

Abstract
There is a lack of information on critical care in Korea. The aim of this study was to determine the current status of Korean intensive care units (ICUs), focusing on the organization, characteristics of admitted patients, and nurse and physician staffing. Critical care specialists in charge of all 105 critical care specialty training hospitals nationwide completed a questionnaire survey. Among the ICUs, 56.4% were located in or near the capital city. Only 38 ICUs (17.3%) had intensive care specialists with a 5-day work week. The average daytime nurse-to-patient ratio was 1:2.7. Elderly people ≥ 65 yr of age comprised 53% of the adult patients. The most common reasons for admission to adult ICUs were respiratory insufficiency and postoperative management. Nurse and physician staffing was insufficient for the appropriate critical care in many ICUs. Staffing was worse in areas outside the capital city. Much effort, including enhanced reimbursement of critical care costs, must be made to improve the quality of critical care at the national level.
Graphical Abstract
Keywords: Critical Care, Intensive Care Units, Organizations, Outcome Assessment, Personnel Staffing, Korea
INTRODUCTION
In 1962, two university hospitals in Korea set up intensive care units (ICUs) as postoperative respiratory care units. Since then, the number of ICUs has continued to increase. When the Korean Society of Critical Care Medicine (KSCCM) was organized in 1980, 18 university hospitals and nine general hospitals had ICUs. Compared with other medical fields, the quality of critical care has lagged behind that of advanced countries. Moreover, the level of critical care quality differs significantly between university hospital ICUs (1).
To analyze the problems in critical care, the first step is to know the current status of critical care at the national level. Little information is available on critical care delivery in Korea. The purpose of this study was to clarify current problems related to ICU organization, critical care-giver staffing, and the characteristics of patients admitted to an ICU.
MATERIALS AND METHODS
Questionnaire survey
In the autumn of 2009, a questionnaire prepared as an official document of the KSCCM was distributed to the critical care physicians in all 105 critical care subspecialty training hospitals. The collected data were specific to the individual ICU rather than the hospital, and included ICU type, number of ICU and hospital beds, any association with a medical school, and nurse and physician staffing levels. We categorized ICUs as medical, surgical, pediatric, neurologic, emergency, coronary care units (CCUs), or mixed (not classified on the basis of patient characteristics). A dedicated physician was defined as a medical doctor who worked in an ICU more than 8 hr a day as a trainee or specialist. Patient information included age, length of stay, ICU admission source, ICU admission diagnosis, receipt of mechanical ventilation, vasoactive or inotropic drugs, blood transfusion(s), invasive monitoring, and cardiopulmonary resuscitation (CPR). Some survey data (including number of nursing staffs on duty per day, and demographic and clinical characteristics of patients per day) were recorded for 5 days and averaged to obtain a representative value for a single day. If necessary, local site visits were performed to clarify the information in the questionnaires.
Statistical analyses
Results are expressed as mean and standard deviation, or as percentages of respondents. Data were analyzed with SAS version 6.12 statistical software (SAS Institute, Cary, NC, USA). Two-tailed Student's t-tests, analyses of variance (ANOVA), Chi-square test, linear by linear association Chi-square test, and logistic regression analysis were used to test the significance of differences in responses, where appropriate. Differences were considered statistically significant at a P value<0.05.
Ethics statement
The study protocol was approved by the institutional review board of Chonnam National University Hospital (CNUH-2013-165). Informed consent was waived.
RESULTS
Response rates
The questionnaires were administered to the 105 hospitals with a critical care training program, and were endorsed by the KSCCM. A total of 220 responses were received from the ICUs in 86 hospitals (81.9%) and critical care data were obtained from 3,197 patients.
Characteristics of the ICUs
To be designated as a critical care subspecialty training hospital, several requirements of the KSCCM should be met. One of the most important is having an appropriate educational environment. As a result, 82.3% of all ICUs are in teaching hospitals, either university or university affiliated hospitals. Among the 220 ICUs (41 in public and 179 in private hospitals), 56.4% were located in (35%) or near (21.4%) the capital city, Seoul. Sixty-two of the ICUs (28.2%) were in hospitals with more than 1000 patient beds; 178 (88.2%) were specialized (Table 1). All but two of the neurologic ICUs admitted neurosurgical patients. Most of the ICUs were open units and most of the specialized ICUs were managed by the relevant hospital department (e.g., a medical ICU was part of a department of internal medicine). Of all the ICUs, 35.5% were affiliated with a Department of Internal Medicine, which was also the case for most CCUs, medical, and mixed ICUs. The next largest group was surgery (22.3%) followed by pediatrics (16.8%). All pediatric ICUs were affiliated with a pediatrics department. Anesthesiology was relatively infrequent as a separate department (14.1% of the total ICUs), but was evenly distributed among the various hospitals. Board certified internal medicine specialists were in charge of all the ICUs in most of the smaller hospitals: 61.1% of hospitals with ≤500 beds, 51.0% of hospitals with 501-1,000 beds, and 34.7% of hospitals with >1,000 beds (P=0.03, by linear-by-linear association Chi-square).
Table 1.
