

Abstract
Background
Induction therapy followed by high-dose chemotherapy and autologous transplantation is the standard treatment for suitable patients with multiple myeloma.
Objective
The aim of this study was to assess whether induction therapy with thalidomide-containing regimens was associated with improved results compared to vincristine, doxorubicin, and dexamethasone, and whether cyclophosphamide, thalidomide, and dexamethasone were associated with better results than thalidomide and dexamethasone.
Methods
The records of 152 patients who underwent autologous transplantation at this institution from August of 2004 to January of 2012 were reviewed, selecting those with at least partial response to a maximum of eight cycles of induction therapy and sufficient follow-up information for analysis.
Results
This study included 89 patients; 44 were female, with a mean age of 55 years (there was a significant trend for increasing age over the years of the study). The median number of induction therapy cycles was four, again with a trend of increase over the years. At least a very good partial response to induction therapy was achieved more often in the cyclophosphamide, thalidomide, and dexamethasone group (61.1%) and in the thalidomide and dexamethasone group (59.2%) than in the vincristine, doxorubicin, and dexamethasone group (16.2%). The overall median progression-free survival was 34 months, with no statistically significant difference between the three groups. The overall median survival was not reached, and there was no significant difference between the three groups; the estimated five-year overall survival was 55%.
Conclusion
Although the quality of responses appeared to be better with thalidomide-containing regimens, these improvements did not translate into improved long-term outcomes. Given its track record, cyclophosphamide, thalidomide, and dexamethasone is currently considered the preferred regimen for first-line induction therapy in the Brazilian public health system.
© 2014 Associação Brasileira de Hematologia, Hemoterapia e Terapia Celular. All rights reserved.
Keywords: Multiple myeloma; Thalidomide; Transplantation, autologous; Cyclophosphamide; Induction chemotherapy
Introduction
The use of induction chemotherapy followed by high-dose chemotherapy and autologous transplantation has become the standard treatment for suitable patients with multiple myeloma, in view of increased response rates and improved overall survival (OS) when compared with conventional chemotherapy.1., 2., 3., 4. In parallel, the use of thalidomide has emerged as an interesting option for the treatment of relapsed or newly diagnosed multiple myeloma.5., 6., 7. Given its typically lower hematologic toxicity than with conventional chemotherapy regimens and its lack of interference with stem-cell mobilization,8 thalidomide was rapidly incorporated into induction regimens.9 One of the new combinations that has demonstrated superiority to the classic vincristine, doxorubicin, and dexamethasone (VAD) regimen is thalidomide and dexamethasone (TD).10 Moreover, randomized trials that assessed triple thalidomide combinations, such as thalidomide, doxorubicin, and dexamethasone (TAD), cyclophosphamide, thalidomide, and dexamethasone (CTD), and bortezomib, thalidomide, and dexamethasone (VTD), have shown significantly improved responses with the triple combinations containing thalidomide, in comparison with corresponding control groups.11., 12., 13.
Patient access to novel agents is limited in the Brazilian public health system, despite the attempt of this system to provide full and comprehensive care to the citizens.14 However, thalidomide has been available for patients with multiple myeloma through the Brazilian public health system for several years, thus becoming a good option for induction therapy prior to autologous transplantation in the Santa Casa de São Paulo Medical School. The present study aimed to describe results with different induction treatments used in patients with multiple myeloma undergoing autologous transplantation.
Methods
Patient selection for analysis
For inclusion in this study, 152 patients with multiple myeloma who underwent autologous transplantation at this institution from August of 2004 to January of 2012 were retrospectively selected based on eligibility criteria for the current analysis. The key inclusion criterion was indication for autologous transplantation according to institutional guidelines (based chiefly on patient performance status and the presence of comorbidities). At least a partial response (PR) – according to the International Myeloma Working Group (IMWG) criteria – to induction regimens was present in all but two patients, who were referred for transplantation as this was deemed the best therapy for them at the time. The number of treatment cycles during the induction phase was three or four, based on the contemporary institutional protocol, which changed from VAD to TD to CTD over the years. Additional selection criteria were the receipt of a maximum of eight cycles of induction regimens (VAD, TD, or CTD) before transplantation, and enough follow-up information to allow for post-transplantation response assessment, as some patients had returned to their original institution for post-transplantation care. The protocol for the current study was approved by the institutional review board, which waived an informed consent from patients given the retrospective nature of the analysis.
