

Abstract
Background:
Ventilator associated pneumonia (VAP) are one of the most common nosocomial infections in intensive care unit (ICU). The ICU patients are at risk of stress ulcer and gastrointestinal bleeding for different reasons. In order to prevent this complication, anti acids are used for patients. This study compared pantoprazole with sucralfate in incidence of ventilator associated pneumonia.
Materials and Methods:
This randomized clinical trial was carried out on ICU patients with mechanical ventilation in Alzahra university hospital in Isfahan from 2010 to 2011. One hundred forty eight ventilated patients were randomly allocated in two groups. The first group was treated with sucralfate and the second group was treated with pantoprazole for stress ulcer prophylaxis and followed up during hospitalization in ICU for nosocomial pneumonia. Data analyzed by SPSS software.
Results:
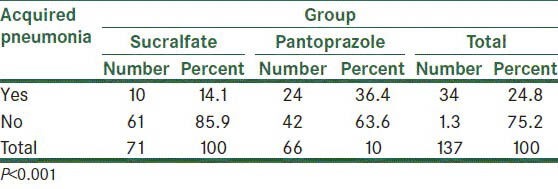
One hundred thirty seven patients were selected for study. During the study period, 34 cases (24.8%) acquired pneumonia, of which 10 were in the sucralfate group and 24 were in the pantoprazole group (14.1% vs. 36.4%). According to Chi-square test, rate of pneumonia was significantly lower in patients receiving sucralfate than the pantoprazole group (P < 0.001).
Conclusion:
On the basis of the results, there is a significant relationship between the kind of drug used for stress ulcer and ventilator associated pneumonia. According to this article, rate of pneumonia was significantly lower in patients receiving sucralfate than the pantoprazole group.
Keywords: Pantoprazole, sucralfate, ventilator associated pneumonia
INTRODUCTION
The prevalence of nosocomial infections in ICU are 5 to 10 times as much as those is general wards. Mechanical ventilator, urinary catheters, and intravenous catheters are the major causes of this difference. Based on the report by Center for Disease Control, nosocomial infections caused 88,000 deaths in the United States.[1] Ventilator-associated pneumonia (VAP) is the first cause of death due to nosocomial infection in ICU with an incidence of 9% in ventilated patients.[2] These infections increase duration of hospitalization, and mortality by 5 to 65% and increase treatment costs.[2,3] Furthermore, several risk factors play a role in its incidence, which can increase hospitalization period in ICU, treatment costs, and mortality.[3] One of the predisposing factors of VAP is related to gastrointestinal disorders and administration of antacids like pantoprazole, and sucralfate, which facilitates colonization of bacteria, especially gram negative bacteria in nasopharynx and their aspiration to the lungs. This process increases the risk of pneumonia, so administration of an appropriate antacid with the least complications can significantly reduce the risk of VAP, and hence, reduce mortality, morbidity, and costs, and improves patients’ health.[4]
Ventilator-associated pneumonia (VAP) is defined as a group of pneumonias that occur 48 h after the patient is ventilated if the patient did not have primary signs of the infection at the time of arriving ICU. VAP is one of the most prevalent nosocomial infections and pneumonia is causes 27% of infections in ICU.
Symptoms and signs of pneumonia are fever, leukocytosis and purulent discharge. Laboratory testing is the best diagnostic method. Administration of antibiotics and cooperation with laboratory are important subjects after diagnosis. Furthermore, as the duration of hospitalization increases, the risk of VAP and incidence of more dangerous organisms in ventilated patients increase.[5]
Finally, the ICU patients are at risk of stress ulcer for different reasons, which can put patients at risk of pneumonia because of the reflux and entering stomach contents to pharynx and lungs.[6] To prevent from stress ulcer, anti reflux and antacids are administered for ICU patients, two of which are sucralfate and pantoprazole.[7] Sucralfate covers the stomach mucosa and prevents movement of bacteria toward pharynx and lungs. Pantoprazole inhibits proton pump, and prevents acid secretion. So patients who receive sucralfate experience aspiration pneumonia less[8] Therefore, this study aimed to compare the incidence of nosocomial pneumonia in two groups of patients receiving these drugs in Al-Zahra Hospital in Isfahan.
MATERIALS AND METHODS
This clinical trial was conducted on two groups of 74 ICU patients in Al-Zahra Hospital in Isfahan. Patients were treated with sucralfate or pantoprazole. The study was conducted between early 2010 to mid 2011. Inclusion criteria were admission to ICU, and accepting to cooperate. Exclusion criteria were early discharge from ICU, death before 10 days, inception of antibiotic before incidence of pneumonia or sensitivity to the drug. The study was approved by the medical universities ethics committee Isfahan University of Medical Sciences.
