

Abstract
Although studies on pediatric dysfunctional voiding are increasing, there have not been enough efforts to validate the Dysfunctional Voiding Symptom Score (DVSS) questionnaire. Therefore, we aimed to translate and validate the DVSS into Korean. The DVSS questionnaire was validated between January and October, 2013. Two bilinguals independently translated the English version of the DVSS questionnaire into Korean, and then reconciled the forward translation of the Korean version. The original DVSS was back-translated into English, then assessed for equivalence to the original. Cognitive debriefing interviews with 5 patients to test the interpretation of the translation were made, then modified and distributed to 48 patients for re-evaluation. A statistical analysis of inter-scale correlation, and test re-test consistency was performed with the Cronbach's alpha coefficient. The changes from patient interviews were reflected in the final version. In an intra-class correlation, the Cronbach's alpha was high in all of the questions (0.97, P < 0.001). Test re-test Cronbach's alpha analysis of reproducibility was higher than 0.8 for all of the 10 questions (P < 0.001). Translation and linguistic validation of Korean version of the DVSS questionnaire was completed by a proper process, with high reliability and validity.
Graphical Abstract
Keywords: Validation Studies, Questionnaires, Urination Disorders
INTRODUCTION
Dysfunctional voiding (DV) is a common clinical problem seen in approximately 40% patients who visit the pediatric urologist (1). DV manifests as numerous symptoms, such as recurrent urinary tract infections, urinary incontinence (UI), as well as bowel symptoms such as constipation and encopresis. According to the Standardization Committee of the International Children's Continence Society (ICCS), DV can be defined as "over activity of the urethral sphincter during the voiding contraction of the detrusor in neurologically normal children". However, such symptoms present in various ways, which makes clinical diagnosis and classification difficult. Although multiple methods have been utilized in the evaluation of pediatric dysfunctional voiding (2, 3), universally applicable methodologies have been rare.
In order to improve diagnostic accuracy, and to detect DV early, Farhat et al. (4) developed the DV scoring system (DVSS) questionnaire. This questionnaire was scientifically validated and evaluated pediatric DV. Silent DV which persists throughout childhood, adolescence and adulthood may be a risk factor for urologic diseases such as interstitial cystitis, prostatitis, or prostatodynia. Retrospective analysis of such patients with the present DVSS may be useful in promoting urological care for children.
Since its development, the DVSS questionnaire has been utilized in many reports investigating DV in the pediatric population. Although studies on pediatric DV are increasing, there are not enough efforts to publish the result of its translation into other languages and subsequent validation. As far as we know, Brazilian (5), and Chinese (6) versions of DVSS have been validated. However, as this questionnaire was written in English, and no similar validated questionnaires exist in Korea, a linguistic validation was necessary. When translating a questionnaire into another language, proper linguistic as well as cultural validation is necessary (7). Once validated, the DVSS questionnaire may become an invaluable tool for analysis of DV. The aim of this study was to validate the DVSS questionnaire into Korean, and put it to clinical use in pediatric patients, with cross-cultural equivalence to the original version.
MATERIALS AND METHODS
Between January and October 2013, the English version of the DVSS questionnaire was translated into Korean and validated. After investigation of linguistic validity, permission for translation was obtained, then forward translation, back-translation, debriefing, review, final proof-reading, and testing and re-testing was performed. Afterwards statistical analysis was performed.
