

Abstract
Background:
Due to the anatomical variations of the paranasal sinuses and its great importance in sinus surgery, as this area is in very close proximity to vital structures including the optic nerve, carotid artery, and skull base, anatomical knowledge of this area is of high importance. The purpose of this study is defining a full and clear impression of paranasal sinus anatomy and its variations as a model for the human population of the country.
Materials and Methods:
This study was conducted on 45 cadavers in Isfahan forensic Medicine center during 2010 to 2011. Nasal and paranasal sinuses endoscopic dissection was done with (zero and 30°) lenses (Olympus). The methods of performed dissection were via the Stamberger technique.
Results:
This study showed that 88.9% (40 cases) of middle turbinates were in a typical form, while 6.7% (3 cases) were in medial and only 4.4% (2 cases) were in the lateral form. We also observed 88.9% (40 cases) with Agger nasi cells, 37.8% (17 cases) with Onodi cells, 28.9% cases with accessory Ostia of maxillary sinus (13 cases), and 15.6% of the cases (7 cases) with concha bullosa. The position of the maxillary sinus ostium was as follows. The inferior 1/3 of hiatus semilunaris in 38 (84.5%), superior 1/3 of hiatus semilunaris in 4 (4.4%), middle 1/3 of hiatus semilunaris in 5 (11.1%). The sphenoid ostia in 53.3% (24 cases) were slit shape, 28.9% (13 cases) oval, and 17.8% (18 cases) were round shape.
Conclusion:
Our survey showed that the distance between anterior nasal spine and anterior wall of the sphenoid sinus was within 7.6 ± 0.2 cm SD.
Keywords: Anatomical variations, onodi cell, paranasal sinuses
INTRODUCTION
Some diagnostic and therapeutically procedures are invasive and may be associated with severe discomfort and side effects for the patients.
By the advent of nasal endoscopy in 1950s, it opened a new window to the world of medicine and revolutionized nasal and paranasal sinus surgeries with better results and less discomfort for the patients.
In order to perform proper nasal endoscopy (diagnostic and therapeutic), complete and exact understanding of anatomy and anatomical variations of paranasal sinuses is vital.
The anatomy of paranasal sinuses is extremely complex due to their close proximity to important organs such as optic nerve, carotid artery, and skull base and this clarifies the importance of recognition of anatomical variations in this area. Functional endoscopic sinus surgery has become popularized during the last decade for treatment of many diseases that related to nose and sinuses all over the world. So, knowledge about the intricate anatomy and normal variations of sinus and related structures is of vital importance for the sinus surgeon to avoid probable complications. Although the importance of variation of sinus anatomic is undeniable, in our country there is not inclusive study on this issue.
MATERIALS AND METHODS
This survey was performed in legal medicine center of Isfahan, with consideration of medical ethics criteria on 45 cadavers (90 nasal cavities) in 2010–2011.
Cadavers were 18 to 60 years without the history of sinus diseases, nasal surgery or facial traumatic injury; all cadavers were dissected during the first day of their death time. All specimens were randomly selected for dissection.
Endoscopy was performed by 0° and 30° degree Olympus telescopes [Figure 1] via Stammberger's method.
Figure 1.

Olympus telescopes, 0° and 30°
By conducting the telescope 0° in first step toward middle meatus, the anatomical characteristics of the area were evaluated. A questionnaire of cadaver's informative data and endoscopic findings (e.g., age, sex, middle turbinate variation, ostium position, etc) for each cadaver was filled out for final analyses.
RESULTS
This study showed that the vast majority of middle turbinates shape were located normally in a typical form 88.9% (40 cases), 6.7% (3 cases) were medially form, and 4.4% (2 cases) wherein lateral form [Figure 2].
Figure 2.
