

Abstract
PURPOSE
This trial was designed to evaluate the optimal dose of massage for individuals with chronic neck pain.
METHODS
We recruited 228 individuals with chronic nonspecific neck pain from an integrated health care system and the general population, and randomized them to 5 groups receiving various doses of massage (a 4-week course consisting of 30-minute visits 2 or 3 times weekly or 60-minute visits 1, 2, or 3 times weekly) or to a single control group (a 4-week period on a wait list). We assessed neck-related dysfunction with the Neck Disability Index (range, 0–50 points) and pain intensity with a numerical rating scale (range, 0–10 points) at baseline and 5 weeks. We used log-linear regression to assess the likelihood of clinically meaningful improvement in neck-related dysfunction (≥5 points on Neck Disability Index) or pain intensity (≥30% improvement) by treatment group.
RESULTS
After adjustment for baseline age, outcome measures, and imbalanced covariates, 30-minute treatments were not significantly better than the wait list control condition in terms of achieving a clinically meaningful improvement in neck dysfunction or pain, regardless of the frequency of treatments. In contrast, 60-minute treatments 2 and 3 times weekly significantly increased the likelihood of such improvement compared with the control condition in terms of both neck dysfunction (relative risk = 3.41 and 4.98, P = .04 and .005, respectively) and pain intensity (relative risk = 2.30 and 2.73; P = .007 and .001, respectively).
CONCLUSIONS
After 4 weeks of treatment, we found multiple 60-minute massages per week more effective than fewer or shorter sessions for individuals with chronic neck pain. Clinicians recommending massage and researchers studying this therapy should ensure that patients receive a likely effective dose of treatment.
Keywords: chronic neck pain, pain management, disability, massage, clinical trial, complementary and alternative medicine, holistic medicine
INTRODUCTION
Neck pain is a common condition, with a 12-month prevalence of 30% to 50% and rates of activity-limiting pain of 1.7% to 11.5%,1 and it accounts for more than 10 million ambulatory medical care visits per year in the United States.2 At least one-half of persons with neck pain report persistent or recurrent neck problems at 1 to 5 years of follow-up.3,4 Neck pain is the eighth leading cause of disability in the United States5 and fourth worldwide.6 It is the second leading reason for use of complementary and alternative medicine (CAM),7 with chiropractic and massage most commonly used.8 In a national survey, 61% of persons with neck pain who used both CAM and conventional therapies perceived CAM therapies to be more helpful for this condition, whereas just 6% perceived conventional treatments to be better.9
Massage is the second most commonly used CAM therapy for neck pain.10,11 Although it is often used as a stand-alone treatment for chronic neck pain in the United States, reviews of research on massage for neck pain draw inconsistent conclusions. Furlan et al12,13 found massage superior to various controls, Brosseau et al14 found it effective immediately posttreatment with further follow-up data lacking, and Patel et al15 were unable to draw conclusions because of the poor quality of mostly clinically irrelevant studies. An earlier Cochrane review16 noted that studies have used such different types and doses of massage that the optimum dose for practice and clinical trials is unknown. We therefore designed a study to evaluate the optimal combination of frequency and length of sessions with therapeutic massage in persons with chronic neck pain. This article describes outcomes 1 week after the end of a 4-week treatment period, our primary endpoint.
METHODS
Design
We conducted a 6-arm trial with 5 dosing schedules of massage. The trial protocol and all study procedures were approved by the Group Health Research Institute institutional review board. Before being screened for eligibility by telephone, prospective participants gave oral consent. Those still eligible gave written consent before an in-person examination and study enrollment. The study protocol, which has been published in detail,17 is summarized below.
Participants
Study participants were recruited from Group Health, an integrated health care system serving about 500,000 persons, and from the general population of greater Seattle. Adults aged 20 to 64 years with chronic nonspecific neck pain lasting at least 3 months who were able and willing to attend treatments at our clinic and give informed consent were potentially eligible. From June 2010 through August 2011, we recruited prospective participants using mailed invitations to Group Health members with neck pain–related visits to primary care clinicians, advertisements in the health plan’s magazine, posters, a study website, neighborhood blogs, and direct-mail postcards.
We excluded individuals whose neck pain had a pathologically identifiable cause (eg, vertebral fracture, metastatic cancer), was complex (eg, cervical radiculopathy, recent automobile accident), or was too mild, defined as scoring less than 4 on a pain intensity scale ranging from 0 to 10 and less than 5 on the Neck Disability Index (NDI) ranging from 0 to 50. We also excluded those with potential contraindications for massage (eg, hypersensitivity to touch), any massage within the last 3 months, massage for neck pain within the last year, or an inability to give informed consent or speak English. Finally, we excluded persons with medicolegal issues related to neck or back pain.
Randomization
At the end of the baseline interview, a research assistant electronically randomized each participant to 1 of the 6 treatment groups. Treatment assignments were generated by a statistician (A.J.C.) using the freely available R software (version 2.11.0, R-Project for Statistical Computing), with random block sizes of 6 and 12 within 2 strata, based on NDI scores (5–14 and ≥15). They were embedded in the computer-assisted telephone interviewing program and inaccessible to study staff before randomization.
Treatments
For the 4-week primary treatment period, participants were randomized to a wait list control group or to 5 different dosing schedules of massage: 30-minute treatments either 2 or 3 times per week, or 60-minute treatments 1, 2, or 3 times per week. We defined adherence as completion of at least 75% of the visits in each protocol.
