

Abstract
A specific prognostication score for hepatitis C virus-positive diffuse large B-cell lymphomas is not available. For this purpose, the Fondazione Italiana Linfomi (FIL, Italian Lymphoma Foundation) carried out a multicenter retrospective study on a large consecutive series of patients with hepatitis C virus-associated diffuse large B-cell lymphoma to evaluate the prognostic impact of clinical and virological features and to develop a specific prognostic score for this subset of patients. All prognostic evaluations were performed on 535 patients treated with an anthracycline-based induction regimen (with rituximab in 255 cases). Severe hepatotoxicity was observed in 14% of patients. The use of rituximab was not associated with increased rate of severe hepatotoxicity. Three-year overall survival and progression-free survival were 71% and 55%, respectively. At multivariate analysis, ECOG performance status of 2 or over, serum albumin below 3.5 g/dL and HCV-RNA viral load over 1000 KIU/mL retained prognostic significance. We combined these 3 factors in a new “HCV Prognostic Score” able to discriminate 3 risk categories with different overall and progression-free survival (low=0; intermediate=1; high-risk ≥2 factors; P<0.001). This score retained prognostic value in the subgroups of patients treated with and without rituximab (P<0.001). The new score performed better than the International Prognostic Index at multivariate analysis and Harrel C-statistic. With the use of three readily available factors (performance status, albumin level and HCV-RNA viral load), the new “HCV Prognostic Score” is able to identify 3 risk categories with different survival, and may be a useful tool to predict the outcome of hepatitis C virus-associated diffuse large B-cell lymphomas.
Introduction
In recent years, many epidemiological studies have increasingly strengthened the evidence that hepatitis C virus (HCV) is associated not only with indolent B-cell non-Hodgkin lymphomas (NHL), but also with diffuse large B-cell lymphomas (DLBCL).1 An Italian case-control study reported an even higher association of HCV infection with DLBCL (Odds Ratio (OR) 3.5) with respect to indolent NHL (OR 2.3), suggesting that approximately one out of 20 cases of DLBCL, at least in Italy, may be attributable to HCV.2 Unlike indolent B-NHL, there seems to be no role for antiviral treatment in HCV-positive DLBCL, because lymphoma cells, suffering from additional oncogenic lesions, may not be critically dependent on antigen stimulation. For this reason, unlike their indolent counterpart, HCV-associated DLBCL patients should be treated with conventional immunochemotherapy schemes such as R-CHOP, although concerns remain with regard to the potential risk of hepatotoxicity.3
The prediction of the prognosis in HCV-positive DLBCL is still a subject for debate. In fact, as previously reported,4,5 HCV-positive DLBCL patients display specific presentation features with respect to their HCV-negative counterparts, potentially affecting many clinical features included in common prognostic scores (i.e. age, number of extranodal sites, stage). Moreover, many laboratory parameters of common prognostic significance (i.e. LDH, blood cell counts) are potentially biased as they are influenced not only by lymphoma but also by chronic HCV infection. Notably, common prognostic indexes for DLBCL (the IPI6 or its variant the R-IPI7) were created and validated in series made up of only HCV-negative patients or with unknown HCV-status, while their predictive significance has never been formally validated in HCV-positive DLBCL.
For these reasons, the Fondazione Italiana Linfomi (FIL, Italian Lymphoma Foundation) carried out a large multi-center retrospective study on a large series of patients affected by DLBCL associated with HCV infection, with the aim of constructing a new prognostic system for HCV-associated DLBCL.
Methods
Patients
We collected data of patients with DLBCL positive for HCV serology who were consecutively diagnosed and treated between 1995 and 2010 at 16 Italian major hematologic institutions belonging to the FIL (known before 2012 as the Intergruppo Italiano Linfomi, IIL). HIV-positive cases were excluded. HCV infection is a big health problem in Italy and the majority of patients with NHL are evaluated for HCV infection. HCV-positive cases made up 17% of all registered cases of DLBCL with available HCV serology from participating centers. HCV serology was not available for 20% of all diagnosed cases in the period examined. We identified 625 DLBCL patients with positive HCV serology. Of these, 535 received a curative-intent anthracycline-containing treatment (with or without rituximab), while 77 were managed with other palliative-intent strategies. To minimize bias due to the heterogeneity of treatments, we restricted our prognostic analyses to the 535 patients treated with curative-intent modality, reporting separately data about the remaining patients. Approval for this retrospective study, based on archive data, was obtained from the Institutional Ethics Committee. Data management and analysis were performed in accordance with the Helsinki Declaration of 1975, revised in 1983 and 2000.
Statistical analysis
Numeric variables were summarized by their median and range. Categorical variables were described by counts and relative frequencies. Association between categorical variables was tested via Fisher exact test for 2 × 2 tables or using the χ2 approximation for larger tables, while the differences in mean values between two groups were evaluated using a t-test for independent data. The Kaplan-Meier product-limit method was used to estimate survival curves, and the log rank test was adopted to evaluate the differences between different groups of patients. Backward stepwise multivariate Cox regression analysis was then applied by checking the applicability assumption to determine the influence of the variables on the overall survival (OS), progression-free survival (PFS) and disease-specific survival (DSS). The limit of significance for all analyses was defined as P<0.05. All variables associated with significant P values in multivariate analysis were then included in the computation of the prognostic model. Because hazard ratios (HRs) of risk factors identified at multivariate analysis were of comparable magnitude, all factors were given the same weight; the presence of a risk factor contributed to the score with an increment of 1. Because of the small number of patients, those with 2 or 3 risk factors were grouped in the highest risk group. Furthermore, the prognostic analysis was performed after randomly splitting the study population into two parts: two-thirds (testing sample) and one-third (validation sample). Finally, the prognostic model was internally validated in the subgroups of patients treated with either R-CHOP or CHOP. To evaluate the discriminative ability of the model, the Harrell C-statistic with 95% confidence interval was determined.
Details about HCV-infection status, hepatic evaluation, definition of hepatotoxicity, treatments, response criteria and prognostic variables are available in the Online Supplementary Appendix.