Induction treatment regimens
Patients were treated with one of three induction regimens administered on an outpatient basis: (1) VAD; vincristine, 0.4 mg/day for four days intravenously (IV), doxorubicin, 9 mg/m2/day for four days IV, and dexamethasone, 40 mg/day on days 1 to 4, 9 to 12, and 17-20 orally; (2) TD; thalidomide, 100 to 200 mg/day according to tolerance, and dexamethasone 40 mg/week orally every 28 days continuously; or (3) CTD; cyclophosphamide, 50 mg/day orally, thalidomide, 100 to 200 mg/day according to tolerance, and dexamethasone, 40 mg/week orally every 28 days continuously. The cyclophosphamide schedule was based on the GBRAM 0002 CTD protocol (NCT01532856),15 comparing three different combinations with thalidomide for patients not eligible for autologous transplantation. Patients treated with VAD underwent transplantation from August of 2004 to September of 2009; those treated with TD, from May of 2007 to June of 2011; and those treated with CTD, from February of 2009 to January of 2012. Mobilization was performed with granulocyte colony-stimulating factor (G-CSF) alone (15 to 20 μg/kg/day for five days) for all patients in the TD and CTD groups, and in ten patients in the VAD group. Twenty-nine patients in the VAD group were mobilized with cyclophosphamide (4 g/m2) + G-CSF (10-15 μg/kg/day); of note, 28 patients in this group came from the randomized GBRAM 0001 trial (NCT01296503),16 designed to assess the role of thalidomide with or without dexamethasone as a maintenance therapy for patients after a single autologous transplantation. All patients had infection prophylaxis with trimethoprim-sulfamethoxazole (800/160 mg four times a week) during induction and after transplantation. Patients who received thalidomide during the induction treatment were given aspirin (100 mg/day) for prophylaxis of deep vein thrombosis, unless contraindicated.
Response assessment
During induction treatment, patients were examined monthly for response using the IMWG criteria, without evaluation of the free light chains.17 A further category [minimum response (MR)], defined by the European Bone Marrow Transplantation (EBMT) criteria, was added in the evaluation of response, which is defined as a reduction in the monoclonal component by more than 25%, but less than 50%.18 An overall response to induction treatment was considered when the response was at least a PR by the IMWG criteria or MR by the EBMT criteria. Patients were reassessed for response at approximately 100 days after transplantation. Response improvement was considered when the response changed between the end of the induction phase and after transplantation from PR to at least a very good PR (VGPR), or if VGPR was maintained between the two phases. None of the patients analyzed in the current study had a failed induction treatment, since all underwent transplantation.
Data collection and statistical analysis
The main objective of this study was to compare the outcomes of patients with multiple myeloma according to the three induction regimens. A secondary objective was the assessment of these outcomes in this institution over the years comprised in the study. Patients' medical records were reviewed in order to collect baseline and follow-up variables of interest, including gender, age, Durie-Salmon (DS) and International Staging System (ISS) stages, paraprotein type, number of cycles of induction treatment, response after induction treatment and after autologous transplantation, and survival status.
Categorical variables were compared between groups using Fisher's exact or the chi-squared test, as appropriate, while continuous variables were analyzed by the Student's t-test in the case of two groups or one-way analysis of variance (ANOVA) for comparisons across the three groups. No formal statistical comparisons were undertaken between treatment groups regarding response rates, given that only responding patients were included in the study. However, the response category (at least VGPR versus less than VGPR) after induction treatment was considered a baseline feature of patients in each group, and was thus included in multivariate models of time-to-event variables of interest. Such variables were OS, defined as the time elapsed between day 1 of transplantation and death from any cause, and progression-free survival (PFS), defined as the time between day 1 of transplantation and relapse or progression of multiple myeloma ascertained by any clinical, laboratory, or radiographic method. For both OS and PFS, data were censored at the last date of contact with a patient who was alive or alive and progression-free, respectively. OS and PFS were estimated by the Kaplan-Meier method and differences between groups were compared using the log-rank test. Kaplan-Meier analyses were also used to identify potential predictor variables for OS and PFS. Such variables were included in Cox regression models that also had treatment group as a covariate. Two-sided p-values were considered statistically significant when < 0.05. Statistical analysis was performed using MedCalc, version 11.0.0.0 (MedCalc® - Mariakerke, Belgium).