On the basis of an earlier study,18 we defined distinct treatment protocols for both 30- and 60-minute treatments, which included range of motion assessment, hands-on check-in, massage applied directly to the neck, addressing compensatory patterns, and integration (reestablishment within a patient of being in a unified body after having received intensive isolated work). Therapists were given time limits for each part of the massage and permitted to use a broad range of massage techniques. No self-care recommendations were permitted. Eight licensed massage therapists with at least 5 years of experience were trained in the study protocol and provided massage treatments in the research clinic at Group Health. Treatment fidelity was monitored by a research assistant who was also a massage therapist and who observed a treatment for all therapists and 34% of those randomized to massage (4% of all treatments).
Outcomes and Follow-up
Outcomes were assessed at baseline and again at 5 weeks (a week after treatment completion) by telephone interviewers who were unaware of treatment assignment. Our prespecified primary outcomes were clinically important improvements in neck pain–related dysfunction and pain intensity. We attempted to obtain follow-up data from all trial participants.
The 10-item, 51-point NDI was used to measure neck pain–related dysfunction; higher scores indicate greater disability. The index shows high internal consistency and test-retest reliability, is responsive to change, and correlates well with the McGill Pain Questionnaire.19,20 The 11-point numerical rating scale was used to measure neck pain intensity; higher scores indicate more intense pain. This scale has demonstrated sensitivity to change and is correlated with other measures of pain intensity.21 Secondary outcomes included mean NDI and neck pain intensity; 3 types of activity limitation22; perceived stress, measured by the 10-item Perceived Stress Scale (higher scores indicate greater stress)22; a single-item, 7-point patient global rating of improvement (higher scores indicate less improvement); and a single question about overall patient satisfaction.23
Sample Size and Power
Details of our sample size calculations and all assumptions have been provided previously17 but are summarized briefly. Because this was a 6-arm dosing study, the calculation of sample size was inherently more complicated. Our sample size was chosen to ensure adequate power to detect a significant difference between at least 2 of the 5 massage treatment groups (and not just adequate power to find a difference between 1 or more of the treatment groups and the control group). We powered our study for the primary binary outcome of a clinically meaningful improvement in neck-related dysfunction (≥5 points on NDI). With 34 participants per group, we have 97% power to find a significant difference between at least 2 of the 6 groups (assuming that the control group had a 7% improvement and the massage groups had an improvement of 35%–70%) and 80% power to find a significant difference between 2 active massage groups. Assuming 10% loss to follow-up, we recruited 38 participants per group, for a total sample size of 228 in the trial.
Statistical Analysis
We calculated summary statistics (frequencies, means, and standard deviations) for baseline study participant characteristics by treatment group to identify any important baseline differences across groups. Following the a priori primary analysis plan, differences across treatment groups in the primary outcomes, a clinically meaningful improvement in neck-related dysfunction (≥5 points on NDI)24 or in pain (≥30% reduction on neck pain intensity scale)25 measured at 5 weeks after randomization, were evaluated using modified Poisson regression fitting a Poisson log-link regression model with generalized estimating equations (GEE) and robust standard errors.26 To avoid the pitfall of multiple comparisons related to having 6 treatment groups, we used the Fisher protected least-significant difference approach.27 This approach makes pairwise comparisons among the 6 treatment groups only if the overall omnibus Wald test statistic is significant. Prespecified secondary analyses using linear regression models with GEE and robust standard errors were used to estimate differences in mean changes from baseline across treatment groups for the 5-week NDI and neck pain intensity outcomes. All adjusted models included baseline NDI and neck pain intensity, age, sex, neck pain longer than 5 years in duration, use of medications for neck pain, and race (white non-Hispanic vs other). All adjusted variables were prespecified except for race, which was shown at baseline to have larger than expected differences across groups and met the adjustment criteria of not being related to any other prespecified adjustment variable and may be predictive of outcome response, drop-out, or both.
We used similar adjusted models to analyze the secondary outcomes. For the binary outcomes—more than 7 days in the past week that normal activities were cut by at least one-half due to neck pain, at least 1 day in the past 4 weeks that neck pain kept you in bed or lying down for most of the day, and at least 1 day in the past 4 weeks neck pain kept you out of work or school—we adjusted for only baseline NDI and neck pain intensity because of model-fitting issues for these uncommon outcomes. Further, for the secondary continuous outcome, perceived stress scale, we also adjusted for baseline perceived stress scale response.
All analyses were conducted according to intention to treat (ie, comparing participants in the groups to which they were originally randomly assigned). Analyses were performed using SAS statistical software (version 9.2; SAS Institute Inc). All P values are 2 sided and Wald based, with statistical significance at the P = .05 level.
RESULTS
Recruitment and Follow-up
Among the 1,027 people successfully assessed for eligibility between July 2010 and August 2011, we found 728 to be ineligible and 91 declined (Figure 1). Of the remaining 228 who were randomized, 37 to 39 persons were allocated to each of the 5 dosing groups or to the single wait list control group. The large majority of participants (86%) were recruited from Group Health. Overall, follow-up was 97%, with group-specific rates ranging from 93% to 100%.
Figure 1.
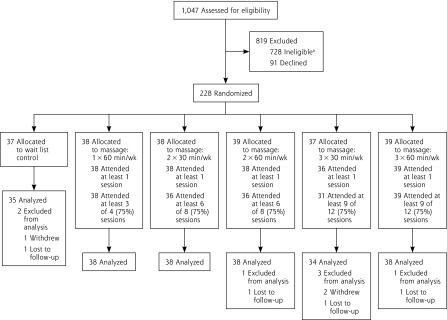
Trial flow.
a Most common reasons for ineligibility: 237 (32.6%) insufficient neck pain; 176 (24.6%) neck pain too complex; 74 (10.2%) prior massage; 140 (19.2%) could not attend treatment clinics.