The DVSS questionnaire
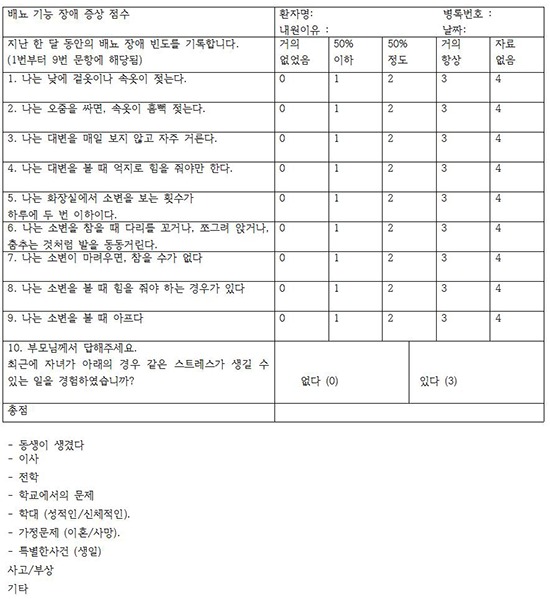
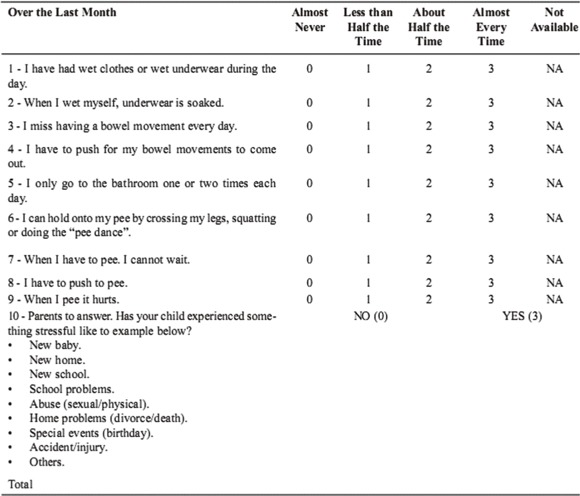
The DVSS questionnaire consists of a validated symptom scoring for wetting and functional disorders in children. The questionnaire is comprised of 10 quantitative and qualitative urological variables assessed by age-appropriate questions for children. The DVSS questionnaire is useful in objectively grading DV in children (4, 5) (Appendix-1).
The validation process
Translation and investigation of linguistic validity
Because Farhat et al. (4), the original creators of the intellectual property of the DVSS questionnaire could not directly participate as mediators in its translation, the first author controlled the translation. The translation research consisted of seven stages as follows between January 2013 and May 2013 (approximately 5 months). The main methodology was similar to the translation of Korean Version of the Pelvic Pain and Urgency/Frequency Patient Symptom Scale, as well as the Expanded Prostate Cancer Index Composite (EPIC) into a Korean version previously performed (7, 8).
1) Permission for translation and acquisition of the original version of the DVSS questionnaire: The corresponding author was directly in contact with the original author of the questionnaire, acquired written permission for the translation and the use of the original English version of the DVSS questionnaire by e-mail.
2) Forward translation: Two translators who were born in Korea and had lived in an English-speaking nation for at least for 1 yr and fluent in both English and Korean proceeded with the first forward translation. They were both informed of the guidelines for the forward translation of the English version of the DVSS questionnaire and then respectively proceeded with translation (ver 1.0a and 1.0b).
3) Reconciliation: The two translators reviewed the ver. 1.0a and 1.0b and produced a reconciled Korean version (Korean ver. 1.1) under the supervision of the corresponding author.
4) Back-translation: The ver. 1.1 was back-translated by a third translator who also was fluent in the English and Korean. A comparison between the original version and the back-translated version was performed. After this comparison, the first author was sent the discordant item concepts between the original and the back-translated versions. Those items were newly forward-translated, and the translation was translated again into English for review by the panel. The process was completed when the panel reviewed and accepted the new translation (Korean ver. 1.2).
5) Debriefing: The Korean ver. 1.2 questionnaire was presented to 5 outpatients presenting with symptoms suggestive of pediatric DV who visited the outpatient clinic of our hospital, and they also replied the questionnaire in order to investigate the appropriateness of the question items for the patients' situations and the linguistic understanding of each item. The patients and their caretakers provided feedback when they misunderstood the original concept of a question, when they had difficulty in understanding a question, and when a question was vague or not smooth. In each case, the authors summarized and organized their feedback. Before participation in this study, patients were informed about this study and consent was obtained.
6) The problems presented during the debriefing were reviewed, and the panel of experts examined the contents. Then, after exchange of feedback, the Korean version 1.3 was completed.
7) Final proof-reading: From the Korean ver. 1.3, the final Korean version of the DVSS questionnaire was completed after checking for errors in spelling or format.
8) Testing and re-testing was performed with the complete questionnaire. To confirm test-retest reliability, a repeat DVSS questionnaire was mailed out 1-2 weeks later or the questionnaire was re-distributed at outpatient follow-up without informing patients of the intent to conduct the same questionnaire. As a result, we obtained retest data from all of the patients who answered the original questionnaire.