Results
Baseline patient characteristics
Table 1 presents the main demographic and clinical features of the 89 patients included in the study, according to induction treatment regimens. Three of these patients had undergone one previous autologous transplantation and 86 had only the index transplantation analyzed herein. Slightly more patients were treated with VAD and TD than with CTD. Overall, nearly half of patients were female, and the mean age was 55 years. There was no significant difference in gender distribution, but there was a significant trend for increasing age among groups, possibly reflecting increasing experience with transplantation over the years. The presence or absence of a plasmacytoma was reported more frequently in the TD and CTD groups, but no significant difference was found between the three groups when only the cases with such information were compared. As expected, the length of follow-up was significantly different among groups; conversely, there were no statistically significant differences in DS or ISS stages; however, regarding DS stage, most patients were in stage III in the three groups. The median number of induction cycles per patient was four, ranging from one to eight; there was a statistically significant progressive increase in the proportion of patients with four or more induction cycles over the years of the study (p-value = 0.01; chi-squared test for trend). The paraprotein type was immunoglobulin (Ig) G in nearly half and IgA in nearly one-quarter of the patients in the three groups, with no significant differences in proportions of other subtypes, including light chains (data not shown).
Table 1.
Baseline patient characteristics according to induction regimens.
| Variable | VAD (n = 31) | TD (n = 31) | CTD (n = 19) | p-value |
|---|---|---|---|---|
| Mean age - years | 52 | 55 | 58 | 0.05 |
| Gender -n | 0.45 | |||
| Male | 19 | 14 | 12 | |
| Female | 20 | 17 | 7 | |
| DSSa - n | 0.46 | |||
| I | 1 | 0 | 0 | |
| II | 2 | 5 | 2 | |
| III | 36 | 25 | 17 | |
| ISSa - n | 0.29 | |||
| I | 11 | 6 | 4 | |
| II | 17 | 9 | 3 | |
| III | 7 | 6 | 7 | |
| Plasmocytoma - n | 0.97 | |||
| Yes | 5 | 5 | 4 | |
| No | 19 | 15 | 15 | |
| Number of cycles -n | n | 0.01 | ||
| < 4 | 21 | 10 | 4 | |
| ≥ 4 | 17 | 16 | 15 | |
| Median follow up - monthsa | 32.2 | 14.2 | 5.5 | < 0.01 |
VAD: vincristine, doxorubicin and dexamethasone; TD: thalidomide and dexamethasone; CTD: cyclophosphamide, thalidomide and dexamethasone; DSS: Durie-Salmon staging system; ISS: International Staging System.
Data were missing for one patient regarding DSS, 19 patients regarding ISS (from lack of beta-2-microglobulin levels), six patients regarding the number of cycles, and 11 patients regarding follow-up.
During the induction phase, at least VGPR was achieved more frequently in the CTD (61.1%) and TD (59.2%) groups than in the VAD group (16.2%); conversely, other response categories were more frequent in the VAD group than with the thalidomide-containing regimens. After transplantation, patients in the TD group had the higher rates of at least VGPR (84.6%) when compared with patients in the CTD (63.1%) and the VAD (48.5%) groups. As a result of more frequent responses qualifying as at least VGPR in the thalidomide-containing groups, response improvement was more frequent in the VAD group.
Long-term outcomes of transplantation
The overall median PFS in the 89 patients was 34 months. As shown in Figure 1, there was no significant difference in PFS between the three groups. Likewise, there was no association between PFS and age (≤ 55 versus > 55 years), the number of induction cycles, the achievement of at least a VGPR after induction treatment, DS stage, or ISS in univariate Kaplan- Meier analyses. The presence of plasmacytoma was marginally associated with decreased PFS (p-value = 0.08). Since age and the number of induction cycles were significantly different between groups, these two covariates were included in a Cox multivariate analyses for PFS that also included treatment groups. Only treatment with TD was marginally (and inversely) associated with PFS (p-value = 0.04) in this multivariate analysis.
