

Abstract
An estimated 3% of the world population is infected with Hepatitis C virus (HCV), a hepatotropic RNA virus, transmitted primarily via the blood route. The major modes of transmission of the virus include injection drug use, unsafe injection practices, blood transfusion etc. HCV causes chronic hepatitis in about 80% of those infected by it. The mainstay in diagnosing infection with HCV is to initially screen high risk groups for antibodies to HCV (anti-HCV). The inclusion of serum to cut-off ratio (S/CO) in recent guidelines is helpful in deciding the supplemental assay to be used to confirm initially reactive screening results. Nucleic acid amplification tests (NAT) are used as confirmatory tools, and also to determine viral load prior to initiating treatment. Quantitative NAT has replaced qualitative assays. Genotyping is an important tool in clinical management to predict the likelihood of response and determine the optimal duration of therapy. The impact of this infection has begun to emerge in India. The problem of professional blood donation despite an existing law against it, and flourishing unsafe injection practices, are potential sources for the spread of hepatitis C in our country. All health care practitioners need to understand how to establish or exclude a diagnosis of HCV infection and to interpret the tests correctly. In the absence of a preventive or therapeutic vaccine, and also of post-exposure prophylaxis against the virus, it is imperative to diagnose infection by HCV so as to prevent hepatic insult and the ensuing complications that follow, including primary hepatocellular carcinoma (HCC). This review aims to help blood bank staff regarding options for diagnosis and management of donors positive for HCV.
Keywords: Blood borne virus, hepatitis C virus diagnosis, nucleic acid test
Introduction
Hepatitis C virus (HCV) is a hepatotropic virus which is one of the major causes of liver disease and a potential cause of substantial morbidity and mortality worldwide. The virus, estimated to infect about 3% of the world population, is primarily transmitted via the parentral route which includes injection drug use, blood transfusion, unsafe injection practices, and other healthcare related procedures. HCV causes acute hepatitis which is mostly subclinical, but which gradually evolves into chronic hepatitis in about 80% of those infected.[1] HCV infected people are at risk for developing chronic liver disease (CLD), cirrhosis, and primary hepatocellular carcinoma (HCC). It has been estimated that HCV accounts for 27% of cirrhosis and 25% of HCC worldwide.[2] The US Center for Disease Control and Prevention (CDC) recommends screening all individuals with risk factors for HCV infection for antibodies to HCV (anti-HCV), or in specific situations, with molecular assays to demonstrate HCV ribonucleic acid (RNA) by reverse transcriptase polymerase chain reaction (RT-PCR).[3,4] The impact of this infection has begun to emerge in India. The problem of professional blood donation despite an existing law against it, and flourishing unsafe injection practices, are potential sources for the spread of hepatitis C in the country. It is imperative to screen and diagnose HCV infection in high risk populations so that those at risk of progressive liver disease may benefit from antiviral therapy and counseling. All health care practitioners need to understand how to establish or exclude a diagnosis of HCV infection and to interpret the tests correctly. This review aims to give an overview of this emerging viral infection, enumerate the transmission patterns discussing the screening, diagnosis, and interpretation of available assays.
The Virus
In the 1970s, it became apparent that most cases of posttransfusion hepatitis were not attributable to either hepatitis A virus (HAV) or hepatitis B virus (HBV) infection, and a new disease entity, termed “non-A, non-B” hepatitis (NANBH) was described for the first time.[5] It took over a decade to identify the etiological agent of NANBH owing to the inability of the virus to propagate efficiently in cell culture.[6] Finally, HCV was discovered in 1989 and established as an important etiological agent of transfusion associated hepatitis. HCV is a RNA virus belonging to the family Flaviviridae, genus Hepacivirus.[1] The HCV virion is 55-65 nm in diameter containing in it a 9.6 kb positive sense single-stranded RNA genome composed of a long open reading frame (ORF) flanked by untranslated regions (UTR's) at both the ends. The precursor is cleaved into at least 10 different proteins: the structural proteins: Core, E1, E2, and p7; as well as the nonstructural (NS) proteins: NS2, NS3, NS4A, NS4B, NS5A, and NS5B. An important feature of the HCV genome is its high degree of genetic variability. The E1 and E2 regions are the most variable, while the 5’UTR and terminal segment of the 3’UTR are highly conserved.[6] HCV has a high propensity for establishing chronic infection. It has been estimated that in chronically infected people approximately 1012 viral particles are generated every day. This remarkable replicative rate in combination with the highly error prone polymerase activity of the virus results in tremendous genetic diversity and existence of various quasispecies within an infected individual.[6] HCV has been classified into six genotypes[1,2,3,4,5,6] with multiple subtypes. Genotyping is recognized as the primary tool for assessing the course of infection and determining treatment duration and response.[7]
Epidemiology of HCV Infection
Global
The estimated global prevalence of HCV infection is 3% which translates to over 180 million people worldwide. High seroprevalence is observed in Asian and African countries, whereas the developed world including North America, northern and western Europe, and Australia have a low prevalence.[2,6] In developing countries, the seroprevalence of HCV displays a high range of variability, ranging from 0.9% in India to higher prevalence from 2.1-6.5% in many countries. Egypt has a reported seroprevalence of about 22% and is the highest in the world.[2] Substantial regional differences exist in the distribution of HCV genotypes in the world. Genotypes 1, 2, and 3 have a worldwide distribution and HCV subtypes 1a and 1b are the most common genotypes prevalent.[7]
Epidemiology: India
HCV is considered an emerging infection in India. There is a lack of existing literature on the true prevalence in general population due to paucity of well-designed population-based studies from the country. Data available is mostly derived from isolated hospital-based studies and blood banks. The estimates thus obtained have been then extrapolated onto the general population. The estimated HCV prevalence at present is 1-1.9%.[8] Only one systematic study from West Bengal determined a prevalence of 0.87%.[9] The majority of the studies in blood donors report prevalence from 0.3-1.85%. The differences can be due to different generations of the anti-HCV assays used and differences in the population and practices between different regions of the country. Studies in different population groups found varying prevalence rates [Table 1].[10,11,12,13,14,15,16,17,18,19]
Table 1.