Results
Patients’ characteristics
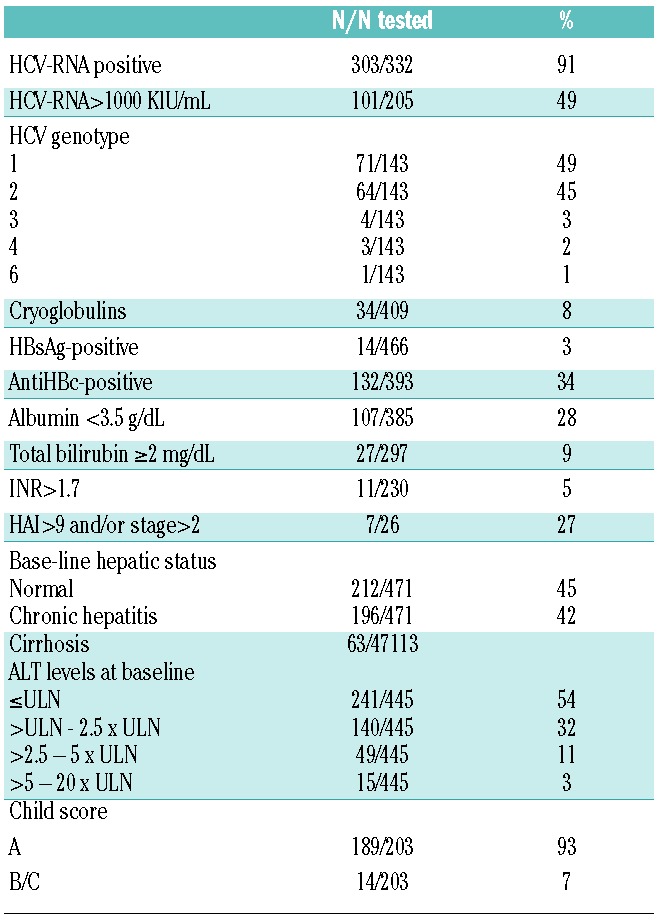
Clinical characteristics and virological features of the 535 patients treated with curative-intent modality are summarized in Tables 1 and 2. Median age was 67 years (range 18–88 years). HCV-RNA status was available in 332 cases: 303 (91%) were HCV-RNA positive. Only a few patients had detectable serum cryoglobulins (34 of 409, 8%), with a median cryocrit value of 3%, and only a fraction of them were symptomatic (9 of 34, 26%). Based on laboratory and imaging findings, 42% and 13% of patients were known to have chronic hepatitis and liver cirrhosis, respectively. Baseline hepatic biopsy was available in 26 cases; 7 (27%) samples not involved by DLBCL showed advanced inflammatory activity (HAI >9) and/or advanced fibrosis (stage >2). Hepatocellular carcinoma (HCC) was detected in 3 patients before treatment while another 4 patients developed it during the course of therapy. Among a subgroup of patients with available data (n=132), HCV infection was known before the diagnosis of DLBCL in 80% of cases (n=105), while it was detected as part of initial investigations for lymphoma in 20% (n=27). Within this subset of patients, liver cirrhosis was slightly more prevalent in patients with previously known HCV infection (28% vs. 12%; P=0.1). Comparison between base-line characteristics of patients treated with curative- and palliative-intent modality is shown in the Online Supplementary Table S1.
Table 1.
Clinical characteristics of 535 patients with HCV-positive DLBCL treated with curative-intent therapy.
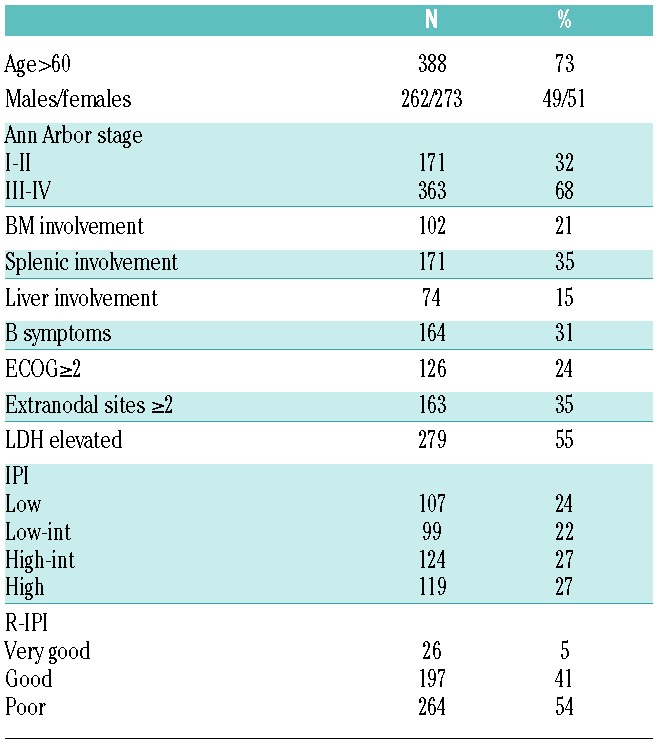
Table 2.
Virological features of 535 patients with HCV-positive DLBCL treated with curative-intent therapy.
