

Abstract
Introduction
About 10% of people present to primary healthcare services with sore throat each year. The causative organisms of sore throat may be bacteria (most commonly Streptococcus) or viruses (typically rhinovirus), although it is difficult to distinguish bacterial from viral infections clinically.
Methods and outcomes
We conducted a systematic review and aimed to answer the following clinical question: What are the effects of interventions to reduce symptoms of acute infective sore throat? We searched Medline, Embase, The Cochrane Library, and other important databases up to September 2013 (Clinical Evidence reviews are updated periodically; please check our website for the most up-to-date version of this review). We included harms alerts from relevant organisations such as the US Food and Drug Administration (FDA) and the UK Medicines and Healthcare products Regulatory Agency (MHRA).
Results
We found 6 studies that met our inclusion criteria. We performed a GRADE evaluation of the quality of evidence for interventions.
Conclusions
In this systematic review, we present information relating to the effectiveness and safety of the following interventions: antibiotics, corticosteroids, non-steroidal anti-inflammatory drugs, and paracetamol.
Key Points
Sore throat is an acute upper respiratory tract infection that affects the respiratory mucosa of the throat.
About 10% of people in Australia present to primary healthcare services with sore throat each year.
The causative organisms of sore throat may be bacteria (most commonly Streptococcus) or viruses (typically rhinovirus), but it is difficult to distinguish bacterial from viral infections clinically.
Paracetamol seems to effectively reduce the pain of acute infective sore throat after regular doses over 2 days.
There is a risk of rare but serious skin reactions with paracetamol (acetaminophen).
Non-steroidal anti-inflammatory drugs (NSAIDs) may reduce the pain of sore throat at 2 to 5 days.
NSAIDs are associated with gastrointestinal and renal adverse effects.
Antibiotics can reduce the proportion of people with symptoms associated with sore throat at 3 days.
Reduction in symptoms seems greater for people with positive throat swabs for Streptococcus than for people with negative swabs.
Antibiotics are generally associated with adverse effects such as nausea, rash, vaginitis, and headache, and widespread use may lead to bacterial resistance.
Corticosteroids added to antibiotics may reduce the severity of pain from sore throat in people compared with antibiotics alone.
Most trials used a single dose of corticosteroid. However, data from other disorders suggest that long-term use of corticosteroids is associated with serious adverse effects.
About this condition
Definition
Sore throat is an acute upper respiratory tract infection that affects the respiratory mucosa of the throat. Since infections can affect any part of the mucosa, it is often arbitrary whether an acute upper respiratory tract infection is called 'sore throat' ('pharyngitis' or 'tonsillitis'), 'common cold', 'sinusitis', 'otitis media', or 'bronchitis' (see figure 1 ). Sometimes, all areas are affected (simultaneously or at different times) in one illness. In this review, we aim to cover people whose principal presenting symptom is sore throat. This may be associated with headache, fever, and general malaise. Suppurative complications include acute otitis media (most commonly), acute sinusitis, and peritonsillar abscess (quinsy). Non-suppurative complications include acute rheumatic fever and acute glomerulonephritis.This review does not include people with previous rheumatic fever or previous glomerulonephritis, who are importantly different from the general population of people with sore throats. It also does not include people who are clinically seriously unwell (as these people are typically not included in the primary studies).
Figure 1.
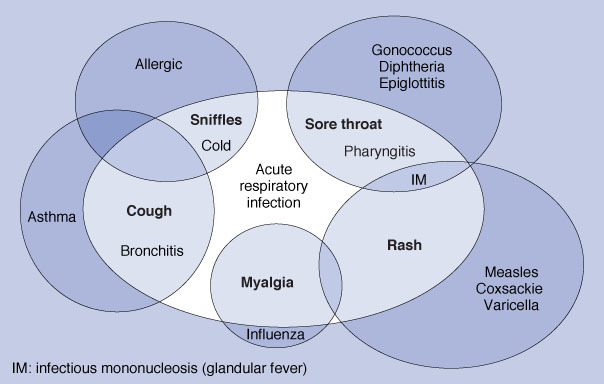
Confusion and overlap in the classification of acute respiratory infections.