Descriptive characteristics of 220 ICUs in 86 Korean hospitals
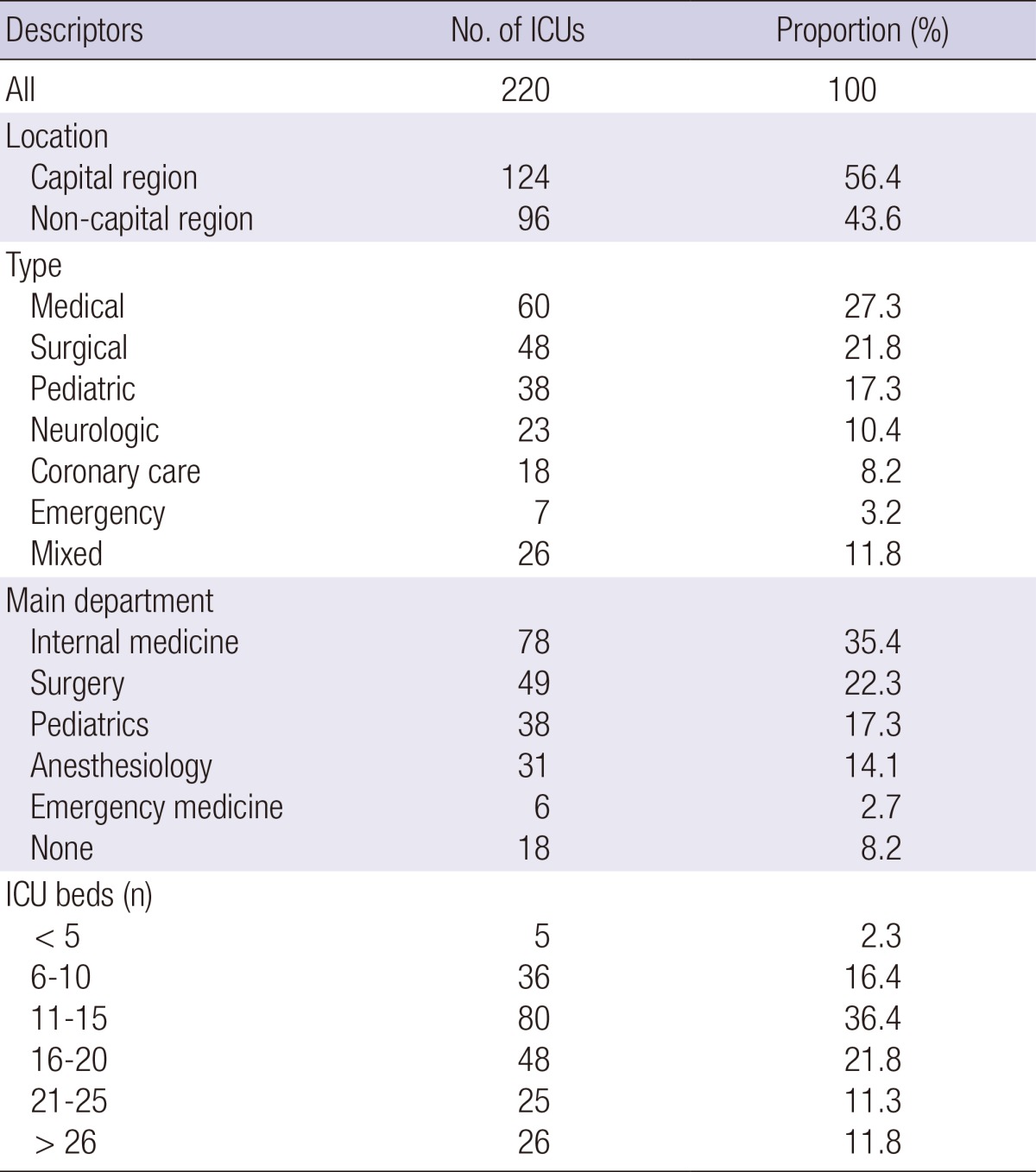
The number of ICU beds varied with the type of unit and the hospital size (median 15 beds, range 11-15; Table 1). The number of units also varied, increasing along with hospital size (Table 2) from 1.4 (≤500 beds) through 2.2 (501-1,000 beds) to 6.2 (>1,000 beds) per hospital. A single mixed or general ICU was more common in smaller hospitals and multiple, specialized ICUs were more common in larger hospitals (P<0.001).
Table 2.
ICU characteristics depending on the hospital size
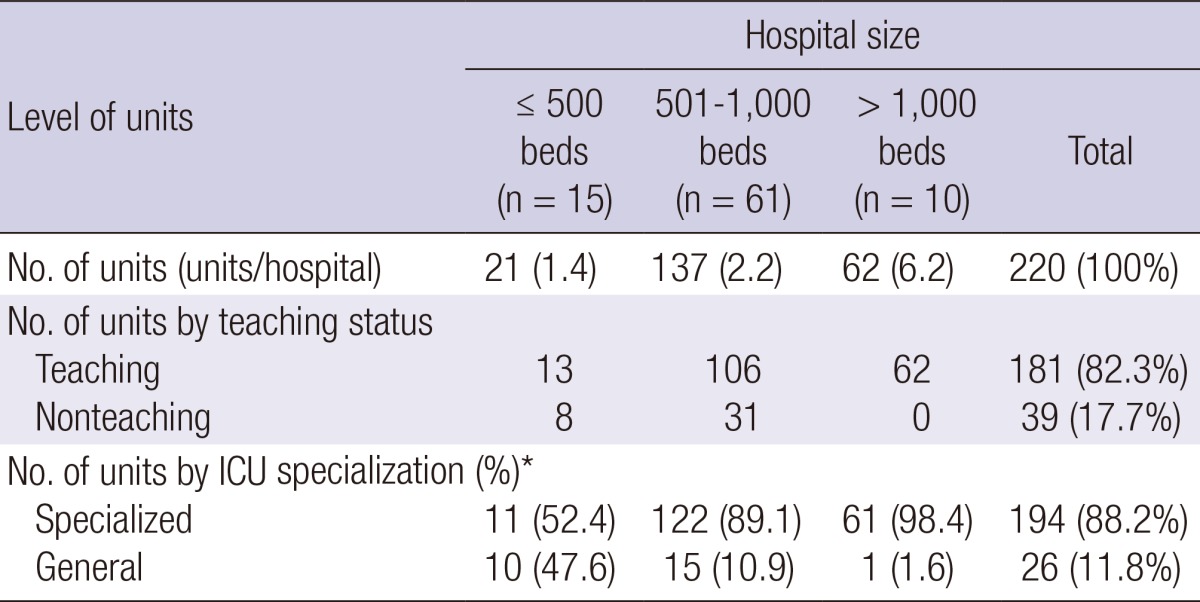
*P<0.001. ICU, intensive care unit; n, number of hospitals. There was a significant association between ICU specialization and the hospital size. P values were calculated with the linear-by-linear Chi-square test.
