

Abstract
Background:
Cytological reports of ameloblastoma are relatively rare in the literature. Appropriate cytologic diagnosis may play a significant role in its preoperative presumptive diagnosis, especially when incisional biopsy findings are inadequate.
Aim:
To systematically study the detailed cytomorphologic features of ameloblastoma and to evaluate the role of fine needle aspiration cytology (FNAC) in its preoperative diagnosis.
Materials and Methods:
In this study, FNAC was done on 26 cases of intra-osseous jaw lesion, clinically diagnosed as odontogenic tumor or developmental odontogenic cysts and detailed cytopathological interpretation was carried out and the results were correlated with the corresponding histopathology.
Results:
Of the 26 cases, 15 were found to be ameloblastoma and sensitivity of FNAC in the diagnosis of ameloblastoma was found to be 86.6%. None of the intra-osseous jaw lesion was false positively diagnosed as ameloblastoma in FNAC and hence the specificity was found to be 100%.
Conclusion:
Presence of cohesive epithelial cell clusters exhibiting smaller basaloid cells with peripherally placed tall columnar cells and occasional large squamous cells either adjoining the basaloid epithelial clusters or in isolated group aids in the specific cytological diagnosis of ameloblastoma and FNAC offers an excellent diagnostic aid that may play a significant role in preoperative presumptive diagnosis of ameloblastoma along with incisional biopsy.
Keywords: Ameloblastoma, cytology, FNAC, odontogenic tumor
Introduction
Ameloblastoma is the most common epithelial odontogenic neoplasm, constituting about 1% of all tumors and cyst of the jaws and annual incidence rate of 0.6 new cases per one million people.[1] Clinically, the most common variant is solid/multicystic ameloblastoma and practically in most of the cases the tumor component present with both solid and cystic areas of varying proportion. Incisional biopsy samplings for an accurate preoperative diagnosis might become inadequate and misrepresentative, since the chance for encountering a cystic areas are high in these types of lesions. Moreover, incisional biopsy is generally attempted at a single site to avoid trauma to the patients. Fine needle aspiration cytology (FNAC) offers an excellent diagnostic aid in these situations, because under same local anesthesia which is given for incisional biopsy, it can be used to sample at multiple sites; additionally, it may facilitate in determining the biopsy site because pure cystic areas can be easily identified during aspiration. Though it is a simple and minimally invasive procedure, practically it is not used as an adjunct diagnostic aid in the intraosseous jaw tumor like ameloblastoma. With this background, an attempt was made to study the cytomorphologic features of the most common odontogenic tumor ameloblastoma and to evaluate the role of FNAC in its preoperative presumptive diagnosis.
Materials and Methods
The study population included total 26 cases of intraosseous jaw lesion which were clinically diagnosed as odontogenic tumor or developmental odontogenic cysts. Ethical clearance for proceeding with the study was obtained from the Institutional ethical committee. After obtaining the informed written consent of the patients, they were subjected to FNAC before incisional biopsy.
The aspirates obtained were smeared on the clean glass slides and immediately fixed with 95% ethyl alcohol. Prepared smears were stained with hematoxylin–eosin (HandE) and Papanicolaou (PAP) stains. The stained smears were systematically studied under microscope [Olympus – Model BX51RTF] and the cytological diagnosis of ameloblastoma was made based on the following cytological features, i.e., presence of cohesive cluster/sheets of basaloid epithelial cells with peripheral tall columnar cells consistent with ameloblast and larger squamous cells either adjoining the basaloid cell clusters or as occasional isolated groups in the smear.[2]
Interpretation of incisional biopsy specimen was made for each individual case by an author who was completely unaware of the cytological diagnosis and finally both the cytological and incisional biopsy diagnoses were correlated with the final histopathological diagnosis.
Results
Based on the above-mentioned cytological features, definitive FNAC diagnosis of ameloblastoma was made for 13 cases of the total 26 cases of intraosseous jaw lesion.
This FNAC diagnosis correctly correlated with the final histopathologic diagnosis of ameloblastoma in 13 cases, except for 2 cases of ameloblastoma that showed inadequate material in the smear, which were interpreted as negative cytology [Table 1].