Treatments
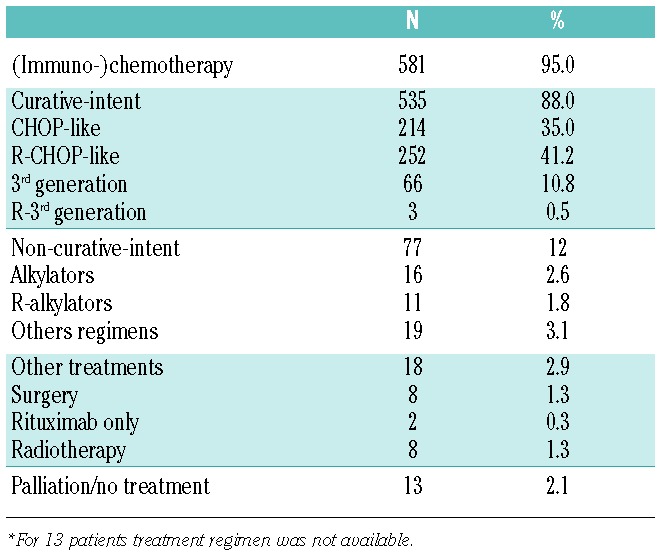
First-line treatments are summarized in Table 3. Overall, 535 patients received a curative-intent anthracycline-containing regimen (88%), with rituximab addition in 255 (42%). In detail, 214 patients (40%) received CHOP-like therapy, 252 (47%) R-CHOP-like, while the remaining 69 (13%) patients were treated with 3rd generation treatments (in 3 cases with rituximab). Seventy-seven patients were managed with other options with non-curative intent (palliative chemotherapy, surgery, radiotherapy, rituximab monotherapy, steroids or observation) and were excluded from the analyses together with 13 patients for whom treatment data were not available. During treatment, cytotoxic drug doses were reduced in 39% of patients (median dose reduction 33%, range 10–75%). Steroids were reduced or stopped in 65 patients (18%) (in 33 for hepatotoxicity). Eighty-three patients (20%) did not complete the planned treatment (30 for progression, 13 for liver toxicity, 40 for other causes). Overall, 69% of patients achieved CR and 16% PR (ORR 85%) while 15% did not respond or progressed.
Table 3.
Treatment regimen in 612 patients with HCV-positive DLBCL.*
Hepatotoxicity
Pre-treatment transaminase levels were normal in 241 (54%) and elevated in 204 (46%) patients (Table 2). Of the 432 evaluable patients, 61 (14%) experienced severe hepatotoxicity (55 patients grade 3 and 6 patients grade 4). Base-line elevated ALT resulted significantly associated with severe hepatotoxicity (P<0.001). The use of rituximab was not associated with increased rate of severe hepatotoxicity (14% with CHOP vs. 16% with R-CHOP; P=0.6). Among patients experiencing severe hepatotoxicity, chemotherapy was stopped in 16 cases (28%), including 3 patients who died because of disease progression and one patient in complete response who died because of liver failure. Sixteen out of 61 patients who developed severe hepatotoxicity had positive HBV serology (1 HBsAg-positive and 15 HBsAg-negative/HBcAb-positive); among them, HBV reactivation was documented in 2 cases.
Survival
The median follow-up time for all patients was two years (range 1–14) (2.8 years for living patients). Overall, 163 patients died. Causes of death were NHL progression in 113 patients, hepatic failure in 12, infection in 6, cardiovascular events in 15, other cancers in 9, and other causes in 8. Three-year OS and PFS of the whole cohort were 71% and 55%, respectively (Figure 1A and B), while 3-year OS and PFS in the subgroup of patients treated with R-CHOP were 71% and 58%, respectively (Figure 1C and D). In a crude comparison between patients treated with R-CHOP and CHOP, R-CHOP retained a borderline benefit for OS (P=0.070) and a significant advantage for PFS (P=0.007) (Online Supplementary Figure S1A and B). Patients who developed severe hepatotoxicity did not exhibit reduced OS and PFS (P=0.8 and 0.7, respectively). Notably, the small subset of responding patients who received antiviral treatment with interferon with or without ribavirin after induction treatment (n=23) displayed a significantly better OS (P=0.008) than those who did not receive it.
Figure 1.
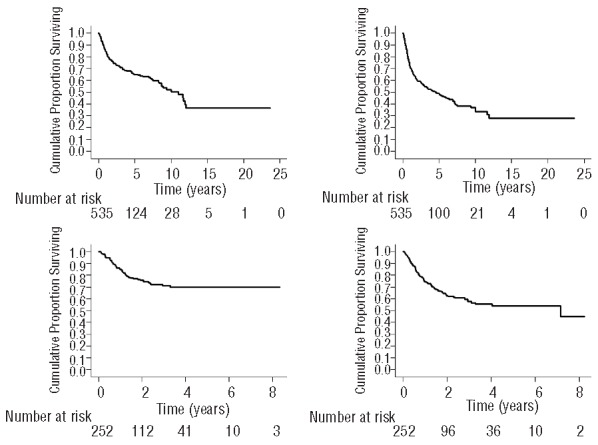
OS and PFS of 535 patients with HCV-positive DLBCL treated with curative-intent therapy (panels A and B); OS and PFS in 252 patients with HCV-positive DLBCL treated with R-CHOP (panels C and D).
Prognostic factors
The parameters associated with a shorter OS and PFS at univariate analysis are listed in Table 4. Notably, all IPI parameters were predictive for OS and PFS. Consequently, the IPI and the R-IPI were predictive for OS and PFS (P<0.001), although the differences in survival between the low-intermediate- and low-risk IPI groups and between the good and very good R-IPI risk groups did not reach statistical significance (Table 4 and Online Supplementary Figure S2). Liver involvement by lymphoma was associated with a poorer outcome, while splenic or bone marrow involvement was not. Base-line HCV-RNA load over 1000 KIU/mL was the only virological parameter affecting OS (P=0.036), as no specific HCV-genotype had any impact on the outcome. Among parameters related with liver function and histopathology, serum albumin below 3.5 g/dL (P<0.001), serum total bilirubin of 2 mg/dL or over (P=0.020), INR over 1.7 (P=0.020), Child score (P=0.026) and elevated HAI (>9) or stage (>2) at liver biopsy (P=0.013) were predictive for OS, while pre-treatment elevated ALT levels were not. According to a forward stepwise multivariate Cox regression analysis on OS, the following parameters retained statistical significance (Table 5): ECOG performance status of 2 or over (HR=4.05, 95%CI: 2.20–7.48; P<0.001), HCV-RNA over 1000 KIU/mL (HR=2.25, 95%CI: 1.22–4.15; P=0.010), serum albumin below 3.5 g/dL (HR=2.42, 95%CI: 1.31–4.48; P=0.005). The same parameters retained predictive value also at multivariate Cox regression analysis on PFS and DSS.
Table 4.