Incidence/ Prevalence
There is little seasonal fluctuation in sore throat. About 10% of the Australian population present to primary healthcare services annually with an upper respiratory tract infection consisting predominantly of sore throat. This reflects about one fifth of the overall annual incidence. However, it is difficult to distinguish between the different types of upper respiratory tract infection. A Scottish mail survey found that 31% of adult respondents reported a severe sore throat in the previous year, for which 38% of these people visited a doctor.
Aetiology/ Risk factors
The causative organisms of sore throat may be bacteria (Streptococcus, most commonly group A beta-haemolytic, but sometimes Haemophilus influenzae, Moraxella catarrhalis, and others) or viruses (typically rhinovirus, but also coronavirus, respiratory syncytial virus, metapneumovirus, Epstein–Barr virus, and others). It is difficult to distinguish bacterial from viral infections clinically. Features suggestive of Streptococcus infection are: fever >38.5°C, exudate on the tonsils, anterior neck lymphadenopathy, and absence of cough. Sore throat can be caused by processes other than primary infections, including GORD, physical or chemical irritation (e.g., from nasogastric tubes or smoke), and occasionally hay fever. However, we consider only primary infections in this review.
Prognosis
The untreated symptoms of sore throat disappear by 3 days in about 40% of people, and untreated fevers in about 85%. By 1 week, 85% of people are symptom-free. This natural history is similar in Streptococcus-positive, Streptococcus-negative, and untested people.
Aims of intervention
To relieve symptoms of sore throat for 48 hours or longer.
Outcomes
Symptom severity: reduction in severity and duration of symptoms (sore throat pain, general malaise, headache, and fever) assessed at 48 hours or longer; patient satisfaction; health care utilisation. Time off work or school. Adverse effects of treatment.
Methods
Clinical Evidence search and appraisal September 2013. The following databases were used to identify studies for this systematic review: Medline 1966 to September 2013, Embase 1980 to September 2013, and The Cochrane Database of Systematic Reviews 2013, issue 9 (1966 to date of issue). Additional searches were carried out in the Database of Abstracts of Reviews of Effects (DARE) and the Health Technology Assessment (HTA) Database. We also searched for retractions of studies included in the review. Titles and abstracts identified by the initial search, run by an information specialist, were first assessed against predefined criteria by an evidence scanner. Full texts for potentially relevant studies were then assessed against predefined criteria by an evidence analyst. Studies selected for inclusion were discussed with an expert contributor. All data relevant to the review were then extracted by an evidence analyst. Study design criteria for inclusion in this review were published systematic reviews and RCTs. Open label trials were included where outcomes were objective; for subjective outcomes, trials were at least single-blinded and containing 20 or more individuals, of whom more than 80% were followed up. There was a minimum length of follow-up of 48 hours. We included RCT and systematic reviews of RCTs where harms of an included intervention were assessed, applying the same study design criteria for inclusion as we did for benefits. In addition, we use a regular surveillance protocol to capture harms alerts from organisations such as the FDA and the MHRA, which are added to the reviews as required. To aid readability of the numerical data in our reviews, we round many percentages to the nearest whole number. Readers should be aware of this when relating percentages to summary statistics such as relative risks (RRs) and odds ratios (ORs). We have performed a GRADE evaluation of the quality of evidence for interventions included in this review (see table). The categorisation of the quality of the evidence (high, moderate, low, or very low) reflects the quality of evidence available for our chosen outcomes in our defined populations of interest. These categorisations are not necessarily a reflection of the overall methodological quality of any individual study, because the Clinical Evidence population and outcome of choice may represent only a small subset of the total outcomes reported, and population included, in any individual trial. For further details of how we perform the GRADE evaluation and the scoring system we use, please see our website (www.clinicalevidence.com).
Table.
GRADE Evaluation of interventions for Sore throat.
