

Abstract
Dental occlusion represent the function of dentomaxillary system at which realization participate all the components of that system holding the equilibrium between them. Setting up the treatment with dental bridges in partial edentuluous is rule by some principles that have aims like restore the morphology and functions change by edentuluous condition and also prevention disorders of remaining teeth and other structures and functions of dentomaxillary system. During the prosthetic treatment with fixed bridgeworks in clinical cases presents in this study , we used also terapeutical techniques specifically other dental domains like endodontology and oral surgery. For avoid the appearance of occlusal dysfunction is necessary a good knowledge and respecting the biomorphocinematic behaviour of dentomaxillary system structure under action of occlusal force during mastication and also biomechanical rules that influence the functional equilibrium of teeth and dental bridges.
Keywords: dental occlusion, corono-radicular amputation, functional equilibrium
Introduction
Dental bridges require additional reliance on the support teeth as they are individually solicitated by the occlusal forces. The removal of one root of a pluriradicular teeth through root amputation or root-coronary one reveals a delicate situation regarding the value of dental-periodontal support for the tooth. This forces us to reconsider the functional conditions of equilibrium for these teeth. By applying dental bridge, the support teeth will form a new functional complex, subject to other conditions of stress and strength than those exerted for unused teeth as support elements for bridges. This requires knowledge of two categories of factors: overload factors for the support teeth and factors that can enhance the resistance forces of these teeth.
Matherial and Method
23 patients were examined for the study aged between 23-47 years with low partial edentulous, interspersed mandibulary with prosthesis or without. Patients had subjective complaints regarding their pluriradicular remaining teeth, which in turn were subjected to radiological examination (dental and periodontal wide).We studied the coronary condition of the periodontium, the degree of deployment and mobility of the remaining teeth, the precision or failure of the endodontic treatment. Biometrics for the diagnosed models was performed to determine the value of local biological indices.
The conservation of any given tooth from the side is a goal because it prevents the transformation of side edentulous into terminal edentulous, with all its difficulties for prosthesis.
The preservation method used for the lateral molars in this study is called root-coronary amputation and consists of removing one of the affected roots with its coronal portion.
The clinical case is representative for coronary-root amputation technique at the lower molars. Patient aged 24 years, presents pulsatile pain during mastication at the level of 37. After performing a retroalveolar dental radiography, we found no endodontic treatment in the mesial root and the existence of a chronic apical periodontitis at this level (fig.1). The distal root is treated correctly from an endodontic point of view.
Fig.1.

Initial X-ray of 37.
In order to avoid extracting it, which would lead to the transformation of side edentulous into terminal edentulous, I decided to remove the mesial root using the root-coronary amputation and preserve the distal root in the form of a sustaining teeth.
We explain to patient what represent the coronary-root amputation technique and he has accepted the remove of mesial root.
In a first phase we performed the ablation of the old dental bridge and created a space of occlusion of several millimeters at the level of 37. This space has two purposes: to avoid overloading the remaining root and to prevent fracturing the remaining coronal portion for the root that is to be extracted.
It is followed by sectioning the coronary portion which represents achieving a vestibulo-oral incision that must intersect the root network, but without being interested in the intraradicular bone septum, which is the main osteogenetic factor at this level (fig.2).
Fig.2.
The section of crown
Root luxation for the root which is to be removed is made with vestibulo-oral movements and using curets, we removed all the chronic inflammatory tissue and we irrigated the socket with sterile saline solution. Alveolar wound is sutured, thus hastening the bone remineralization process.
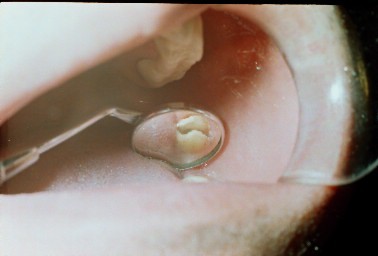
The sutured of alveolar wound was realized with two separated thread for ten days. After that, the stitches are removed and the coronal portion of the remaining root is prepared under the form of a bont (fig.3).
Fig.3.

Modified of 37 form as premolar
After surgery we applied at patient the follow-up procedures about six weeks for periodontal and endodontic treatment and than we made the final prosthetic restoration (Fig. 4). Premature removal of contacts and occlusal interferences by selective grinding can be done both after the stage of temporary prosthesis or after final prosthesis.
Fig.4.