Prognostic factors at univariate analyses (Cox) in 535 patients with HCV-positive DLBCL treated with curative-intent therapy.
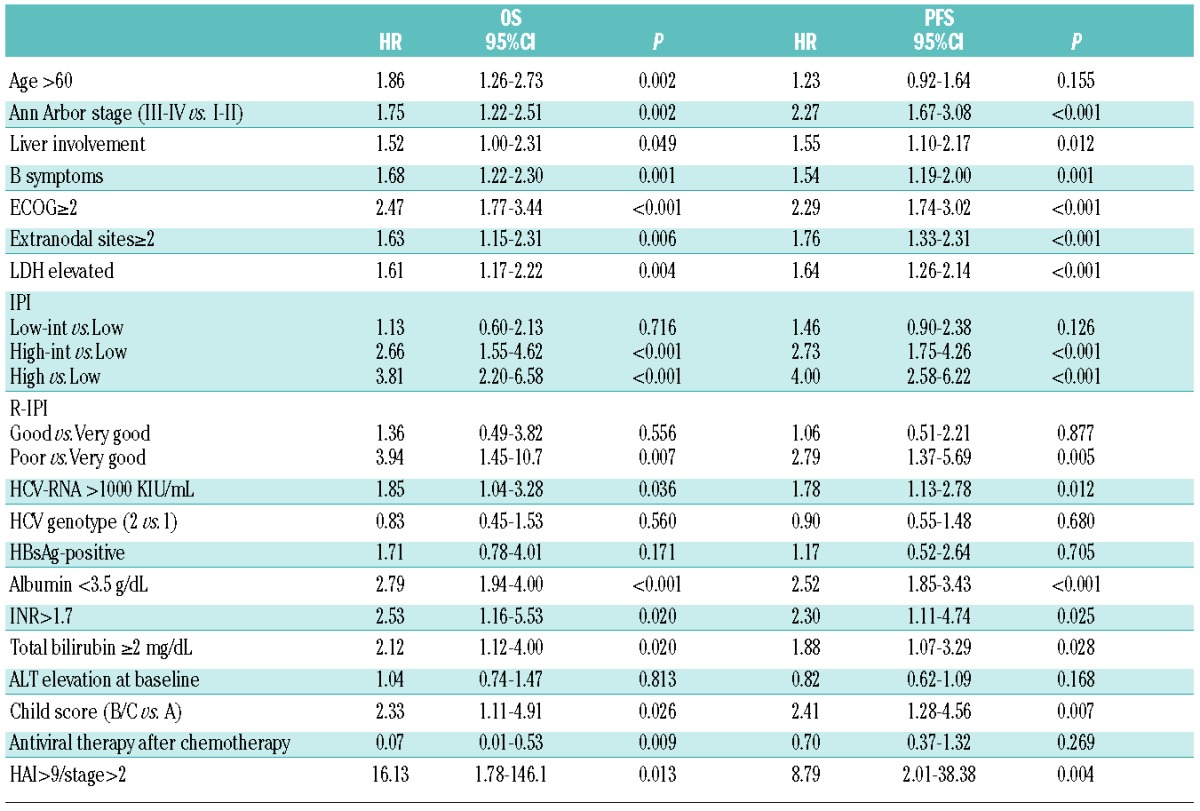
Table 5.
Prognostic factors at Cox regression multivariate analysis in HCV-positive DLBCL (171 patients).

Prognostic model
We combined the 3 factors significantly associated to a worse OS and PFS (ECOG ≥2, albumin <3.5 g/dL, HCV-RNA load >1000 KIU/mL), in an “HCV Prognostic Score” (HPS) able to discriminate 3 categories of risk (low=0; intermediate=1; high-risk ≥2 factors; P<0.001) (Figure 2A). All 3 parameters were concurrently available in 171 patients. The 3 categories of risk resulted well balanced, as 30% of patients (n=51) were classified as low-risk, 46% (n=79) as intermediate-risk, and 24% (n=41) as high-risk. A comparison of HPS and IPI distribution is shown in the Online Supplementary Table S2. During a median follow-up time of two years, 8% (n=4), 31% (n=24) and 56% (n=23) of patients belonging respectively to low-, intermediate-and high-risk groups died, corresponding to an estimated 3-year OS of 92% (95%CI: 76–97%) for the low-risk group, 77% (95%CI: 64–85%) for the intermediate-risk group, and 39% (95%CI: 21–56%) for the high-risk group. HPS score was predictive also for PFS (P<0.001), with 3-year PFS 81%, 61% and 19% in low-, intermediate- and high-risk groups, respectively (Figure 2B) and for DSS (Online Supplementary Figure S3). There was no statistical difference between OS and PFS of the patients for whom all 3 parameters were available and OS and PFS of patients without all 3 parameters (OS: P=0.67; PFS: P=0.72). HPS score retained prognostic value in the subgroup of patients treated with R-CHOP (n=110; OS and PFS P<0.001) (Figure 3A and B) and in those treated with CHOP (n=50; OS and PFS P<0.001) (Figure 3C and D). After adjusting according to prognostic factors (ECOG, albumin and HCV-RNA) or according to the whole HPS score in a multivariate fashion, R-CHOP retained a prognostic benefit both for OS and PFS (P<0.001) (Online Supplementary Figure S4).
Figure 2.