Physician and nurse staffing of the ICUs
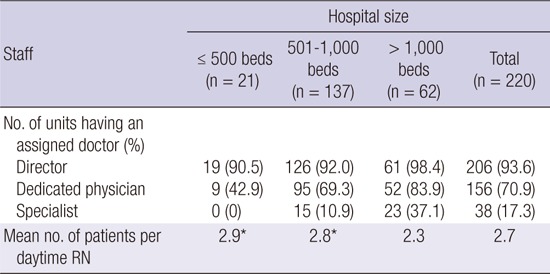
Most ICUs had a director who played a major role in the administrative duties and was partly involved in management of the ICU patients. Overall, 70.9% of the ICUs were staffed by dedicated physicians who worked in the unit more than 8 hr a day (Table 3). The dedicated physician included medical specialists, critical care subspecialists, interns (in only 12 ICUs), and residents. Only 38 ICUs (17.3%) had specialists on duty 5 days each week, and that decreased to 17 ICUs (7.7%) when the data from pediatric ICUs were excluded. Fulltime adult critical care subspecialists were only available in 17 units in nine hospitals (Fig. 1) and 12 of the 17 units (70%) were located in Seoul. The daytime nurse-to-patient ratio averaged 1:2.7, and was greater in small and medium sized hospitals than in large ones (P<0.001). In 19 ICUs, one nurse cared for four or more patients.
Table 3.
Physician and nurse staffing of ICUs
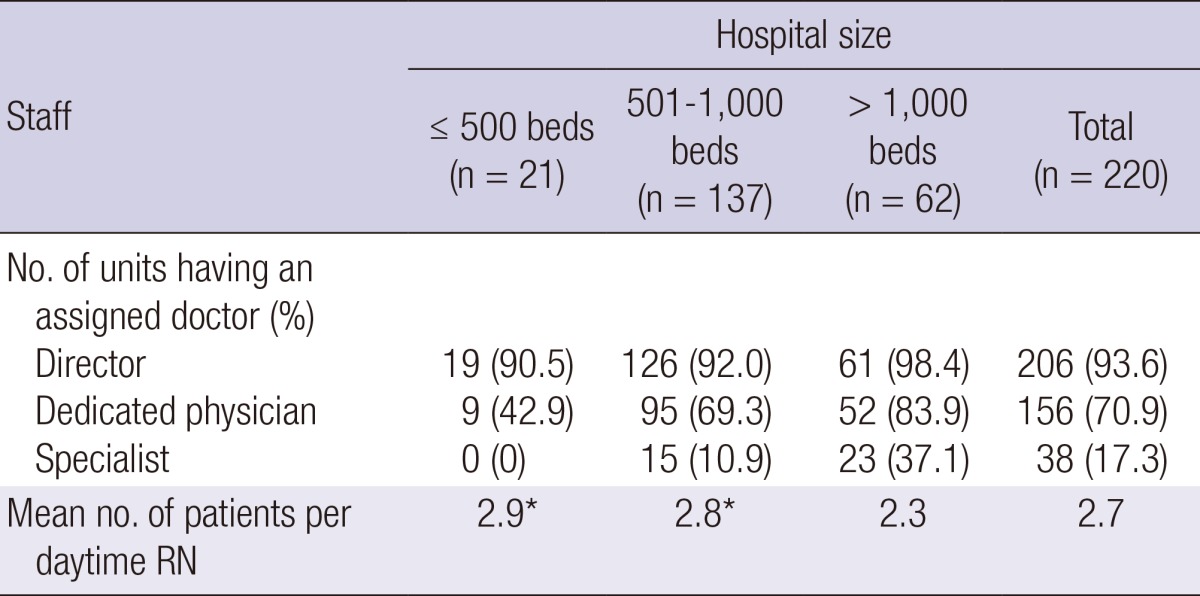
n, number of units. *P<0.001 compared with hospitals with more than 1,000 beds. One-way ANOVA, Tukey HSD post-hocanalysis.
Fig. 1.

Percentage of ICUs having an assigned doctor. CCU, coronary care unit.
Available technology in the ICUs
A picture archiving communication system was available in 98.6% of the ICUs and electronic medical records were available in 49.1% (Table 4). Local arterial blood gas analysis monitoring was available in 61.4% of the ICUs and a local patient information database was available in 71.4% of the ICUs. The number of ventilators and monitors per bed were 0.66 and 1.10, respectively.
Table 4.