Baseline Characteristics
Baseline characteristics were well balanced across groups, except for the percent of participants of white, non-Hispanic race/ethnicity and the percent having more than 7 days of usual activity restricted because of neck pain (Table 1). Study participants typically had moderately severe neck pain, but relatively few reported substantial activity limitations due to their pain.
Table 1.
Baseline Demographics and Measures Related to Neck Pain
| Variable | Control (n = 37) |
1 × 60 Min/wk (n = 38) |
2 × 30 Min/wk (n = 38) |
2 × 60 Min/wk (n = 39) |
3 × 30 Min/wk (n = 37) |
3 × 60 Min/wk (n = 39) |
|---|---|---|---|---|---|---|
| Demographics | ||||||
| Age, mean (SD), y | 44.4 (12.2) | 50.2 (10.9) | 42.3 (11.3) | 48.7 (11.5) | 45.7 (11.5) | 49.0 (9.9) |
| Women, No. (%) | 26 (70.3) | 30 (78.9) | 28 (73.7) | 28 (71.8) | 25 (67.6) | 27 (69.2) |
| College graduate, No. (%) | 27 (73.0) | 22 (57.9) | 26 (68.4) | 25 (64.1) | 27 (73) | 28 (78.1) |
| White non-Hispanic, No. (%) | 30 (81.1) | 30 (78.9) | 27 (71.1) | 32 (84.2) | 20 (54.1) | 29 (76.3) |
| Married, No. (%) | 22 (59.5) | 22 (57.9) | 27 (71.1) | 23 (59.0) | 26 (70.3) | 24 (61.5) |
| Family income >$45,000/y, No. (%) | 27 (73.0) | 25 (65.8) | 21 (55.3) | 29 (74.4) | 27 (73.0) | 23 (59.0) |
| Unemployed, No. (%) | 6 (16.2) | 9 (23.7) | 6 (15.8) | 8 (20.5) | 8 (21.6) | 7 (17.9) |
| Work that requires lifting and carrying, No. (%) | 8 (21.6) | 7 (18.4) | 13 (34.2) | 8 (20.5) | 7 (18.9) | 10 (25.6) |
| Measures of neck pain impact | ||||||
| Neck Disability Index, mean (SD) | 13.4 (4.8) | 14 (4.6) | 13.4 (3.8) | 13.7 (5.1) | 13.1 (5.6) | 14.3 (5.5) |
| Neck pain intensity, mean (SD) | 5.6 (1.3) | 5.9 (1.5) | 5.8 (1.4) | 5.6 (1.1) | 6.1 (1.5) | 5.7 (1.2) |
| Duration of neck pain >5 y, No. (%) | 11 (29.7) | 15 (39.5) | 19 (50.0) | 16 (41.0) | 12 (32.4) | 17 (43.6) |
| >7 Days usual activity restricted due to neck pain in the past 3 mo, No. (%) | 9 (24.3) | 6 (15.8) | 4 (10.5) | 8 (20.5) | 6 (16.2) | 11 (28.2) |
| >3 Days of neck exercise in past week, No. (%) | 13 (35.0) | 14 (36.8) | 8 (21.1) | 14 (35.9) | 11 (29.7) | 15 (38.5) |
| Any medications for neck pain in past week, No. (%) | 21 (56.8) | 22 (57.9) | 23 (60.5) | 25 (64.1) | 18 (48.7) | 28 (71.8) |
| NSAID use for neck pain, No. (%) | 19 (51.4) | 15 (39.5) | 17 (44.7) | 20 (51.3) | 11 (29.7) | 15 (38.5) |
| Opioid use for neck pain, No. (%) | 1 (2.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Measures of quality of life | ||||||
| SF-36 General health very good or excellent, No. (%) | 25 (67.6) | 25 (65.8) | 22.0 (57.9) | 26 (66.7) | 23 (62.2) | 29 (74.4) |
| SF-36 Mental health,a mean (SD) | 75.8 (15.2) | 76.3 (16.0) | 78.4 (14.3) | 77.1 (16.8) | 78.3 (11.7) | 78.9 (13.1) |
| SF-36 Physical health, mean (SD) | 80.2 (13.7) | 76.6 (19.6) | 81.1 (15.4) | 73.8 (17.8) | 79.6 (20.2) | 78.5 (16.4) |
| Miscellaneous measures | ||||||
| Worry, mean (SD) | 4.6 (1.9) | 4.3 (2.6) | 3.6 (2.6) | 4.1 (2.2) | 4.2 (2.4) | 4 (2.4) |
| Perceived Stress Scale, mean (SD) | 16.9 (6.9) | 15.9 (7.2) | 16.1 (5.6) | 17 (6.5) | 17.1 (4.9) | 15.8 (6.9) |
| Very satisfied with overall care for neck pain No. (%) | 1 (4.0) | 2 (7.4) | 1 (3.2) | 5 (17.9) | 1 (3.0) | 2 (6.1) |
| Expectation of massage helpfulness, mean (SD) | 7.7 (1.4) | 7.4 (2.3) | 7.4 (1.9) | 7.4 (1.8) | 7.2 (2.0) | 7.7 (2.3) |
| Expect neck pain to be much better or completely gone in 1 year, No. (%) | 13 (35.1) | 11 (28.9) | 10 (26.3) | 13 (33.3) | 12 (33.3) | 11 (28.2) |
| Top treatment choice was massage, No. (%) | 26 (76.5) | 25 (69.4) | 17 (48.6) | 22 (62.9) | 24 (68.6) | 25 (67.6) |
| Had prior massage for back or neck pain, No. (%) | 25 (67.6) | 28 (73.7) | 21 (55.3) | 22 (56.4) | 20 (54.1) | 25 (64.1) |
| Neck-related disability days | ||||||
| >7 Days in past 4 weeks that normal activities were cut by half a day or more because of neck pain, No. (%) | 5 (13.5) | 4 (10.5) | 1 (2.6) | 2 (5.1) | 4 (10.8) | 6 (15.4) |
| ≥1 Day in the past 4 weeks that neck pain kept you in bed or lying down for all or most of the day, No. (%) | 3 (8.1) | 4 (10.5) | 2 (5.3) | 0 (0.0) | 5 (13.5) | 2 (5.1) |
| ≥1 Day in past 4 weeks that neck pain kept you out of work or school, No. (%) | 2 (5.7) | 3 (8.6) | 1 (2.7) | 2 (5.4) | 1 (2.9) | 3 (8.1) |
NSAID = nonsteroidal anti-inflammatory drug; SF-36 = 36-Item Short Form Health Survey.