Table 1.
Correlation of FNAC, incisional biopsy, and final histopathological diagnosis of ameloblastoma
The sensitivity of FNAC in the diagnosis of ameloblastoma was found to be 86.6%
None of the intraosseous jaw lesion was false positively diagnosed as ameloblastoma by FNAC and hence the specificity of FNAC in diagnosing ameloblastoma was found to be 100%.
Preoperative incisional biopsy diagnosis of ameloblastoma correlated correctly with the final histopathological diagnosis in 11 cases, except for 4 cases in which the incisional biopsy diagnosis was found to be calcifying epithelial odontogenic cyst (CEOC), calcifying epithelial odontogenic tumor (CEOT), aneurysmal bone cyst (ABC), and squamous odontogenic tumor (SOT) [Table 1].
Sensitivity of incisional biopsy in the diagnosis of ameloblastoma was 73.3%.
The histopathological diagnoses of remaining 11 intraossseus jaw lesions were found to be developmental odontogenic cysts, including 6 cases of dentigerous cyst and 5 cases of odontogenic keratocyst. In FNAC, they showed inadequate material for cytological interpretation.
Discussion
Ameloblastoma is a locally invasive neoplasm and nearly always arise as an intraosseous jaw lesion and often causes sufficient expansion of the jaw cortical plate. This inherent property of the tumor makes the needle penetration easy and FNAC can be done with relative ease as an adjunct aid in the diagnosis. But practically, these lesions are rarely aspirated and their cytological findings have been poorly documented in the literature.
The reason may be due to the fact that easy accessibility of the site for biopsy and lack of clear-cut criteria for cytological diagnosis for this lesion.
Though incisional biopsy is considered as a prime diagnostic modality for preoperative presumptive diagnosis of these lesions, they do not grow as a uniform solid mass, but rather contain multiple cystic spaces macroscopically; they render some difficulty in obtaining the adequate and representative sample during the biopsy procedure for its accurate diagnosis.
Considering the above situation, we believe that FNAC has an advantage as an adjunct diagnostic aid, i.e., sampling can be done at multiple sites and deeper aspect of the tumor can be sampled which might assist in arriving at the accurate preoperative diagnosis, especially when an incisional biopsy is superficial and inadequate for interpretation.
With this background, the primary aim of our study was to evaluate the utility of FNAC in preoperative presumptive diagnosis of ameloblastoma and FNAC was done on total 26 cases of intraosseous jaw lesion that were provisionally diagnosed as odontogenic tumor or developmental odontogenic cysts.
In this study, in 13 cases the preliminary FNAC diagnosis of ameloblastoma correlated with the final histopathological diagnosis except for two cases which showed inadequate material for interpretation.
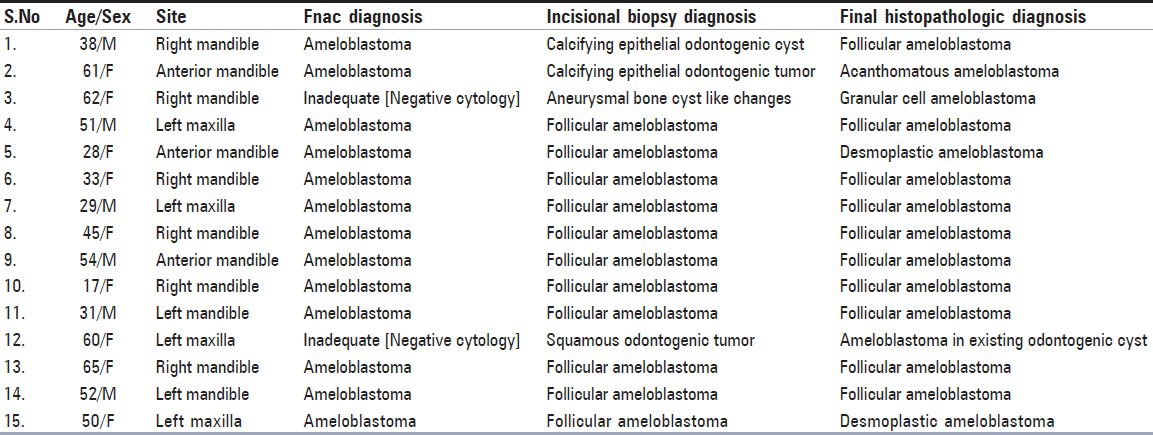
FNAC smears of ameloblastoma predominantly showed cohesive branched cluster of cells and the individual cells in the clusters were basaloid in nature, exhibiting round to oval nucleus, with finely granular and evenly distributed chromatin [Figure 1].