Technologies available in the ICU
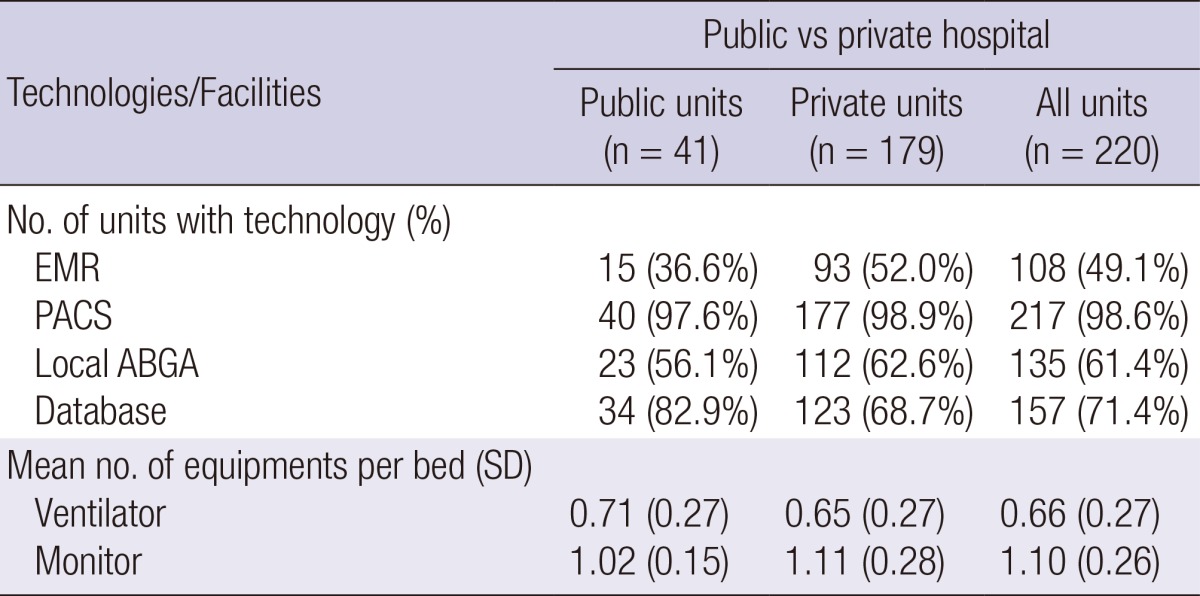
There was no difference between public and private hospitals.
Characteristics of ICU patients
Table 5 shows the demographic and clinical characteristics of 3,197 patients in the ICUs. The mean age of the adult patients was 60 yr. The age distribution of ICU patients differed with hospital size; the percentage of elderly patients over 65 yr of age was higher in smaller than in larger hospitals (Fig. 2). The most common ICU admission was from the emergency room. The most common reasons for ICU admission were respiratory insufficiency (20.2%) and postoperative management (12.8%) among adults, and prematurity (56.4%) followed by respiratory insufficiency (13.6%) among children (Table 6). Central venous catheterization was the most common intervention (43.4%) (Table 7). Pulmonary artery catheterization was only done in 1.2% of the units, most often in surgical and CCUs. All interventions were performed more frequently in larger hospitals.
Table 5.
Demographic and clinical characteristics of 3,197 ICU patients in 86 Korean hospitals
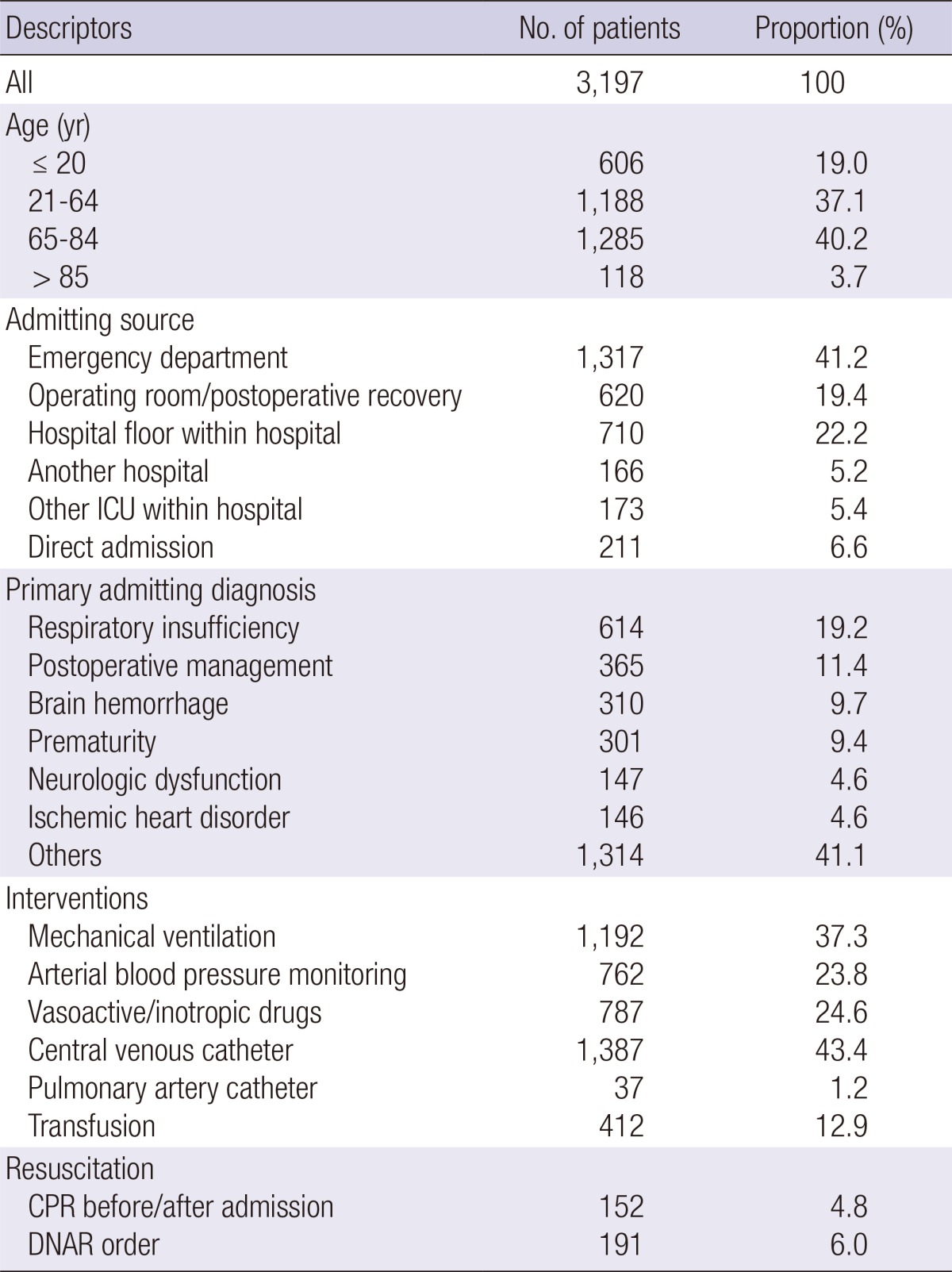
Fig. 2.