Notes: NDI is a 0 to 50 scale; higher scores indicate worse function. Neck pain intensity is a 0 to 10 scale; higher scores indicate more pain. SF-36 scales are all scaled to a 0 to 100 scale; higher scores indicate better function. Perceived Stress Scale is a 0 to 40 scale; higher scores indicate more stress. Worry and expectations are both 0 to 10 scales; higher scores indicate more worry or higher expectations, respectively.
On the 5-item Mental Health Inventory.
Treatment Adherence
Treatment adherence, defined as attending at least 75% of the assigned dose, was at least 95% in 4 massage dosing groups and 84% in the fifth group (30 minutes 3 times weekly). Because self-care recommendations were proscribed, it was not surprising that only 6 of 184 participants (3.3%) in the massage groups reported doing self-care activities they claimed were recommended by the study massage therapists, with those recommendations spread evenly among the groups.
Nonstudy Treatments
The use of medication as a nonstudy treatment varied across groups. Among those randomized to 60 minutes 3 times weekly treatments, medication use in the prior week dropped from 71.8% at baseline to 34.2%, and in the 30 minutes 3 times weekly group, medication use increased from 48.7% to 67.7%. In all other treatment groups, the absolute percentage change in medication use varied between −13.2% and 2.6%. Medication use in the control group increased slightly from 56.8% to 62.9%. Approximately one-third of participants reported doing neck exercises at least 3 times per week at both baseline and 5 weeks. Overall, 11% of participants made visits to health care professionals during the 5 weeks of treatment, mostly primary care physicians and chiropractors, with the highest percentage seen in the wait list control group (17%).
Neck Dysfunction and Neck Pain Intensity
A higher proportion of participants randomized to any dose of massage reported clinically important improvements in both the NDI and neck pain intensity relative to those randomized to the wait list control condition (Table 2). These differences were statistically significant only for the more frequent 60-minute treatment groups, however: the adjusted likelihood of improvement in NDI score for the 2 times weekly and 3 times weekly groups relative to the control group was 3.41 (95% CI, 1.05–11.08; P = .04) and 4.98 (95% CI, 1.64–1 5.17; P = .0 05), respectively. The adjusted likelihood of improvement in neck pain intensity was 2.30 (95% CI, 1.26–4.18; P = .007) and 2.73 (95% CI, 1.52–4.91; P = .001), respectively.
Table 2.
Primary Outcomes: Clinically Relevant Improvements in Neck Pain Measures
| Outcome by Massage Dose | Unadjusted | Adjusteda | |||||
|---|---|---|---|---|---|---|---|
|
| |||||||
| % (95% CI) | RR (95% CI) | P Value | Overall P Value | RR (95% CI) | P Value | Overall P Value | |
| Clinically relevant improvement in NDIb | |||||||
| Control | 8.6 (2.9–25.3) | 1.00 | – | .001 | 1.00 | – | .003 |
| 1 × 60 min/wk | 18.4 (9.4–36.0) | 2.15 (0.60–7.67) | .24 | 1.96 (0.53–7.33) | .32 | ||
| 2 × 30 min/wk | 15.8 (7.6–32.9) | 1.84 (0.50–6.81) | .36 | 1.90 (0.53–6.86) | .33 | ||
| 2 × 60 min/wk | 31.6 (19.8–50.4) | 3.68 (1.13–11.98) | .03 | 3.41 (1.05–11.08) | .04 | ||
| 3 × 30 min/wk | 11.8 (4.7–29.5) | 1.37 (0.33–5.68) | .66 | 1.61 (0.40–6.46) | .50 | ||
| 3 × 60 min/wk | 47.4 (33.9–66.2) | 5.53 (1.78–17.15) | .003 | 4.98 (1.64–15.17) | .005 | ||
| Clinically relevant improvement in neck pain intensityc | |||||||
| Control | 25.7 (14.6–45.2) | 1.00 | – | <.001 | 1.00 | – | <.001 |
| 1 × 60 min/wk | 34.2 (22.0–53.2) | 1.33 (0.65–2.72) | .43 | 1.17 (0.58–2.37) | .66 | ||
| 2 × 30 min/wk | 42.1 (29.0–61.1) | 1.64 (0.83–3.22) | .15 | 1.61 (0.83–3.13) | .16 | ||
| 2 × 60 min/wk | 63.2 (49.5–80.5) | 2.46 (1.33–4.54) | .004 | 2.30 (1.26–4.18) | .007 | ||
| 3 × 30 min/wk | 44.1 (30.2–64.4) | 1.72 (0.87–3.38) | .12 | 1.61 (0.81–3.18) | .17 | ||
| 3 × 60 min/wk | 76.3 (63.9–91.1) | 2.97 (1.64–5.36) | .000 | 2.73 (1.52–4.91) | .001 | ||
RR = relative risk.