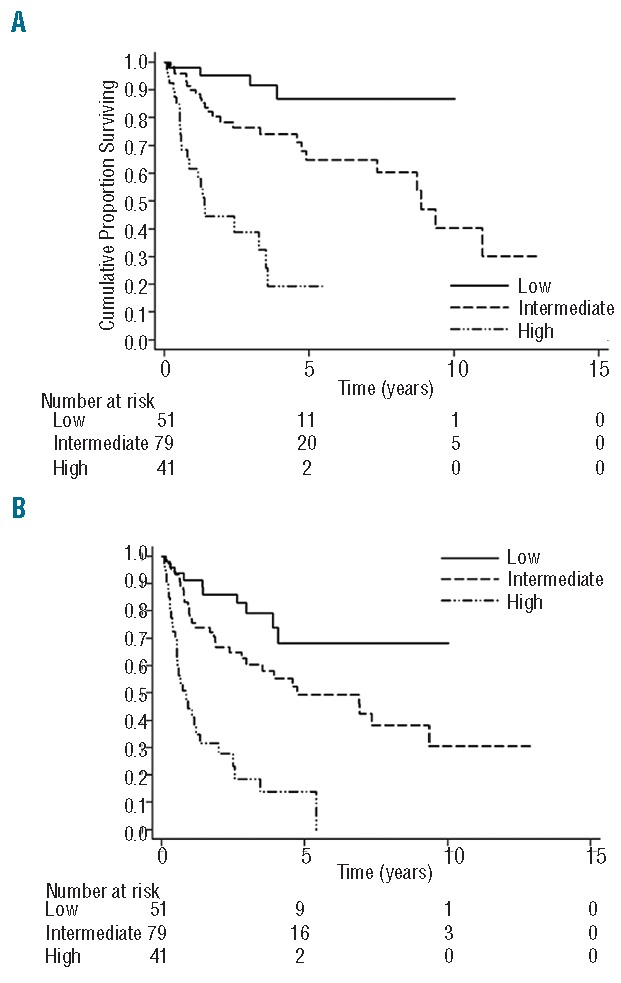
OS according to HCV prognostic score (HPS) categories (A); PFS according to HCV prognostic score (HPS) categories (B) (171 patients).
Figure 3.
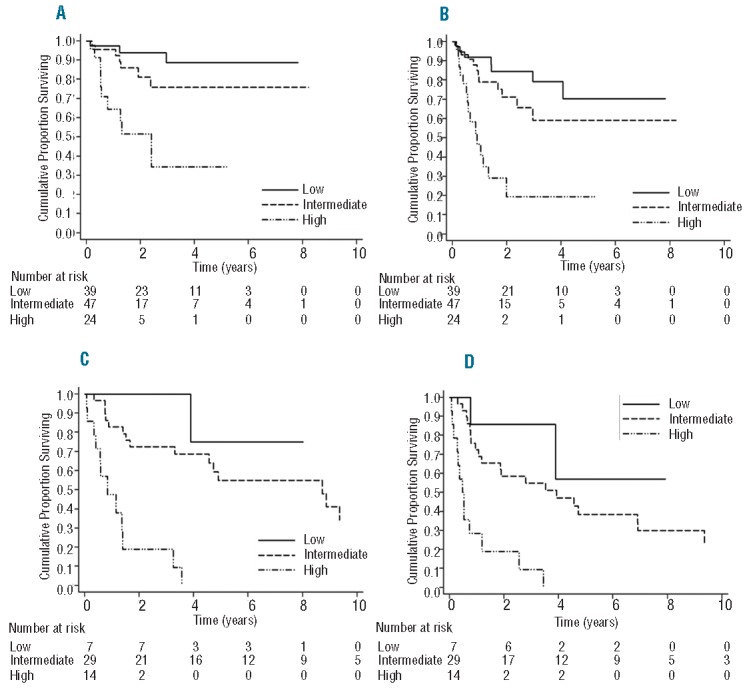
OS according to HCV prognostic score (HPS) categories in the subgroup of patients treated with R-CHOP (A); PFS according to HCV prognostic score (HPS) categories in the subgroup of patients treated with R-CHOP (B); OS according to HCV prognostic score (HPS) categories in the subgroup of patients treated with CHOP (C); PFS according to HCV prognostic score (HPS) categories in the subgroup of patients treated with CHOP (D).
After adjusting by the IPI in multivariate Cox regression analysis, the HPS retained prognostic effect for OS (P<0.001), while the IPI itself did not, both on the whole population (Likelihood ratio test P=0.29) and in the subgroup of patients treated with R-CHOP (Likelihood ratio test P=0.07). The C-statistic was a little higher in the model with HPS with respect to the C-statistic of the model with the IPI (for OS: 0.73 (range 0.70–0.78) vs. 0.67 (range 0.63–0.72); for PFS: 0.70 (range 0.650–0.76) vs. 0.66 (range 0.62–0.70)). In addition, the predictive power of HPS was significantly higher than that of R-IPI for OS (0.73 (range 0.70–0.78) vs. 0.66 (range 0.62–0.69)) and higher with borderline significance for PFS (0.70 (range 0.65–0.76) vs. 0.64 (range 0.60–0.67)).
Split sample analysis
To internally validate the model, we performed the prognostic analysis after splitting the study population into two parts (testing and validation samples). After stepwise procedure in two-thirds of patients (n=353) randomly chosen (testing sample), the only parameters that retained prognostic significance on OS at multivariate analysis were still HCV-RNA load (HR 3.42, 95%CI: 1.62–7.19; P=0.001), albumin below 3.5 g/dL (HR 2.94, 95%CI: 1.38–6.27; P=0.005) and ECOG (HR 2.94, 95%CI: 1.36–6.34; P=0.006). All the same parameters retained prognostic significance also on PFS.
In the 112 patients of the testing sample for whom all 3 parameters were available, the prognostic model, obtained by selecting these 3 parameters, still identified three prognostic groups (0 factors, 1 factor, 2 or more factors) with statistically different OS and PFS (P<0.001) (Online Supplementary Figure S5A and B). When applied to the remaining one-third of patients (validation sample; total n=182 patients; 59 patients with all 3 parameters available) the model maintained prognostic significance for OS (P<0.001) (Online Supplementary Figure S6) and PFS (P<0.001).
Discussion
In this study, we present clinical and virological features, toxicity data and prognostic evaluation of the largest series of HCV-associated DLBCL reported so far.