Figure 1.
FNA smears of ameloblastoma showing cohesive branched epithelial cell clusters (H and E, x200)
These features, i.e., predominant cohesive clusters of basaloid cells on FNA smear, are consistent with the epithelial origin of these tumors.
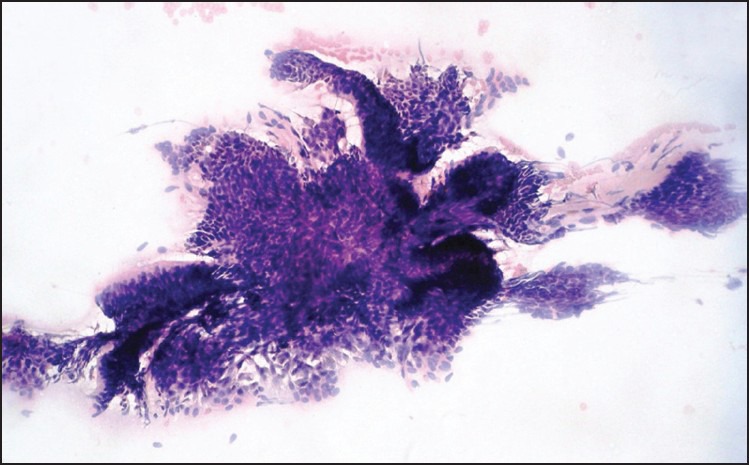
Another most important observation in FNAC was the presence of peripheral columnar cells in the cluster with nucleus polarized away from the cluster margin. These cells appeared elongated and resembled ameloblasts which was considered as an important diagnostic feature for definitive diagnosis of ameloblastoma in FNAC [Figure 2].
Figure 2.
FNAC smears of ameloblastoma showing basaloid epithelial cell clusters with peripheral tall columnar cells exhibiting reversely polarized nuclei (ameloblasts) (H and E, x400)
Also, occasional squamous cells with abundant cytoplasm and central nucleus either adjoining the basaloid epithelial clusters or in isolated forms were seen in some of the cases.
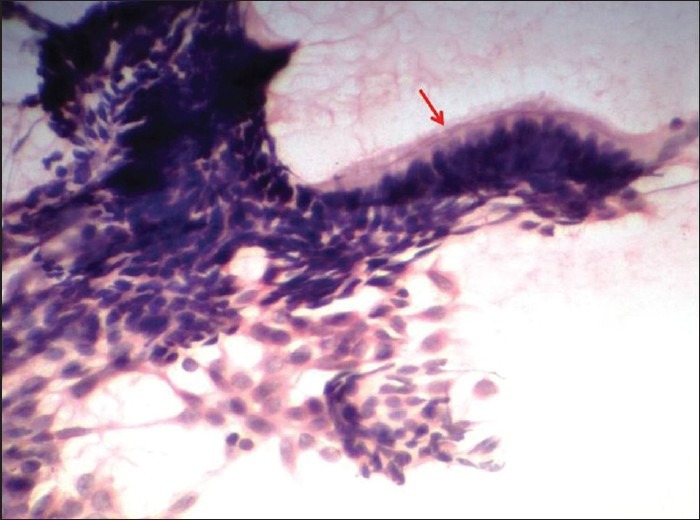
Interestingly in one of the cases, the cytological smear showed an abundant squamous cells and the corresponding histopathology of the lesion was found to be an acanthomatous variant of ameloblastoma, i.e., ameloblastoma with extensive squamous metaplasia [Figure 3].
Figure 3.
