

Abstract
Deficiency of sterol C4 methyl oxidase, encoded by the SC4MOL gene, has recently been described in four patients from three different families. All of the patients presented with microcephaly, congenital cataracts, and growth delay in infancy. The first patient has suffered since the age of six years from severe, diffuse, psoriasiform dermatitis, sparing only her palms. She is now 20 years old. The second patient is a 5 year old girl who has just started to develop dry skin and hair changes. The third and fourth patients are a pair of affected siblings with a severe skin condition since infancy. Quantitative sterol analysis of plasma and skin scales from all four patients showed marked elevation of 4α-methyl- and 4, 4′-dimethylsterols, consistent with a deficiency in the first step of sterol C4 demethylation in cholesterol biosynthesis. Mutations in the SC4MOL have been identified in all of the patients.
SC4MOL deficiency is the first autosomal recessive disorder identified in the sterol demethylation complex. Cellular studies with patient-derived fibroblasts have shown a higher mitotic rate than control cells in cholesterol-depleted medium, with increased de novo cholesterol biosynthesis and accumulation of methylsterols. Immunologic analyses of granulocytes and B cells from patients and obligate carriers in the patients’ families indicated dysregulation of immune-related receptors. Inhibition of sterol C4 methyl oxidase in human transformed lymphoblasts induced activation of the cell cycle. Additional studies also demonstrated diminished EGFR signaling and disrupted vesicular trafficking in cells from the affected patients. These findings suggest that methylsterols play an important role in epidermal biology by their influence on cell proliferation, intracellular signaling, vesicular trafficking and immune response. SC4MOL is situated within the psoriasis susceptibility locus PSORS9, and may be a genetic risk factor for common skin conditions.
Introduction
Cholesterol is a key component of cell membranes, lipid rafts and the immediate precursor of steroids, vitamin D and bile acids. Many disorders of cholesterol synthesis share common clinical features, such as abnormal morphogenesis, growth delay and psychomotor disabilities [1]. However, there are also striking differences suggesting that reduced de novo cholesterol synthesis per se may not primarily underlie some of the symptoms including cataracts, skin, and immunoglobin abnormalities. Recent studies implicate the accumulation of pre-cholesterol sterols and the replacement of cholesterol with some of these sterols in lipid rafts as playing a key role in the underlying pathophysiology [2]. The metabolic pathway for cholesterol synthesis is shown in Figure 1. SC4MOL deficiency has only recently been described and is the first autosomal recessive disorder identified in the sterol demethylation complex. Biochemical and immunologic abnormalities in these patients underscore the important role of methylsterols in human biology and suggest novel methods of therapy.
Figure 1.
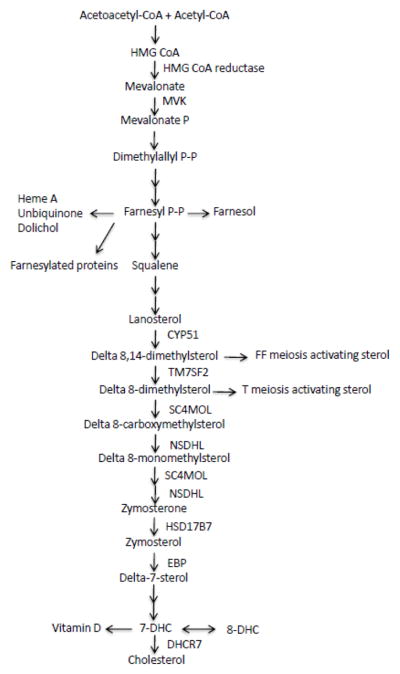
A scheme of metabolic pathway for cholesterol biogenesis.