We confirm in a larger cohort previous findings about the efficacy and the safety of rituximab in terms of hepa-totoxicity in HCV-positive DLBCL.8 In fact, we did not record any difference in terms of severe hepatotoxicity between the patients treated with R-CHOP and those treated with CHOP, while, after adjusting by prognostic factors, patients treated with R-CHOP displayed a better OS and PFS. Interestingly, in the subgroup of patients monitored with viremia, the viral load invariably increased after treatment with R-CHOP (or CHOP), in agreement with the findings of Ennishi et al.3 However, we did not find any clear direct relation between the increase in HCV-RNA and severe hepatotoxicity. The interplay between HCV-RNA and transaminases in HCV-positive NHL during (immuno-)chemotherapy has been analyzed only in a limited number of patients in a few previous studies,3,8–15 with conflicting conclusions. While small case series suggested that HCV-RNA peak may precede or coincide with the development of an ALT flare,11,13 as for HBV,16 in the majority of the reports, HCV-RNA seems to behave irrespective of ALT levels and, therefore, does not seem to be useful to predict hepatotoxicity.8,10,12,15,17 In our study, the only risk factor for severe hepatotoxicity was an increase in base-line value of ALT, similar to findings in the Japanese study.3
So far, only a few studies have evaluated the prognosis of HCV-positive DLBCL.3–5 In the pre-rituximab era, Besson et al. reported a worse OS in HCV-positive DLBCL patients treated with intense chemotherapeutic protocols.4 On the contrary, the retrospective study of Ennishi et al.3 of 131 HCV-positive patients treated with R-CHOP showed that there was no significant difference in prognosis according to HCV infection, with only a border-line worse outcome in HCV-positive patients (3-year OS 75% vs. 84%; P=0.07). Interestingly, the outcome of the patients treated with R-CHOP in our study (3-year OS 71%) is similar to that of the Japanese study (3-year OS 75%). In addition, it does not substantially differ from that of the comparable population of HCV-negative patients treated with 6 or 8 R-CHOP14 in the RICOVER-60 study (3-year OS 78% and 72%, respectively). Consistent with the Japanese study,3 the occurrence of severe hepatotoxicity in our patients (14%) did not have any impact on survival.
An intriguing finding is that the delivery of antiviral therapy in responding patients after induction treatment may influence survival, improving OS. This is in accordance with preliminary findings18 and suggests that successful antiviral therapy in DLBCL patients in CR after R-CHOP, together with the reduction in the risk of progression to cirrhosis, may also ideally reduce the risk of relapse by eradicating a possible trigger of lymphoma recurrence. Therefore, our data support the importance of validating this attractive integrated treatment strategy prospectively.
The primary aim of our study was to develop a specific prognostic model for HCV-positive DLBCL patients. HPS score consists of one clinical parameter (ECOG) and 2 laboratory parameters (albumin levels and HCV-RNA). With the use of this score, 3 prognostic categories with significantly different OS, PFS and DSS were identified. Interestingly, 2 factors (ECOG and albumin) may reflect in part both lymphoma activity and liver condition, while high HCV-RNA load is a merely virological parameter. Performance status has been consistently demonstrated to be a prognostic factor in aggressive lymphomas,6,7,19 especially in the elderly population,20 as it comprises overall disease burden and behavior, and the patient’s comorbidities and consequent ability to tolerate therapies with curative intent. In HCV-positive DLBCL, performance status may be affected also by hepatic condition, as a considerable proportion of patients (near to 15% both in the present and in the Japanese3 studies) display features of cirrhosis. Low albumin concentration was predictive of inferior survival in DLBCL also in the seminal study of the IPI, but it was not included in that score because of an insufficient number of cases.6 Moreover, it is included in prognostic models for other lymphoma subtypes, such as splenic marginal-zone lymphoma21 and Hodgkin lymphoma.22 In addition, low albumin is one of the defining parameters of the Child-Pugh score for assessing prognosis in HCV-related cirrhosis.23 HCV-RNA load has been consistently related to the severity of hepatitis infection.24 Despite different proposed cut-off levels, the majority of studies confirmed that higher base-line viral loads are associated with lower sustained virological response rates after antiviral therapy.25–27 A high base-line viral load may reflect a more advanced hepatic infection, with possible lower tolerance to chemotherapy.24 In accordance with this hypothesis, a large population-based study demonstrated that high viral loads significantly predict a more rapid progression toward end-stage liver disease.28 In addition, this finding may indirectly suggest that, at least in some cases, the model of the intimate biological relationship between HCV chronic infection and lymphoproliferation may still be valid even at DLBCL stage.29,30 Moreover, high viraI load has been recently demonstrated to predict worst long-term outcome also in HCC,31 another HCV-related cancer.
Although the number of patients with all 3 independent parameters of the HPS available is relatively small, we performed the analysis with a 2-step procedure (one for creating the model and one for its validation)21,32 to confirm the robustness of the model. Multivariate analysis of prognostic parameters of two-thirds of the population still identified the same 3 variables that were able to stratify 3 subgroups with statistically different OS and PFS. The model was also effective in the remaining one-third of patients. The prediction of the prognosis is a key issue in a potentially curable but highly heterogeneous disease like DLBCL. Moreover, the identification of patients at “low” or at “high” risk could have even increased therapeutic implications in a “difficult to treat” population like HCV-positive DLBCL patients, in whom toxicity development is not negligible. Notably, the IPI has never been validated in a specific HCV-positive DLBCL population, as in previous HCV-positive DLBCL series the IPI was not found to be able to stratify patients into different risk classes, only in part due to small sample size.3–5 In our series, the IPI and the R-IPI was predictive of the prognosis in univariate analysis, although differentiation between risk classes was not accurate, especially in intermediate-risk categories. Unlike the IPI, the HPS allows patients to be stratified into risk categories with a clear-cut different prognosis. In fact, even if all IPI single factors, and consequently the whole score, reached prognostic significance in univariate analysis, only ECOG maintained it in multivariate analysis and was included in the final model, while other parameters did not. One of the possible explanations for this may be that hepatitis-induced liver damage may alter the prognostic significance of LDH, as suggested by previous series.3–5 Another reason may be that age as categorical variable (with the standard cut off of 60 years) did not retain prognostic significance in multivariate analysis, probably as a result of the high proportion (73%) of elderly patients in this setting of DLBCL owing to the particular epidemiology of HCV infection in Italy. In our series, the HPS performed better than the IPI in the overall prediction of the prognosis in HCV-positive DLBCL, both in the whole cohort and in the subgroup of patients treated with R-CHOP, as it maintained prognostic significance after adjusting by the IPI in multivariate analysis, while the IPI did not. Moreover, the HPS was shown to have a higher predictive value with respect to the R-IPI also according to the Harrel C-statistic, reaching the threshold (C >0.70) necessary to be useful on the level of the individual patient.33 In patients treated with R-CHOP, however, although the HPS clearly identifies the group of patients with a high-risk disease, the prognosis of the intermediate- and the low-risk groups seems to be less clearly different. This could be due to the interaction of the independent prognostic benefit of rituximab addition to CHOP, as demonstrated in multivariate analysis. Some limitations of our study have to be discussed. First, we did not have a matched-pair control group to make a direct comparison of prognosis and outcome with HCV-negative DLBCL patients. Moreover, the new HPS model was developed on only a small proportion of the patients treated with curative-intent therapy, as base-line HCV-RNA load was not available in many cases. However, there was no difference in OS and PFS between the patients with all 3 parameters and the patients without all parameters.