(a) FNAC smear of acanthomatous ameloblastoma exhibiting abundant squamous cells (Pap, x400) and (b) basaloid epithelial cell cluster with columnar cells (H and E, x200)
Of the two cases of ameloblastoma that showed negative cytology in FNAC, one case was found to be a granular cell variant of ameloblastoma and in the cytological smears it exhibited no cellular features diagnostic of ameloblastoma, except for the presence of abundant bloody materials. But the corresponding incisional biopsy diagnosis was found to be an aneurysmal bone cyst [Table 1].
Deshpande et al.[3] reported cytological features in two cases of granular cell ameloblastoma and stated that “recognition of large cell with abundant cytoplasm exhibiting eosinophilic granules dispersed singly or in loosely cohesive groups along with individual tightly cohesive basaloid epithelial cell clusters might facilitate its diagnosis in cytology.”
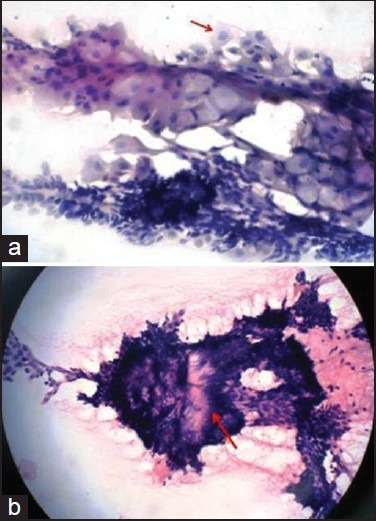
In our case, evaluation of the resected gross specimen in an attempt to find out the reason for failure to obtain the representative sample during FNAC showed complete cavitations, with the lesional tissue confining to the bony wall. This probably explains the reason for inadequate material from representative site, giving unsatisfactory results in such cases [Figure 4a].
Figure 4.
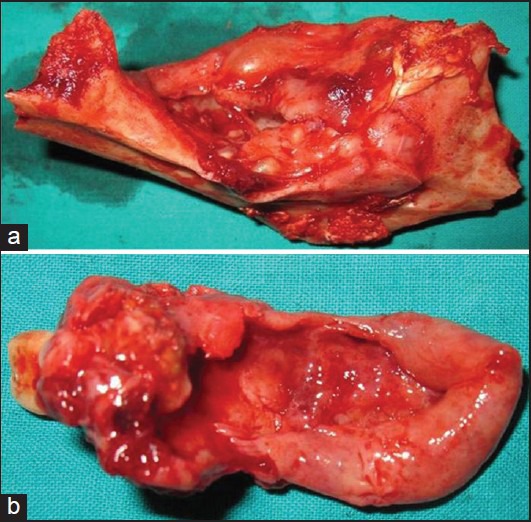
Gross specimens of ameloblastoma that showed inadequate material for interpretation in cytology
Similarly, the gross specimen of the other ameloblastoma which showed negative cytology in FNAC was found to be basically a cystic lining attached to a resected bone without any solid tissue mass [Figure 4b].
The cytological findings of ameloblastoma reported in our study were found to be consistent with ameloblastoma FNAC case series report by Günhan[2] and few other individual case reports in the literature.[4,5,6,7]
In the present study, sensitivity of FNAC in the diagnosis of ameloblastoma was found to be 86.6% and since there was no false-positive diagnosis, the specificity was found to be 100% and the sensitivity of incisional biopsy was found to be 73.3%.
The result of our study, i.e., sensitivity of 86.6% is approximately in accordance with the study results of Günhan O[2] and Uçok et al.[8] for the diagnosis of ameloblastoma, i.e., 100% and 93.5%, respectively.
The two negative cytology reports were mainly because of the complete cystic degeneration of the lesion, that had limited the procurement of adequate sample during aspiration and leaving those two cases, FNAC was found to be very effective in accurate preoperative diagnosis. Moreover, of the total four cases in which the incisional biopsy showed lack of correlation (i.e. CEOC, CEOT, ABC and SOT) with the final histopathological diagnosis of ameloblastoma, in two cases FNAC diagnosis correlated correctly with the final histopathological diagnosis which further indicates the importance of FNAC as an adjunct diagnostic aid in arriving at the correct preoperative diagnosis [Table 1].