HCV prevalence in different population groups
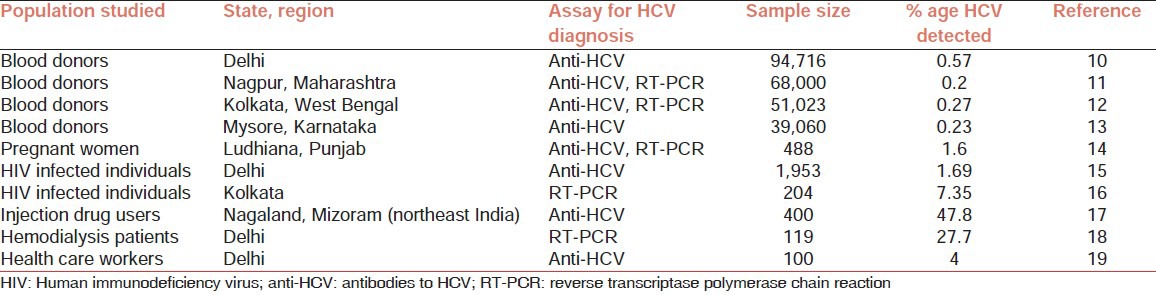
Parenteral transmission through blood transfusion and infected needles and syringes remain the most significant route of transmission for HCV in our country. Blood transfusion is an effective mode of transmission as it allows a large quantum of infective virions into the susceptible patient. In developed countries, numerous corrective measures have reduced the spread of infection through this route. This has been documented in Japan where HCV prevalence dropped from 4.9 to 1.9% after mandatory screening was introduced in 1990, and in the US where the prevalence dropped from 3.84 to 0.57%.[20] In India, mandatory screening for HCV was introduced in 2002. Many of the more recent blood donor studies report prevalence of <1.0%, indicating that increased screening and education of donors is working. Replacement donors typically have higher HCV infection rates than voluntary donors.[21]
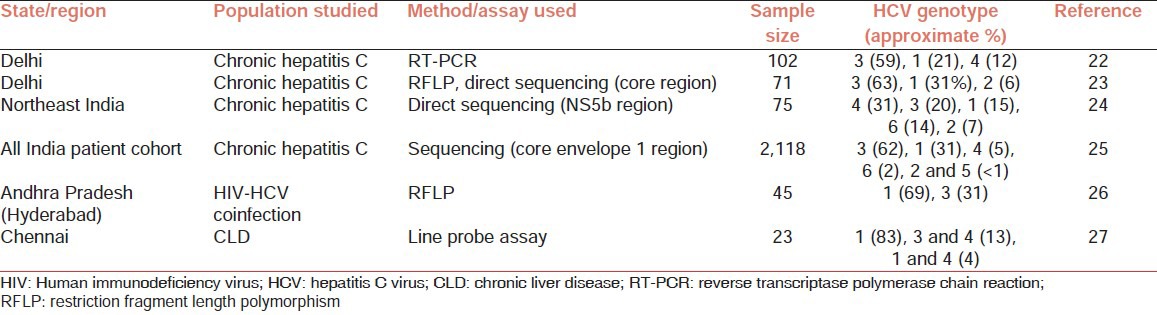
HCV genotypes predominant in India are genotypes 3 and 1, constituting approximately 60 and 30% of the six genotypes, respectively. Genotype 4 constitutes about 4%, the remaining genotypes contributing to <2% each. Most of the reported studies from India have shown that genotype 3 predominates in the north, east, and west India; whereas genotype 1 is commoner in south India. The reason for this difference between these regions is yet to be explained. Various HCV genotypes prevalent across different regions in India, as observed in select recent studies are shown in Table 2.[22,23,24,25,26,27]
Table 2.
HCV genotype distribution in India
Natural history following infection with HCV
Hepatitis C can present as acute or chronic hepatitis. Most of the cases of acute hepatitis C are asymptomatic. Symptomatic acute hepatitis with jaundice is seen in 10-15% of patients only and can be severe, but fulminant liver failure is rare. Spontaneous clearance is observed in 25-50% of those with symptomatic infection and in 10-15% of those with asymptomatic infection.[1,28] The natural history following exposure to HCV is summarized in Figure 1.
Figure 1.