Figure 1.
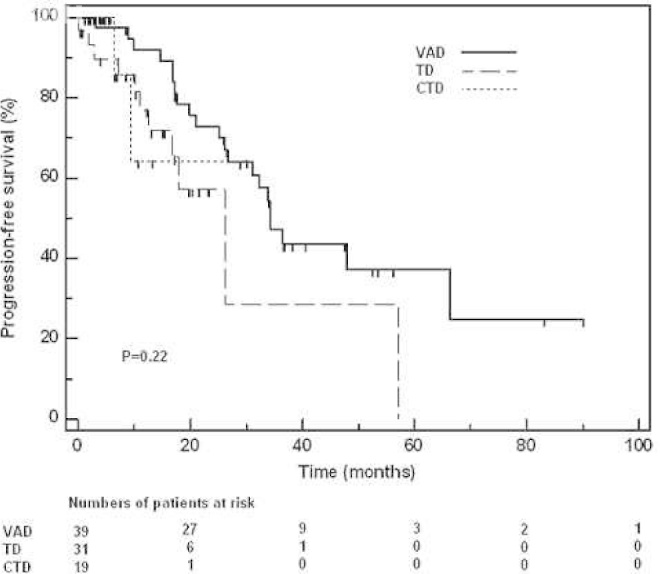
Progression-free survival according to induction regimens. CTD: cyclophosphamide, thalidomide and dexamethasone; TD: thalidomide and dexamethasone; VAD: vincristine, doxorubicin and dexamethasone. Marks represent censoring.
The median OS of the 89 patients was not reached, and the estimated survival proportion at five years was 55%. Figure 2 shows the distribution of OS; there was no significant difference between the three groups. There was no association between OS and the presence of plasmacytoma, the number of induction cycles, the achievement of at least a VGPR after induction treatment, or DS stage in univariate Kaplan-Meier analyses. However, age was marginally associated with OS, with younger patients having a shorter survival time (p-value = 0.06). Likewise, there as a marginal association between ISS and OS (p-value = 0.05). In a stepwise Cox multivariate analyses for OS that included age, the number of induction cycles, ISS, and treatment groups as covariates, only the presence of ISS stage 3 was associated with OS (p-value = 0.01).
Figure 2.
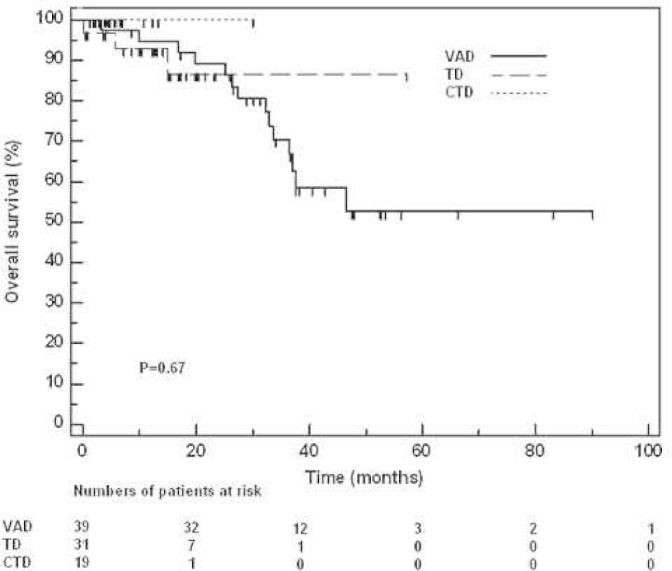
Overall survival according to induction regimens. CTD: cyclophosphamide, thalidomide and dexamethasone; TD: thalidomide and dexamethasone; VAD: vincristine, doxorubicin and dexamethasone. Marks represent censoring.