Clinical presentation
The first patient is a Caucasian female who was diagnosed at age 15 years with a long standing history of severe psoriasiform dermatitis affecting her entire body but sparing the palms (Figure. 2A) [1]. In addition she demonstrated chronic arthralgias, small stature, microcephaly, delayed puberty and intellectual disability. Skin was normal at birth and dermatitis was first noted around her umbilicus at the age of two. It subsequently progressed to her back and trunk with generalization to the remainder of her body by the age of six. The dermatitis worsens in the winter or when under stress, and only partially responds to standard anti-inflammatory therapy. The patient also had a history of congenital cataracts, mild developmental delay, microcephaly (at 13 years of age, her head circumference was 53.5 cm, <3rd percentile), and failure to thrive. Her height was at the 3% between 9 and 39 months of age, but at age 13 years, her weight was 28.6 kg (< 3rd % ile, 50% for a 9-year-old) and her height was 140 cm (<3rd %ile, 50th % for a 10–1/2 year old). A skeletal survey at age 15 years identified only delayed skeletal maturation. Skin biopsy showed psoriasiform hyperplasia, dilated capillaries in the dermal papillae, and neutrophils in the epidermis and stratum corneum originally felt to be consistent with psoriasis. However closer examination of the tissue revealed the presence of several foamy cells in the dermis. Oil red O staining revealed intracellular lipid in these cells, reminiscent of that reported in patients with congenital hemidysplasia with ichthyosiform erythroderma and limb defects [3] syndrome [4]. The foam cells were CD68 negative, indicating that they were not macrophages, thus differentiating them from the cells seen in CHILD syndrome and verruciform xanthoma. Rather, immunohisochemistry and hematoxylin and eosin stained sections suggested that they were lipid-laden fibroblasts. Taken together, the histologic features are consistent with a psoriasiform dermatitis with some features of a verruciform xanthoma. Traditional therapies for psoriasis were implemented, including topical corticosteroids, calcipotriene, cyclosporine A, etanercept, phototherapy, and oral isotretinoin. However, while her skin briefly improved with cyclosporine A treatment, she did not exhibit a long term response to any of the therapies. Subsequent additional evaluation revealed markedly elevated levels of serum IgE (1,486 IU/ml; normal <180) and IgA (684 IU/ml; normal <218). Her serum lipid profile showed a persistently low total cholesterol level (85 mg/dl; normal 140–176), low HDL (28 mg/dl; normal 35–75) and low LDL (49 mg/dl; normal 70–160), but normal triglycerides 84 mg/dl; normal 50–200) and VLDL 8 mg/dl; normal 8–14).
Figure 2.
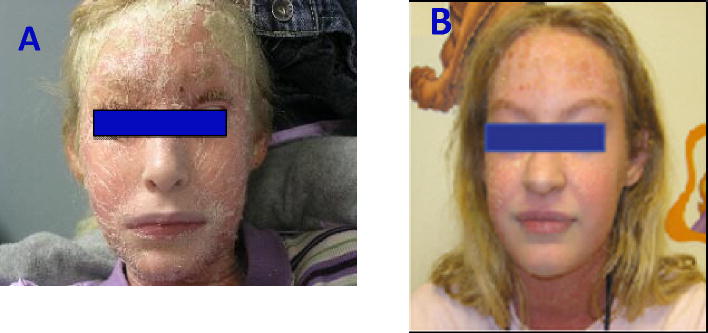
Pictures of patients with SC4MOl deficiency. A. The index patient with skin lesions; B. Improved skin condition of the index patient after cholesterol and statin treatment.
The second patient was diagnosed at 2 years old. She is an Hispanic female who presented with microcephaly, congenital cataracts and developmental and growth delay. She has joint contracture most marked in the low extremities. Her serum total cholesterol levels are in the range of 90 mg/dl [5]. Now age five years of life, her skin is dry but has never demonstrated a marked psoriasiform rash.
The third and fourth patients are two affected siblings from one family, and both presented with severe skin manifestations similar to patient one beginning in early infancy. Cholesterol levels in these two patients have been within normal limits (John McGrath, King’s College, London, UK, personal communication).