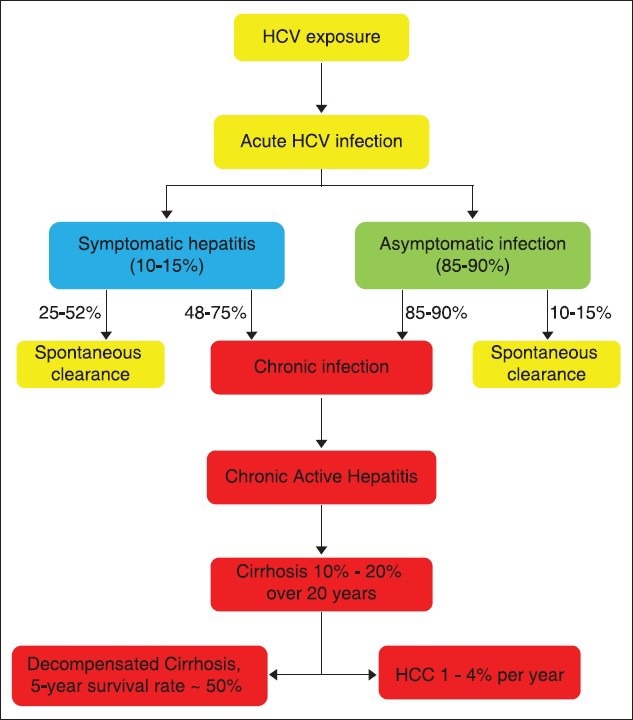
Natural history following infection with hepatitis C virus
Chronic hepatitis C is marked by the persistence of HCV RNA in the blood for at least 6 months after the onset of acute infection. The risk of progression to chronic infection[28] by HCV is influenced by various factors including:
Age at the time of infection (more if infection occurs at age >25 years)
Gender (males > females)
Ethnicity (higher in Africans than in Caucasians and Hispanic whites)
Coinfection with human immunodeficiency virus (HIV), HBV
Concomitant alcohol consumption
Comorbid conditions like cancer, immunosuppression, insulin resistance, nonalcoholic steatohepatitis, obesity, etc.
Treatment for HCV infection
Treatment for HCV infection is available. The role of treatment in acute infection is being evaluated and currently the existing data shows that response to 6 months of standard therapy with interferon (IFN) in terms of absence of HCV RNA from serum is excellent and progression to chronicity is reduced. The recommended treatment for chronic HCV infection is a combination of a pegylated IFN alpha and ribavirin. The treatment duration depends on the genotype of the virus and it has two goals. The first is to achieve sustained eradication of HCV, that is, sustained virologic response (SVR), which is defined as the persistent absence of HCV RNA in serum for 6 months or more after completing antiviral treatment. The second goal is to prevent progression to cirrhosis, HCC, and decompensated liver disease requiring liver transplantation.
Modes of transmission
HCV is transmitted from one person to another principally by parenteral route. The major routes of transmission are:
Injection drug use,
blood transfusion, and
unsafe therapeutic injections.
Other routes of transmissions include;
healthcare related procedures (occupational exposures like needle stick injuries),
tattooing,
perinatal transmission, and
sexual transmission
Transmission through occupational, perinatal, and sexual routes is less efficient as compared to transmission through large or repeated percutaneous exposures. Hence, these routes are not considered to be major sources of new HCV infection regardless of the population or geographic area.[29]
Screening for HCV infection
HCV screening has several potential benefits. By detecting HCV infection early, antiviral treatment can be offered earlier in the course of the disease which is more effective than starting at a later stage.[30] Further, early detection together with counseling and lifestyle modifications may reduce the risk of transmission of HCV infection to other people. The optimal approach to screen for HCV is to test the individuals having risk factors for exposure to the virus. The American Association for the Study of Liver Diseases (AASLD) recommends[4] screening for HCV for the following individuals:
Recipient of blood or blood components (red cells, platelets, fresh frozen plasma).
Recipient of blood from a HCV-positive donor.
Injection drug user (past or present).
-
Persons with following associated conditions;
- persons with HIV infection,
- persons with hemophilia,
- persons who have ever been on hemodialysis, and
- persons with unexplained abnormal aminotransferase levels.
- Children born to HCV-infected mothers.
- Healthcare workers after a needle stick injury or mucosal exposure to HCV-positive blood.
- Current sexual partners of HCV-infected persons.
Risk of HCV infection in recipients of blood transfusion
Prior to 1992, blood transfusions carried a high risk of HCV infection, approximately 15-20% with each unit transfused.[31] In 1988, 90% of cases of posttransfusion hepatitis were due to NANBH viruses which was later found out to be due to HCV. The move to all-volunteer blood donors instead of paid donors had significantly reduced the risk of posttransfusion hepatitis to 10%. Screening of blood further reduced the rate of posttransfusion hepatitis C by a factor of about 10,000; to a current rate of 1 per million transfusions.[32] The few cases that still occur are due to newly infected people donating blood before they have developed antibodies (window period) to the virus, which can take up to 6-8 weeks.
Virological Tools for Diagnosis
Virological diagnosis of HCV infection is based on two categories of laboratory tests, namely serologic assays detecting specific antibody to HCV (anti-HCV) (indirect tests) and assays that can detect, quantify, or characterize the components of HCV viral particles, such as HCV RNA and core antigen (direct tests). Direct and indirect virological tests play a key role in the diagnosis of infection, therapeutic decision-making, and assessment of virological response to therapy.