In conclusion, a specific prognostic model for HCV-positive DLBCL is able to identify 3 risk-categories with different survival in patients treated with R-CHOP or CHOP and may be a clinically useful prognostic tool for stratifying HCV-positive DLBCL patients.
Supplementary Material
Footnotes
The online version of this article has a Supplementary Appendix.
Funding
Supported by Associazione Italiana Ricerca contro il Cancro (AIRC), My first AIRC grant 2011 (to LA).
Authorship and Disclosures
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.de Sanjose S, Benavente Y, Vajdic CM, Engels EA, Morton LM, Bracci PM, et al. Hepatitis C and non-Hodgkin lymphoma among 4784 cases and 6269 controls from the International Lymphoma Epidemiology Consortium. Clin Gastroenterol Hepatol. 2008;6(4):451–8 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mele A, Pulsoni A, Bianco E, Musto P, Szklo A, Sanpaolo MG, et al. Hepatitis C virus and B-cell non-Hodgkin lymphomas: an Italian multicenter case-control study. Blood. 2003;102(3):996–9 [DOI] [PubMed] [Google Scholar]
- 3.Ennishi D, Maeda Y, Niitsu N, Kojima M, Izutsu K, Takizawa J, et al. Hepatic toxicity and prognosis in hepatitis C virus-infected patients with diffuse large B-cell lymphoma treated with rituximab-containing chemotherapy regimens: a Japanese multi-center analysis. Blood. 2010;116(24):5119–25 [DOI] [PubMed] [Google Scholar]
- 4.Besson C, Canioni D, Lepage E, Pol S, Morel P, Lederlin P, et al. Characteristics and outcome of diffuse large B-cell lymphoma in hepatitis C virus-positive patients in LNH 93 and LNH 98 Groupe d’Etude des Lymphomes de l’Adulte programs. J Clin Oncol. 2006;24(6):953–60 [DOI] [PubMed] [Google Scholar]
- 5.Visco C, Arcaini L, Brusamolino E, Burcheri S, Ambrosetti A, Merli M, et al. Distinctive natural history in hepatitis C virus positive diffuse large B-cell lymphoma: analysis of 156 patients from northern Italy. Ann Oncol. 2006;17(9):1434–40 [DOI] [PubMed] [Google Scholar]
- 6.A predictive model for aggressive non-Hodgkin’s lymphoma. The International Non-Hodgkin’s Lymphoma Prognostic Factors Project. N Engl J Med. 1993;329 (14):987–94 [DOI] [PubMed] [Google Scholar]
- 7.Sehn LH, Berry B, Chhanabhai M, Fitzgerald C, Gill K, Hoskins P, et al. The revised International Prognostic Index (R-IPI) is a better predictor of outcome than the standard IPI for patients with diffuse large B-cell lymphoma treated with R-CHOP. Blood. 2007;109(5):1857–61 [DOI] [PubMed] [Google Scholar]
- 8.Arcaini L, Merli M, Passamonti F, Bruno R, Brusamolino E, Sacchi P, et al. Impact of treatment-related liver toxicity on the outcome of HCV-positive non-Hodgkin’s lymphomas. Am J Hematol. 2010;85(1):46–50 [DOI] [PubMed] [Google Scholar]
- 9.Ennishi D, Terui Y, Yokoyama M, Mishima Y, Takahashi S, Takeuchi K, et al. Monitoring serum hepatitis C virus (HCV) RNA in patients with HCV-infected CD20-positive B-cell lymphoma undergoing rituximab combination chemotherapy. Am J Hematol. 2008;83(1):59–62 [DOI] [PubMed] [Google Scholar]
- 10.Marignani M, Mangone M, Cox MC, Angeletti S, Veggia B, Ferrari A, et al. HCV-positive status and hepatitis flares in patients with B-cell non-Hodgkin’s lymphoma treated with rituximab-containing regimens. Dig Liver Dis. 2011;43(2):139–42 [DOI] [PubMed] [Google Scholar]
- 11.Pitini V, Sturniolo G, Arrigo C, Leonardi S, Pino S, Altavilla G. HCV genotype 2 as a risk factor for reactivation in patients with B-cell lymphoma undergoing rituximab combination chemotherapy. Br J Haematol. 2010;150(1):116–8 [DOI] [PubMed] [Google Scholar]
- 12.Nooka A, Shenoy PJ, Sinha R, Lonial S, Flowers CR. Hepatitis C reactivation in patients who have diffuse large B-cell lymphoma treated with rituximab: a case report and review of literature. Clin Lymphoma Myeloma Leuk. 2011;11(5):379–84 [DOI] [PubMed] [Google Scholar]
- 13.Hsieh CY, Huang HH, Lin CY, Chung LW, Liao YM, Bai LY, et al. Rituximab-induced hepatitis C virus reactivation after spontaneous remission in diffuse large B-cell lymphoma. J Clin Oncol. 2008;26(15):2584–6 [DOI] [PubMed] [Google Scholar]
- 14.Ennishi D, Yokoyama M, Terui Y, Takeuchi K, Ikeda K, Tanimoto M, et al. Does rituximab really induce hepatitis C virus reactivation? J Clin Oncol. 2008;26(28):4695–6 [DOI] [PubMed] [Google Scholar]