Intensive care unit (ICU) patients were selected if they met the inclusion criteria. Then they or their companions were briefed, and after they agreed to cooperate, patients were consecutively assigned to each group. The first patient was selected randomly. Matching is essential in removing confounding factors that play a role in pneumonia, so group matching was done for gender and age ± 3 years. One group received pantoprazole, and the second group received sucralfate. Pneumonia was compared during their hospitalization period. Diagnostic criteria for pneumonia were CDC criteria.[9]
Data were entered into computer and analyzed using SPSS version 18. Tables were made using Word, and charts were drawn using Excel.
Statistical tests like Chi-square, Fisher's exact test (to compare qualitative data), and student t-test (to compare quantitative data) were used.
RESULTS
In this study, 148 ICU patients who met inclusion criteria entered the study, and were divided to two groups of 74 (sucralfate and pantoprazole groups). During the study period, 11 patients were excluded for different reasons like not using the drug, changing the drug by the physician, and so on. Three of them were from the pantoprazole and 8 of them were from sucralfate group. In the end, 71 patients in the pantoprazole group and 66 patients in the sucralfate group were studied.
Mean age of all patients was 50.6 ± 20.4 years old ranging from 10 to 89 years old. Mean age of sucralfate and pantoprazole groups was 49.8 ± 19.5 and 51.5 ± +21.4 years old, respectively. Because two groups were matched for age, their mean age was similar. The results are shown in Table 1.
Table 1.
Frequency distribution of variables in both groups
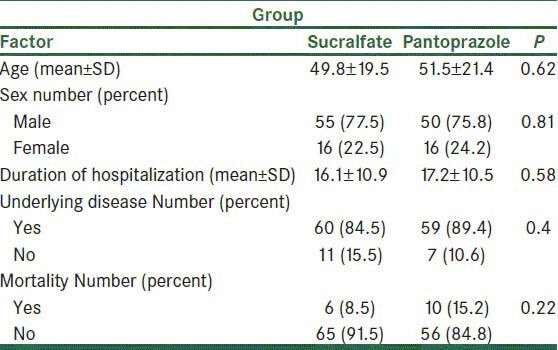
It is noteworthy that 105 patients were men and 32 were women. As for each group, 55 and 50 (77.5% vs. 75.5%) were men in the sucralfate and pantoprazole group, respectively. Because two groups were matched for sex, its distribution was similar in both groups [Table 1].
Mean hospitalization period in all patients was 21.7 ± 13.3 days with minimum and maximum duration of 4 and 90 days, respectively. Mean duration of hospitalization in the sucralfate and pantoprazole groups was 21.1 ± 13.8 and 22.4 ± 12.9 days. On the basis of t test, the mean duration of hospitalization was not different in two groups. (P = 0.56) [Table 1].
The duration of being ventilated in sucralfate group and pantoprazole group was 16.1 ± 10.9 and 17.2 ± 10.5 days, respectively. t-test showed no significant difference between the two groups. (P = 0.58) [Table 1].
Underlying disease
In this study, 119 patients (86.9%) had underlying diseases like hypertension, diabetes, cancer, asthma, cardiovascular diseases, myocardial infarction, CVA, and so on. Sixty of them were in the sucralfate group and 59 of them were in the pantoprazole group. (84.5% vs. 89.4%) Chi-square test showed no significant difference between the two groups. (P = 0.4) [Table 1].
Total numbers of deceased patients were 16 (11.7%), of whom 6 were from the sucralfate group and 10 were from the pantoprazole group. (8.5% vs. 15.2%) Chi-square test showed no significant difference between the two groups. (P = 0.22) [Table 1].
During the study period, of 137 ICU patients, 34 (24.8%) acquired pneumonia, 10 of whom were in the sucralfate group and 24 were in the pantoprazole group (14.1% vs. 36.4%). Chi-square test showed that the incidence of pneumonia in sucralfate group was significantly lower than that in the pantoprazole group (P < 0.001). The results are shown in Table 2.
Table 2.