Biochemical and Genetics Findings
All patients with sterol C4 methyl oxidase have exhibited an abnormal plasma sterol profile gas chromatography-mass spectrometry (GC-MS), with 20- and 500-fold elevation of 4α-monomethyl sterols and 4, 4′-dimethyl sterols, respectively [6]. Similar sterol profiles were present in skin scales of all four patients. No 4-carboxylmethylsterol or 4-methylsterone were detected in either skin scales or skin fibroblasts from these patients. SMO deficiency is a block at the first step of demethylation of 4,4′-dimethylsterols. The fact that both 4α-monomethylsterols and 4,4′-dimethyl sterols were elevated in all four patients suggests some degree of residual sterol C4 methyl activity. Nonetheless, the levels of plasma 4,4′-dimethyl sterols in SMO patients are much greater than the dimethylsterol levels that may occasionally be seen in patients with congenital hemidysplasia with ichthyosiform erythroderma and limb defects [3] syndrome. Methylsterol levels were also mildly elevated in the plasma of the parents of all the four patients, suggesting a subclinical effect in the heterozygous state [1]
The SC4MOL gene is ubiquitously expressed in almost all human tissues. Multiple GEO expression profiles of this gene are present in the NIH database (GDS596; http://www.ncbi.nlm.nih.gov/sites/entrez). Two different mRNA variants are reported, consistent with alternative splicing. Isoform 2 differs from isoform 1 by the absence of exon 2. The tissue expression profiles of the probes targeting the exon 2–3 junction vs. the exon 4–5 junction are almost identical, indicating that isoform 1 is the major RNA isoform in most human tissues. The expression of this gene is highest in liver, brain, adrenal gland, lymphoblast, skin, testis, and vascular tissues. Expression data of SC4MOL in cultured epidermal keratinocytes (GDS2611, GDS2903) and normal leukocytes (GDS3207) can also be found in the GEO database.
Two heterozygous variations from the published sequence were identified in the SC4MOL gene of the first patient; c.519T>A and c.731A>G encoding p.H173Q and p.Y244C, respectively, in the predicted SMO protein. The 519T>A mutation was carried by the patient’s father, and the 731A>G was present in the mother. Both positions encode amino acids within highly conserved metal-binding domains in SMO and neither of the variants was identified in any of the databases for common SNPs in populations. In addition, H173Q alters a predicted active site encompassing the second iron-binding motif of the enzyme. One homozygous variation in SC4MOL was identified in the second patient, c.G343G>A encoding p.G115R. The amino acid G115 is also high conserved across evolution and the change of G115R is predicted to be damaging. Both parents of the second patient were heterozygous for the same variant.
Cell hyperproliferation in SMO deficiency
C4-methylsterols are members of a family of molecules known as meiosis activating sterols (MAS). They were first identified in high concentration in testis and ovary and play roles in activation of meiosis. However, the effect of MAS on cell cycle regulation and mitosis is unknown [7, 8]. The fact that mutations in DHCR14B/LBR, SC4MOL, NSDHL, and EBP or their mouse homologues result in proliferative skin disease led to an examination of cell proliferation in the skin fibroblasts from the index patient. The rate of cell division was found to be higher in patient fibroblasts than control cells when cultured in cholesterol-restricted medium, a condition under which de novo cholesterol biosynthesis is stimulated [9]. The S-G2-M to G0-G1 ratio in patient skin fibroblasts was 3-fold higher than control cells. Thus, cholesterol-restricted medium induced the patient cells to proceed into S-G2-M. To further examine a potential link between MAS production and cell division, transformed control human lymphoblasts were cultured in the presence of a sterol methyl oxidase inhibitor, 3-amino-1,2,4-triazole (ATZ) [10, 11]. Under these conditions, the S-G2-M/G0-G1 ratio increased 3-fold in treated lymphoblasts, while neither simvastatin (an inhibitor of HMG-CoA reductase ) or fluconazole (a weak inhibitor of lanosterol 14α demethylase; CYP51) had a significant effect on cell cycle progression. These data demonstrated that alterations in sterol methyl oxidase impact cell cycle activation [1].