Adjusted for baseline Neck Disability Index and neck pain intensity, age, sex, duration of neck pain more than 5 years, use of medications for neck pain, and race/ethnicity (white non-Hispanic vs other).
Improvement of at least 5 points from baseline at 5 weeks postrandomization.
Improvement of at least 30% from baseline at 5 weeks postrandomization.
Although the adjusted mean NDI scores worsened in the wait list control group after 5 weeks, they improved in all the massage groups (Table 3). Mean reductions in NDI from baseline were significantly greater in the massage groups than in the control group except for the 30-minute 3 times weekly dose. Improvements in adjusted mean neck pain intensity were significantly greater than that in the control group only in the 60-minute treatment 2 and 3 times weekly and in the 30-minute treatment 2 times weekly groups.
Table 3.
Secondary Outcomes: Mean Improvements in Neck Pain Measures
| Outcome by Massage Dose | Unadjusted | Adjusteda | |||||
|---|---|---|---|---|---|---|---|
|
| |||||||
| Mean Change (95% CI) |
Mean Difference (95% CI) |
P Value | Overall P Value | Mean Difference (95% CI) |
P Value | Overall P Value | |
| Neck Disability Index | |||||||
| Control | 1.45 (−0.20 to 3.10) | Ref | – | <.001 | Ref | – | <.001 |
| 1 × 60 min/wk | −0.86 (−2.09 to 0.36) | −2.31 (−4.37 to −0.26) | .03 | −2.31 (−4.29 to −0.32) | .02 | ||
| 2 × 30 min/wk | −0.89 (−2.33 to 0.54) | −2.34 (−4.53 to −0.16) | .04 | −2.35 (−4.51 to −0.18) | .03 | ||
| 2 × 60 min/wk | −2.06 (−3.51 to −0.62) | −3.52 (−5.71 to −1.32) | .002 | −3.44 (−5.53 to −1.35) | .001 | ||
| 3 × 30 min/wk | 0.05 (−1.26 to 1.35) | −1.41 (−3.51 to 0.70) | .19 | −1.73 (−3.78 to 0.33) | .10 | ||
| 3 × 60 min/wk | −4.36 (−6.25 to −2.47) | −5.81 (−8.32 to −3.30) | <.001 | −5.63 (−7.94 to −3.32) | <.001 | ||
| Neck pain intensity | |||||||
| Control | −0.51 (−1.35 to 0.32) | Ref | – | <.001 | Ref | – | <.001 |
| 1 × 60 min/wk | −1.21 (−1.84 to −0.58) | −0.70 (−1.74 to 0.35) | .19 | −0.43 (−1.36 to 0.50) | .37 | ||
| 2 × 30 min/wk | −1.66 (−2.29 to −1.03) | −1.14 (−2.19 to −0.10) | .03 | −1.02 (−1.93 to −0.12) | .03 | ||
| 2 × 60 min/wk | −2.21 (−2.81 to −1.61) | −1.70 (−2.72 to −0.67) | .001 | −1.56 (−2.46 to −0.66) | .001 | ||
| 3 × 30 min/wk | −1.62 (−2.19 to −1.05) | −1.10 (−2.12 to 0.09) | .03 | −0.83 (−1.73 to 0.07) | .07 | ||
| 3 × 60 min/wk | −2.74 (−3.22 to −2.25) | −2.22 (−3.19 to −1.26) | <.001 | −2.07 (−2.94 to −1.20) | <.001 | ||
Ref = reference group.
Adjusted for baseline Neck Disability Index and neck pain intensity, age, sex, duration of neck pain of more than 5 years, use of medications for neck pain, and race/ethnicity (white non-Hispanic vs other).
We performed linear tests for trend in the outcomes based on the number of 60-minute treatments per week (0 to 3 massages per week). These tests showed a significant dose-dependent benefit for both the adjusted NDI and neck pain intensity. For each additional weekly massage, there was an estimated −1.81-point improvement in NDI (95% CI, −2.52 to −1.10; P <.001) and an estimated −0.75-point improvement in neck pain intensity (95% CI, −1.01 to −0.47; P <.001).
Other Outcomes
There were no statistically significant differences between groups for any secondary outcomes except for the proportion of participants who reported their neck pain was much better or completely gone (omnibus P <.001) (Table 4). Three massage groups were significantly more likely to report this level of improvement than the control group: benefit was evident the 30 minutes 3 times weekly group (20.4%; 95% CI, 10.2%–40.6%); the 60 minutes 2 times weekly group (18.9%; 95% CI, 10.0%–35.8%), and the 60 minutes 3 times weekly group (40.6%; 95% CI, 27.8%–59.5%). Moreover, the last group fared significantly better than all other treatment groups.
Table 4.