Reliability analysis
The questionnaire data was recorded in commercial statistical software (Excel/2003 for Microsoft Windows). Descriptive statistics were used to describe the sample, to verify the content validity of the adapted instrument, and to determine the pretest results the following analyses were performed. The main methodology was similar to the development and validation of the Korean version of the Expanded Prostate Cancer Index Composite described by Chung et al. (7), and the Chinese DVSS validation methodology (6).
1) Cronbach's coefficient alpha was used to verify reliability. Cronbach's alpha values>0.70 were established as constituting evidence of satisfactory internal consistency.
2) Intraclass correlation coefficient (ICC) was used to verify reliability with reference to the stability of the instrument (test-retest). ICC values≥0.90 were considered evidence of stability. Statistical analyses of reliability and validity were performed with SPSS for Windows (version 17.0 K, SPSS, Chicago, IL, USA). To confirm reliability, test-retest correlation was assessed by intra-class correlation coefficient, and the internal consistency of each subscale was assessed by Cronbach's alpha coefficient. To confirm validity, the propriety of composition of the domain categories, interscale correlation between the function and bother subscales of each domain, and the inter-scale correlation among each subscale were analyzed.
Ethics statement
Prior to debriefing of the questionnaire in this study, the study protocol was approved by the institutional review board of Seoul National University Hospital (IRB No. H-1305-574-489).
RESULTS
Forward translation and reconciliation
In the forward translation process, consensus of the basic terminology was reached. The "Dysfunctional Voiding Symptom Score" was translated in this study without disagreement in Korean by both translators. "Half the time" was translated into "half" by Translator B and "50%" by Translator A, which has the same meaning, but Translator B chose to write it in numbers. As for Question 4, Translator A translated it as "I have to push hard when I have a bowel movement", and Translator B chose to express it as "I have to push a lot when I have a bowel movement" in Korean. Question 6 was translated as "When I hold urine, I cross my legs, squat, or move my legs as if I am dancing." by Translator A, and "When I hold urine, I cross my legs, squat, or dance as if I am holding urine." in Korean by Translator B.
Backward translation
Translator C translated "Dysfunctional voiding symptom score" as "Voiding dysfunction symptom score", which the panel considered acceptable. During the back translation, question 6 was quite awkward, "When I hold my urine in, I have to do so by crossing my legs, squatting, or tapping my feet lightly on the floor", which was due to a misunderstanding by the translator. The panel decided to use the original reconciled forward Korean translation without further correction. The back translation done by Translator C was a little bit formal compared with the original DVSS questionnaire, which was because she had older subjects in mind. The original DVSS is written in easy English, targeting younger subjects, which caused this difference. However, the panel decided that such subtle differences in nuances did not affect the overall meaning, and used the original reconciled forward Korean translation.
Results of the debriefing
After completion of the final backward translation of the DVSS questionnaire, 5 patients provided feedback for the questionnaire provided during the debriefing process. The questions that were considered unclear and were requested to be modified were identified during debriefing. As for question 3, the patients were asked whether they missed having a bowel movement every day. The original question itself is confusing, in that the patient does not know whether to answer whether they do not defecate on an everyday basis, or whether they fail to defecate daily occasionally. The options to choose from are also confusing. The option 'almost never' means that the patient rarely misses having a daily bowel movement, which could be easily phrased into 'I usually have a daily bowel movement'. Likewise, the answer 'almost every time' is also confusing. When the patient answers that he or she misses having a bowel movement almost every time, a more simple expression would be that 'I rarely have a bowel movement every day (daily)'. The option 'not available' was also pointed out as confusing, because patients considered 'I do not precisely remember' as more easy to understand. However, in an effort to keep the validated questionnaire as similar to the original as possible, question 3 was changed to mean " I do not have a bowel movement every day", and was changed into the Korean accordingly; "I do not have a bowel movement more than once every day." Question number 5 was also confusing, in that it asked patients whether they went to the bathroom one or two times each day, answering 'almost never' might mean that they might miss voiding during the daytime completely, or void more times than three during the day. As for patients with enuresis or daytime frequency, most patients answered 'almost never' to question number 5. However, daytime voiding frequencies of more than 7 times or 10 times could not be quantitatively analyzed. Therefore, in order to minimize confusion, we modified the question to "I go to the bathroom less than two times during the day", in order to clarify the meaning of the question, and changed the Korean question accordingly; "I go to the bathroom to void less than twice day" The patients commented that they could understand other questions without too much difficulty. However, as for question 10, they often asked whether they had to ask 3 points each for each option that they answered yes. We informed them that regardless how may options the patient might answer yes to question 10, they would be counted as 3 points, without any additional points. The final corrected version was completed. After completion, 5 patients debriefed the questionnaire, and responded that no questions were confusing.