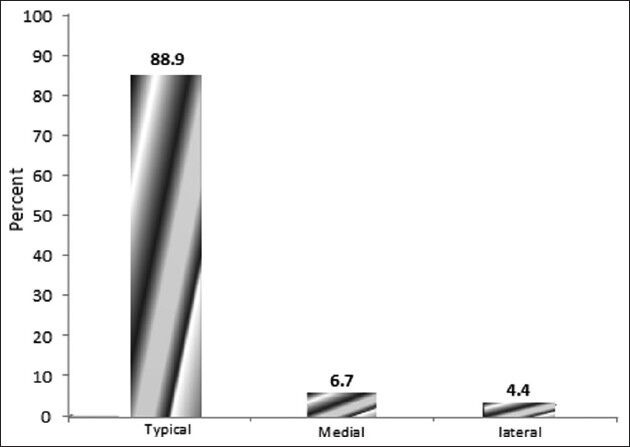
Middle turbinate location
Based on this study, the following data was observed: In 88.9% (40 cases) agger nasi cells, in 37.8% (17 cases) onodi cells, in 28.9% (13 cases) accessory ostia, and in 15.6% (7 cases) concha bullosa were observed [Figure 3].
Figure 3.
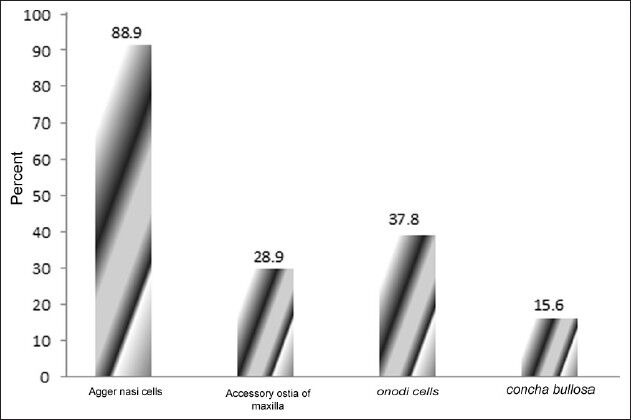
Air cell variations of nose & paranasal sinuses
The position of the maxillary sinus ostium within hiatus semilunaris was as follows: inferior 1/3 of hiatus semilunaris in 38 cases (84.5%), superior 1/3 of hiatus semilunaris in 4 (4.4%), and middle 1/3 of hiatus semilunaris in 5 (11.1%) cases [Figure 4].
Figure 4.
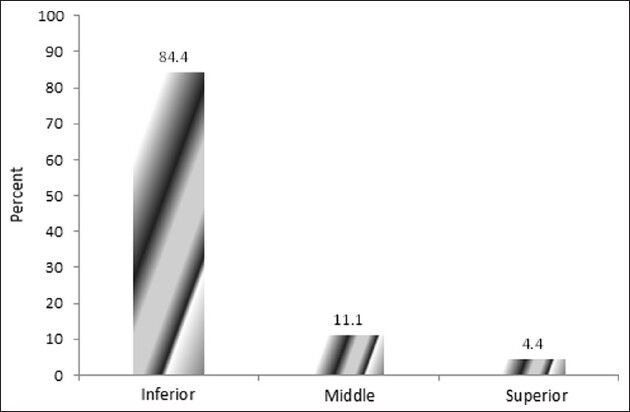
The position of maxillary sinus ostium
Sphenoid ostium in 53.3% (24 cases) was slit shape, in 28.9% (13 cases) oval, and in 17.8% (78 cases) were round [Figure 5].
Figure 5.
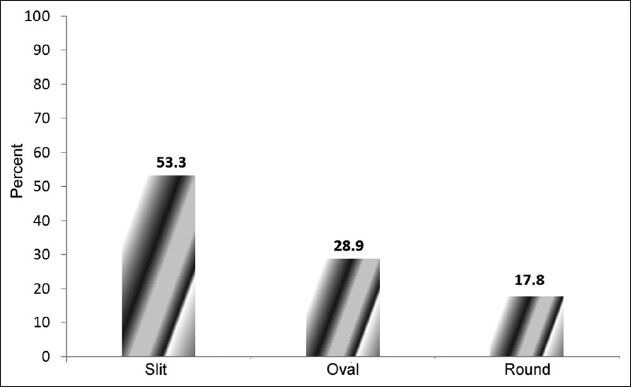
Shape of sphenoid sinus ostium
Our survey shows that the distance between anterior nasal spine and anterior wall of the sphenoid was 7.6 ± 0.2 cm SD.
DISCUSSION
The frequencies of variations of paranasal sinuses were evaluated in this study by using the endoscopic approach in cadavers. The result of the study indicates that the typical form of middle turbinate has been more prevalent (88.9%).