| Important outcomes | Adverse effects, Symptom severity, Time off work or school | ||||||||
| Studies (Participants) | Outcome | Comparison | Type of evidence | Quality | Consistency | Directness | Effect size | GRADE | Comment |
| What are the effects of interventions to reduce symptoms of acute infective sore throat? | |||||||||
| 1 (154) | Symptom severity | Paracetamol versus placebo | 4 | –2 | 0 | 0 | 0 | Low | Quality points deducted for incomplete reporting of results and sparse data |
| 7 (1070) | Symptom severity | NSAIDs versus placebo | 4 | –1 | 0 | –1 | 0 | Low | Quality point deducted for incomplete reporting of results; directness point deducted for inclusion of a co-intervention |
| 27 (12,835) | Symptom severity | Antibiotics versus placebo | 4 | 0 | 0 | –1 | 0 | Moderate | Directness point deducted for narrow inclusion criteria |
| 3 (209) | Symptom severity | Corticosteroids versus placebo in people receiving antibiotics | 4 | 0 | 0 | –1 | 0 | Moderate | Directness point deducted for population differences between studies |
| 1 (92) | Time off work or school | Corticosteroids versus placebo in people receiving antibiotics | 4 | –2 | 0 | 0 | 0 | Low | Quality points deducted for sparse data and incomplete results |
We initially allocate 4 points to evidence from RCTs, and 2 points to evidence from observational studies. To attain the final GRADE score for a given comparison, points are deducted or added from this initial score based on preset criteria relating to the categories of quality, directness, consistency, and effect size. Quality: based on issues affecting methodological rigour (e.g., incomplete reporting of results, quasi-randomisation, sparse data [<200 people in the analysis]). Consistency: based on similarity of results across studies. Directness: based on generalisability of population or outcomes. Effect size: based on magnitude of effect as measured by statistics such as relative risk, odds ratio, or hazard ratio.
Glossary
- Low-quality evidence
Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate.
- Moderate-quality evidence
Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate.
Acute bronchitis
Acute otitis media
Acute sinusitis
Common cold
Tonsillitis
Disclaimer
The information contained in this publication is intended for medical professionals. Categories presented in Clinical Evidence indicate a judgement about the strength of the evidence available to our contributors prior to publication and the relevant importance of benefit and harms. We rely on our contributors to confirm the accuracy of the information presented and to adhere to describe accepted practices. Readers should be aware that professionals in the field may have different opinions. Because of this and regular advances in medical research we strongly recommend that readers' independently verify specified treatments and drugs including manufacturers' guidance. Also, the categories do not indicate whether a particular treatment is generally appropriate or whether it is suitable for a particular individual. Ultimately it is the readers' responsibility to make their own professional judgements, so to appropriately advise and treat their patients. To the fullest extent permitted by law, BMJ Publishing Group Limited and its editors are not responsible for any losses, injury or damage caused to any person or property (including under contract, by negligence, products liability or otherwise) whether they be direct or indirect, special, incidental or consequential, resulting from the application of the information in this publication.
References
- 1.Del Mar C, Pincus D. Incidence patterns of respiratory illness in Queensland estimated from sentinel general practice. Aust Fam Physician 1995;24:625–629,632. [PubMed] [Google Scholar]
- 2.Benediktsdóttir B. Upper airway infections in preschool children – frequency and risk factors. Scand J Prim Health Care 1993;11:197–201. [DOI] [PubMed] [Google Scholar]
- 3.Hannaford PC, Simpson JA, Bisset AF, et al. The prevalence of ear, nose and throat problems in the community: results from a national cross-sectional postal survey in Scotland. Fam Pract 2005;22:227–233. [DOI] [PubMed] [Google Scholar]
- 4.Dagnelie CF, Bartelink ML, van der Graaf Y, et al. Towards a better diagnosis of throat infections (with group A beta-hemolytic streptococcus) in general practice. Br J Gen Pract 1998;48:959–962. [PMC free article] [PubMed] [Google Scholar]
- 5.Del Mar CB, Glasziou PP, Spinks AB. Antibiotics for sore throat. In: The Cochrane Library, Issue 9, 2013. Chichester, UK: John Wiley & Sons, Ltd. Search date 2008. [Google Scholar]
- 6.Thomas M, Del Mar C, Glaziou P. How effective are treatments other than antibiotics for acute sore throat? Br J Gen Pract 2000;50:817–820. [PMC free article] [PubMed] [Google Scholar]
- 7.Russo M, Bloch M, de Looze F, et al. Flurbiprofen microgranules for relief of sore throat: a randomised, double-blind trial. Br J Gen Pract 2013;63:e149–e155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hayward G, Thompson MJ, Perera R, et al. Corticosteroids as standalone or add-on treatment for sore throat. In: The Cochrane Library, Issue 10, 2012. Chichester, UK: John Wiley & Sons, Ltd. Search date 2012. [Google Scholar]