Discussion
The present study was based on a cohort of patients that were treated at a single center in Brazil and had as one of its goals the comparison between the effectiveness of induction therapy with newer regimens (CTD and TD) and that of classic VAD. A direct comparison of response rates with these three regimens was not deemed appropriate, given the fact that only responding patients were selected for analysis (with the exception of two patients who were not at least in PR at the time of transplantation). It is noteworthy, however, that the quality of responses appeared better with the two oral regimens, since at least a VGPR was achieved more frequently in these groups than in the VAD group. Conversely, such improved responses did not translate into improved long-term outcomes, as shown by the PFS and OS analyses. However, the retrospective nature of this study and the selection criteria for analysis should be considered when comparing long-term outcomes in patients. Importantly, the PFS and OS curves in the present study resemble those from clinical trials of these same therapeutic strategies, considering the fact that only patients responding to induction therapy were included in the present analysis.
The use of high-dose chemotherapy followed by autologous transplantation remains a standard treatment for eligible patients with multiple myeloma. Throughout the years, the classic VAD regimen has been replaced by newer, more effective regimens for induction prior to autologous transplantation, and thalidomide is a component of some of these newer strategies. In Brazil, this drug is made available by the government, allowing for its widespread use for patients with multiple myeloma. It has been demonstrated that the TD regimen is superior to VAD with regard to responses during the induction phase.10 Conversely, clinical trials that have used the CTD regimen as first-line therapy for induction prior to transplantation are scant. The first report on the activity of CTD in this setting was a retrospective study by Wu et al., in which CTD was considered to have higher efficacy and more rapid responses than the cyclophosphamide, vincristine, doxorubicin, and methylprednisolone regimen; however, no survival comparisons were made between the two induction regimens.19 Morgan et al. conducted a randomized study and demonstrated an advantage of CTD over the cyclophosphamide, vincristine, doxorubicin, and dexamethasone regimen, mainly in terms of better responses (complete response [CR] and near CR) in the induction phase, as well as after transplantation; this study was notable for the large number of patients enrolled (n = 1,110).12
The recent paradigm shift in the treatment of multiple myeloma has allowed improvements in response rates and patient survival. The successful use of high-dose chemotherapy rescued by autologous stem-cell transplantation was followed by the use of new systemic agents (immunomodulators and proteasome inhibitors) for induction therapy with increased refinement in the combinations of these agents and the use of three-drug regimens. Many centers around the world have been able to incorporate combinations of an immunomodulator and bortezomib in their daily practice as induction therapy for patients who are eligible for transplantation.13 However, such combinations are not feasible in many other places due to their cost. There are no studies in Brazil that have assessed first-line induction therapy with two or three agents for patients with multiple myeloma, regardless of their eligibility for transplantation. The chief importance of the present study was the assessment of results between transplantation-eligible patients treated with a novel agent, thalidomide, in the public health system. Arguably, nearly two-thirds of Brazilian patients with multiple myeloma are treated in the public health system, in which thalidomide is available. However, the incorporation of other novel agents in this system has so far proved difficult. Therapies that are currently available in this system were assessed and the results with the regimen that the authors currently find most suitable, namely the combination of an immunomodulator, an alkylating agent, and a corticosteroid, were described.
The present study assessed whether first-line induction therapy with thalidomide-containing regimens might be associated with improved results, when compared with VAD, and whether a three-drug regimen (CTD) might be associated with improved results, when compared with TD. Despite the retrospective nature of this study, the relatively small number of patients in each of the three groups, and the selection of patients who achieved at least a PR to induction therapy, the data suggest that thalidomide-containing combinations lead to improved responses, in comparison with VAD. In the future, the authors plan to collect additional data, from other institutions in Brazil, in order to analyze results in a larger dataset and over time. Meanwhile, CTD is considered to be the best regimen for first-line induction therapy in the public health system.
Conflicts of interest
The authors declare no conflicts of interest.
