

Abstract
The failures of root canal preparation are due to some anatomical deviation (canal in “C” or “S”) and some technique errors. The technique errors are usually present in canal root cleansing and shaping stage and are the result of endodontic treatment objectives deviation. Objectives: Our study was made on technique errors while preparing the canal roots with hand ProTaper. Methodology: Our study was made “in vitro” on 84 extracted teeth (molars, premolars, incisors and canines). The canal root of these teeth were cleansed and shaped with hand ProTaper by crown-down technique and canal irrigation with NaOCl(2,5%). The dental preparation control was made by X-ray. Results: During canal root preparation some failures were observed like: canal root overinstrumentation, zipping and stripping phenomenon, discarded and/or fractured instruments. Conclusions: Hand ProTaper represents a revolutionary progress of endodontic treatment, but a deviation from accepted rules of canal root instrumentation can lead to failures of endodontic treatment.
Keywords: root canal, technique errors, ProTaper
Introduction
Hand ProTaper instruments represent a revolutionary breakthrough when it comes to mechanical treatment of root canals. It has some advantages compared with those of steel or nickel-titanium due to its convex triangular cross-sectional shape, its tip designed for guiding and the fact that its helical angle and slope are variable [1],[2],[3].
For increased efficiency and avoidance of failures regarding root canals instrumentation with hand ProTaper one must follow several basic principles, the so-called "golden rules":
-achieve access to the root canal axis;
- perform initial permeability of the root canal manually with a steel needle K-file, with easy progressive passive movements;
- widen the canal entering carefully, using Gates Glidden drills;
- use only tools for well irrigated and lubricated channels (Glyde, sodium hypochlorite);
- control frequently the turns by notifying the distortion area;
- use tools only for recommended movement;
- it is contraindicated to force the needle into the root canal [4],[5],[6].
In order to use hand ProTaper during endodontic treatment it is indicated to perform several special movements:
Easy needle penetration in dentin by turning clockwise;
Release of the needle by rotating counterclockwise 45-90 degrees;
Cut of dentin by turning clockwise while withdrawing the needle;
Repeat these movements until reaching the desired length;
Depending on the root canal anatomy, hand ProTaper needle can be used in a reciprocal movement back and forth [5],[7].
Those precurved hand ProTaper needles represent instruments of choice for the treatment of root canals which presents anatomical difficulties, thresholds or internal resorbtion [8].
During root canals instrumentation, the failures that may occur are due both to anatomical aberrations (channels C or S) and procedural errors. The latter frequently occur during root canal cleansing and shaping, the result being deviation from the principles of endodontic treatment [4],[8].
Materials and methods
Our study was conducted within the Department of Endodontic of Faculty of Dental Medicine, University Craiova, in vitro, on a total of 84 extracted teeth (mono and pluriradicular): 42 front teeth, 23 premolars and 19 molars.
We have prepared the access cavity and permeable root canals with Kerr needle number 10 (purple) or number 15 (white).
We set the length of these channels using Kerr needles number 15. Mechanical channel treatment was performed with hand ProTaper, through crown-down technique, following the sequence of those needles, according to the manufacturer.
Preparation steps were accompanied by abundant irrigation of canals with sodium hypochlorite (2.5%).
After using each hand ProTaper needle and after penetrating the canal with the precurved needle, in case of curved canals, we used needles Kerr number 10 for removing the remaining intracanal debris.
Using X-ray, we checked the accuracy of mechanical preparation for the root canals. In this study we stopped on procedural errors that occur due to changes of working length that is overinstrumentation and underinstrumentation of root canals.
Matherial and Method
Our study was conducted within the Department of Endodontic of Faculty of Dental Medicine, University Craiova, in vitro, on a total of 84 extracted teeth (mono and pluriradicular): 42 front teeth, 23 premolars and 19 molars.
We have prepared the access cavity and permeable root canals with Kerr needle number 10 (purple) or number 15 (white).
We set the length of these channels using Kerr needles number 15. Mechanical channel treatment was performed with hand ProTaper, through crown-down technique, following the sequence of those needles, according to the manufacturer.
Preparation steps were accompanied by abundant irrigation of canals with sodium hypochlorite (2.5%).
After using each hand ProTaper needle and after penetrating the canal with the precurved needle, in case of curved canals, we used needles Kerr number 10 for removing the remaining intracanal debris.
Using X-ray, we checked the accuracy of mechanical preparation for the root canals. In this study we stopped on procedural errors that occur due to changes of working length that is overinstrumentation and underinstrumentation of root canals.
Results and Discussion
Subinstrumentation of root canal is the procedural error in which the needle will act on a shorter length than the one established by odontometry, having as a result an obstruction of the root canal which does not reach the apical level [9],[10].
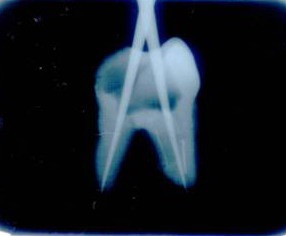
In the study (Fig.1), subinstrumentation appeared where the rules were not respected regarding the preparation of the root canals, namely:
Fig.1.