Anti-HCV Antibodies
The “serologic window” between HCV infection and the detection of specific antibodies varies from patient to patient. With current assays, seroconversion occurs on an average at 6-8 weeks after the onset of infection. In patients with spontaneously resolving infection, anti-HCV may persist throughout life, or decrease slightly while remaining detectable, or gradually disappear after several years.[33] Anti-HCV persists indefinitely in patients who develop chronic infection, although antibodies may become undetectable in hemodialysis patients or in cases of profound immunosuppression.
Anti-HCV detection
Serological assays for detecting anti-HCV were developed and improved following the initial discovery of the virus because of the urgent need to screen blood donors and prevent transmission. Anti-HCV is typically identified by using enzyme-linked immunosorbent assay (ELISA). Three generations of ELISAs [Table 3] have been developed since 1989. The first generation assays, which incorporated the recombinant c100-3 epitope from the NS4 region, were used until 1992, when they were replaced by second generation assays, which additionally incorporated epitopes c22-3 and c33c from the HCV core and NS3 regions, respectively. The third generation assays contained reconfigured core and NS3 antigens and in addition a newly incorporated antigen from the NS5 region.[34,35,36]
Table 3.
The different generations of immunoassays for anti-HCV

The window period has been documented to decrease from approximately 16 weeks to 10 weeks and finally to 8 weeks with the introduction of first-, second-, and third-generation anti-HCV ELISAs, respectively. The newest generation of immunoassays available, that is, fourth generation of tests is those that simultaneously detect HCV capsid antigen as well as antibodies to the core, NS3, NS4, and NS5 regions of the virus. These assays have further reduced the window period of HCV detection by 17 days to already existing assays. But the literature supporting the inclusion of these assays as 4th generation on the basis of improved sensitivity, specificity is limited.[1,36]
Supplemental anti-HCV test and significance of signal-to-cut off (S/CO) ratio
Recombinant immunoblot assays (RIBA) were used in the past as supplemental assays to confirm serological reactivity by ELISA, but are now clinically obsolete with the availability of molecular tests.[37] Confirmation of serological reactive tests may be done by a nucleic acid test (NAT) for detection of HCV RNA. Recent studies have also suggested that higher the anti-HCV antibody titer in patient's serum; more are the chances of it being true positive than false positive. This was the basis of inclusion of measurement of anti-HCV S/CO ratio that indirectly represents higher antibody levels in patient's sample, as a marker for confirmation of serological reactive results. CDC in 2003 expanded the earlier guidelines to recommend an option for inclusion of S/CO ratio to determine the need for supplementary testing.[38]
This was based on the analysis of many thousands of repeatedly reactive samples screened for anti-HCV, and their results compared to those generated by a supplemental assay. It was estimated that for ELISA, a S/CO of 3.8, and for chemiluminescence immunoassay (CLIA) a S/CO of 8, predicted true viremia in 95-98% cases. Since then, various studies have also confirmed the usefulness of S/CO in predicting true positive anti-HCV results.[1,39,40,41] This should be limited to only diagnostic tests as this criteria does not hold true for screening assays.
HCV core antigen (HCV Ag) detection
During the past decade, several assays for the detection of the core antigen of HCV by ELISA or CLIA have been developed.[42] These assays were envisioned as alternatives to NAT to be used in resource-limited settings, where molecular laboratory services are either not available or not widely utilized owing to cost issues. Since these assays are either ELISA or CLIA based, they are user friendly, require less technical expertise and are less expensive compared to molecular techniques. Evaluations in transfusion settings have shown that the HCVcore Ag assay detects HCV infection as effective as NAT, about 40-50 days earlier than the current third generation anti-HCV screening assays. HCV core antigen levels closely follow HCV RNA dynamics, and allow clinical monitoring of a patient's therapy, independently of HCV genotype.[42,43] The major limitation of the HCV core Ag assay is its lower sensitivity limiting its utility. A new generation CLIA based quantitative test (Architect HCV Ag Test, Abbot, Germany) with sensitivity comparable to that of end point PCR (~1,000 IU/ml) but less than that of real time RT-PCR has been reported.[44,45]
NAT: Detection of HCV RNA
Molecular virological techniques play a key role in diagnosis and monitoring of treatment for HCV. Because it is difficult to cultivate the virus in cell culture, molecular techniques were instrumental in first identifying HCV, making it one of the first pathogens to be identified by purely molecular methods. NAT is considered the ‘gold standard’ for detecting active HCV replication. HCV NAT is extremely useful in establishing the diagnosis of acute HCV infection, since RNA is detectable as early as 1 week after exposure via needle-stick or blood transfusion, and at least 4-6 weeks prior to seroconversion as demonstrated in a number of transmission settings.[46,47,48] The diagnosis of HCV infection is established with antibody screening followed by NAT for HCV RNA for confirmation as well as for follow-up of patients on treatment.[1] Viral load assessment at baseline is also critical for determining response kinetics during therapy. Table 4 enumerates the role of NAT in HCV diagnosis.
Table 4.
Role of NAT in HCV diagnosis

Qualitative NAT
Qualitative NAT have traditionally been considered as confirmatory tools for HCV diagnosis. These assays commonly utilize conventional RT-PCR or transcription-mediated amplification (TMA). The present indication of qualitative NAT is to confirm viremia (especially low level viremia) in patients with reactive anti-HCV results, and to screen blood donations for evidence of infection with HCV.[1,49] With the availability of more sensitive quantitative PCR that has a lower limit of detection (LOD) to as low as 30 copies/ml, qualitative assays have taken a back seat especially in diagnostic laboratories.