Immune dysregulation
Many of the defects of cholesterologenesis are associated with immunological manifestations. The first patient’s skin briefly improved with cyclosporine A, but, she ultimately became resistant to treatment, suggesting that her immune response differed compared to other cholesterol pathway disorders and common psoriasis. Activated CD16+ granulocytes (identified by CD25+CD69+ and CD86+HLA-DR+ subsets) were increased 30- and 20-fold, with a 30- and 15-fold increase in the number of toll-like receptor (TLR)-2+TLR-4− granulocytes in the patient and her father, respectively compared with healthy controls, [1]. Up-regulation of TLR-2, but not TLR-4, is considered typical for patients with psoriasis [12] or psoriatic arthritis [13], but not those with rheumatoid arthritis. Over-expression of TLR-2 and down regulation of TLR-4 in granulocytes likely reflects dysregulation of the immune response in the patient following normal bacterial infections. Consistent with this interpretation, expression of the granulocyte-specific CD16b isoform was also markedly down regulated in both the patient and her father, suggesting a defect in phagocyte function. No significant differences were observed in the monocyte population. In the lymphocyte compartment, both patient and father had a significantly higher proportion of CD8dim T cells that were also CD28− CD56+ compared to controls. Down regulation of CD8 and CD28 and accumulations of CD28−CD56+ T cells are indicative of pervasive immune activation in the setting of chronic inflammatory disease or aging [14].
SC4MOl regulates epidermal growth factor receptor (EGFR) signaling and vesicular trafficking
Disruptions of C4 demethylation complex genes cause skin manifestation associated with elevations of sterol intermediates in skin, but the underlying mechanism is still largely unknown [15]. EGFR signaling is of critical importance for keratinocyte proliferation and differentiation. A significant deficiency in EGFR signal transduction was detected in SC4MOL patient fibroblasts (Figure 3) as well as in NSDHL-deficient mouse embryonic fibroblasts [15]. Addition of ketoconazole, an inhibitor for the upstream gene CYP51A1, to the cell culture medium reduced the level of C4 methylsterols in these cells and improved the EGFR signaling. It has been reported that SC4MOL is required for effective endosomal trafficking of EGFR [15]. Specifically, silencing SC4MOL and NSDHL prevents association of internalized EGFR with RAB11 positive recycling endosomes in cancer cells and increases association of EGFR with RAB7 endosomes. Treatment with ketoconazole normalizes EGFR degradation in SC4MOL depleted cells [15]. Of note, it has been suggested that SC4MOL may directly regulate the endocytic recycling of receptors such as ADP ribosylation factor (ARF) GTPases including ARF1, ARF4 and 5. Reduced co-localization of EGFR and ARF5 has been reported in SC4MOL-silenced cells [15]. Although the phospholation of EGFR appears to be increased due to the impaired EGFR trafficking to lysosome for degradation, the downstream EGF specific ERK phospholation was also reduced in patient’s fibroblast (Figure 3). Therefore the impairment of intracellular trafficking in SC4MOL deficiency is likely at multiple steps of vesicular trafficking. Given that sterols are important component of lipid rafts, methylsterols likely regulates vesicular trafficking through the association of lipid rafts with microtubule or cytoskeleton or both.
Figure 3.