Percentage of elderly patients depending on the hospital size. There was a significant association between the percentage of elderly patients and the hospital size (P < 0.001). Data from pediatric ICU were excluded. P values were calculated by the linear-by-linear chi-square test.
Table 6.
Primary admitting diagnosis
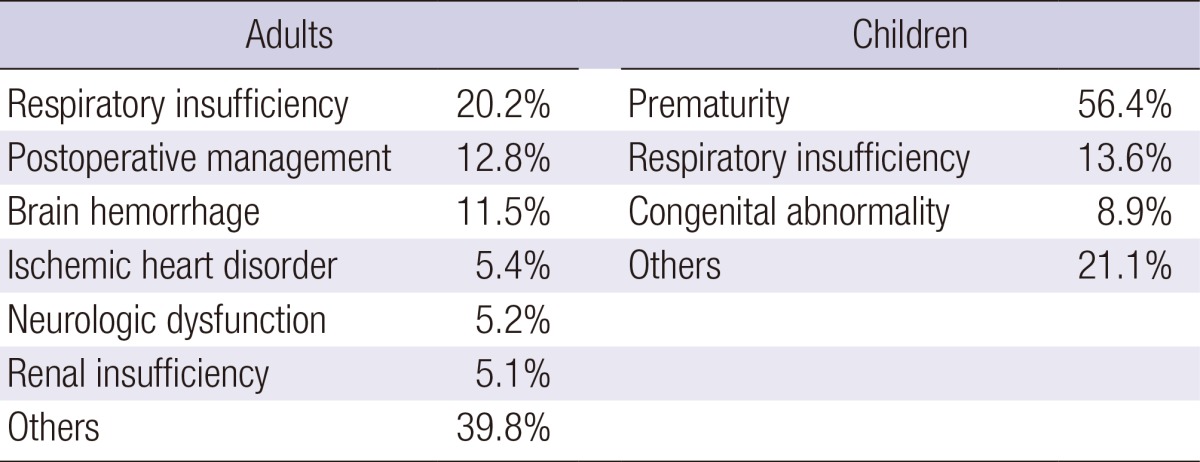
Table 7.
ICU interventions depending on the hospital size
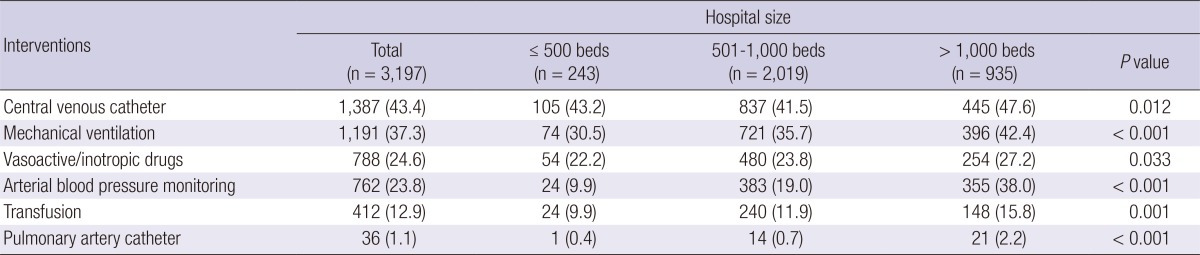
There was a significant association between ICU interventions and the hospital size. P values were calculated by the linear-by-linear Chi-square test.
The mean percentage of patients receiving CPR before or after ICU admission was 4.8%, and a mean of 6.0% of patients had "do not attempt resuscitation" orders (Table 8). These percentages were significantly higher in medical ICUs than in other types of ICU, and also in smaller hospitals compared to larger ones.
Table 8.