Quantitative NAT
Quantification of HCV RNA can be accomplished by many methods. Commonly available formats include quantitative RT-PCR (qRT-PCR) and branched deoxyribonucleic acid (bDNA) technology. Table 5 summarizes currently available quantitative NAT's for HCV.
Table 5.
Commercial HCV RNA quantification tests (RUO, Research use only; ASR, Analyte-specific reagents). Data collected from the manufacturer's website

Owing to its good sensitivity (99%) and specificity (98-99%) quantitative PCR has replaced qualitative PCR.[4,49] Prior to 1997, the interpretation of quantitative NAT was hampered by the use of individual reporting units that were specific to individual assays. In response to this, WHO established a preparation of HCV to be used as a globally recognized standard for calibration of quantitative assays.[1] For monitoring purposes, it is important to use the same assay before and throughout during therapy.[4,49]
Iatrogenic exposure and postexposure prophylaxis
The potential of health care delivery to transmit HCV to healthcare worker (HCW) is increasingly being recognized especially if infection control or disinfection practices are inadequate and contaminated equipment is shared among patients. The mechanisms of transmission in the healthcare setting are related to:[50]
Improperly cleaned, disinfected, or sterilized equipment
Medication administration (e.g., direct syringe reuse, contamination of medication through syringe reuse, etc.)
Blood sampling
The CDC in collaboration with healthcare infection control practices advisory committee (HICPAC) has issued recommendations following occupational exposure to HCV.[51,52,53] These recommendations emphasize that each institution should have its own policy regarding follow-up of personnel who sustain percutaneous or permucosal exposure to suspected HCV infected blood. They minimally recommend:
Baseline testing for anti-HCV in source.
Baseline and follow-up testing for anti-HCV and alanine aminotransferase (ALT) levels in exposed at 6 months and 1 year postexposure.
Confirmation by NAT of all anti-HCV reactive results.
Education of workers about the risk for and prevention of blood-borne infections.
Blood Transfusion Issues and Donor Counseling
Guidelines for donor notification for donors positive for transfusion transmissible infections (TTIs) are outlined in ‘An Action Plan for Blood Safety’ by National AIDS Control Organization (NACO) 2004.[54] A blood donor is offered an option to know his TTI status at the time of registration for blood donation after due counseling and give consent for the same.
Notifying donors regarding a single positive screening test is fraught with the risk of causing undue anxiety and stress to a donor. If a screening test is positive, the blood unit should be immediately discarded. Presently there are no guidelines regarding confirming the test results before informing the donor. In case of samples with low S/CO and grey zone samples, a retesting of the donor samples using a different assay would be imperative before notifying the donor. There are clear cut guidelines regarding donor notification and referral for HIV positive blood donors with ‘integrated counseling and testing centers’ available for the same. Donors who are positive for viral hepatitis markers have to be counseled by blood bank staff. An algorithm for donor counseling for HCV positive donors is outlined in Figure 2.
Figure 2.
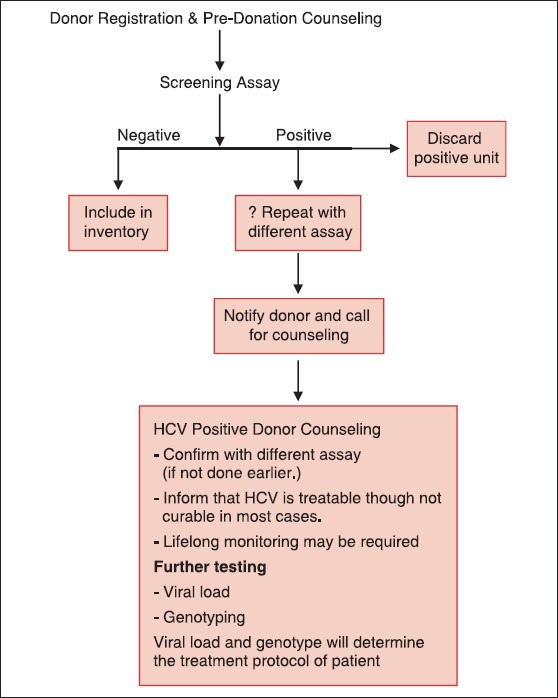
Algorithm for donor counseling for HCV positive donors
Looking Further: HCV Vaccines
Vaccine development for HCV is currently one of the most challenging fields in virology today. Various obstacles that hinder the development[55,56] of an effective preventive or therapeutic vaccine for HCV include:
Considerable genetic heterogeneity of isolates within and between geographic locales (six genotypes, >100 subtypes).
Evolution and existence of quasispecies in an individual (especially HVR1 of E2 gene).
Poorly defined immunological correlates of protection.
Lack of efficient in vitro propagation (robust cell culture system/small animal models) to isolate the virus.
Despite these obstacles, both preventive as well as therapeutic vaccines for HCV are under development and also under various phases of vaccine trials,[55] but a successful vaccine remains to be developed.
Footnotes
Source of Support: Nil
Conflicting Interest: None declared.