Statistical validation
After review of such feedback about the final correction version of the questionnaire, two reviewers decided to distribute this debriefed version and test and re-test its validity. This final questionnaire was distributed to 48 patients. The demographics of these 48 patients were as following. The mean age of the patients was 8.0 yr (±3.37, SD) Twenty-four patients were male, and 24 were female. The chief complaints were evaluated (Table 1). Among the 48 patients analyzed, 29 (60.4%) showed DV symptoms, and 19 (39.6%) perceived themselves as asymptomatic. In an intra-class correlation, the Cronbach's alpha was high in a comparison of all of the questions (0.97, P<0.001). Test re-test analysis of reproducibility showed that the Pearson's coefficients and Cronbach's alpha were higher than 0.7 for all of the 10 questions of the DVSS questionnaire, and such a correlation was statistically significant (P<0.001) (Table 2). Such high internal consistency reflected the reliability of the Korean version of DVSS. In addition, a multivariate logistic regression analysis of factors affecting DV showed that question number 7 "When I have to pee, I cannot wait" showed statistically significant correlation with self-reported DV symptoms (Table 3).
Table 1.
Patient demographics
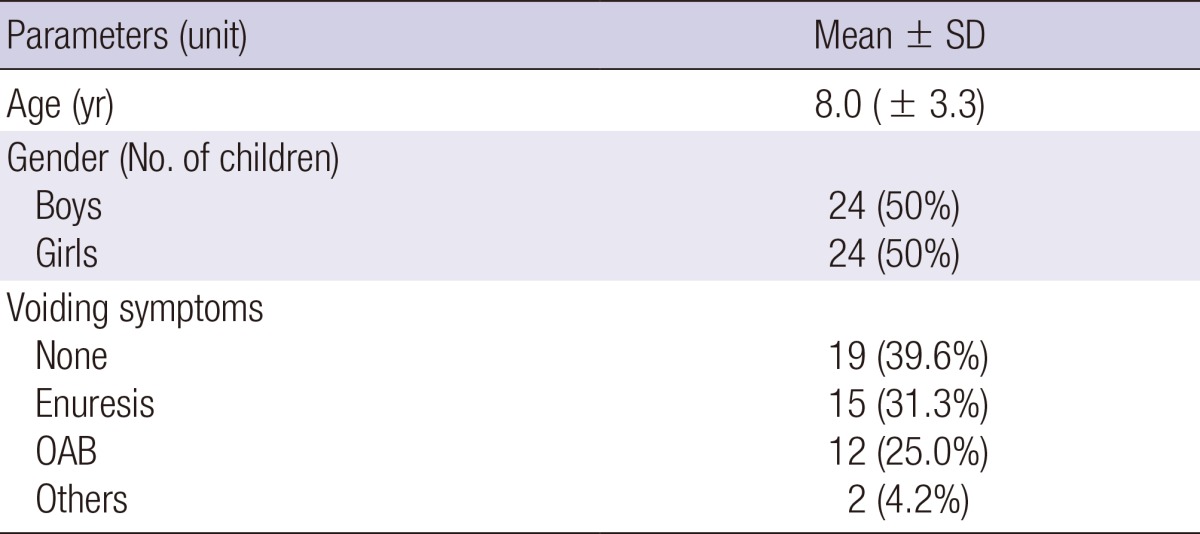
OAB, Overactive bladder.
Table 2.