Frequency distribution of the incidence of pneumonia in two groups
Radiography findings
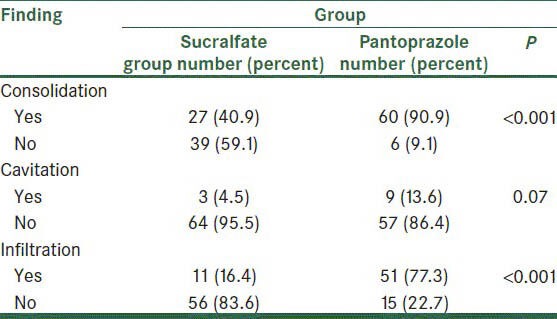
According to the results, 87 patients (65.9%) had consolidation in their X-ray, of whom 27 were in the sucralfate group and 60 were in the pantoprazole group. (40.9% vs. 90.9%) Chi-square test showed that consolidation was significantly higher in the pantoprazole group (P < 0.001).
Cavitation was seen in X-ray of 12 patients (9%), 3 of whom were in the sucralfate group and 9 were in the pantoprazole group (4.5% vs. 13.6%). Chi-square test showed no significant difference (P = 0.07).
New, progressive or chronic infiltration was seen in 62 cases, of whom 11 were in sucralfate and 51 were in pantoprazole group (16.4% vs. 77.3%). Chi-square showed a significant difference. (P < 0.001) The results are shown in Table 3.
Table 3.
Frequency distribution of radiography findings in two groups
Clinical findings
Table 4 shows the frequency distribution of clinical findings in both groups. The number of patients with fever was 116 (84.7%), of whom 54 were in sucralfate group and 62 were in pantoprazole group (76.1% vs. 93.9%). Chi-square test showed a significant difference. (P = 0.004) Furthermore, the number of patients with leukocytosis was 108 people (78.8%), of whom 45 people were in pantoprazole group and 63 were in sucralfate group (63.4% vs. 95.5%). The difference was significant (P < 0.001).
Table 4.
Frequency distribution of clinical findings in two groups
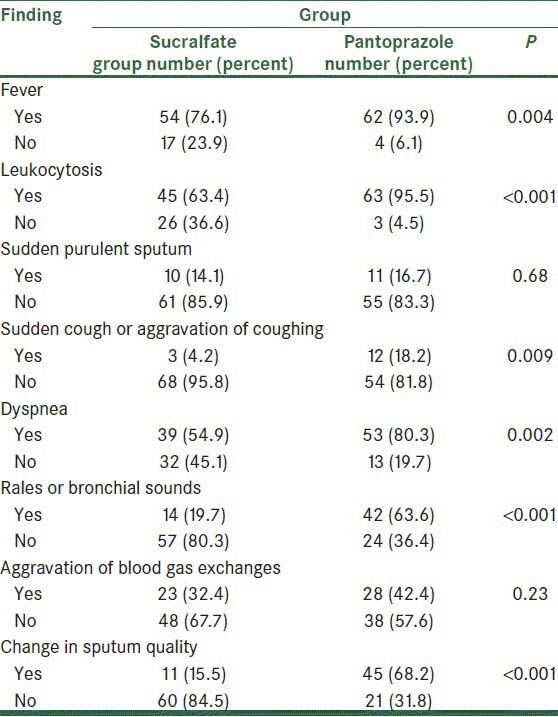
Twenty-one patients (15.3%) suddenly had purulent sputum, of whom 10 were in sucralfate group and 11 were in the pantoprazole group. (14.1% vs. 16.7%) Chi-square showed no significant difference between the two groups (P = 0.68).
Fifteen patients suddenly had cough or their cough aggravated, of whom 3 were in the sucralfate group and 12 were in the pantoprazole group. (4.2% vs. 18.2%) Chi-square test showed a significant difference between the two groups (P = 0.009).
Dyspnea was seen in 92 patients (67.2%), of whom 39 patients were in sucralfate group and 53 were in the pantoprazole group (54.9% vs. 80.3%). The difference between the two groups was significant (P = 0.002).
Tachypnea was observed in 115 patients (83.9%), of whom 56 were in sucralfate group and 59 were in the pantoprazole group. (78.9% vs. 89.4%), but the difference was not significant (P = 0.09).
Fifty-six patients had rales, of whom 14 were in the sucralfate group and 42 were in the pantoprazole group (19.7% vs. 63.6%). The difference was significant (P < 0.001).
During the study, in 51 patients (37.2%) blood gas exchange aggravated, of whom 23 were in the sucralfate group and 28 were in the pantoprazole group. (32.4% vs. 42.4%) The difference was not significant (P = 0.023).
Finally, the properties of sputum changed or increased in 56 patients (40.9%), of whom 11 were in the sucralfate group and 45 were in the pantoprazole group (15.5% vs. 68.2%). The difference was significant in two groups (P < 0.001).