- 15.Tsutsumi Y, Ichiki K, Shiratori S, Kawamura T, Tanaka J, Asaka M, et al. Changes in hepatitis C virus antibody titer and viral RNA load in non-Hodgkin’s lymphoma patients after rituximab chemotherapy. Int J Lab Hematol. 2009;31(4):468–70 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Kusumoto S, Tanaka Y, Ueda R, Mizokami M. Reactivation of hepatitis B virus following rituximab-plus-steroid combination chemotherapy. J Gastroenterol. 2011;46(1): 9–16 [DOI] [PubMed] [Google Scholar]
- 17.Aksoy S, Abali H, Kilickap S, Erman M, Kars A. Accelerated hepatitis C virus replication with rituximab treatment in a non-Hodgkin’s lymphoma patient. Clin Lab Haematol. 2006;28(3):211–4 [DOI] [PubMed] [Google Scholar]
- 18.La Mura V, De Renzo A, Perna F, D’Agostino D, Masarone M, Romano M, et al. Antiviral therapy after complete response to chemotherapy could be efficacious in HCV-positive non-Hodgkin’s lymphoma. J Hepatol. 2008;49(4):557–63 [DOI] [PubMed] [Google Scholar]
- 19.Ziepert M, Hasenclever D, Kuhnt E, Glass B, Schmitz N, Pfreundschuh M, et al. Standard International prognostic index remains a valid predictor of outcome for patients with aggressive CD20+ B-cell lymphoma in the rituximab era. J Clin Oncol. 2010;28(14): 2373–80 [DOI] [PubMed] [Google Scholar]
- 20.Pfreundschuh M, Schubert J, Ziepert M, Schmits R, Mohren M, Lengfelder E, et al. Six versus eight cycles of bi-weekly CHOP-14 with or without rituximab in elderly patients with aggressive CD20+ B-cell lymphomas: a randomised controlled trial (RICOVER-60). Lancet Oncol. 2008;9(2): 105–16 [DOI] [PubMed] [Google Scholar]
- 21.Arcaini L, Lazzarino M, Colombo N, Burcheri S, Boveri E, Paulli M, et al. Splenic marginal zone lymphoma: a prognostic model for clinical use. Blood. 2006;107 (12):4643–9 [DOI] [PubMed] [Google Scholar]
- 22.Hasenclever D, Diehl V. A prognostic score for advanced Hodgkin’s disease. International Prognostic Factors Project on Advanced Hodgkin’s Disease. N Engl J Med. 1998;339(21):1506–14 [DOI] [PubMed] [Google Scholar]
- 23.Planas R, Balleste B, Alvarez MA, Rivera M, Montoliu S, Galeras JA, et al. Natural history of decompensated hepatitis C virus-related cirrhosis. A study of 200 patients. J Hepatol. 2004;40(5):823–30 [DOI] [PubMed] [Google Scholar]
- 24.Adinolfi LE, Utili R, Andreana A, Tripodi MF, Marracino M, Gambardella M, et al. Serum HCV RNA levels correlate with histological liver damage and concur with steatosis in progression of chronic hepatitis C. Dig Dis Sci. 2001;46(8):1677–83 [DOI] [PubMed] [Google Scholar]
- 25.Fried MW, Shiffman ML, Reddy KR, Smith C, Marinos G, Goncales FL, Jr, et al. Peginterferon alfa-2a plus ribavirin for chronic hepatitis C virus infection. N Engl J Med. 2002;347(13):975–82 [DOI] [PubMed] [Google Scholar]
- 26.Itoh Y, Nishimura T, Hashimoto H, Yamaguchi K, Niimi T, Yokomizo C, et al. Simple formula to predict response to peginterferon alpha2b and ribavirin combination therapy in genotype 1 chronic hepatitis C patients with high viral loads. Hepatol Res. 2011;41(2):126–32 [DOI] [PubMed] [Google Scholar]
- 27.Neukam K, Camacho A, Caruz A, Rallon N, Torres-Cornejo A, Rockstroh JK, et al. Prediction of response to pegylated interferon plus ribavirin in HIV/hepatitis C virus (HCV)-coinfected patients using HCV genotype, IL28B variations, and HCV-RNA load. J Hepatol. 2012;56(4):788–94 [DOI] [PubMed] [Google Scholar]
- 28.Hisada M, Chatterjee N, Kalaylioglu Z, Battjes RJ, Goedert JJ. Hepatitis C virus load and survival among injection drug users in the United States. Hepatology. 2005;42(6): 1446–52 [DOI] [PubMed] [Google Scholar]
- 29.Marcucci F, Mele A. Hepatitis viruses and non-Hodgkin lymphoma: epidemiology, mechanisms of tumorigenesis, and therapeutic opportunities. Blood. 2011;117(6): 1792–8 [DOI] [PubMed] [Google Scholar]
- 30.Kasama Y, Sekiguchi S, Saito M, Tanaka K, Satoh M, Kuwahara K, et al. Persistent expression of the full genome of hepatitis C virus in B cells induces spontaneous development of B-cell lymphomas in vivo. Blood. 2010;116(23):4926–33 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Shindoh J, Hasegawa K, Matsuyama Y, Inoue Y, Ishizawa T, Aoki T, et al. Low Hepatitis C Viral Load Predicts Better Long-Term Outcomes in Patients Undergoing Resection of Hepatocellular Carcinoma Irrespective of Serologic Eradication of Hepatitis C Virus. J Clin Oncol. 2013;31(6): 766–73 [DOI] [PubMed] [Google Scholar]
- 32.Solal-Celigny P, Roy P, Colombat P, White J, Armitage JO, Arranz-Saez R, et al. Follicular lymphoma international prognostic index. Blood. 2004;104(5):1258–65 [DOI] [PubMed] [Google Scholar]
- 33.Hosmer DWLS. Applied Logistic Regression. New York, NY, 2000 [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.