Test re-test correlation analysis and Cronbach's alpha
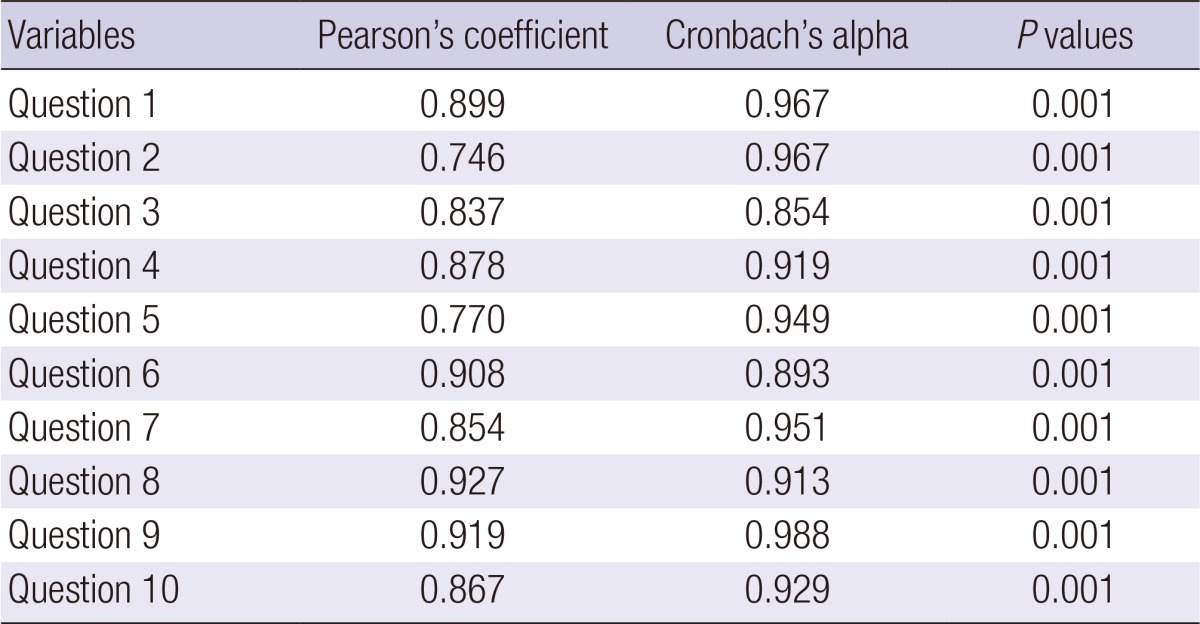
The questions are those of the final Korean version of the dysfunctional voiding symptom score (DVSS) questionnaire.
Table 3.
Multivariate logistic regression analysis of factors affecting dysfunctional voiding
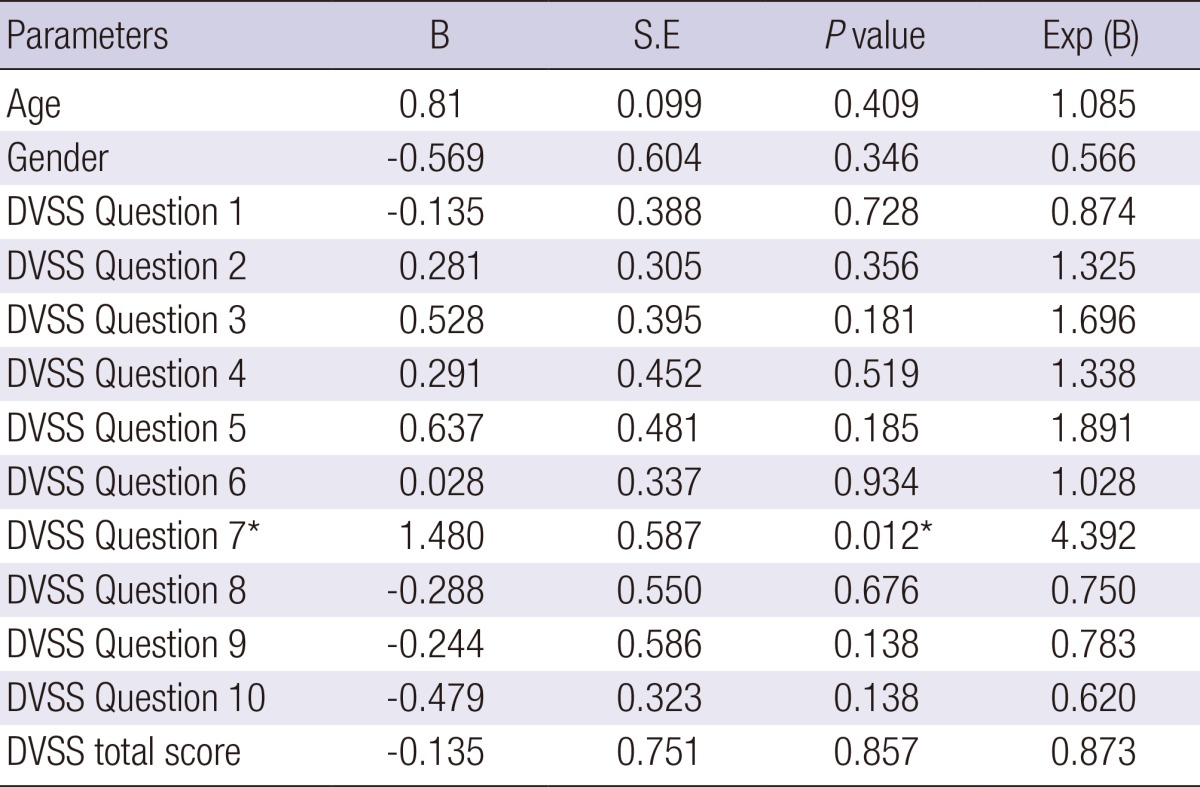
The questions are those of the final Korean version of the DVSS questionnaire. *P<0.05.
DISCUSSION
During the validation of the DVSS questionnaire, we experienced several obstacles not described in literature. First of all, the double negative expressions in English were often awkward when translated into Korean. Simplifying the original sentence was often required in order to make a smooth translation, and after debriefing, such modifications improved the understanding of the responder. Some of the options for the answers were rather ambiguous, especially 'not available'. We modified the expression to mean 'I do not recall' in Korean. After we modified the expression, the responders showed improved understanding of the questionnaire.
According to the statistical analysis of our study, the Korean version of the DVSS had a reliable test-retest consistency, showing reliability of the questionnaire translation. However, that questions such as number 5 only asked the total number of voiding per day, without specification of daytime or nighttime, and that there was no weight in multiple stressors in question 10 might have benefited from additional questions. However, because this study was about validation of a previous questionnaire and not development of a new one, such items could not be added. That question number 7, which evaluated urgency, showed correlation with self-reporting of symptoms was interesting. In the Chinese validation process, when the questions