References
- 1.Forman MS, Valsamakis A. Hepatitis C virus. In: Versalovic J, Carrol KC, Funke G, Jorgensen JH, Landry ML, Warrock DW, editors. Murray's Manual of Clinical Microbiology. 10th ed. Washington: American Society of Microbiology Press; 2011. pp. 1437–55. [Google Scholar]
- 2.Alter MJ. Epidemiology of hepatitis C virus infection. World J Gastroenterol. 2007;13:2436–41. doi: 10.3748/wjg.v13.i17.2436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Alter MJ, Seeff LB, Bacon BR, Thomas DL, Rigsby MO, Di Bisceglie AM. Testing for hepatitis C virus infection should be routine for persons at increased risk for infection. Ann Intern Med. 2004;141:715–7. doi: 10.7326/0003-4819-141-9-200411020-00013. [DOI] [PubMed] [Google Scholar]
- 4.Ghany MG, Strader DB, Thomas DL, Seeff LB. American association for the study of liver diseases. Diagnosis, management, and treatment of hepatitis C: An update. Hepatology. 2009;49:1335–74. doi: 10.1002/hep.22759. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Feinstone SM, Kapikian AZ, Purcell RH, Alter HJ, Holland PV. Transfusion-associated hepatitis not due to viral hepatitis type A or B. N Engl J Med. 1975;292:767–70. doi: 10.1056/NEJM197504102921502. [DOI] [PubMed] [Google Scholar]
- 6.Lemon SM, Walker C, Alter MJ, Min Kyung Y. Hepatitis C virus. In: Knipe DM, Hpwley PM, editors. Field's Virology. 5th ed. Netherlands, Philadelphia: Wolters Kluwer, Lippincott Williams & Wilkins; 2007. pp. 1253–304. [Google Scholar]
- 7.Zein NN. Clinical significance of hepatitis C genotypes. Clin Microbiol Rev. 2000;13:223–35. doi: 10.1128/cmr.13.2.223-235.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mukhopadhya A. Hepatitis C in India. J Biosci. 2008;33:465–73. doi: 10.1007/s12038-008-0065-0. [DOI] [PubMed] [Google Scholar]
- 9.Nayak NC, Jain D, Vasdev N, Gulwani H, Saigal S, Soin A. Etiologic types of end-stage chronic liver disease in adults: Analysis of prevalence and their temporal changes from a study on native liver explants. Eur J Gastroenterol Hepatol. 2012;24:1199–208. doi: 10.1097/MEG.0b013e32835643f1. [DOI] [PubMed] [Google Scholar]
- 10.Meena M, Jindal T, Hazarika A. Prevalence of hepatitis B virus and hepatitis C virus among blood donors at a tertiary care hospital in India: A five-year study. Transfusion. 2011;51:198–202. doi: 10.1111/j.1537-2995.2010.02801.x. [DOI] [PubMed] [Google Scholar]
- 11.Tulsiani S, Choudhury N, Desai P, Shah R, Mathur A, Harimoorthy V, et al. True positivity of anti-Hepatitis C Virus Enzyme-linked immunosorbent assay reactive blood donors: A prospective study done in western India. Asian J Transfus Sci. 2012;6:165–8. doi: 10.4103/0973-6247.98927. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Choudhury N, Tulsiani S, Desai P, Shah R, Mathur A, Harimoorthy V. Serial follow-up of repeat voluntary blood donors reactive for anti-HCV ELISA. Asian J Transfus Sci. 2011;5:26–31. doi: 10.4103/0973-6247.75979. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Pallavi P, Ganesh CK, Jayashree K, Manjunath GV. Seroprevalence and trends in transfusion transmitted infections among blood donors in a university hospital blood bank: A 5 year study. Indian J Hematol Blood Transfus. 2011;27:1–6. doi: 10.1007/s12288-010-0047-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Sood A, Midha V, Bansal M, Sood N, Puri S, Thara A. Perinatal transmission of hepatitis C virus in northern India. Indian J Gastroenterol. 2012;31:27–9. doi: 10.1007/s12664-012-0163-7. [DOI] [PubMed] [Google Scholar]
- 15.Raizada A, Dwivedi S, Bhattacharya S. Hepatitis B, Hepatitis C and HIV co-infection at an antiretroviral centre in Delhi. Trop Doct. 2011;41:154–6. doi: 10.1258/td.2011.100440. [DOI] [PubMed] [Google Scholar]
- 16.Saha K, Firdaus R, Santra P, Pal J, Roy A, Bhattacharya MK, et al. Recent pattern of co-infection amongst HIV sero-positive individuals in a tertiary care hospital, Kolkata. Virol J. 2011;8:116. doi: 10.1186/1743-422X-8-116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Mahanta J, Borkakoty B, Das HK, Chelleng PK. The risk of HIV and HCV infections among injection drug users in northeast India. AIDS Care. 2009;21:1420–4. doi: 10.1080/09540120902862584. [DOI] [PubMed] [Google Scholar]
- 18.Jasuja S, Gupta AK, Choudhry R, Kher V, Aggarwal DK, Mishra A, et al. Prevalence and associations of hepatitis C viremia in hemodialysis patients at a tertiary care hospital. Indian J Nephrol. 2009;19:62–7. doi: 10.4103/0971-4065.53324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Jindal N, Jindal M, Jilani N, Kar P. Seroprevalence of hepatitis C virus (HCV) in health care workers of a tertiary care centre in New Delhi. Indian J Med Res. 2006;123:179–80. [PubMed] [Google Scholar]