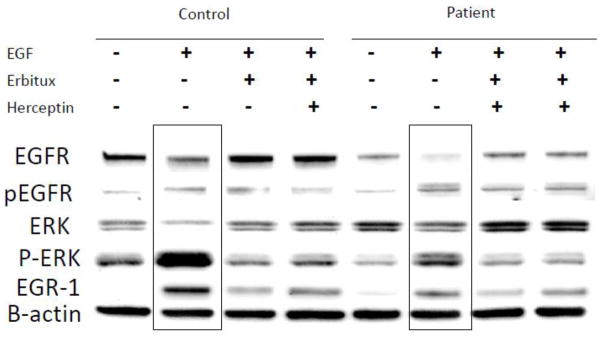
Impaired EGFR signaling in the skin fibroblast from the index SC4MOL deficient patient. EGFR specific phospholation of ERK, induced by EGF, and the expression of its downstream transcriptional factor EGR-1 are significantly reduced in the fibroblast from SC4MOL deficient patient compared to those from controls. It also appears that the overall level of EGFR is lower in the cells from the patient, suggestive of a reduction at the expression of EGFR in SC4MOL deficiency.
EGFR is normally expressed in the epidermis, sebaceous glands, and hair follicular epithelium, where it plays roles in maintenance of normal skin health, including control of differentiation, protection against damage induced by ultraviolet radiation, inhibition of inflammation, and acceleration of wound healing [16]. Eighty to 90% of respondents of EGFR inhibition therapy develop variable degrees of skin rash that is often reversible with withdraw of the therapy. Inhibition of EGFR is believed to cause follicular occlusion and rupture because of premature epithelial differentiation and an increase in the expression of genes that stimulate inflammation, apoptosis and cell attachment. Therefore diminished EGFR signaling in SC4MOL deficient patients will likely alter the skin permeability barrier and further promote bacterial overgrowth, thus exacerbating cutaneous injury in these patients.
Epidermal hyperplasia and the barrier dysfunctions
Cholesterol is vital for permeability of the skin barrier and its disruption leads to epidermal hyperplasia and accelerated DNA synthesis, potentially playing a role in the development of psoriasis [17]. However, there is considerable controversy over whether this represents an intrinsic effect or a secondary reaction to outside exposures [18]. Either possibility is also conceivable to explain the epidermal abnormalities observed in patients with SC4MOl deficiency. The fact that the second patient exhibits immunocyte abnormalities (even somewhat more severe than those of the first patient) without inflammatory skin disease supports a primary role for the methylsterols in the pathogenesis of the immune abnormalities. Similarly, all obligate carriers tested thus far have had significant immunocyte abnormalities without inflammatory skin diseases. These observations lead to the possibility that use of supplementation of topical cholesterol and using cholesterologenesis inhibitor, statin, to reduce methylsterol level in epidermis are important in treating these patients and reverse their skin condition.
Treatment
If methylsterols play a primary role in this condition, the use of a statin to block substrate entry into the metabolic pathway could be of clinical benefit to SC4MOL deficient patients. Under these conditions, supplementation with the end product of the pathway (cholesterol) is also likely to be necessary. To examine this possibility, an initial treatment protocol for the first patient provided purified food grade cholesterol at 100 mg/kg/day. After three months of cholesterol supplementation, the patient’s methylsterol level was reduced by about 20% with normalization of the plasma cholesterol level, but the methylsterol level dropped no further [5].The addition of an oral statin (10 mg/day) plus bile acids (30 mg/kg/day) along with cholesterol normalized the methylsterol levels in blood. In the two years following institution of this therapy, the patient’s weight and linear growth improved dramatically with a maximum growth velocity of 0.8 cm/month. Her chronic arthralgias also resolved and her skin disease has improved dramatically (Figure 1B). Analysis of immunocyte profiles pre and post therapy revealed a significant reduction in granulocyte activation after treatment, approaching the levels seen in her parents. Although the second patient has no overt skin manifestation, increased expression of CD25 and TLR-2 in leukocytes was observed that was similar to that of the index patient [5].