The study conducted by Nick-Akhlagh and colleagues on 75 patients with no history of sinus disease has reported the incidence of paradoxical turbinate were 5 percent. In this study, the prevalence of agger nasi cells in patients with sinus disease was 46%.[1]
The frequency of Onodi cells in our study was 37.8% compared whit results obtained by Zadanfarokh and colleagues on 25 cadavers which has been 36%. Comparative results performed by the authors showed that the frequency of onodi cells in patient whit chronic sinusitis were less than normal subjects.[2]
Another anatomical variation is concha bullosa which is a large bony cavity within the middle concha. It contains one or more air cells, and the communications of these cells sometimes are variable and complicated. In ref.[2] the incidence of these cells was 15% and it is shown that in patients with chronic sinusitis the prevalence of concha bullosa cells has been 28%. This rate has been 12.5% in patients with sinusitis symptoms in Dr. Bradaranfar and colleagues’ study.[3]
In our study, the prevalence of concha bullosa cells was 15.6%. The existence of accessory ostia were 28.9 in our study while this rate has been reported as 6% in.[2]
The prevalence of this variation maxillary ostia by L.C Prasanna was noted in 9 (22.5%) cases and absence in 31 (77.5%).[4]
Our studies showed that in more than 84% percent of cases, the maxillary sinus ostium has located inferior 1/3 of hiatus semilunaris and in 11.1% in middle 1/3 of it. In ref.[4], the study shows that the position of the maxillary sinus ostium in 40 dissected specimens as follows: the superior 1/3 of hiatus semilunaris in 4 (10%), inferior 1/3 of hiatus semilunaris in 21 (52.5%), middle 1/3 of hiatus semilunaris in 11 (27.5%) and absent in 4 (10%).
The anterior nasal spine to anterior sphenoid wall distance has been other parameter of our study that was equal to 7.6 cm ± 0.2 SD. Study conducted in Turkey on 50 cadavers by Turgut et al. showed that this rate was 7.5 cm.[5]
Anatomical sphenoid sinus shape variation was observed with the highest figure 53.3% was related to the slit shape.
CONCLUSIONS
Knowledge of anatomy of nasal cavity and paranasal sinuses, in addition to its different variations and racial varieties can be helpful for all Rhinologic surgeons in order to perform a safe nasal procedure with minimal rate of complications awareness about anatomical variations in endoscopic sinus surgery, can help surgeons earn this goal.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Nikakhlagh S, Saki N, Tahmasebi M, Johari H. Anatomic variations of the bone in sinonasal L CT scan: A report of 279 cases. Med Jundishapur Scientific Medical Journal. 6:476–83. winter 1380. [Google Scholar]
- 2.Zadanfarokh H, Naderian M. Comparison of the anatomic position of the lateral nasal wall in patients with chronic sinusitis and cadavers with endoscopic method. J Iran Univ Med Sci. 2008;1380:424–7. [Google Scholar]
- 3.Baradaranfar MH, Labibi M. Anatomic variations of paranasal sinuses in patients with chronic sinusitis and their correlation with CT scan staging. Acta Med Iranica. 2007;45:477–80. [Google Scholar]
- 4.Prasanna LC, Mamatha H. The location of maxillary sinus ostium and its clinical application. Indian J Otolaryngol Head Neck Surg. 2010;62:335–7. doi: 10.1007/s12070-010-0047-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Turgut S, Gemusalan Y, Arifoglu Y, Sinav A. Endoscopic anatomic distances on the lateral nasal wall. J Otolaryngol. 1996;25:371–4. [PubMed] [Google Scholar]
- 6.Cummings CW, Haughey BH, Regan Thomas J, Haker L, Flint PW. 5th ed. 2005. Cummings Otolaryngol Head Neck Surg; pp. 1229–53. [Google Scholar]
- 7.Setliff RC, Catalano PJ, Catalano LA, Francis C. An aatomic classification of the ethmoidal bulla. Otolaryngol Head Neck Surg. 2001;125:598–602. doi: 10.1067/mhn.2001.120398. [DOI] [PubMed] [Google Scholar]
- 8.Fact sheet: Sinus surgery, in health information website. [Last accessed on 2011 Oct 25]. Available from: http://www.Entnet.org/HealthInformation/sinusSurgery.cfm” .