Mean age of patients with and without pneumonia was, respectively, 54.6 ± 18 and 49.3 ± 21 years. According to t test, the age of the patients did not have a significant effect on pneumonia (P = 0.2). Figure 1 shows mean and confidence interval of age in both groups.
Figure 1.
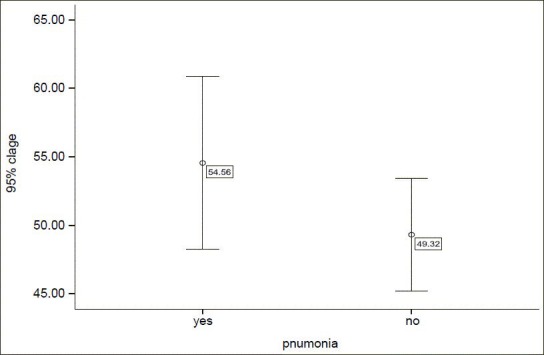
Mean and confidence interval of age in patients with and without pneumonia
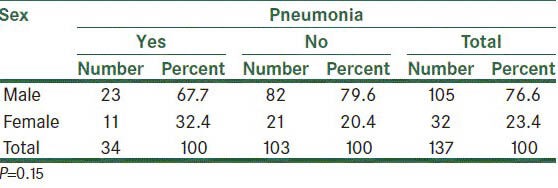
From sex point of view, pneumonia occurred in 23 men and 11 women (67.6% vs. 32.4%), but Chi-square test showed no significant difference between the two sexes. (P = 0.15) The results are shown in Table 5.
Table 5.
Frequency distribution of the incidence of pneumonia in men and women
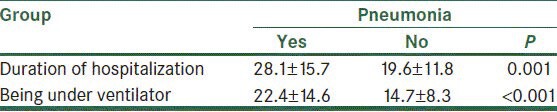
Mean duration of hospitalization in ICU in pneumonia patients was 28.1 ± 15.7 days, and in patients without pneumonia was 9.6 ± 11.8 days. t-test showed a significant difference between the two groups. (P = 0.001) The results are shown in Table 6. Furthermore, mean time of being ventilate in patients with and without pneumonia was 22.4 ± 14.6 and 14.7 ± 8.3 days, and the difference was significant (P < 0.001). The results are shown in Table 6. In group with and without pneumonia, respectively, 29 and 90 people had underlying diseases (85.3% vs. 87.4%), but the difference was not significant (P = 0.75).
Table 6.
Mean and standard deviation of duration of hospitalization and being ventilated based on acquiring pneumonia
DISCUSSION
The main objective of this study was to compare pantoprazole and sucralfate in causing nosocomial VAP in ICU of Al-Zahra Hospital.
In this study, the two groups did not have a significant difference in age, sex, duration of ventilation, duration of hospitalization in ICU, and underlying diseases. So, they were matched and the confounding effect of those factors and the bias was not present in the study. In other words, the two groups could be compared.
During this study, 137 patients were studied, of whom 34 (24.8%) acquired pneumonia. 14.1% were in the sucralfate group and 36.4% were in the pantoprazole group. That is, the incidence of pneumonia in the sucralfate group was significantly lower than that in the pantoprazole group. Sucralfate and pantoprazole are among most common drugs used in ICU to prevent stress ulcer. Sucralfate covers the stomach mucosa and prevents the movement of bacteria toward pharynx and lungs while pantoprazole inhibits proton pump and prevents acid secretion. So patients who receive sucralfate experience aspiration pneumonia less.[8]
Stress ulcer is the most common cause of gastrointestinal bleeding in ICU patients, and its prophylaxis can reduce mortality. Paying attention to drug side effects, especially pneumonia and its costs can limit using this prophylaxis.[10]
Reza Ghaffari et al. (2008) from Tehran University of Medical Sciences compared the incidence of aspiration pneumonia in two groups of patients receiving ranitidine and sucralfate. The incidence of pneumonia was significantly less in sucralfate group than in ranitidine group.[9]
Nezam Seyed Kazem (2005) from Zahedan University of Medical Sciences compared ranitidine and sucralfate drugs, which showed no effect in prevention of stress ulcer bleeding.[11]
In the present study, other variables like age and sex did not have a meaningful effect on the incidence of pneumonia, but duration of ICU hospitalization and duration of being ventilated were the factors effective on pneumonia. Furthermore, logistic regression test showed that in addition to administered drug, duration of being ventilated had a significant effect on the incidence of pneumonia. Of course, the drug had a more powerful effect on the incidence of pneumonia in that it was 3 times as much in the sucralfate group as in the pantoprazole group.