Conclusion
SC4MOL deficiency is a newly discovered inborn error of cholesterol metabolism characterized by the accumulation of a large amount of methylsterols, particularly dimethylsterols in the affected patients. Although the pathogenesis of this gene defect is not fully understood, there are clearly associations between cholesterologenesis and immune regulation, an effect likely mediated by the abnormally accumulating methylsterols. Most importantly, this disorder is at least partially corrected with cholesterol and statin supplements, particularly the immune dysregulation, skin disease, and growth delay. Therefore it is important to screen for this disorder by plasma or skin sterol analysis in the patients with inflammatory proliferative skin disease with unknown etiology.
Highlights.
Four described SC4MOL deficiency patients described, 4 with skin manifestations
Deficiency of SC4MOL disrupts the cell cycle and immune regulation
The EGFR signaling pathway is down regulated in SC4MOL deficient fibroblast
Epidermal hyperplasia and barrier dysfunctions in SC4MOL deficiency
Treatment with statin and cholesterol supplementation improves symptoms
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.He M, Kratz LE, Michel JJ, Vallejo AN, Ferris L, Kelley RI, Hoover JJ, Jukic D, Gibson KM, Wolfe LA, Ramachandran D, Zwick ME, Vockley J. Mutations in the human SC4MOL gene encoding a methyl sterol oxidase cause psoriasiform dermatitis, microcephaly, and developmental delay. J Clin Invest. 2011;121:976–984. doi: 10.1172/JCI42650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rakheja D, Boriack RL. Precholesterol sterols accumulate in lipid rafts of patients with Smith-Lemli-Opitz syndrome and X-linked dominant chondrodysplasia punctata. Pediatr Dev Pathol. 2008;11:128–132. doi: 10.2350/06-10-0179.1. [DOI] [PubMed] [Google Scholar]
- 3.Schenk B, Imbach T, Frank CG, Grubenmann CE, Raymond GV, Hurvitz H, Korn-Lubetzki I, Revel-Vik S, Raas-Rotschild A, Luder AS, Jaeken J, Berger EG, Matthijs G, Hennet T, Aebi M. MPDU1 mutations underlie a novel human congenital disorder of glycosylation, designated type If. J Clin Invest. 2001;108:1687–1695. doi: 10.1172/JCI13419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ishibashi M, Matsuda F, Oka H, Ishiko A. Abnormal lamellar granules in a case of CHILD syndrome. J Cutan Pathol. 2006;33:447–453. doi: 10.1111/j.0303-6987.2006.00470.x. [DOI] [PubMed] [Google Scholar]
- 5.He M, Smith L, Chang R, Kratz L, Michel J, Vallejo A, Kelley R, Li X, Vockley J. Clinical Evaluation and Treatment of Two Patients with SC4MOL Deficiency, a New Disorder in Cholesterologenesis. American College of Medical Genetics Annual Meeting; 2011; Vancouver. 2011. [Google Scholar]
- 6.Mandato C, Brive L, Miura Y, Davis JA, Di Cosmo N, Lucariello S, Pagliardini S, Seo NS, Parenti G, Vecchione R, Freeze HH, Vajro P. Cryptogenic liver disease in four children: a novel congenital disorder of glycosylation. Pediatr Res. 2006;59:293–298. doi: 10.1203/01.pdr.0000196378.30165.26. [DOI] [PubMed] [Google Scholar]
- 7.Xie H, Xia G, Byskov AG, Andersen CY, Bo S, Tao Y. Roles of gonadotropins and meiosis-activating sterols in meiotic resumption of cultured follicle-enclosed mouse oocytes. Mol Cell Endocrinol. 2004;218:155–163. doi: 10.1016/j.mce.2003.11.030. [DOI] [PubMed] [Google Scholar]