Resuscitation history and do not attempt resuscitation status depending on ICU type and hospital size

DISCUSSION
In 2009, there were a total of 975 ICUs and 10,446 ICU beds in Korea, according to data from the National Health Insurance Corporation. The estimated 17 adult ICU beds per 100,000 populationis comparable to other advanced countries (2). Besides medical infrastructure, we are confident that our medical science and technology has grown to a level nearly the equal as that in advanced countries. However, we cannot say that the management and the outcomes in critical care units have reached the same levels as in advanced countries. In a multicenter retrospective analysis of 1090 ICU patients from 18 hospitals with 500-2,200 beds, the overall mortality rate was 24% (3). Considering that those were relatively large hospitals, it is apparent that our mortality rate is worse than that of advanced countries (2). It is clear that there are substantial differences among countries in clinical performance, medical resources, and national spending on health-care. Nevertheless, our findings and their implications raise some serious issues, which may account for this poor outcome.
First, the mean daytime nurse-to-patient ratio was 1:2.7 in this survey, and varied from 1:2.9 in small hospitals to 1:3.2 in mixed ICUs. One nurse provided care for more than four patients in 19 of the surveyed units. This situation could become worse at night due to decreased personnel on night shifts, as often occurs in the open ward setting. Moreover, because there are very few respiratory therapists in Korea, overall bedside duties of ICU nurses are increased, with a corresponding loss of quality of patient care. The increasing need for critical care beds, combined with decreasing budgets and nurse shortages, might lead to inadequate staffing and compromised patient safety in hospitals worldwide. Many studies have demonstrated a relationship between decreased nurse staffing levels and increased adverse patient outcomes in the ICU, including mortality, infection, and pressure ulcers (4-8). To overcome these problems, minimum standards of nurse staffing levels adopted by of critical care nurses associations (9, 10) have resulted in nurse-to-patient ratios of 1:1 or 1:2 in many advanced countries (11, 12).
Second, physician staffing is a serious problem for Korean critical care. In this survey, 70.9% of ICUs had dedicated physicians who worked more than 8 hr a day. That result does not seem bad, but most of the physicians were not intensivists or specialists. Only 7.7% of adult ICUs were staffed by physician specialists for 5 days each week. The outcome of severe sepsis and compliance with the Surviving Sepsis Campaign in Korea was poor in ICUs without fulltime intensivists (1). In several studies that evaluated the association between ICU physician staffing and patient outcomes, higher staffing of intensivists was associated with lower hospital mortality and morbidity (13-17). Furthermore, a new paradigm for 24-hr intensivist coverage in the ICU has emerged recently because of its impact on patient outcomes (18, 19). Staffing with intensivists may also decrease resource use because specialists may be better at reducing inappropriate ICU admissions, preventing complications that prolong length of stay, and recognizing opportunities for prompt discharge. Intensivists take primary responsibility in managing the critically ill patients in the ICUs of many advanced countries (20, 21).
Third, the deficiencies in nurse and physician staffing are related to an unreasonable health insurance reimbursement system and an inappropriate medical law in Korea. Currently, the reimbursement rates are estimated to support only 30%-50% of the original critical care cost. For this reason, most Korean ICUs operate at a deficit, and hospitals tend to avoid further investment in the human resources of their ICUs. Furthermore, Korean medical legislation mandates that neonatal ICUs, but not necessarily adult ICUs, must have dedicated specialists. Our findings show that advanced computer technologies are frequently adopted, with picture archiving communication system available in 98.6% of the surveyed ICUs. However, only 38 ICUs (17.3%) have specialists on duty for 5 days each week.
Korea is categorized as an aging society and is rapidly becoming an aged society. When data from pediatric ICUs were excluded, 53% of the adult patients in this study were elderly people (≥65 yr of age). As the population continues to age, the burden of acute and chronic illness and the demand for critical care services will rise (22). This study shows that critically ill patients may not be treated by the best equipped health-care professionals, even in large hospitals and teaching institutions. The situation in smaller, non-academic hospitals would be expected to be worse. The quality and patient outcome in critical care will worsen over time if current critical care practices remain unchanged. In 2008, as the only organization representing all professional components of critical care in Korea, the KSCCM introduced a subspecialty system for critical care medicine after 6 yr of discussion with other medical societies including those concerned with anesthesiology, emergency medicine, internal medicine, neurology, neurosurgery, pediatrics, surgery, and thoracic surgery. We anticipate that this system will increase the supply of qualified intensivists and will improve quality, efficiency, and outcomes of critical care in Korea. To implement this system, policy makers need to understand the current problems and improve critical care policy, including critical care cost and medical law.
We recognize that our study has several limitations. Our sample size was small, which limited the precision of the results. In addition, the survey was targeted to critical care subspecialty training hospitals instead of using a stratified random sampling method. Thus, the results may not provide a full description of critical care delivery in Korea. However, the results do increase our understanding of the current situation and problems in Korean ICUs. Second, more than half of ICUs in this study were located in the capital region, which occupies only 12% of the area of the country but houses about 50% of the Korea's population and medical institutions. Consequently, we did not need to adjust for these factors when analyzing the results. A third limitation is that we did not include mortality and complications data from each unit in the estimate of the ICUs quality of care. This study could be viewed as the first step in building a Korean critical care database, with more detailed morbidity and mortality data to be collected in the future.
In conclusion, we have described the organization and staffing of ICUs in Korean university and teaching hospitals, and characteristics of admitted patients. The data collected in this survey indicate that staffing of nurses and physiciansis poor compared with that in advanced countries. We believe that the roles of health-care professionals are important, and much effort including enhanced reimbursement of critical care costs must be made to improve the quality of critical care at the national level.