Adjusted Secondary Outcomes at 5 Weeks Postrandomization
| Outcome | Control (n = 37) |
1 × 60 Min/wk (n = 38) |
2 × 30 Min/wk (n = 38) |
2 × 60 Min/wk (n = 39) |
3 × 30 Min/wk (n = 37) |
3 × 60 Min/wk (n = 39) |
Overall P |
|---|---|---|---|---|---|---|---|
| >7 Days in past 4 weeks that normal activities were cut by half a day or more because of neck pain, % (95% CI) | 8.9 (4.0 to 19.8) |
5.1 (2.3 to 11.8) |
1.9 (0.3 to 12.2) |
2.8 (0.8 to 9.2) |
4.7 (1.6 to 13.7) |
7.9 (3.3 to 18.9) |
.35 |
| ≥1 Day in the past 4 weeks that neck pain kept you in bed or lying down for all or most of the day, % (95% CI) | 6.5 (2.0 to 21.2) |
6.9 (2.9 to 16.7) |
4.3 (0.9 to 20.3) |
0.0a (n/a) |
8.5 (3.8 to 18.7) |
3.5 (1.0 to 12.8) |
.67 |
| ≥1 Day in the past 4 weeks that neck pain kept you out of work or school, % (95% CI) | 4.6 (1.1 to 19.8) |
6.8 (2.4 to 19.1) |
2.2 (0.4 to 14.1) |
3.6 (0.9 to 14.7) |
1.8 (0.4 to 7.8) |
4.9 (1.2 to 19.8) |
.73 |
| Perceived Stress Scale, mean (95% CI) | −0.42 (−2.4 to 1.6) |
−1.1 (−2.3 to 0.1) |
−1.6 (−3.3 to 0.2) |
−1.5 (−3.1 to 0.0) |
−3.7 (−5.5 to −1.9) |
−1.5 (−3.2 to 0.3) |
.21 |
| Compared with when you began the study, neck pain is much better or completely gone, % (95% CI) | 2.5 (0.4 to 14.8) |
7.1 (2.2 to 18.2) |
9.3 (3.6 to 23.9) |
18.9 (10.0 to 35.8) |
20.4 (10.2 to 40.6) |
40.6 (27.8 to 59.5) |
<.001 |
| Very satisfied with care for neck pain, % (95% CI) | 22.2 (11.2 to 44.0) |
40.0 (27.6 to 57.8) |
40.6 (27.8 to 59.2) |
54.6 (41.1 to 72.5) |
25.9 (16.3 to 44.3) |
47. 0 (33.2 to 66.5) |
.06 |
n/a = not applicable.
Note: All variables are adjusted for baseline Neck Disability Index and neck pain intensity. The outcomes Perceived Stress Scale, neck pain is much better/completely gone, and satisfaction with care for neck pain additionally adjusted for age, sex, duration of neck pain more than 5 years, use of medications for neck pain, and race (white non-Hispanic vs other). The Perceived Stress Scale was further adjusted for baseline score for this scale.
No participant in this group was kept in bed for most of the day because of neck pain.
Adverse Events
During the 4-week treatment period, 10 participants (5.2% of the total) reported 14 adverse events (11 mild and 3 moderately severe) at least possibly related to massage. All these events were related to pain, primarily spine pain. Adverse event frequencies were similar in participants attending 30-minute and 60-minute treatments (4% vs 6%, respectively) and in those attending 1, 2, or 3 times per week (7.9% vs 2.6% vs 6.7%, respectively).
DISCUSSION
Our findings demonstrate that the beneficial effects of massage treatments for chronic nonspecific neck pain increase with dose. Although 30-minute massages, either 2 or 3 times a week, failed to provide significant benefits compared with the wait list control condition, the beneficial effects of 60-minute massages increased with dose and were especially evident for those receiving massage 2 or 3 times per week. Compared with their control counterparts, massage participants were 3 times more likely to have a clinically meaningful improvement in neck function if they received 60 minutes of massage twice a week and 5 times more likely if they received 60 minutes of massage 3 times a week. Our results confirm the effectiveness of a 60-minute massage for persons with chronic neck pain. Changes in the use of medications for neck pain or visits to clinicians could not explain these findings. In addition, we found few adverse events, most of which were mild. Our findings are similar to those of our small trial of massage for chronic neck pain18 and a large trial of massage for back pain.28 Massage thus appears relatively safe when provided by appropriately trained therapists, but can be associated with transient increases in pain.
Our findings also suggest that previously published studies of massage for neck pain may have not administered adequate doses. For example, the newest Cochrane review of massage for neck pain15 reported 9 trials of massage for subacute or chronic neck pain. Among the 7 trials with conceivably relevant designs, 4 trials included only a single session of a single massage technique applied for less than 5 minutes, 1 trial included only five 30-minute treatments over 2 weeks, 1 included five 45-minute treatments over 1 month, and the last was a series of weekly 60-minute massages. In addition, most trials lacked massage resembling conventional massage practice in the United States, where 60-minute treatments administered by licensed massage therapists are the norm, a wide range of massage techniques are used in a single session, and self-care recommendations are provided.29 This review notes that there is little information regarding optimal parameters for the massage, including the number of treatments per week and the length of each session.
We found slightly different results in our controls and 60-minute weekly massage group than we did in a previously published study18 comparing weekly massage with a control condition of receipt of a self-care book. Participants in both studies reported similar ratings of neck pain and dysfunction before treatment; however, among the control groups, clinically important improvement in that earlier study was worse for pain (only 10% improved vs 26% in this trial) but similar for neck dysfunction (approximately 8% improved in both studies). More participants receiving weekly 60-minute massages in that earlier study reported clinically relevant improvement in both pain (48% improved vs 34% in this trial) and dysfunction (35% improved vs 18% in this trial). Virtually all participants in the prior study received self-care recommendations, most commonly pertaining to stretching, but such recommendations were prohibited in this trial, which may at least partially explain the difference between study results. Conceivably, these differences could reflect variability due to small sample sizes. Potentially, these combined results may indicate that 60 minutes once a week may still be an effective treatment relative to a control condition, but likely less effective relative to 2 to 3 times per week as indicated by this trial.