- 20.Donahue JG, Muñoz A, Ness PM, Brown DE, Jr, Yawn DH, McAllister HA, Jr, et al. The declining risk of post-transfusion hepatitis C virus infection. N Engl J Med. 1992;327:369–73. doi: 10.1056/NEJM199208063270601. [DOI] [PubMed] [Google Scholar]
- 21.Thakral B, Marwaha N, Chawla YK, Saluja K, Sharma A, Sharma RR, et al. Prevalence and significance of hepatitis C (HCV) seropositivity in blood donors. Indian J Med Res. 2006;124:431–8. [PubMed] [Google Scholar]
- 22.Rehan HS, Manak S, Yadav M, Deepinder, Chopra D, Wardhan N. Diversity of genotype and mode of spread of Hepatitis C virus in Northern India. Saudi J Gastroenterol. 2011;17:241–4. doi: 10.4103/1319-3767.82576. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chakravarti A, Dogra G, Verma V, Srivastava AP. Distribution pattern of HCV genotypes and its association with viral load. Indian J Med Res. 2011;133:326–31. [PMC free article] [PubMed] [Google Scholar]
- 24.Medhi S, Goswami B, Das AK, Singh TB, Husain SA, Sehgal A, et al. New insights into hepatitis C virus infection in the tribal-dominant part of Northeast India. Arch Virol. 2012;157:2083–93. doi: 10.1007/s00705-012-1374-z. [DOI] [PubMed] [Google Scholar]
- 25.Narahari S, Juwle A, Basak S, Saranath D. Prevalence and geographic distribution of hepatitis C genotypes in Indian patient cohort. Infect Genet Evol. 2009;9:643–5. doi: 10.1016/j.meegid.2009.04.001. [DOI] [PubMed] [Google Scholar]
- 26.Ponamgi SP, Rahamathulla S, Kumar YN, Chandra M, Lakshmi N, Habibullah CM, et al. Prevalence of hepatitis C virus (HCV) coinfection in HIV inected individuals in south India and characterization of HCV genotypes. Indian J Med Microbiol. 2009;27:12–6. [PubMed] [Google Scholar]
- 27.Saravanan S, Velu V, Kumarasamy N, Shankar EM, Nandakumar S, Murugavel KG, et al. The prevalence of hepatitis B and hepatitis C virus infection among patients with chronic liver disease in south India. Int J Infect Dis. 2008;12:513–8. doi: 10.1016/j.ijid.2008.02.006. [DOI] [PubMed] [Google Scholar]
- 28.Chen SL, Morgan TR. The natural history of hepatitis C (HCV) infection. Int J Med Sci. 2006;3:47–52. doi: 10.7150/ijms.3.47. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Shepard CW, Finelli L, Alter MJ. Global epidemiology of hepatitis C virus infection. Lancet Infect Dis. 2005;5:558–67. doi: 10.1016/S1473-3099(05)70216-4. [DOI] [PubMed] [Google Scholar]
- 30.Hayashi N, Takehara T. Antiviral therapy for chronic hepatitis C: Past, present, and future. J Gastroenterol. 2006;41:17–27. doi: 10.1007/s00535-005-1740-7. [DOI] [PubMed] [Google Scholar]
- 31.Alter MJ, Hadler SC, Judson FN, Mares A, Alexander WJ, Hu PY, et al. Risk factors for acute non-A, non-B hepatitis in the United States and association with hepatitis C virus infection. JAMA. 1990;264:2231–5. [PubMed] [Google Scholar]
- 32.Blajchman MA, Vamvakas EC. The continuing risk of transfusion-transmitted infections. N Engl J Med. 2006;355:1303–5. doi: 10.1056/NEJMp068178. [DOI] [PubMed] [Google Scholar]
- 33.Lefrere JJ, Guiramand S, Lefrere F, Mariotti M, Aumont P, Lerable J, et al. Full or partial seroreversion in patients infected by hepatitis C virus. J Infect Dis. 1997;175:316–22. doi: 10.1093/infdis/175.2.316. [DOI] [PubMed] [Google Scholar]
- 34.Barrera JM, Franscis B, Ercilla G, Nelles M, Archod D, Darner J, et al. Improved detection of Anti-HCV in Post transfusion Hepatitis by third generation ELISA. Vox Sang. 1995;68:15–8. doi: 10.1111/j.1423-0410.1995.tb02538.x. [DOI] [PubMed] [Google Scholar]
- 35.Morishima C, Gretch DR. Clinical use of Hepatitis C virus test for the diagnosis and monitoring during therapy. Clin Liver Dis. 1999;3:717–40. doi: 10.1016/s1089-3261(05)70235-x. [DOI] [PubMed] [Google Scholar]
- 36.Colin C, Lanoir D, Touzet S, Meyoud-Kraemer L, Bailley F, Trepo C HEPATITIS Group. Sensitivity and specificity of third-generation hepatitis C virus antibody detection assays: An analysis of the literature. J Viral Hepat. 2001;8:87–95. doi: 10.1046/j.1365-2893.2001.00280.x. [DOI] [PubMed] [Google Scholar]
- 37.Dow BC, Buchanan I, Munro H, Follet EA, Davidson F, Presscot LE, et al. Relevance of RIBA-3 supplementary test to HCV PCR positivity and genotypes for HCV confirmation of blood blood donors. J Med Virol. 1996;49:132–6. doi: 10.1002/(SICI)1096-9071(199606)49:2<132::AID-JMV10>3.0.CO;2-G. [DOI] [PubMed] [Google Scholar]