REFERENCES
- 1.San Miguel J.F., Blade Creixenti J., Garcia-Sanz R. Treatment of multiple myeloma. Haematologica. 1999;84(1):36–58. [PubMed] [Google Scholar]
- 2.Attal M., Harousseau J.L., Stoppa A.M., Sotto J.J., Fuzibet J.G., Rossi J.F. A prospective, randomized trial of autologous bone marrow transplantation and chemotherapy in multiple myeloma. Intergroupe Francais du Myelome. N Engl J Med. 1996;335(24):1844–1845. doi: 10.1056/NEJM199607113350204. author reply 1845. [DOI] [PubMed] [Google Scholar]
- 3.Child J.A., Morgan G.J., Davies F.E., Owen R.G., Bell S.E., Hawkins K. Medical Research Council Adult Leukaemia Working Party. High-dose chemotherapy with hematopoietic stem-cell rescue for multiple myeloma. N Engl J Med. 2003;348(19):1875–1883. doi: 10.1056/NEJMoa022340. [DOI] [PubMed] [Google Scholar]
- 4.Bladé J., Rosinol L., Sureda A., Ribera J.M., Díaz-Mediavilla J., García-Larana J. Programa para el Estudio de la Terapéutica en Hemopatía Maligna (PETHEMA). High-dose therapy intensification compared with continued standard chemotherapy in multiple myeloma patients responding to the initial chemotherapy: long-term results from a prospective randomized trial from the Spanish cooperative group PETHEMA. Blood. 2005;106(12):3755–3759. doi: 10.1182/blood-2005-03-1301. [DOI] [PubMed] [Google Scholar]
- 5.Singhal S., Mehta J., Desikan R., Ayers D., Roberson P., Eddlemon P. Antitumor activity of thalidomide in refractory multiple myeloma. N Engl J Med. 1999;341(21):1565–1571. doi: 10.1056/NEJM199911183412102. Comment In: N Engl J Med. 2001;344(25):1951-2; N Engl J Med. 2000;343(13):972-3; N Engl J Med. 2000;342(13):975; author reply 975-6; N Engl J Med. 1999;341(21):1606-9. [DOI] [PubMed] [Google Scholar]
- 6.Rajkumar S.V., Blood E., Vesole D., Fonseca R., Greipp P.R. Eastern Cooperative Oncology Group. Phase III clinical trial of thalidomide plus dexamethasone compared with dexamethasone alone in newly diagnosed multiple myeloma: a clinical trial coordinated by the Eastern Cooperative Oncology Group. J Clin Oncol. 2006;24(3):431–436. doi: 10.1200/JCO.2005.03.0221. Comment in: J Clin Oncol. 2006;24(3):334-6; J Clin Oncol. 2006; 24(18):2967-8; author reply 2968-9; Nat Clin Pract Oncol. 2008;5(12):690-1. [DOI] [PubMed] [Google Scholar]
- 7.Rajkumar S.V., Rosinol L., Hussein M., Catalano J., Jedrzejczak W., Lucy L. Multicenter, randomized, double-blind, placebo-controlled study of thalidomide plus dexamethasone compared with dexamethasone as initial therapy for newly diagnosed multiple myeloma. J Clin Oncol. 2008;26(13):2171–2177. doi: 10.1200/JCO.2007.14.1853. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kumar S., Giralt S., Stadtmauer E.A., Harousseau J.L., Palumbo A., Bensinger W. International Myeloma Working Group. Mobilization in myeloma revisited: IMWG consensus perspectives on stem cell collection following initial therapy with thalidomide-, lenalidomide-, or bortezomib-containing regimens. Blood. 2009;114(9):1729–1735. doi: 10.1182/blood-2009-04-205013. [DOI] [PubMed] [Google Scholar]
- 9.Reece D.E. Hematology Am Soc Hematol Educ Program. 2005. An update of the management of multiple myeloma: the changing landscape; pp. 353–359. [DOI] [PubMed] [Google Scholar]
- 10.Cavo M., Zamagni E., Tosi P., Tacchetti P., Cellini C., Cangini D. Bologna 2002 study. Superiority of thalidomide and dexamethasone over vincristine-doxorubicindexamethasone (VAD) as primary therapy in preparation for autologous transplantation for multiple myeloma. Blood. 2005;106(1):35–39. doi: 10.1182/blood-2005-02-0522. [DOI] [PubMed] [Google Scholar]