Reports of large FNAC series of ameloblastoma are rare, usually features one or two cases. This study is one among the largest series featuring 15 cases along with Günhan[2] and Uçok et al.[8] (featuring 10 and 16 cases consecutively) and first of such from India.
Moreover, documentation by both Günhan[2] and Uçok et al.[8] were found to be retrospective study and to the best of our knowledge till date, this is the first prospective cytological study of ameloblastoma in which FNAC was carried out initially and specific FNAC diagnosis was given for each individual case and later correlated with the corresponding histopathology.
Though FNAC was found to be efficient in arriving at a specific diagnosis of ameloblastoma in majority of the cases in this study, possibility of getting an inadequate material and hence the negative reports cannot be completely ruled out, especially in situation where there is complete cystic degeneration of solid/multicystic ameloblastoma without a trace of solid area or in cases of unicystic variant of ameloblastoma.
Conclusion
Based on our experience, we conclude that FNAC offers an excellent, simple, safe, and minimally invasive adjunct diagnostic aid along with an incisional biopsy in the preoperative presumptive diagnosis of ameloblastoma and they exhibit distinctive cytological features for its diagnosis. Hence, with the correct clinicoradiologic correlation, preoperative cytological diagnosis of ameloblastoma can be rendered with reasonable high accuracy with the aid of FNAC, which potentially might avoid repeat incisional biopsy in the relevant situation.
Acknowledgement
The authors would like to acknowledge Professor Dr.K. Shankar M.D.S., and his team Department of Oral and Maxillofacial Surgery, MGPGI, Pondicherry, Dr.B.Krishnan M.D.S., Assistant Professor and Dr.G.Arunprasad M.D.S., Senior Resident, JIPMER, Pondicherry for their valuable help in providing clinical, radiological and surgical details of the cases.
Footnotes
Source of Support: Nil
Conflict of Interest: Nil.
References
- 1.Reichart PA, Philipsen HP. Chapter 5. Solid/Multicystic ameloblastoma. In: Peter A Reichart, Hans P Philipsen., editors. Odontogenic tumours and allied lesions. 1st ed. London, UK: Quintessence Publishing Co Ltd; 2004. pp. 43–5. [Google Scholar]
- 2.Günhan O. Fine needle aspiration cytology of ameloblastoma – A report of ten cases. Acta Cytol. 1996;40:967–9. doi: 10.1159/000334010. [DOI] [PubMed] [Google Scholar]
- 3.Deshpande A, Umap P, Munshi M. Granular cell ameloblastoma of the jaw. A report of two cases with fine needle aspiration cytology. Acta Cytol. 2000;44:81–5. doi: 10.1159/000326231. [DOI] [PubMed] [Google Scholar]
- 4.Radhika S, Nijhawan R, Das A, Dey P. Ameloblastoma of the mandible — Diagnosis by fine needle aspiration cytology. Diagn Cytopathol. 1993;9:310–3. doi: 10.1002/dc.2840090313. [DOI] [PubMed] [Google Scholar]
- 5.Mathew S, Rappaport K, Ali SZ, Busseniers AE, Rosenthal DL. Ameloblastoma. Cytologic findings and literature review. Acta Cytol. 1997;41:955–60. doi: 10.1159/000332767. [DOI] [PubMed] [Google Scholar]
- 6.Choudhury M, Dhar S, Bajaj P. Primary diagnosis of ameloblastoma by fine needle aspiration: A report of two cases. Diagn Cytopathol. 2000;23:414–6. doi: 10.1002/1097-0339(200012)23:6<414::aid-dc11>3.0.co;2-g. [DOI] [PubMed] [Google Scholar]
- 7.Lee HJ, Jung ES, Kim BK, Kang CS. Fine Needle Aspiration Cytology of Ameloblastoma: A Case Report. Korean J Cytopathol. 2002;13:70–3. [Google Scholar]
- 8.Uçok O, Dogan N, Uçok C, Günhan O. Role of fine needle aspiration cytology in preoperative presumptive diagnosis of ameloblastoma. Acta Cytol. 2005;49:38–42. doi: 10.1159/000326093. [DOI] [PubMed] [Google Scholar]