ACKNOWLEDGMENTS
We thank staffs of the participating hospitals, which included The Catholic University (Univ.) of Korea Daejeon St. Mary's Hospital; The Catholic Univ. of Korea Seoul St. Mary's Hospital; The Catholic Univ. of Korea Bucheon St. Mary's Hospital; The Catholic Univ. of Korea St. Paul's Hospital; The Catholic Univ. of Korea St. Vincent's Hospital; The Catholic Univ. of Korea Uijeongbu St. Mary's Hospital; Gangnam Severance Hospital; Kangbuk Samsung Hospital; Kangwon National Univ. Hospital; Konkuk Univ. Hospital; Konkuk Univ. Chungju Hospital; Konyang Univ. Hospital; Kyungpook National Univ. Hospital; Gyeongsang National Univ. Hospital; Kyunghee Univ. Medical Center; Keimyung Univ. Dongsan Medical Center; Korea Univ. Guro Hospital; Korea Univ. Ansan Hospital; Korea Univ. Anam Hospital; Kosin Univ. Gospel Hospital; Kwandong Univ. Myongji Hospital; Kwangju Christian Hospital; National Police Hospital; National Cancer Center; National Medical Center; NHIS Ilsan Hospital; Dankook Univ. Hospital; Daegu Catholic Univ. Medical Center; Daegu Fatima Hospital; Daedong Hospital; Sun Medical Center; Dongkang Medical Center; Dongguk Univ. Ilsan Hospital; Dongsuwon General Hospital; Samsung Changwon Hospital; Maryknoll Medical Center; Jungang General Hospital; Pusan National Univ. Hospital; Busan St. Mary's Hospital; Seoul National Univ. Bundang Hospital; Daejin Medical Center; Samsung Medical Center; Seoul National Univ. Hospital; Asan Medical Center; SMG-SNU Boramae Medical Center; Sunlin Hospital Handong Univ.; St. Carollo Hospital; Soonchunhyang Univ. Hospital Gumi; Soonchunhyang Univ. Hospital Bucheon; Soonchunhyang Univ. Hospital Cheonan; Severance Hospital; Ajou Univ. Hospital; Andong Medical Group; Wonju Severance Christian Hospital; Yeungnam Univ. Hospital; Presbyterian Medical Center; Wallace Memorial Baptist Hospital; Ulsan Univ. Hospital; Wonwang Univ. Sanbon Hospital; Wonwang Univ. Hospital; Korea Institute of Radiological & Medical Sciences; Eulji Medical Center; EwhaWomans Univ. Medical Center; Inje Univ. Seoul Paik Hospital; Inje Univ. Busan Paik Hospital; Inje Univ. Sanggye Paik Hospital: Inje Univ. IlsanPaik Hospital; Inha Univ. Hospital; Chonnam National Univ. Hospital; Chonbuk National Univ. Hospital; Jeju National Univ. Hospital; With Cheju Halla General Hospital; Chosun Univ. Hospital; ChungAng Univ. Hospital; Changwon Fatima Hospital; Cheongju St. Mary's Hospital; Chungnam National Univ. Hospital; Chungbuk National Univ. Hospital; Bundangcha Hospital; Hallym Univ. Medical Center; Hanyang Univ. Guri Hospital; Hangyang Univ. Hospital; Kepco Medical Center; Haedong Hospital; Chonnam National Univ. Hwasun Hospital.
Footnotes
This study was performed under auspices of the Korean Society of Critical Care Medicine.
No author received financial support and there are no potential conflicts of interest for any authors.
References
- 1.Kim JH, Hong SK, Kim KC, Lee MG, Lee KM, Jung SS, Choi HS, Lee JH, Jung KS, Lee SS, et al. Influence of full-time intensivist and the nurse-to-patient ratio on the implementation of severe sepsis bundles in Korean intensive care units. J Crit Care. 2012;27:414.e11–414.e21. doi: 10.1016/j.jcrc.2012.03.010. [DOI] [PubMed] [Google Scholar]
- 2.Wunsch H, Angus DC, Harrison DA, Collange O, Fowler R, Hoste EA, de Keizer NF, Kersten A, Linde-Zwirble WT, Sandiumenge A, et al. Variation in critical care services across North America and Western Europe. Crit Care Med. 2008;36:2787–2793.e1-9. doi: 10.1097/CCM.0b013e318186aec8. [DOI] [PubMed] [Google Scholar]
- 3.Kang CH, Kim YI, Lee EJ, Park K, Lee JS, Kim Y. The variation in risk adjusted mortality of intensive care units. Korean J Anesthesiol. 2009;57:698–703. doi: 10.4097/kjae.2009.57.6.698. [DOI] [PubMed] [Google Scholar]
- 4.Stone PW, Mooney-Kane C, Larson EL, Horan T, Glance LG, Zwanziger J, Dick AW. Nurse working conditions and patient safety outcomes. Med Care. 2007;45:571–578. doi: 10.1097/MLR.0b013e3180383667. [DOI] [PubMed] [Google Scholar]
- 5.Cho SH, Hwang JH, Kim J. Nurse staffing and patient mortality in intensive care units. Nurs Res. 2008;57:322–330. doi: 10.1097/01.NNR.0000313498.17777.71. [DOI] [PubMed] [Google Scholar]
- 6.Sales A, Sharp N, Li YF, Lowy E, Greiner G, Liu CF, Alt-White A, Rick C, Sochalski J, Mitchell PH, et al. The association between nursing factors and patient mortality in the Veterans Health Administration: the view from the nursing unit level. Med Care. 2008;46:938–945. doi: 10.1097/MLR.0b013e3181791a0a. [DOI] [PubMed] [Google Scholar]