Our study’s strengths include rigorous randomization, assessment of follow-up outcomes by interviewers unaware of treatment group, high adherence to the massage dose in each group, high follow-up rates, and massage protocols that both maximized standardization of treatment and allowed the study massage therapists’ sufficient latitude to provide treatments they thought would benefit their patients. Our study’s major limitations include modest sample sizes in each group, inability to control for nonspecific effects of attention with the use of a wait list control design, and inclusion of patients who had primarily mild to moderate neck pain. The prohibition of giving self-care recommendations might be a limitation in the sense that massage therapists typically make such recommendations, but this prohibition enhances our confidence that the findings are due to the massage itself. In unpublished data from a larger study describing the practice of 126 massage therapists,29 we found that they recommended self-care for 87% of the 165 visits for chronic neck pain, most commonly body awareness (49%), hot and/or cold therapy (43%), and exercise (42%). Additional limitations include only short-term follow-up and our inability to fully assess how representative our patients are of those with chronic nonspecific neck pain in primary care.
Few studies of nonpharmacologic CAM therapies have evaluated the effect of dose on outcomes. In 2 small studies, Haas et al30,31 found greater improvement for back pain and cervicogenic headache among patients who received 3 or 4 chiropractic treatments per week for 3 weeks than among those receiving fewer treatment per week. In a 5-arm, 8-week trial of massage for persons with osteoarthritis, Perlman et al32 found that 60 minutes of weekly or twice weekly massage was clearly superior to usual care and appeared better than 30 minutes of twice weekly massage.
Our findings have important implications for both clinical practice and research. At baseline, only about 5% of participants were very satisfied with their overall care for neck pain, suggesting that new therapeutic alternatives are needed for family physicians. Outcome data suggest that patients seeking massage for chronic neck pain are more likely to benefit if they have multiple 60-minute treatments per week than if they have only 1. Such a treatment schedule might prove challenging for many patients because of time and financial constraints. Our findings also suggest that future trials evaluating massage for chronic neck pain, which we think would be important, should include multiple 60-minute treatments each week for the first 4 weeks of treatment, self-care recommendations, and longer-term follow-up.
Acknowledgments
We thank our research team, including Beth Lapham, our research assistants (Zoe Bermet, Kevin Filocamo, Melissa Parson, Kirsten Sullivan), massage therapists (Christine Chmielewski, Lesely Ernst, Tom Harvey, Michael Jacobus, Maureen McKelvey, Dawn Schmidt, Carol Tiebout), nurse practitioners (Wendy Robinson, David Diechert), programmers (Jane Grafton and DT Tran), and massage consultant Diana Thompson.
Footnotes
Conflicts of interest: authors report none.
Funding support: Our study was funded by grant R01 AT004411 from the National Center for Complementary and Alternative Medicine, National Institutes of Health.
Prior presentations: International Forum XII for Primary Care Research on Low Back Pain. Odense, Denmark, October 2012.
Disclaimer: The funders had no role in the interpretation or reporting of results. The views expressed herein do not necessarily represent the views of the funders.
Trial registration: NCT01122836 (ClinicalTrials.gov).
References
- 1.Hogg-Johnson S, van der Velde G, Carroll LJ, et al. The burden and determinants of neck pain in the general population: results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. Spine (Phila Pa 1976). 2008;33(4 Suppl):S39–S51 [DOI] [PubMed] [Google Scholar]
- 2.Riddle DL, Schappert SM. Volume and characteristics of inpatient and ambulatory medical care for neck pain in the United States: data from three national surveys. Spine (Phila Pa 1976). 2007;32(1):132–140; discussion 141 [DOI] [PubMed] [Google Scholar]
- 3.Haldeman S, Dagenais S. What have we learned about the evidence-informed management of chronic low back pain? Spine J. 2008;8(1):266–277 [DOI] [PubMed] [Google Scholar]
- 4.Carroll LJ, Hogg-Johnson S, Cote P, et al. Course and prognostic factors for neck pain in workers: results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. Spine (Phila Pa 1976). 2008;33(4 Suppl):S93–100 [DOI] [PubMed] [Google Scholar]
- 5.Murray CJ, Abraham J, Ali MK, et al. The State of US Health, 1990–2010: burden of diseases, injuries, and risk factors. JAMA. 2012;307(17):1809–181622550196 [Google Scholar]
- 6.Vos T, Flaxman AD, Naghavi M, et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2163–2196 Correction in Lancet. 2013;381(9867):628 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Barnes PM, Bloom B, Nahin RL. Complementary and alternative medicine use among adults and children: U.S., 2007. National Health Statistics Reports 2008;10(12):1–23 [PubMed] [Google Scholar]
- 8.Wolsko PM, Eisenberg DM, Davis RB, Kessler R, Phillips RS. Patterns and perceptions of care for treatment of back and neck pain: results of a national survey. Spine (Phila Pa 1976). 2003;28(3):292–297, discussion 298 [DOI] [PubMed] [Google Scholar]