Underinstrumentation of root canal – observation of incomplete aspect of canal obstruction at the level of mesial root
Errors in determining the initial working length;
Insufficient permeability of root canal with Kerr needle number 10;
Insufficient use of canal irrigation with sodium hypochlorite;
Deliberate action for a short period of time for the hand ProTaper needles, on the canal, without taking into consideration the originally established working length.
Also, other procedural errors leading to subinstrumentation are represented by the obliteration of the root canal at apex with dentin chips or broken tools.
We found that the obliteration of the canal with foreign bodies or dentin chips is the result of:
Compaction of dentin chips (smear layer, dentine fragments);
Compaction of tissue debris;
Transport of particles of restorative material from the pulp chamber.
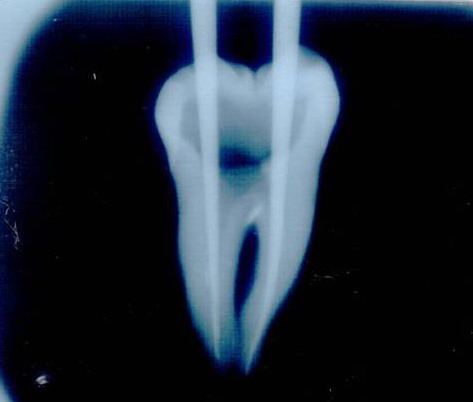
Obliteration with hand Proteper instruments (Fig.2) or Kerr number 10 needles used for root canal permeability (Fig. 3) that were broken inside the canal was the result of:
Fig.2.


Canal obliteration with Pro Taper hand instruments
Excessive pressure or rotation maneuvers;
Attempts to withdraw with a strong rotation counterclockwise;
Use of hand ProTaper needles or Kerr in distortion areas.
As a result of an inadequate treatment, prominent thresholds were established on the wall surface.
Thus, the access of instrument to the apex was made difficult, sometimes leading to the creation of a false canal path.
The appearance of thresholds in the canal wall was made possible by:
Inserting un precurved instruments in curved root canals;
Using a hand ProTaper needle shorter than previously established working length;
Applying apical excessive pressure during insertion or instrumentation of a root canal.
Fig.3.

Canal obliteration with Kerr needle
Throughout the study there were cases of overinstrumentation of the root canals, cases in which the needles had exceeded the apical constriction.
During radiological examination, we could see the master cone, which exceeded the root apex. (Fig.4)
Fig.4.

Overinstrumentation of root canal by exceeding apical constriction
Conclusions
Although hand ProTaper instruments represent a revolutionary advance in endodontic treatment, deviation from the principles of mechanical treatment may have a negative effect on prognosis and success rate of treatment.
The use of needles with evident distortions as well as improper handling of them by practitioners can have a negative effect on prognosis and success rate of canal treatment.
References
- 1.Ankrum MT, Hartwell GR, Truitt JE. Endo ProTaper and Profile systems : breakage and distortion in severely curved roots of molars. Journal of Endodontics. 2004;30:234–237. doi: 10.1097/00004770-200404000-00013. [DOI] [PubMed] [Google Scholar]
- 2.Kuhn G, Jordan L. Fatigue and mechanical properties of nickel titanium endodontic instruments. Journal of Endodontics. 2002;28:716–720. doi: 10.1097/00004770-200210000-00009. [DOI] [PubMed] [Google Scholar]
- 3.Peng B, et al. Defects in ProTaper S1 instruments after clinical use : longitudinal examination. International Endodontic Journal. 2005;38:550–557. doi: 10.1111/j.1365-2591.2005.00991.x. [DOI] [PubMed] [Google Scholar]
- 4.Ruddle CJ. Cleaning and shaping the root canal system. In: Cohen S., Burns RC, editors. Pathway of the pulp. 8. St. Louis: Mosby-Year Book; 2002. [Google Scholar]
- 5.Ruddle CJ. The ProTaper technique. Endod Topics. 2005;10:187–190. [Google Scholar]
- 6.Sonntag D, Delschen S, Stachnis V. Root canal shaping with manual and rotary Ni-Ti files performed by students. International Endodontic Journal. 2003;36:715–723. doi: 10.1046/j.1365-2591.2003.00703.x. [DOI] [PubMed] [Google Scholar]
- 7.Ruddle CJ. Shaping for success. Everything old is new again. Dentistry today. 2006;25(4):120–127. [PubMed] [Google Scholar]
- 8.Spili P, et al. The impact of instrument fracture on endodontic treatment. Journal of Endodontics. 31(12):845–850. doi: 10.1097/01.don.0000164127.62864.7c. [DOI] [PubMed] [Google Scholar]
- 9.Smadi L. Comparison between two methods of working length determination and its effect on radiographic extent of root canal filling : a clinical study. BMC Oral Health. 2006;6(4):1–6. doi: 10.1186/1472-6831-6-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Veltri M, Mollo A, et al. In vitro comparision of shaping abilities of ProTaper and GT rotary files. J Endod. 2004;30:163–166. doi: 10.1097/00004770-200403000-00009. [DOI] [PubMed] [Google Scholar]