- 11.Lokhorst H.M., van der Holt B., Zweegman S., Vellenga E., Croockewit S., van Oers M.H. Dutch-Belgian Hemato-Oncology Group (HOVON). A randomized phase 3 study on the effect of thalidomide combined with adriamycin, dexamethasone, and high-dose melphalan, followed by thalidomide maintenance in patients with multiple myeloma. Blood. 2010;115(6):1113–1120. doi: 10.1182/blood-2009-05-222539. [DOI] [PubMed] [Google Scholar]
- 12.Morgan G.J., Davies F.E., Gregory W.M., Bell S.E., Szubert A.J., Navarro Coy N. National Cancer Research Institute Haematological Oncology Clinical Studies Group. Cyclophosphamide, thalidomide, and dexamethasone as induction therapy for newly diagnosed multiple myeloma patients destined for autologous stem-cell transplantation: MRC Myeloma IX randomized trial results. Haematologica. 2012;97(3):442–450. doi: 10.3324/haematol.2011.043372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Cavo M., Tacchetti P., Patriarca F., Petrucci M.T., Pantani L., Galli M. GIMEMA Italian Myeloma Network. Bortezomib with thalidomide plus dexamethasone compared with thalidomide plus dexamethasone as induction therapy before, and consolidation therapy after, double autologous stem-cell transplantation in newly diagnosed multiple myeloma: a randomised phase 3 study. Lancet. 2010;376(9758):2075–2085. doi: 10.1016/S0140-6736(10)61424-9. [DOI] [PubMed] [Google Scholar]
- 14.Lopes L.C., Barberato-Filho S., Costa A.C., Osorio-de-Castro C.G. Rational use of anticancer drugs and patient lawsuits in the state of Sao Paulo. Southeastern Brazil. Rev Saude Publica. 2010;44(4):620–628. doi: 10.1590/s0034-89102010000400005. [DOI] [PubMed] [Google Scholar]
- 15.ClinicalTrials.gov . Identifier NCT01532856, Iberoamerican protocol with thalidomide in patients with symptomatic newly diagnosed multiple myeloma over 65 years. 2012 Feb 10. Bethesda (MD): National Library of Medicine (US)http://clinicaltrials.gov/show/NCT01532856 [cited 22 May 2013]. Available from: [Google Scholar]
- 16.ClinicalTrials.gov . Identifier NCT01296503, Thalidomide plus dexamethasone as maintenance therapy for multiple myeloma. 2011 Jan 27 – 2011 Feb 14. Bethesda (MD): National Library of Medicine (US)http://clinicaltrials.gov/show/NCT01532856 [cited 22 May 2013]. Available from: [Google Scholar]
- 17.Durie B.G., Harousseau J.L., Miguel J.S., Bladé J., Barlogie B., Anderson K. International Myeloma Working Group. International uniform response criteria for multiple myeloma. Leukemia. 2006;20(9):1467–1473. doi: 10.1038/sj.leu.2404284. Comment in: Leukemia. 2006;20(9):1467-73. [DOI] [PubMed] [Google Scholar]
- 18.Bladé J., Samson D., Reece D., Apperley J., Björkstrand B., Gahrton G. Criteria for evaluating disease response and progression in patients with multiple myeloma treated by high-dose therapy and haemopoietic stem cell transplantation. Myeloma Subcommittee of the EBMT. European Group for Blood and Marrow Transplant. Br J Haematol. 1998;102(5):1115–1123. doi: 10.1046/j.1365-2141.1998.00930.x. [DOI] [PubMed] [Google Scholar]
- 19.Wu P., Davies F.E., Horton C., Jenner M.W., Krishnan B., Alvares C.L. The combination of cyclophosphamide, thalidomide and dexamethasone is an effective alternative to cyclophosphamide - vincristine - doxorubicin - methylprednisolone as induction chemotherapy prior to autologous transplantation for multiple myeloma: a case- matched analysis. Leuk Lymphoma. 2006;47(11):2335–2338. doi: 10.1080/10428190600821955. [DOI] [PubMed] [Google Scholar]