were classified into domains of 'overactive bladder symptoms', 'difficult elimination symptoms', and 'stress and dysuria symptoms', all of the domains showed statistical significance with presence of DV (5). Why such discrepancy was observed is not definite, but might be caused by the small number of patients, and a selection bias at the outpatient department. In future studies, randomized case controlled validation might be beneficial.
During this study, the authors translated the English DVSS questionnaire into Korean and investigated its linguistic validity. This study has an advantage that is the first prospective validation of the DVSS questionnaire in Korea. The Korean version of the DVSS questionnaire can be used as a screening test for diagnosing pediatric DV patients in the future. However, due to limited follow-up in some cases, and improvement of symptoms during follow-up which affected questionnaire results, an accurate test-pretest analysis was not possible. In future studies, a short-term follow-up and re-test would provide more valuable information. In addition, it shows promise for clinical application in the future. The Korean version of DVSS was developed to reflect the original version, and was adapted to the Korean culture and language. Reliability and validity were acceptable.
In conclusion, the cross-cultural adaptation process of the DVSS questionnaire to be used on Korean children was successfully completed following internationally accepted methodologies. The Korean version of DVSS is acceptable as an accurate diagnostic tool with cross-cultural variety in international multicenter research.
ACKNOWLEDGMENT
We are obliged to Ms. Jinjoo Kim as well as doctors Sungchan Park, Sung Yong Cho, Young Jae Im, and Chang Hee Yoo for valuable help in data acquisition and patient interviewing.
