
- Snyder-Mackler L. Fitzgerald G.K. Bartolozzi A.R. Ciccotti M.G (1997) The relationship between passive joint laxity and functional outcome after anterior cruciate ligament injury. American Journal of Sports Medicine 25, 191-195 [DOI] [PubMed] [Google Scholar]
- Tropp H. (1986) Pronator muscle weakness in functional instability of the ankle joint. International Journal of Sports Medicine 7, 291-294 [DOI] [PubMed] [Google Scholar]
- Wester J.U., Jespersen S.M., Nielsen K.D. (1996) Wobble board training after partial sprain of the lateral ligaments of the ankle: a prospective randomized study. Journal of Orthopaedic & Sports Physical Therapy 23, 332-336 [DOI] [PubMed] [Google Scholar]
- Wilkerson G.B., Pinerola J.J., Caturano R.W. (1997) Invertor vs. evertor peak torque and power deficiencies associated with lateral ankle ligament injury. Journal of Orthopaedic & Sports Physical Therapy 26, 78-86 [DOI] [PubMed] [Google Scholar]
- Wong D.L.K., Glasheen-Wray M., Andrews L.F. (1984) Isokinetic evaluation of the ankle invertors and evertors. Journal of Orthopaedic & Sports Physical Therapy 5, 246-252 [DOI] [PubMed] [Google Scholar]
- Wright I.C., Neptune R.R., Bogert A.J., Nigg B.M. (2000) The influence of foot positioning on ankle sprains. Journal of Biomechanics 33, 513-519 [DOI] [PubMed] [Google Scholar]
- WMADH (2000) World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. Journal of the American Medical Association 20, 3043-3045 [PubMed] [Google Scholar]