- 9.Eisenberg DM, Kessler RC, Van Rompay MI, et al. Perceptions about complementary therapies relative to conventional therapies among adults who use both: results from a national survey. Ann Intern Med. 2001;135(5):344–351 [DOI] [PubMed] [Google Scholar]
- 10.Goode AP, Freburger J, Carey T. Prevalence, practice patterns, and evidence for chronic neck pain. Arthritis Care Res (Hoboken). 2010;62(11):1594–1601 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Eisenberg DM, Davis RB, Ettner SL, et al. Trends in alternative medicine use in the United States, 1990–1997: results of a follow-up national survey. JAMA. 1998;280(18):1569–1575 [DOI] [PubMed] [Google Scholar]
- 12.Furlan AD, Yazdi F, Tsertsvadze A, et al. A systematic review and meta-analysis of efficacy, cost-effectiveness, and safety of selected complementary and alternative medicine for neck and low-back pain. Evid Based Complement Alternat Med. 2012;2012:953139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Furlan AYF, Tsertsvadze A, Gross A, et al. Complementary and Alternative Therapies for Back Pain II. Evidence Report/Technology Assessment No. 194. Prepared by the University of Ottawa Evidence-based Practice Center under Contract No. 290-2007-10059-I (EPCIII). AHRQ Publication No. 10(11)E007. Rockville, MD: Agency for Healthcare Research and Quality; 2010 [Google Scholar]
- 14.Brosseau L, Wells GA, Tugwell P, et al. Ottawa Panel evidence-based clinical practice guidelines on therapeutic massage for neck pain. J Bodyw Mov Ther. 2012;16(3):300–325 [DOI] [PubMed] [Google Scholar]
- 15.Patel KC, Gross A, Graham N, et al. Massage for mechanical neck disorders. Cochrane Database Syst Rev. 2012;9:CD004871. [DOI] [PubMed] [Google Scholar]
- 16.Haraldsson BG, Gross AR, Myers CD, et al. ; Cervical Overview Group Massage for mechanical neck disorders. Cochrane Database Syst Rev. 2006;3(3):CD004871. [DOI] [PubMed] [Google Scholar]
- 17.Sherman KJ, Cook AJ, Kahn JR, Hawkes RJ, Wellman RD, Cherkin DC. Dosing study of massage for chronic neck pain: protocol for the dose response evaluation and analysis of massage [DREAM] trial. BMC Complement Altern Med. 2012;12:158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Sherman KJ, Cherkin DC, Hawkes RJ, Miglioretti DL, Deyo RA. Randomized trial of therapeutic massage for chronic neck pain. Clin J Pain. 2009;25(3):233–238 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Vernon H, Mior S. The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Ther. 1991;14(7):409–415 [PubMed] [Google Scholar]
- 20.Pietrobon R, Coeytaux RR, Carey TS, Richardson WJ, DeVellis RF. Standard scales for measurement of functional outcome for cervical pain or dysfunction: a systematic review. Spine. 2002;27(5):515–522 [DOI] [PubMed] [Google Scholar]
- 21.Von Korff M, Jensen MP, Karoly P. Assessing global pain severity by self-report in clinical and health services research. Spine.2000;25(24)3140–3151 [DOI] [PubMed] [Google Scholar]
- 22.Reiss P. Current estimates from the national health interview survey: United States. In: National Center for Health Statistics , ed. DHHS Publication PHS 86-1584, 1986. Vital and health statistics. Hyattsville MD: National Center for Health Statistics; 1984 [Google Scholar]
- 23.Cherkin DC, MacCornack FA. Patient evaluations of low back pain care from family physicians and chiropractors. West J Med. 1989;150(3):351–355 [PMC free article] [PubMed] [Google Scholar]
- 24.Hurwitz EL, Morgenstern H, Harber P, Kominski GF, Yu F, Adams AH. A randomized trial of chiropractic manipulation and mobilization for patients with neck pain: clinical outcomes from the UCLA neck-pain study. Am J Public Health. 2002;92(10):1634–1641 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Farrar JT, Young JP, Jr, LaMoreaux L, Werth JL, Poole RM. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94(2):149–158 [DOI] [PubMed] [Google Scholar]
- 26.Zou G. A modified Poisson regression approach to prospective studies with binary data. Am J Epidemiol. 2004;159(7):702–706 [DOI] [PubMed] [Google Scholar]
- 27.Levin J, Serlin R, Seaman M. A controlled, powerful multiple-comparison strategy for several situations. Psychol Bull. 1994;115(1):153–159 [Google Scholar]
- 28.Cherkin D, Sherman K, Kahn J, et al. A comparison of the effects of 2 types of massage and usual care on chronic low back pain: a randomized controlled trial. Ann Intern Med. 2011;155(1):1–9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Sherman KJ, Cherkin DC, Kahn J, et al. A survey of training and practice patterns of massage therapists in two US states. BMC Complement Altern Med. 2005;5:13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Haas M, Groupp E, Kraemer DF. Dose-response for chiropractic care of chronic low back pain. Spine J. 2004;4(5):574–583 [DOI] [PubMed] [Google Scholar]
- 31.Haas M, Groupp E, Aickin M, et al. Dose response for chiropractic care of chronic cervicogenic headache and associated neck pain: a randomized pilot study. J Manipulative Physiol Ther. 2004;27(9):547–553 [DOI] [PubMed] [Google Scholar]
- 32.Perlman AI, Ali A, Njike VY, et al. Massage therapy for osteoarthritis of the knee: a randomized dose-finding trial. PLoS One. 2012;7(2):e30248. [DOI] [PMC free article] [PubMed] [Google Scholar]