In a study by Miano et al. (2009), ranitidine and pantoprazole were compared in their role in preventing VAP. Of 377 patients in the pantoprazole group, there were 35 cases (9.3%) of pneumonia while 7 cases (1.5%) of 457 patients in the ranitidine group acquired pneumonia, that is, the incidence of pneumonia was significantly higher in the pantoprazole group.[12]
David and Metz compared ranitidine, sucralfate, and pantoprazole in the incidence of aspiration pneumonia and found no significant difference among the three groups.[13]
CONCLUSION
The role of anti acid medication in the incidence of nosocomial pneumonia is justified by the fact that these drugs lay the ground for bacterial growth by reducing stomach acid, so the increased bacterial growth and aspiration of stomach content increase the probability of nosocomial pneumonia. In the present study, the incidence of nosocomial pneumonia was higher in the pantoprazole group than in the sucralfate group.
Footnotes
Source of Support: Isfahan University of medical sciences
Conflict of Interest: None declared.
REFERENCES
- 1.Ghiasvandian MS. Nosocomial infection in the intensive care unit. Hayat. 2002;8:27–34. [Google Scholar]
- 2.Koenig SM, Truwit JD. Ventilator-associated pneumonia: Diagnosis, treatment, and prevention. Clin Microbiol Rev. 2006;19:637–57. doi: 10.1128/CMR.00051-05. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Abele-Horn M, Dauber A, Bauernfeind A, Russwurm W, Seyfarth-Metzqer I, Gleich P, et al. Decrease in nosocomial pneumonia in ventilated patients by selective oropharyngeal decontamination (SOD) Intensive Care Med. 1997;23:187–95. doi: 10.1007/s001340050314. [DOI] [PubMed] [Google Scholar]
- 4.Doschner I. Stress ulcer prophylaxis and ventilation peunmonia. Available from: http://www.JSTOR.org/pss .
- 5.Zandyeh M, Falhgari G, Salavsti M, Borzoo S. Study of applying proposed infection control standards in ICU. J Shahr-e-Kord Univ Med Sci. 2005;6:79–86. [Google Scholar]
- 6.Fabian TC, Boucher BA, Croce MA, Kuhl DA, Janning SW, Coffey BC, et al. Pneumonia and stress ulceration in severely injured patients. A prospective evaluation of the effects of stress ulcer prophylaxis. Arch Surg. 1993;128:185–91. doi: 10.1001/archsurg.1993.01420140062010. [DOI] [PubMed] [Google Scholar]
- 7.Ryan P, Dawson J, Teres D, Celoria G, Navab F. Nosocomial pneumonia during stress ulcer prophylaxis with cimetidine and sucralfate. Arch Surg. 1993;128:1353–7. doi: 10.1001/archsurg.1993.01420240061011. [DOI] [PubMed] [Google Scholar]
- 8.Quenot JP, Thiery N, Barbar S. When should stress ulcer prophylaxis be used in the ICU. Available from: http://nananaru.webs.com/med/reviews . [DOI] [PubMed]
- 9.Najafi A, Ghaffari SR, Mojtahedzadeh M, Khajavi MR, Haji Mohammadi F, Haji Mohammadi M. Comparison the incidence of aspiration pneumonia in criticaly ill patients recieving sucralfate or ranitidine in Sina hospital in the years of 1382-1383. J Iran Soc Anesthesiol Intensive Care. 2005;2:28–36. [Google Scholar]
- 10.Horan TC, Gaynes RP. 3rd ed. Philadelphia: Lippincott Williams and Wilkins; 2004. Surveillance of nosocomial infections; pp. 1659–702. [Google Scholar]
- 11.Nezam K, Borjian S, Rahati O. The effect of prophylaxis therapy on prevention from gastrointestinal bleeding in ICU in patients. Zahedan J Res Med Sci. 2005;7:9–15. [Google Scholar]
- 12.Miano TA, Reichert MG, Houle TT, Macgregor DA, Kincaid EH, Bowton DL. Nosocomial pneumonia risk and stress ulcer prophylaxis: A comparison of pantoprazole vs ranitidine in cardiothoracic surgery patients. Chest. 2009;136:440–7. doi: 10.1378/chest.08-1634. [DOI] [PubMed] [Google Scholar]
- 13.David C. Gastrointestinal effects of stress-related mucosal disease: Risk of nosocomial pneumonia. Available from: http://www.medscape.com/viewarticle/