- 38.Recommendations for prevention and control of hepatitis C (HCV) infection and HCV-related chronic disease. Centres for Disease Control and Prevention. MMWR Recomm Rep. 1998;47:1–39. [PubMed] [Google Scholar]
- 39.Kim S, Kim JH, Yoon S, Park YH, Kim HS. Clinical performance evaluation of four automated chemiluminescence immunoassays for hepatitis C virus antibody detection. J Clin Microbiol. 2008;46:3919–23. doi: 10.1128/JCM.01603-08. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Ren RF, Lv QS, Zhuang H, Li JJ, Gong XY, Gao GJ, et al. Significance of the signal-to-cutoff ratios of anti-hepatitis C enzyme immunoassays in screening of Chinese blood donors. Transfusion. 2005;45:1816–22. doi: 10.1111/j.1537-2995.2005.00611.x. [DOI] [PubMed] [Google Scholar]
- 41.Oethinger M, Mayo DR, Falcone J, Barua PK, Griffith BP. Efficiency of the Ortho VITROS Assay for the detection of hepatitis C virus-specific antibodies increased by elimination of supplemental testing of samples with very low sample-to-cutoff ratios. J Clin Microbiol. 2005;43:2477–80. doi: 10.1128/JCM.43.5.2477-2480.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Seme K, Poljak M, Babic DZ, Mocilnik T, Vince A. The role of core antigen detection in management of hepatitis C: A critical review. J Clin Virol. 2005;32:92–101. doi: 10.1016/j.jcv.2004.10.005. [DOI] [PubMed] [Google Scholar]
- 43.Gaudy C, Thevenas C, Tichet J, Mariotte N, Goudeau A, Dubois F. Usefulness of the hepatitis C core antigen assay for screening a population undergoing routine medical checkup. J Clin Chem. 2005;43:1722–6. doi: 10.1128/JCM.43.4.1722-1726.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Morota K, Fujinami R, Kinukawa H, Machida T, Ohno K, Saegusa H, et al. A new sensitive and automated chemiluminescent microparticle immunoassay for quantitative determination of hepatitis C virus core antigen. J Virol Methods. 2009;157:8–14. doi: 10.1016/j.jviromet.2008.12.009. [DOI] [PubMed] [Google Scholar]
- 45.Kesli R, Polat H, Terzi Y, Kortoglu MG, Uyar Y. Comparison of a newly developed automated and quantitative hepatitis C virus (HCV) core antigen test with the HCV RNA assay for clinical usefulness in confirming Anti-HCV results. J Clin Microbiol. 2011;49:4089–93. doi: 10.1128/JCM.05292-11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Maheshwari A, Ray S, Thuluvath PJ. Acute hepatitis C infection. Lancet. 2008;372:321–32. doi: 10.1016/S0140-6736(08)61116-2. [DOI] [PubMed] [Google Scholar]
- 47.Glenn SA, Wright DJ, Klienman SH, Hirschkorn D, Tu Y, Helderbrant C, et al. Dynamics of viremia in early hepatitis C virus infection. Transfusion. 2005;45:994–1002. doi: 10.1111/j.1537-2995.2005.04390.x. [DOI] [PubMed] [Google Scholar]
- 48.Kamal SM. Acute hepatitis C: A systematic review. Am J Gastroenterol. 2008;103:1283–97. doi: 10.1111/j.1572-0241.2008.01825.x. [DOI] [PubMed] [Google Scholar]
- 49.Scott JD, Gretch DR. Molecular diagnostics of hepatitis C virus infection: A systematic review. JAMA. 2007;297:724–32. doi: 10.1001/jama.297.7.724. [DOI] [PubMed] [Google Scholar]
- 50.World Health Organization; 2009. Screening donated blood for transfusion-transmissible infections: Recommendations. [PubMed] [Google Scholar]
- 51.Panlilo AL, Schaefer MK, Thompson ND. Hepatitis viruses. In: Mayhall CG, editor. Hospital Epidemiology and Infection Control. 4th ed. Philadelphia: Lippincott Williams and Wilkins; 2012. pp. 662–74. [Google Scholar]
- 52.Centers for Disease Control and Prevention (CDC). Recommendations for follow-up of health-care workers after occupational exposure to hepatitis C virus. MMWR Morb Mortal Wkly Rep. 1997;46:603–6. [PubMed] [Google Scholar]
- 53.Atlanta, Georgia: US Department of Health and Human Services; 1995. Centers for Disease Control and Prevention. Risk of acquiring hepatitis C for health care workers and recommendations for prophylaxis and follow-up after occupational exposure. Hepatitis surveillance Report no. 56; pp. 3–6. [Google Scholar]
- 54.New Delhi: Ministry of Health and Family Welfare, Government of India; 2004. National AIDS Control Organization. An action plan for blood safety; pp. 33–7. [Google Scholar]
- 55.Strickland GT, El-Kamary SS, Klenerman P, Nicosia A. Hepatitis C vaccine: Supply and demand. Lancet Infect Dis. 2008;8:379–86. doi: 10.1016/S1473-3099(08)70126-9. [DOI] [PubMed] [Google Scholar]
- 56.Yu CI, Chiang BL. A new insight into Hepatitis C vaccine development. J Biomed Biotechnol 2010. 2010 doi: 10.1155/2010/548280. 548280. [DOI] [PMC free article] [PubMed] [Google Scholar]