Appendix 1
The original dysfunctional voiding symptom score (DVSS) questionnaire
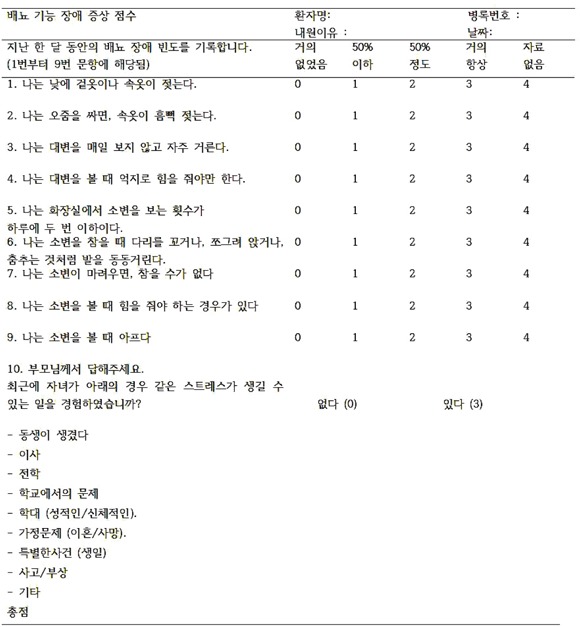
Appendix 2
The Korean version of the dysfunctional voiding symptom score (DVSS) score
Footnotes
We have no conflicts of interest to disclose.
References
- 1.Snodgrass W. Relationship of voiding dysfunction to urinary tract infection and vesicoureteral reflux in children. Urology. 1991;38:341–344. doi: 10.1016/0090-4295(91)80148-z. [DOI] [PubMed] [Google Scholar]
- 2.Akbal C, Genc Y, Burgu B, Ozden E, Tekgul S. Dysfunctional voiding and incontinence scoring system: quantitative evaluation of incontinence symptoms in pediatric population. J Urol. 2005;173:969–973. doi: 10.1097/01.ju.0000152183.91888.f6. [DOI] [PubMed] [Google Scholar]
- 3.Tokgöz H, Tan MO, Sen I, Ilhan MN, Biri H, Bozkirli I. Assessment of urinary symptoms in children with dysfunctional elimination syndrome. Int Urol Nephrol. 2007;39:425–436. doi: 10.1007/s11255-006-9062-0. [DOI] [PubMed] [Google Scholar]
- 4.Farhat W, Bägli DJ, Capolicchio G, O'Reilly S, Merguerian PA, Khoury A, McLorie GA. The dysfunctional voiding scoring system: quantitative standardization of dysfunctional voiding symptoms in children. J Urol. 2000;164:1011–1015. doi: 10.1097/00005392-200009020-00023. [DOI] [PubMed] [Google Scholar]
- 5.Calado AA, Araujo EM, Barroso U, Jr, Netto JM, Filho MZ, Macedo A, Jr, Bagli D, Farhat W. Cross-cultural adaptation of the dysfunctional voiding score symptom (DVSS) questionnaire for Brazilian children. Int Braz J Urol. 2010;36:458–463. doi: 10.1590/s1677-55382010000400009. [DOI] [PubMed] [Google Scholar]
- 6.Chang SJ, Chen TH, Su CC, Yang SS. Exploratory factory analysis and predicted probabilities of a Chinese version of Dysfunctional Voiding Symptom Score (DVSS) questionnaire. Neurourol Urodyn. 2012;31:1247–1251. doi: 10.1002/nau.22254. [DOI] [PubMed] [Google Scholar]
- 7.Chung KJ, Kim JJ, Lim SH, Kim TH, Han DH, Lee SW. Development and validation of the Korean version of expanded prostate cancer index composite: questionnaire assessing health-related quality of life after prostate cancer treatment. Korean J Urol. 2010;51:601–612. doi: 10.4111/kju.2010.51.9.601. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Son HC, Jung YJ, Chang JS, Kim SH, Hong SK, Oh SJ, Parsons CL, Lee KS. Translation and linguistic validation of the Korean version of the pelvic pain and urgency/frequency patient symptom scale. Int Neurourol J. 2010;14:112–121. doi: 10.5213/inj.2010.14.2.112. [DOI] [PMC free article] [PubMed] [Google Scholar]