- 8.Cukurcam S, Betzendahl I, Michel G, Vogt E, Hegele-Hartung C, Lindenthal B, Eichenlaub-Ritter U. Influence of follicular fluid meiosis-activating sterol on aneuploidy rate and precocious chromatid segregation in aged mouse oocytes. Hum Reprod. 2007;22:815–828. doi: 10.1093/humrep/del442. [DOI] [PubMed] [Google Scholar]
- 9.Gibson KM, Hoffmann G, Schwall A, Broock RL, Aramaki S, Sweetman L, Nyhan WL, Brandt IK, Wappner RS, Lehnert W, et al. 3-Hydroxy-3-methylglutaryl coenzyme A reductase activity in cultured fibroblasts from patients with mevalonate kinase deficiency: differential response to lipid supplied by fetal bovine serum in tissue culture medium. J Lipid Res. 1990;31:515–521. [PubMed] [Google Scholar]
- 10.Hashimoto F, Hayashi H. Identification of intermediates after inhibition of cholesterol synthesis by aminotriazole treatment in vivo. Biochim Biophys Acta. 1991;1086:115–124. doi: 10.1016/0005-2760(91)90162-b. [DOI] [PubMed] [Google Scholar]
- 11.Hashimoto F, Hayashi H. Peroxisomal cholesterol synthesis in vivo: accumulation of 4-methyl intermediate sterols after aminotriazole inhibition of cholesterol synthesis. Biochim Biophys Acta. 1994;1214:11–19. doi: 10.1016/0005-2760(94)90003-5. [DOI] [PubMed] [Google Scholar]
- 12.Begon E, Michel L, Flageul B, Beaudoin I, Jean-Louis F, Bachelez H, Dubertret L, Musette P. Expression, subcellular localization and cytokinic modulation of Toll-like receptors (TLRs) in normal human keratinocytes: TLR2 up-regulation in psoriatic skin. Eur J Dermatol. 2007;17:497–506. doi: 10.1684/ejd.2007.0264. [DOI] [PubMed] [Google Scholar]
- 13.Candia L, Marquez J, Hernandez C, Zea AH, Espinoza LR. Toll-like receptor-2 expression is upregulated in antigen-presenting cells from patients with psoriatic arthritis: a pathogenic role for innate immunity? J Rheumatol. 2007;34:374–379. [PubMed] [Google Scholar]
- 14.Michel JJ, Turesson C, Lemster B, Atkins SR, Iclozan C, Bongartz T, Wasko MC, Matteson EL, Vallejo AN. CD56-expressing T cells that have features of senescence are expanded in rheumatoid arthritis. Arthritis Rheum. 2007;56:43–57. doi: 10.1002/art.22310. [DOI] [PubMed] [Google Scholar]
- 15.Sukhanova A, Gorin A, Serebriiskii IG, Gabitova L, Zheng H, Restifo D, Egleston BL, Cunningham D, Bagnyukova T, Liu H, Nikonova A, Adams GP, Zhou Y, Yang DH, Mehra R, Burtness B, Cai KQ, Klein-Szanto A, Kratz LE, Kelley RI, Weiner LM, Herman GE, Golemis EA, Astsaturov I. Targeting C4-demethylating genes in the cholesterol pathway sensitizes cancer cells to EGF receptor inhibitors via increased EGF receptor degradation. Cancer discovery. 2013;3:96–111. doi: 10.1158/2159-8290.CD-12-0031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Overbeck TR, Griesinger F. Two cases of psoriasis responding to erlotinib: time to revisiting inhibition of epidermal growth factor receptor in psoriasis therapy? Dermatology (Basel, Switzerland) 2012;225:179–182. doi: 10.1159/000342786. [DOI] [PubMed] [Google Scholar]
- 17.Wolf R, Orion E, Ruocco E, Ruocco V. Abnormal epidermal barrier in the pathogenesis of psoriasis. Clin Dermatol. 2012;30:323–328. doi: 10.1016/j.clindermatol.2011.08.022. [DOI] [PubMed] [Google Scholar]
- 18.Wolf R, Wolf D. Abnormal epidermal barrier in the pathogenesis of atopic dermatitis. Clin Dermatol. 2012;30:329–334. doi: 10.1016/j.clindermatol.2011.08.023. [DOI] [PubMed] [Google Scholar]