Final prosthetic restoration
Results and discussion
Removing one of the roots of a tooth bridge sustainer raises two points of view regarding its prosthesis: a decrease in the dent- periodontal resistance of dental bridge sustainer and vulnerability of dental bridge balance and stability.
In the process of mastication, through the process of jaw muscle contraction, occlusal forces can occur, which act on the teeth as individual chewing units and tend to move them in relation to the initial position of implantation in the dental alveoli [7]. These occlusal forces have a relatively constant value during life, in condition of natural teeth, and their value is lower in patients carrying total or partial prothesis[11]. The forces that oppose occlusal forces, which are meant to keep the natural teeth in position, after the cessation of occlusal forces, are called reactional forces[7]. The balanced interaction between occlusal functional forces and resistance ones maintain the functional equilibrium position or kinematic one for the teeth[7].
In case of partially reduced edentulous the prosthetic restoration of functional equilibrium is done using dental bridges, whose architectural and structural balance should harmonize with the functional balance of the support teeth[1]. The existence of a low partial mandible edentulous, in which there is a single distal tooth for support which undergoes a prosthetic intervention, as coronary-root amputation is, without the possibility of supplementing the support teeth in the distal area, certain measures should be considered in order to prevent an overloading of the remaining distal root[9]. Thus, by provisional prosthesis, the practitioner obtains an immobilization of the remaining distal root and through the occlusal forces action an active response reaction of these root is also obtained[2].
The architecture and the design of the dental bridge will be done in such a way as to avoid overloading the distal root, but respecting the occlusal morphology and reducing the vestibulo-oral size of this bridge[6][9]. An important role has the occlusal equilibration step for removing premature contacts and occlusal interferences thus preventing the phenomenon of occlusal trauma[10]. The overall goal of selective tooth grinding and fullmouth equilibration is to develop a state of homeostasis between the tissues that interact within the masticatory system and the local environmental factors[5]. This modification process can help to establish a functional equilibrum between the teeth, supporting tissues, neuromuscular system and temporomandibular joint5. It is generally agreed that when occlusal adjustment is performed to treat abnormal tooth mobility, periodontal therapy has a more favorable outcome, with the clinical attachment level reportedly being improved in some cases[3][4][5][8]
Conclusions
In case of low bridges, the use of a single tooth as a distal support, with coronary-root amputation is done taking into account: root morphology, mobility, crown-root ratio and tooth position on the arch. Use of the aggregation elements on both divergent or convergent roots, requires time to analyze possible effects on periodontal tooth support involved.
Project the body bridge which should be contained within the perimeter shape of the teeth horizontal bases of support. Develop occlusal contacts capable of providing stimuli favorable for periodontal tooth support. The occlusal equilibration phase is mandatory, it can be achieved both in the phase of provisional prosthesis or final prosthesis.
Refernces
- 1.Ackermann F. Le méchanisme des mâchoires. Paris: Ed Masson et C-ie; 1953. pp. 430–443. [Google Scholar]
- 2.Arens ED, et al., editors. Practical Lessons in Endodontic Surgery. London: Quintessence Publishing Co, Inc; 1998. pp. 191–197. [Google Scholar]
- 3.Burgett FG, Nissle RR, Morrison EC, et al. A randomiyed occlusal adjustment in periodontitis patiens. J Clin periodontal. 1992;19:281–287. doi: 10.1111/j.1600-051x.1992.tb00666.x. [DOI] [PubMed] [Google Scholar]
- 4.Caffesse R. Management of periodontal disease with occlusal abnormalities. Dent Clin North Am. 1980;24:215–230. [PubMed] [Google Scholar]
- 5.Charles Mc N. Science and Practice of Occlusion. London: Quintessence Publishing Co, Inc; 1997. pp. 404–420. [Google Scholar]
- 6.Kois J. C., Spear F. M. Periodontal prosthesis: Creating successful restorations. J Am Dent Assoc. 1992;123:108–113. doi: 10.14219/jada.archive.1992.0269. [DOI] [PubMed] [Google Scholar]
- 7.Popa S. Protetică Dentară. Bucuresti: Edit. Medicală; 2001. pp. 87–134. [Google Scholar]
- 8.Ramfjord S. P., Ash M. M. Signifiance of occlusion in the etiology and treatment of early, moderate and advanced periodontitis. J Periodontol. 1981;52:511–515. doi: 10.1902/jop.1981.52.9.511. [DOI] [PubMed] [Google Scholar]
- 9.Shillingburg H. T. Jr., et al. Fundamentals of fixed prosthodontics. 3. London: Quintessence Publishing Co, Inc; 1997. pp. 212–222. [Google Scholar]
- 10.Standlee J. P., Caputo A. A. Load transfer by fixed partial dentures with three abutments. Quintessence Int. 1988;19:403–410. [PubMed] [Google Scholar]
- 11.Tillitson E. W., Craig R. W., Peyton F. A. Experimental stress analysis of fixed partial dentures by use of dynamic method. J. Dent . Res. 1971;50:422–429. doi: 10.1177/00220345710500025201. [DOI] [PubMed] [Google Scholar]