- 7.Blot SI, Serra ML, Koulenti D, Lisboa T, Deja M, Myrianthefs P, Manno E, Diaz E, Topeli A, Martin-Loeches I, et al. Patient to nurse ratio and risk of ventilator-associated pneumonia in critically ill patients. Am J Crit Care. 2011;20:e1–e9. doi: 10.4037/ajcc2011555. [DOI] [PubMed] [Google Scholar]
- 8.Hugonnet S, Uckay I, Pittet D. Staffing level: a determinant of late-onset ventilator-associated pneumonia. Crit Care. 2007;11:R80. doi: 10.1186/cc5974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bray K, Wren I, Baldwin A, St Ledger U, Gibson V, Goodman S, Walsh D. Standards for nurse staffing in critical care units determined by: the British Association of Critical Care Nurses, the Critical Care Networks National Nurse Leads, Royal College of Nursing Critical Care and In-flight Forum. Nurs Crit Care. 2010;15:109–111. doi: 10.1111/j.1478-5153.2010.00392.x. [DOI] [PubMed] [Google Scholar]
- 10.Hartigan RC. The Synergy Model: establishing criteria for 1:1 staffing ratios. Crit Care Nurse. 2000;20:112, 114–116. [PubMed] [Google Scholar]
- 11.Sirio CA, Tajimi K, Taenaka N, Ujike Y, Okamoto K, Katsuya H. A cross-cultural comparison of critical care delivery: Japan and the United States. Chest. 2002;121:539–548. doi: 10.1378/chest.121.2.539. [DOI] [PubMed] [Google Scholar]
- 12.Mallick R, Strosberg M, Lambrinos J, Groeger JS. The intensive care unit medical director as manager: impact on performance. Med Care. 1995;33:611–624. doi: 10.1097/00005650-199506000-00004. [DOI] [PubMed] [Google Scholar]
- 13.Pronovost PJ, Angus DC, Dorman T, Robinson KA, Dremsizov TT, Young TL. Physician staffing patterns and clinical outcomes in critically ill patients: a systematic review. JAMA. 2002;288:2151–2162. doi: 10.1001/jama.288.17.2151. [DOI] [PubMed] [Google Scholar]
- 14.Treggiari MM, Martin DP, Yanez ND, Caldwell E, Hudson LD, Rubenfeld GD. Effect of intensive care unit organizational model and structure on outcomes in patients with acute lung injury. Am J Respir Crit Care Med. 2007;176:685–690. doi: 10.1164/rccm.200701-165OC. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Dimick JB, Pronovost PJ, Heitmiller RF, Lipsett PA. Intensive care unit physician staffing is associated with decreased length of stay, hospital cost, and complications after esophageal resection. Crit Care Med. 2001;29:753–758. doi: 10.1097/00003246-200104000-00012. [DOI] [PubMed] [Google Scholar]
- 16.Pronovost PJ, Jenckes MW, Dorman T, Garrett E, Breslow MJ, Rosenfeld BA, Lipsett PA, Bass E. Organizational characteristics of intensive care units related to outcomes of abdominal aortic surgery. JAMA. 1999;281:1310–1317. doi: 10.1001/jama.281.14.1310. [DOI] [PubMed] [Google Scholar]
- 17.Suarez JI, Zaidat OO, Suri MF, Feen ES, Lynch G, Hickman J, Georgiadis A, Selman WR. Length of stay and mortality in neurocritically ill patients: impact of a specialized neurocritical care team. Crit Care Med. 2004;32:2311–2317. doi: 10.1097/01.ccm.0000146132.29042.4c. [DOI] [PubMed] [Google Scholar]
- 18.Gajic O, Afessa B, Hanson AC, Krpata T, Yilmaz M, Mohamed SF, Rabatin JT, Evenson LK, Aksamit TR, Peters SG, et al. Effect of 24-hour mandatory versus on-demand critical care specialist presence on quality of care and family and provider satisfaction in the intensive care unit of a teaching hospital. Crit Care Med. 2008;36:36–44. doi: 10.1097/01.CCM.0000297887.84347.85. [DOI] [PubMed] [Google Scholar]
- 19.Haupt MT, Bekes CE, Brilli RJ, Carl LC, Gray AW, Jastremski MS, Naylor DF, PharmD MR, Md AS, Wedel SK, et al. Guidelines on critical care services and personnel: recommendations based on a system of categorization of three levels of care. Crit Care Med. 2003;31:2677–2683. doi: 10.1097/01.CCM.0000094227.89800.93. [DOI] [PubMed] [Google Scholar]
- 20.Judson JA, Fisher MM. Intensive care in Australia and New Zealand. Crit Care Clin. 2006;22:407–423. doi: 10.1016/j.ccc.2006.03.012. [DOI] [PubMed] [Google Scholar]
- 21.Offenstadt G, Moreno R, Palomar M, Gullo A. Intensive care medicine in Europe. Crit Care Clin. 2006;22:425–432. doi: 10.1016/j.ccc.2006.03.007. [DOI] [PubMed] [Google Scholar]
- 22.Angus DC, Kelley MA, Schmitz RJ, White A, Popovich J, Jr Committee on Manpower for Pulmonary and Critical Care Societies (COMPACCS) Caring for the critically ill patient: current and projected workforce requirements for care of the critically ill and patients with pulmonary disease: can we meet the requirements of an aging population? JAMA. 2000;284:2762–2770. doi: 10.1001/jama.284.21.2762. [DOI] [PubMed] [Google Scholar]